Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection †



Abstract
1. Introduction
1.1. Current Clinical Technologies
1.2. Previous Studies on Acoustic Analysis of the Chest
1.3. Acoustic Properties of the Lungs
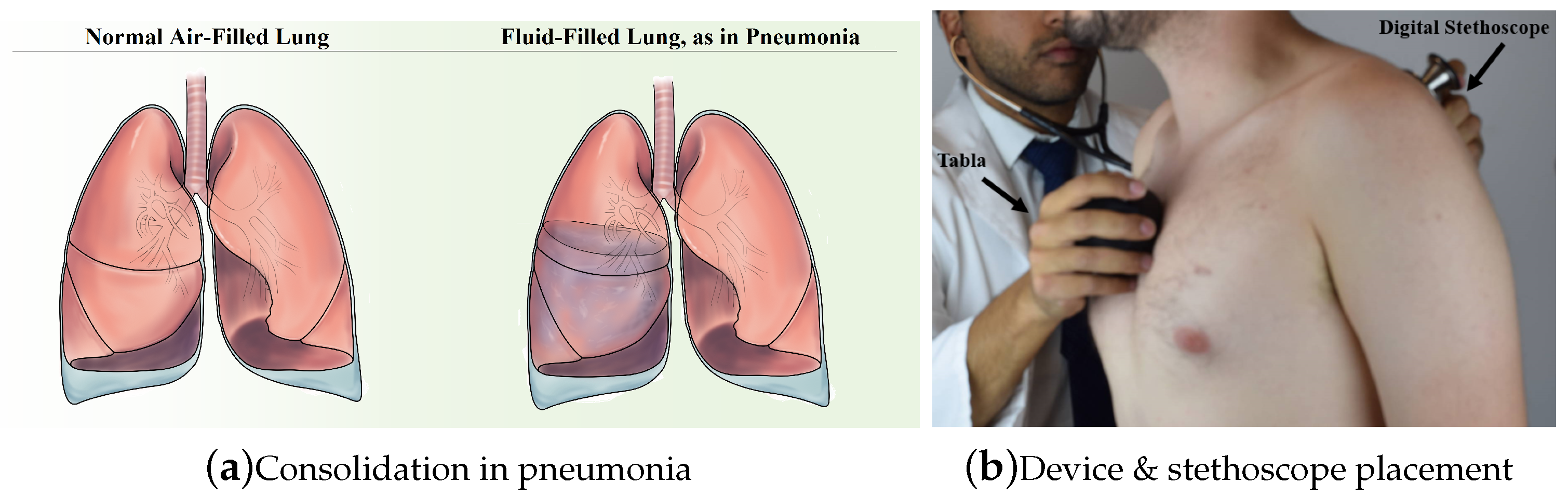
