Optimization and Technical Validation of the AIDE-MOI Fall Detection Algorithm in a Real-Life Setting with Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
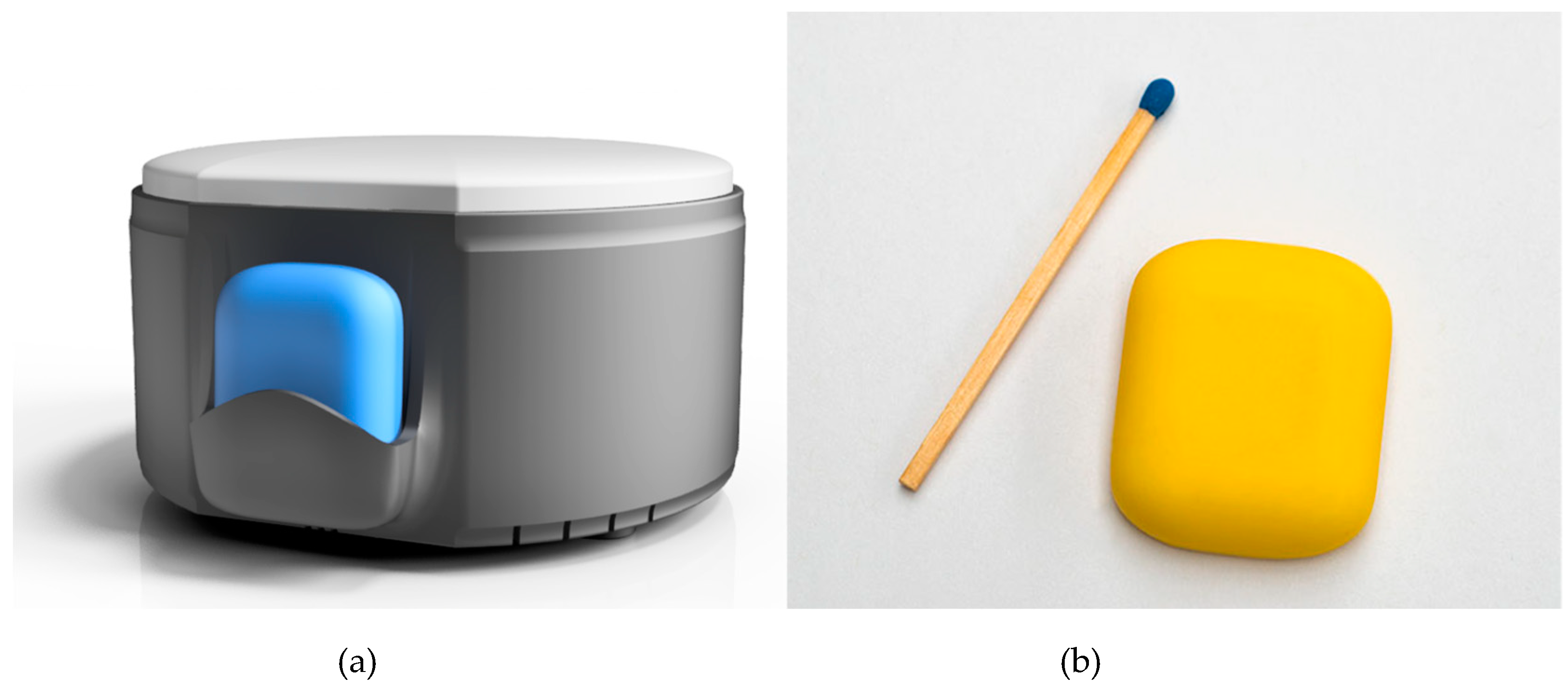
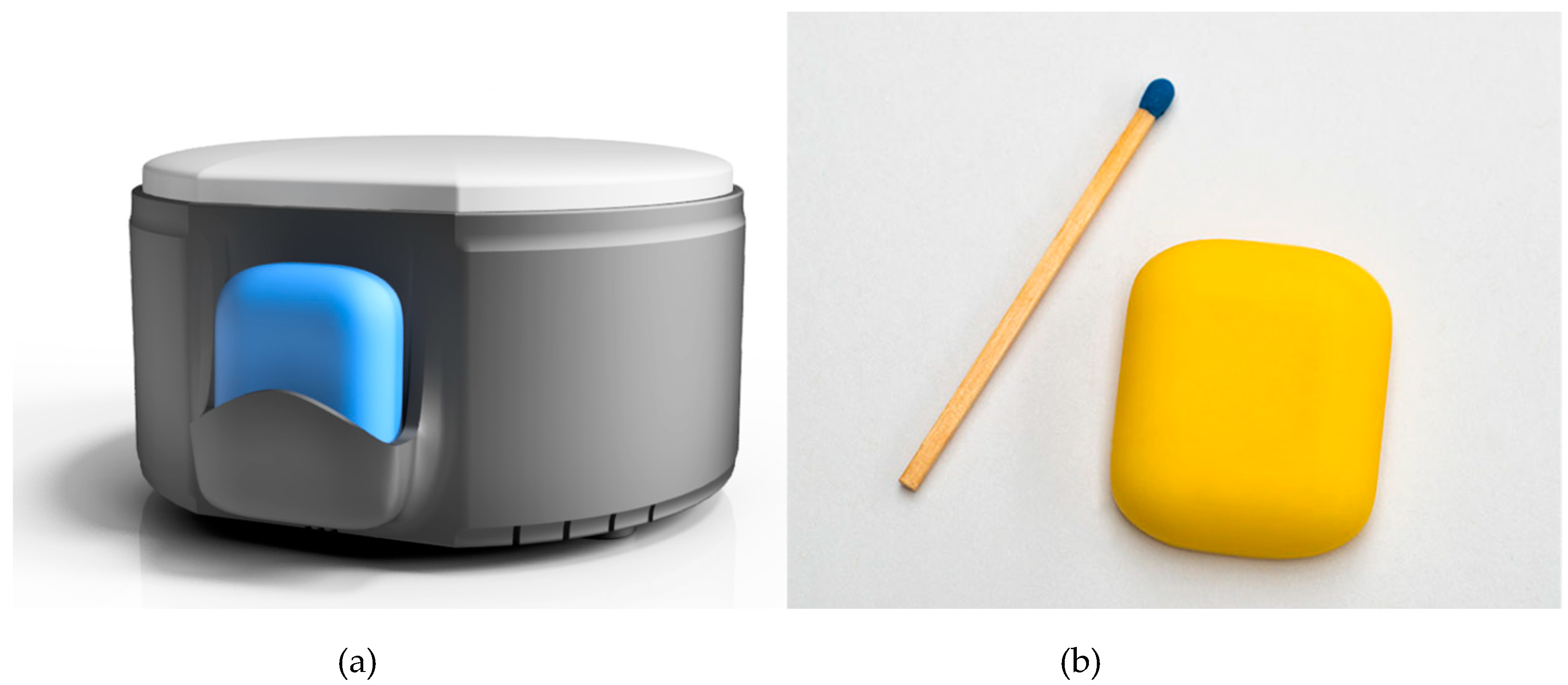
2.1. Material–Sensor System
2.2. Subject Recruitment
2.3. Study
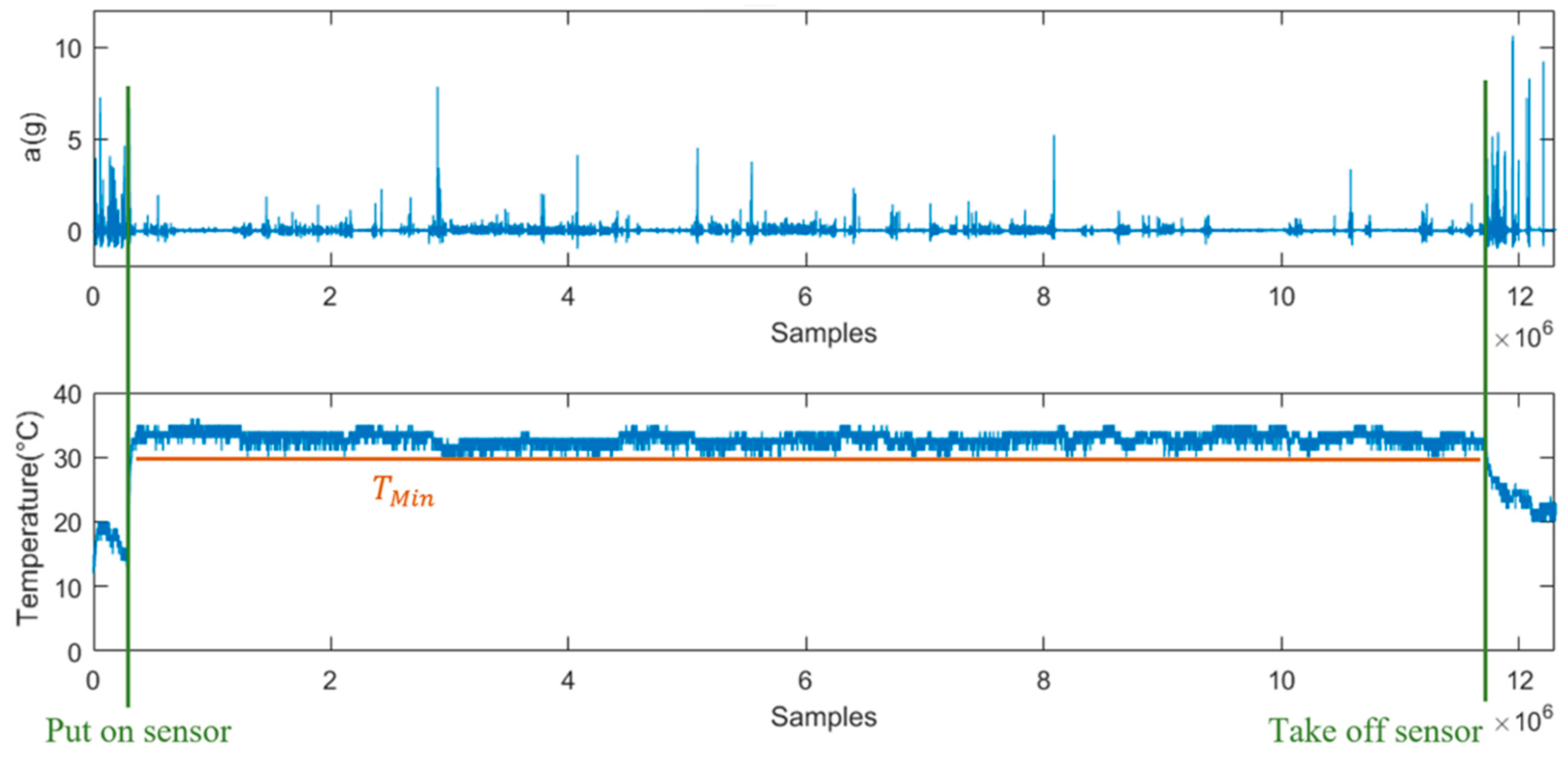
2.4. Sensor Data Collection
2.5. Fall Definition
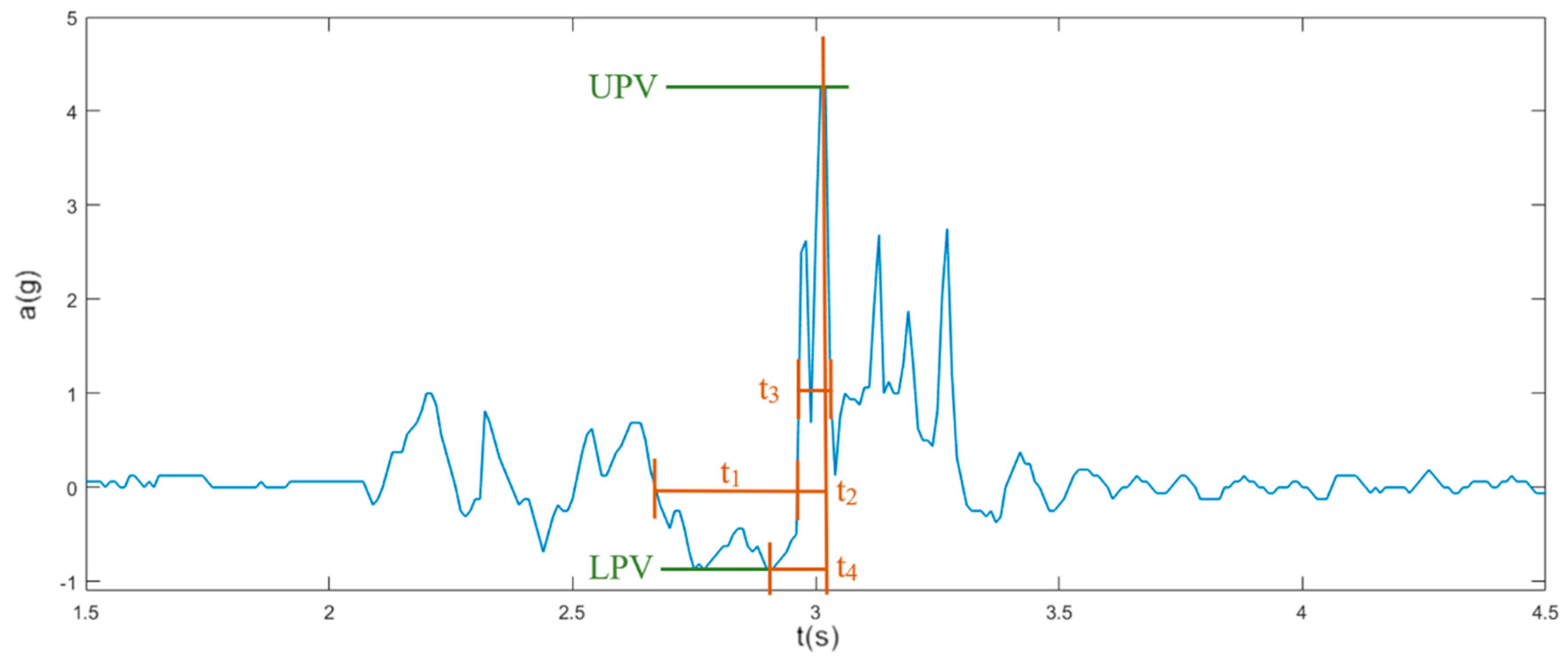
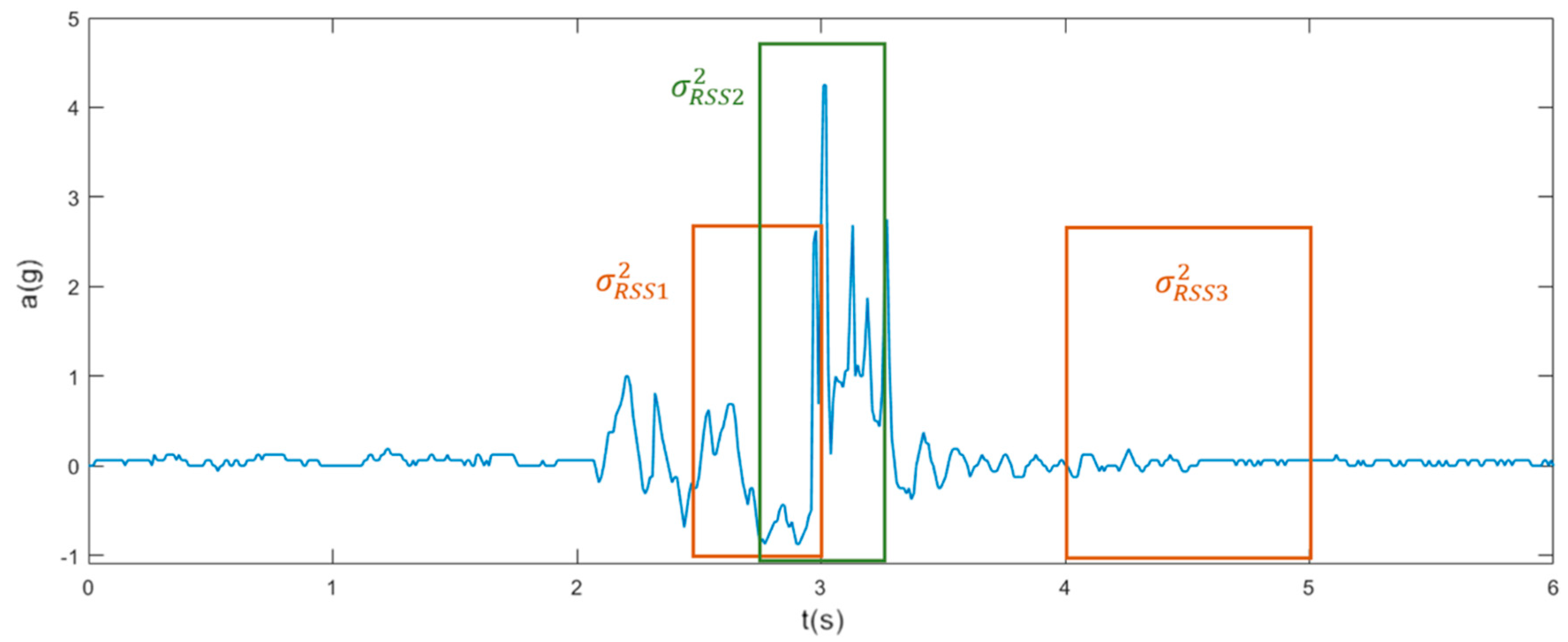
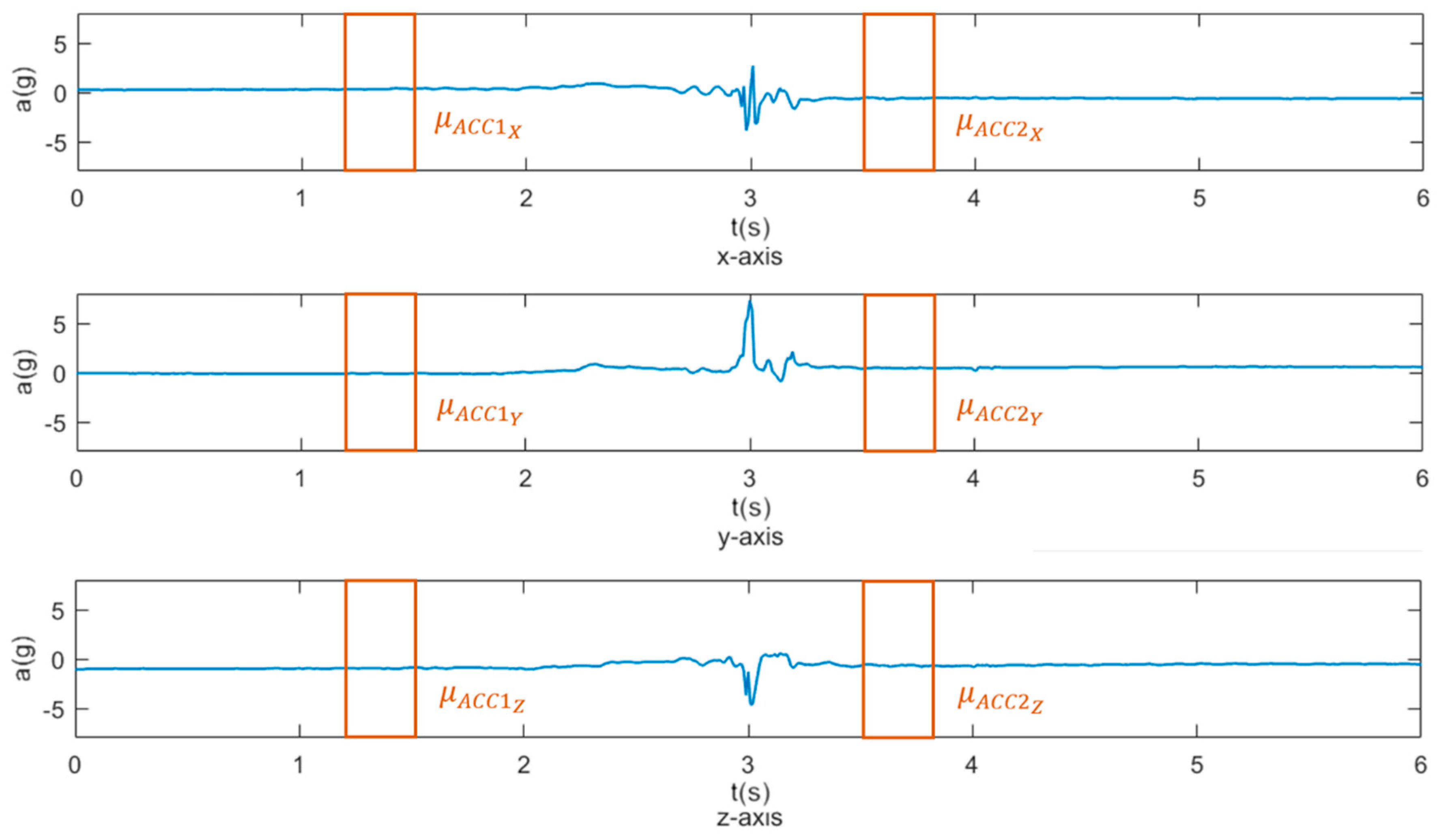
2.6. Feature Selection
2.7. Analysis
3. Results
3.1. Demographics and Data Collection
3.2. Features Extraction
3.3. Algorithms Comparisons
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lord, S.R.; Sherrington, C.; Menz, H.B.; Close, J.C.T. Falls in Older People: Risk Factors and Strategies for Prevention, 2nd ed.; Cambridge University Press: Cambridge, UK, 2007; pp. 1–395. [Google Scholar]
- Fuller, G.F. Falls in the elderly. Am. Fam. Phys. 2000, 61, 2159–2168, 2173–2174. [Google Scholar]
- Tinetti, M.E.; Liu, W.L.; Claus, E.B. Predictors and prognosis of inability to get up after falls among elderly persons. JAMA 1993, 269, 65–70. [Google Scholar] [CrossRef]