1.4. Pathophysiology and Physical Exam Findings in Pneumonia
2. Materials and Methods
2.1. Approach and Statement of Contributions
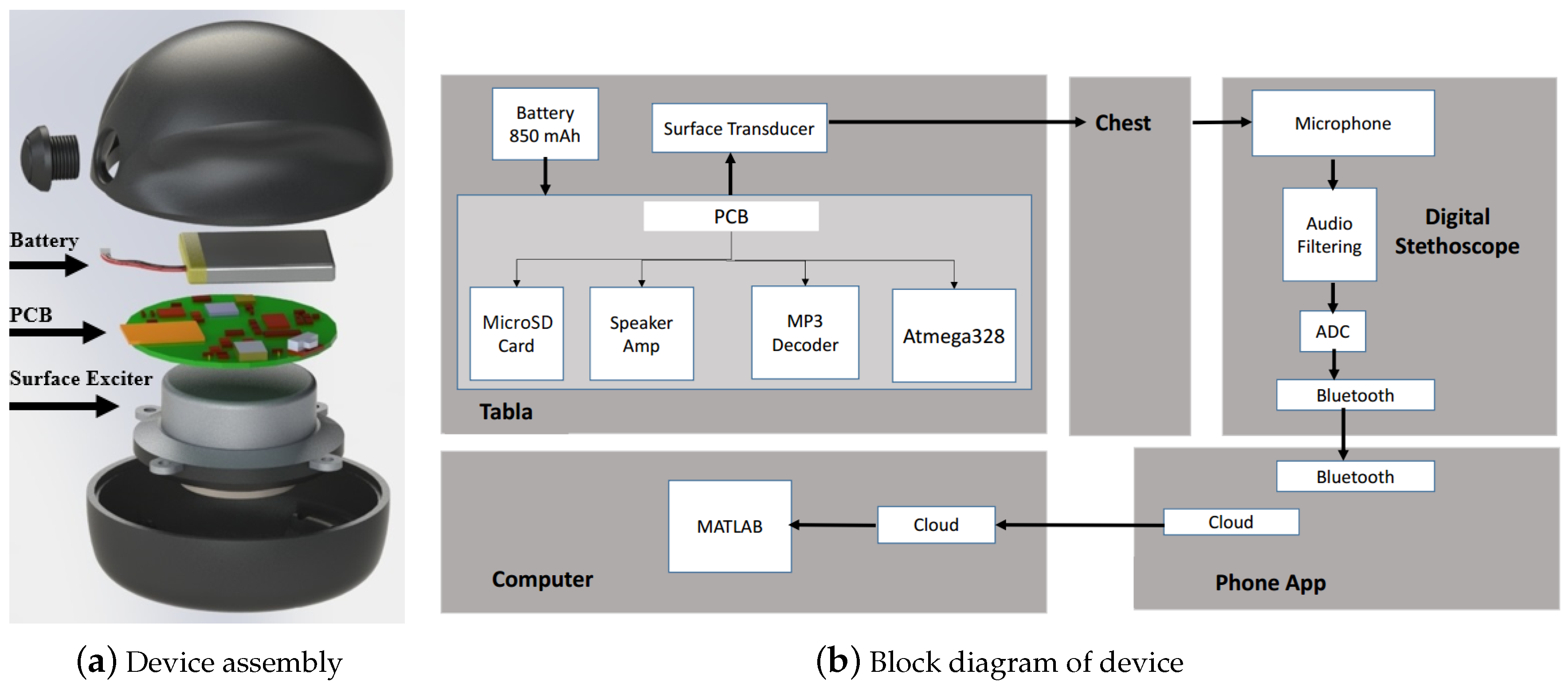
2.2. Principle of Operation
2.3. Actuator
2.4. Sensors
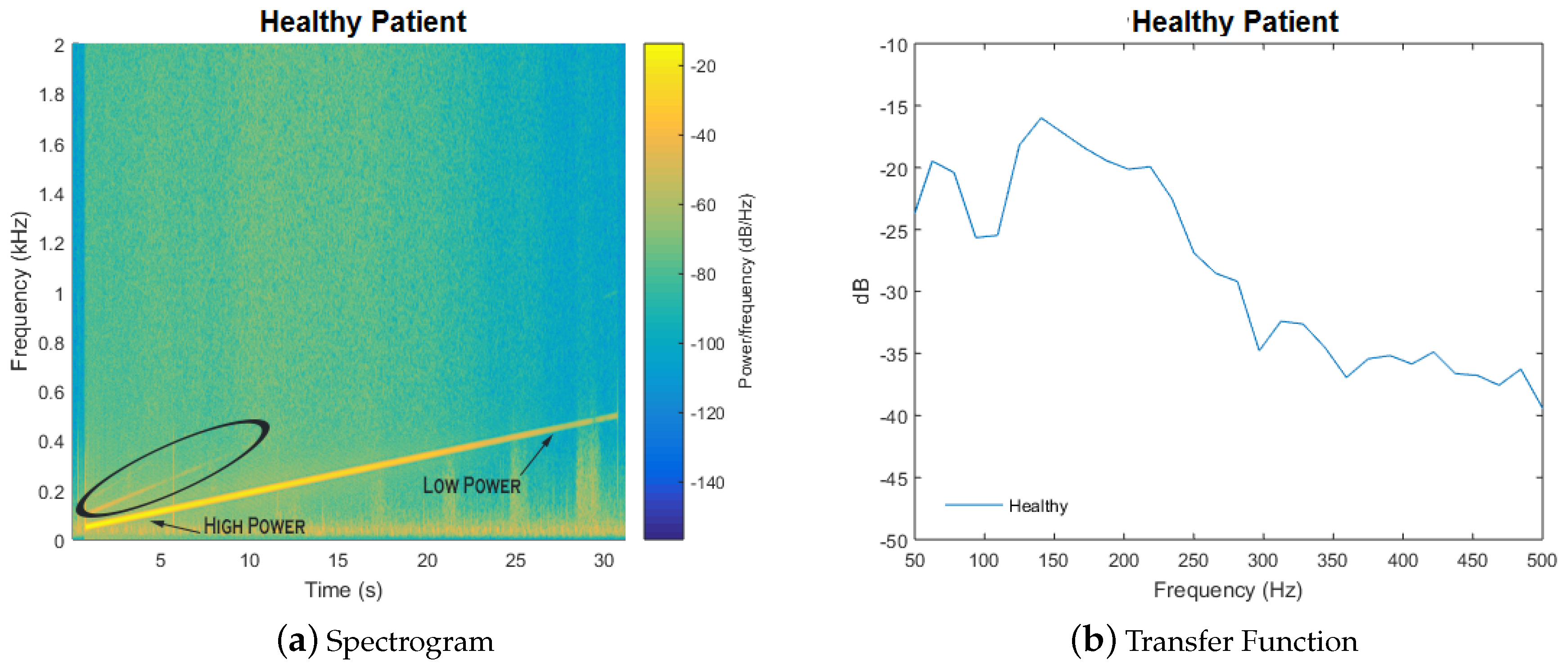
2.5. Signal
2.6. Signal Processing
2.7. Classification
3. Results and Discussion
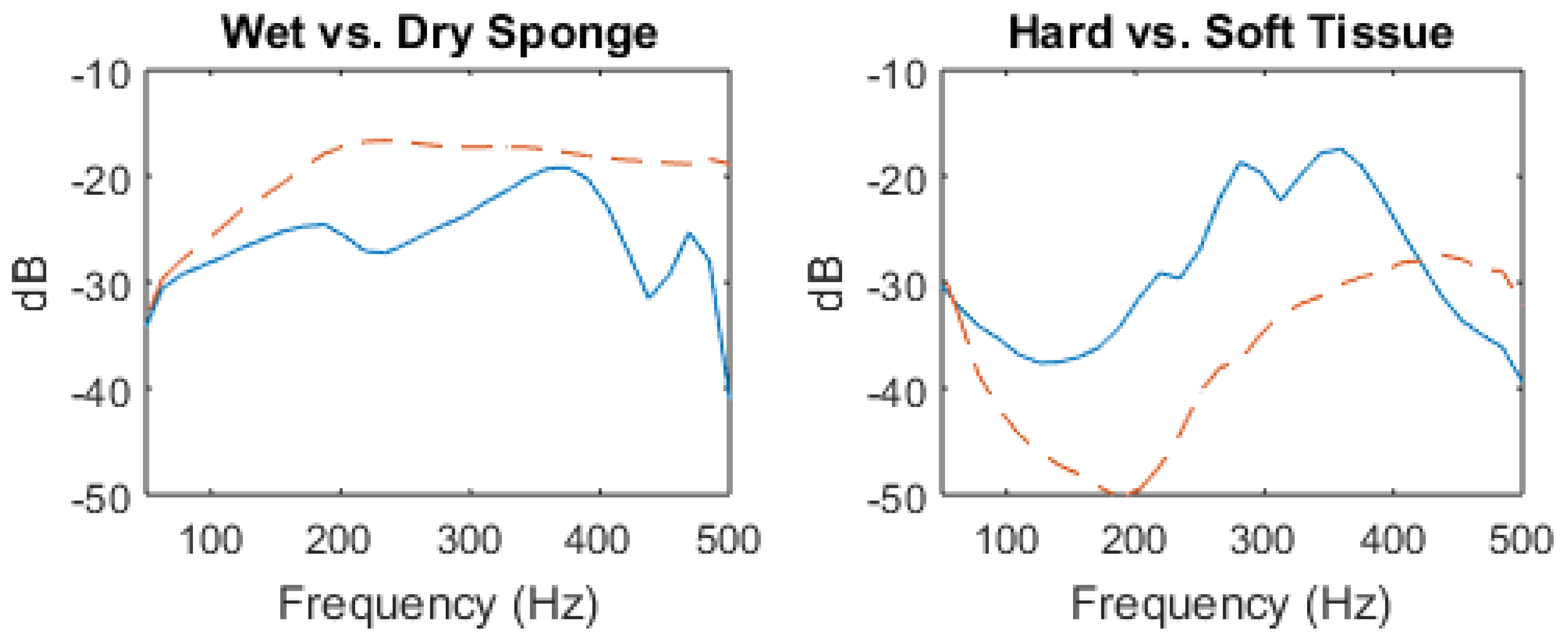
3.1. Water Filled Sponge vs. Air Filled Sponge
3.2. Solid Tissue vs. Air-Filled Cavity Response