- Simpson, P.M.; Bendall, J.C.; Tiedemann, A.; Lord, S.R.; Close, J.C. Epidemiology of emergency medical service responses to older people who have fallen: A prospective cohort study. Prehosp. Emerg. Care 2014, 18, 185–194. [Google Scholar] [CrossRef] [PubMed]
- King, M.B.; Tinetti, M.E. Falls in community-dwelling older persons. J. Am. Geriatr. Soc. 1995, 43, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, W.J.; Green, M.F. Covert muscle injury in aged patients admitted to hospital following falls. Age Ageing 1985, 14, 174–178. [Google Scholar] [CrossRef]
- Roush, R.E.; Teasdale, T.A.; Murphy, J.N.; Kirk, M.S. Impact of a personal emergency response system on hospital utilization by community-residing elders. South Med. J. 1995, 88, 917–922. [Google Scholar] [CrossRef]
- Fleming, J.; Brayne, C. Inability to get up after falling, subsequent time on floor, and summoning help: Prospective cohort study in people over 90. BMJ 2008, 337, 1279–1282. [Google Scholar] [CrossRef]
- Vallabh, P.; Malekian, R. Fall detection monitoring systems: A comprehensive review. J. Ambient Intell. Humaniz. Comput. 2017, 9, 1809–1833. [Google Scholar] [CrossRef]
- Chaudhuri, S.; Thompson, H.; Demiris, G. Fall Detection Devices and their Use with Older Adults: A Systematic Review. J. Geriatr. Phys. Tehr. 2014, 37, 178–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwickert, L.; Becker, C.; Lindemann, U.; Maréchal, C.; Bourke, A.; Chiari, L. Sturzerkennung mit am Körper getragenen Sensoren: Ein systematischer Review. Z. Gerontol. Geriatr. 2013, 46, 706–719. [Google Scholar] [CrossRef]
- Bagala, F.; Becker, C.; Cappello, A.; Chiari, L.; Aminian, K.; Hausdorff, J.M.; Zijlstra, W.; Klenk, J. Evaluation of accelerometer-based fall detection algorithms on real-world falls. PLoS ONE 2012, 7, e37062. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.S.; Hoey, J. Review of fall detection techniques: A data availability perspective. Med. Eng. Phys. 2017, 39, 12–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skubic, M.; Harris, B.H.; Stone, E.; Ho, K.C.; Bo-Yu, S.; Rantz, M. Testing non-wearable fall detection methods in the homes of older adults. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 557–560. [Google Scholar]