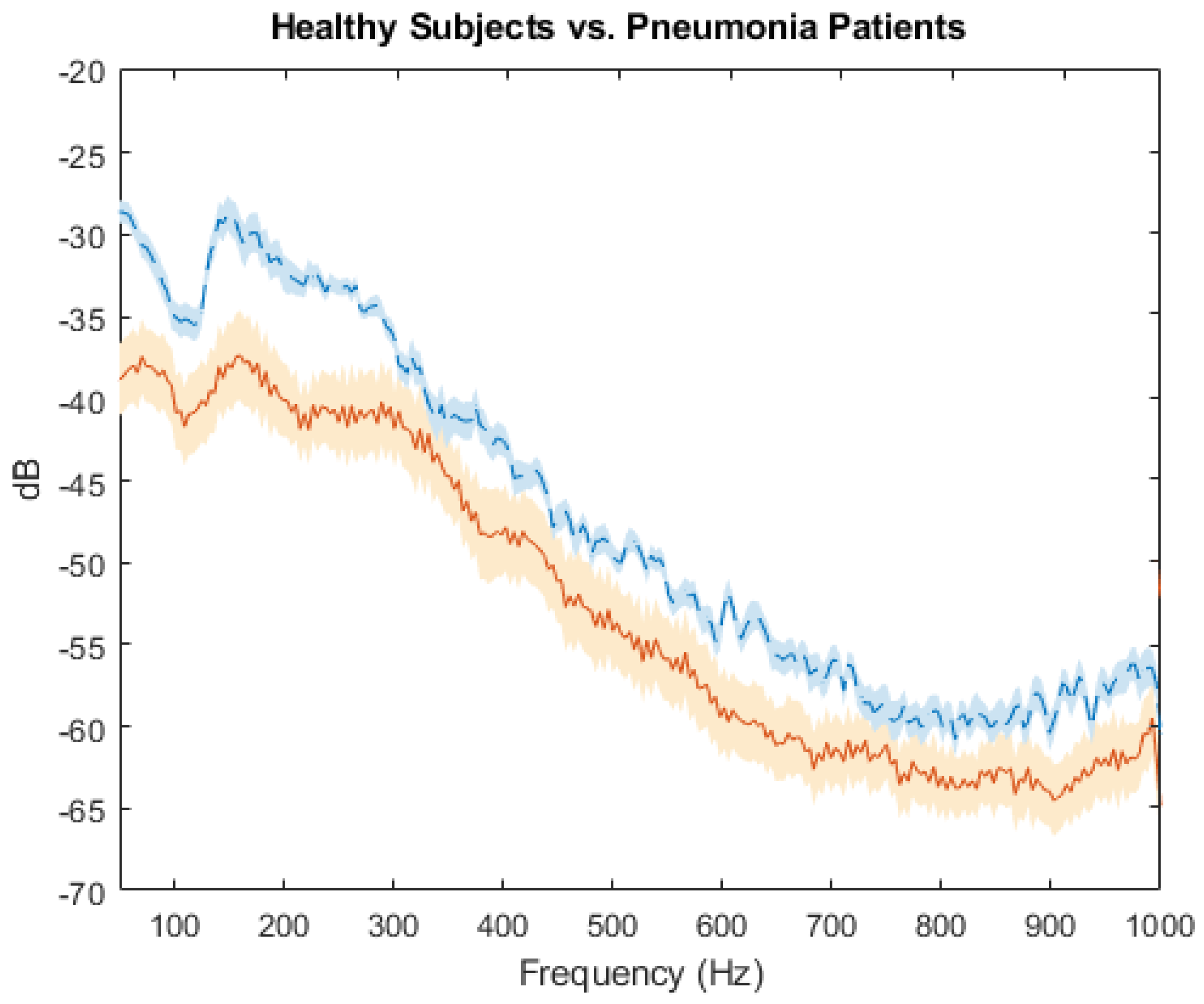
3.3. Clinical Proof of Concept
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Pneumonia Fact Sheet 2016. Available online: http://www.who.int/mediacentre/factsheets/fs331/en/ (accessed on 8 December 2016).
- UNICEF. Pneumonia Kills Half a Million Children under Five in Sub-Saharan Africa. Available online: https://www.unicef.org/media/media_89995.html (accessed on 8 December 2016).
- Kadilli, E. Pneumonia Acute Respiratory Infection Diagnostic Aid Target Product Profile. Available online: https://www.unicef.org/supply/files/Pneumonia_Diagnostics_Aid_Device_TPP_Introduction.pdf (accessed on 12 November 2016).
- Reissig, A.; Gramegna, A.; Aliberti, S. The role of lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia. Eur. J. Intern. Med. 2012, 23, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Syrjälä, H.; Broas, M.; Suramo, I.; Ojala, A.; Lähde, S. High-resolution computed tomography for the diagnosis of community-acquired pneumonia. Clin. Infect. Dis. 1998, 27, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Albaum, M.N.; Hill, L.C.; Murphy, M.; Li, Y.H.; Fuhrman, C.R.; Britton, C.A.; Kapoor, W.N.; Fine, M.J. Interobserver reliability of the chest radiograph in community-acquired pneumonia. Chest 1996, 110, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Agarwal, R.; Aggarwal, A.N.; Singh, N.; Mishra, N.; Khilnani, G.; Samaria, J.; Gaur, S.; Jindal, S.; Pneumonia Guidelines Working Group. Guidelines for diagnosis and management of community-and hospital-acquired pneumonia in adults: Joint ICS/NCCP (I) recommendations. Lung India 2012, 29, 27–62. [Google Scholar] [CrossRef] [PubMed]
- Watkins, R.R.; Lemonovich, T.L. Diagnosis and management of community-acquired pneumonia in adults. Am. Fam. Phys. 2011, 83, 1299–1306. [Google Scholar]
- Guarino, J. Auscultatory percussion of the chest. Lancet 1980, 315, 1332–1334. [Google Scholar] [CrossRef]
- Wipf, J.E.; Lipsky, B.A.; Hirschmann, J.V.; Boyko, E.J.; Takasugi, J.; Peugeot, R.L.; Davis, C.L. Diagnosing pneumonia by physical examination: Relevant or relic? Arch. Intern. Med. 1999, 159, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Dai, Z.; Mansy, H.A.; Sandler, R.H.; Balk, R.A.; Royston, T.J. Sound transmission in the chest under surface excitation: An experimental and computational study with diagnostic applications. Med. Biol. Eng. Comput. 2014, 52, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Mansy, H.A.; Balk, R.A.; Warren, W.H.; Royston, T.J.; Dai, Z.; Peng, Y.; Sandler, R.H. Pneumothorax effects on pulmonary acoustic transmission. J. Appl. Physiol. 2015, 119, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Mor, R.; Kushnir, I.; Meyer, J.J.; Ekstein, J.; Ben-Dov, I. Breath sound distribution images of patients with pneumonia and pleural effusion. Respir. Care 2007, 52, 1753–1760. [Google Scholar] [PubMed]
- Sánchez Morillo, D.; León Jiménez, A.; Moreno, S.A. Computer-aided diagnosis of pneumonia in patients with chronic obstructive pulmonary disease. J. Am. Med. Inform. Assoc. 2013, 20, e111–e117. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Berstein, A. Acoustic transmission of the respiratory system using speech stimulation. IEEE Trans. Biomed. Eng. 1991, 38, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.A. Transmission of lung sounds. Semin. Respir. Med. 1985, 6, 166–170. [Google Scholar] [CrossRef]
- Gavriely, N.; Palti, Y.; Alroy, G. Spectral characteristics of normal breath sounds. J. Appl. Physiol. 1981, 50, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.A. Sound speed in pulmonary parenchyma. J. Appl. Physiol. 1983, 54, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Marrie, T.; File, T. Epidemiology, Pathogenesis, and Microbiology of Community-Acquired Pneumonia in Adults; UpTodate: Waltham, MA, USA, 2017. [Google Scholar]
- Metlay, J.P.; Kapoor, W.N.; Fine, M.J. Does this patient have community-acquired pneumonia?—Diagnosing pneumonia by history and physical examination. J. Am. Med. Assoc. 1997, 278, 1440–1445. [Google Scholar] [CrossRef]
- Sarkar, M.; Madabhavi, I.; Niranjan, N.; Dogra, M. Auscultation of the respiratory system. Ann. Thorac. Med. 2015, 10, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Tabla: An acoustic device designed for low cost pneumonia detection. In Proceedings of the 2017 IEEE Healthcare Innovations and Point of Care Technologies (HI-POCT), Bethesda, MD, USA, 6–8 November 2017; pp. 172–175.