- Bosch-Jorge, M.; Sánchez-Salmerón, A.J.; Valera, Á.; Ricolfe-Viala, C. Fall detection based on the gravity vector using a wide-angle camera. Expert Syst. Appl. 2014, 41, 7980–7986. [Google Scholar] [CrossRef] [Green Version]
- Kangas, M.; Korpelainen, R.; Vikman, I.; Nyberg, L.; Jamsa, T. Sensitivity and false alarm rate of a fall sensor in long-term fall detection in the elderly. Gerontology 2015, 61, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Lipsitz, L.A.; Tchalla, A.E.; Iloputaife, I.; Gagnon, M.; Dole, K.; Su, Z.Z.; Klickstein, L. Evaluation of an Automated Falls Detection Device in Nursing Home Residents. J. Am. Geriatr. Soc. 2016, 64, 365–368. [Google Scholar] [CrossRef]
- Bloch, F.; Gautier, V.; Noury, N.; Lundy, J.E.; Poujaud, J.; Claessens, Y.E.; Rigaud, A.S. Evaluation under real-life conditions of a stand-alone fall detector for the elderly subjects. Ann. Phys. Rehabil. Med. 2011, 54, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Bourke, A.K.; O’Brien, J.V.; Lyons, G.M. Evaluation of a threshold-based tri-axial accelerometer fall detection algorithm. Gait Posture 2007, 26, 194–199. [Google Scholar] [CrossRef]