- Yernault, J.C.; Bohadana, A. Chest percussion. Eur. Respir. J. 1995, 8, 1756–1760. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Loudon, R.G. Sound Spectral Analysis of Voice-Transmitted Sound 1, 2. Am. Rev. Respir. Dis. 1986, 134, 167–169. [Google Scholar] [PubMed]
- Understanding Exciters—Principles and Applications. Available online: http://www.daytonaudio.com/media/resources/understanding-and-using-dayton-audio-exciters-revised.pdf (accessed on 2 September 2017).
- 3 M Littmann Electronic Stethoscope. Available online: https://www.littmann.com/3M/en_US/littmann-stethoscopes/products/~/Electronic-Stethoscopes (accessed on 5 March 2017).
- Eko Core Digital Stethoscope. Available online: https://ekodevices.com/core (accessed on 5 March 2017).
- ThinkLabs One Digital Stethoscope. Available online: https://www.thinklabs.com (accessed on 5 March 2017).
- Smith, J.D. Vibration Measurement and Analysis; Butterworth-Heinemann: Oxford, UK, 2013. [Google Scholar]
- Kahrs, M.; Brandenburg, K. Applications of Digital Signal Processing to Audio and Acoustics; Springer Science & Business Media: Berlin/Heidelberg, Germany, 1998; Volume 437. [Google Scholar]
- Tiwari, V. MFCC and its applications in speaker recognition. Int. J. Emerg. Technol. 2010, 1, 19–22. [Google Scholar]
- Eronen, A.; Klapuri, A. Musical instrument recognition using cepstral coefficients and temporal features. In Proceedings of the 2000 IEEE International Conference on Acoustics, Speech, and Signal Processing (ICASSP’00), Istanbul, Turkey, 5–9 June 2000; Volume 2, pp. II753–II756. [Google Scholar]
- Nioutsikou, E.; Symonds-Tayler, J.R.N.; Bedford, J.L.; Webb, S. Quantifying the effect of respiratory motion on lung tumour dosimetry with the aid of a breathing phantom with deforming lungs. Phys. Med. Biol. 2006, 51, 3359. [Google Scholar] [CrossRef] [PubMed]
- Moinuddin, B.M. Automated Classification of Medical Percussion Signals for the Diagnosis of Pulmonary Injuries. Ph.D. Thesis, University of Windsor, Windsor, ON, Canada, 2013. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Priority | Design Parameters |
|---|---|
| 5 (high) | Ease of use, high accuracy |
| 4 | Long operational lifespan (>2 years) |
| 3 | Highly portable, low cost, reliable, safe, automated diagnosis, robust |
| 2 | Low training requirements, long battery life, low maintenance, high comfort |
| 1 (low) | Little to no familiarity with technology required |
| Actuator Choice | |||||
|---|---|---|---|---|---|
| Criteria | Weight | Piezo | Solenoid | Speaker | Surf. Exciter |
| Intensity | 5 | 1 | 5 | 2 | 4 |
| Portability | 3 | 5 | 1 | 4 | 4 |
| Cost | 3 | 4 | 3 | 3 | 3 |
| Battery | 2 | 4 | 2 | 4 | 4 |
| Weighted Score | 40 | 41 | 39 | 49 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, A.; Ruiz, J.; Bao, C.; Roy, S. Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection. Sensors 2018, 18, 2689. https://doi.org/10.3390/s18082689
Rao A, Ruiz J, Bao C, Roy S. Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection. Sensors. 2018; 18(8):2689. https://doi.org/10.3390/s18082689
Chicago/Turabian StyleRao, Adam, Jorge Ruiz, Chen Bao, and Shuvo Roy. 2018. "Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection" Sensors 18, no. 8: 2689. https://doi.org/10.3390/s18082689
APA StyleRao, A., Ruiz, J., Bao, C., & Roy, S. (2018). Tabla: A Proof-of-Concept Auscultatory Percussion Device for Low-Cost Pneumonia Detection. Sensors, 18(8), 2689. https://doi.org/10.3390/s18082689