- Kangas, M.; Konttila, A.; Winblad, I.; Jamsa, T. Determination of simple thresholds for accelerometry-based parameters for fall detection. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2007, 2007, 1367–1370. [Google Scholar] [PubMed]
- Noury, N.; Fleury, A.; Rumeau, P.; Bourke, A.K.; Laighin, G.O.; Rialle, V.; Lundy, J.E. Fall detection–principles and methods. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 1663–1666. [Google Scholar]
- Andò, B.; Baglio, S.; Lombardo, C.O.; Marletta, V. An Event Polarized Paradigm for ADL Detection in AAL Context. IEEE Trans. Instrum. Meas. 2015, 64, 1814–1825. [Google Scholar] [CrossRef]
- Luque, R.; Casilari, E.; Morón, M.J.; Redondo, G. Comparison and characterization of android-based fall detection systems. Sensors 2014, 14, 18543–18574. [Google Scholar] [CrossRef]
- Gibson, R.M.; Amira, A.; Ramzan, N.; Casaseca-De-La-Higuera, P.; Pervez, Z. Multiple comparator classifier framework for accelerometer-based fall detection and diagnostic. Appl. Soft Comput. J. 2016, 39, 94–103. [Google Scholar] [CrossRef]
- Jin, X.; Shao, J.; Zhang, X.; An, W.; Malekian, R. Modeling of nonlinear system based on deep learning framework. Nonlinear Dyn. 2016, 84, 1327–1340. [Google Scholar] [CrossRef]
- Albert, M.V.; Kording, K.; Herrmann, M.; Jayaraman, A. Fall classification by machine learning using mobile phones. PLoS ONE 2012, 7, e36556. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, A.T.; Barshan, B. Detecting falls with wearable sensors using machine learning techniques. Sensors 2014, 14, 10691–10708. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, F.; Scarpato, N.; Patrizia, F.; D’Ottavi, G.; Boavida, F.; Roselli, M.; Garrisi, G. Personal and Sensitive Data in the e-Health-IoT Universe. In Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering; Springer: Berlin, Germany, 2016; p. 170. [Google Scholar]
- Kangas, M.; Vikman, I.; Nyberg, L.; Korpelainen, R.; Lindblom, J.; Jämsä, T. Comparison of real-life accidental falls in older people with experimental falls in middle-aged test subjects. Gait Posture 2012, 35, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Klenk, J.; Becker, C.; Lieken, F.; Nicolai, S.; Maetzler, W.; Alt, W.; Zijlstra, W.; Hausdorff, J.M.; van Lummel, R.C.; Chiari, L.; et al. Comparison of acceleration signals of simulated and real-world backward falls. Med. Eng. Phys. 2011, 33, 368–373. [Google Scholar] [CrossRef]
- Broadley, R.W.; Klenk, J.; Thies, S.B.; Kenney, L.P.J.; Granat, M.H. Methods for the Real-World Evaluation of Fall Detection Technology: A Scoping Review. Sensors 2018, 18, 2060. [Google Scholar] [CrossRef]
- Rucco, R.; Sorriso, A.; Liparoti, M.; Ferraioli, G.; Sorrentino, P.; Ambrosanio, M.; Baselice, F. Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review. Sensors 2018, 18, 1613. [Google Scholar] [CrossRef]
- Thilo, F.J.; Bilger, S.; Halfens, R.J.; Schols, J.M.; Hahn, S. Involvement of the end user: Exploration of older people’s needs and preferences for a wearable fall detection device–A qualitative descriptive study. Patient Prefer. Adherence 2017, 11, 11–22. [Google Scholar] [CrossRef]
- Scarpato, N.; Pieroni, A.; Di Nunzio, L.; Fallucchi, F. E-health-IoT universe: A review. Int. J. Adv. Sci. Eng. Inf. Technol. 2017, 7, 2328–2336. [Google Scholar] [CrossRef]
- ST. LIS2DS12–MEMS Digital Output Motion Sensor: Ultra-Low-Power High-Performance 3-Axis “Pico” Accelerometer; ST2008; ST: Geneva, Switzerland, 2008; pp. 1–53. [Google Scholar]
- Microelectronic, E.M.; Sa, M. EM9209: High Sensitivity, 1.5–72 kbps, 2.4 GHz FSK Transceiver; EM Microelectronic-Marin SA: Marin-Epagnier, Switzerland, 2014; pp. 1–43. [Google Scholar]
- Micron. NAND Flash Memory: MT29F1G01ABBFDSF; Micron: Boise, ID, USA, 2007; pp. 1–118. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- O’Connell, B.; Myers, H. The sensitivity and specificity of the Morse Fall Scale in an acute care setting. J. Clin. Nurs. 2002, 11, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Schwendimann, R.; De Geest, S.; Milisen, K. Evaluation of the Morse Fall Scale in hospitalised patients. Age Ageing 2006, 35, 311–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lamb, S.E.; Jørstad-Stein, E.C.; Hauer, K.; Becker, C. Development of a common outcome data set for fall injury prevention trials: The Prevention of Falls Network Europe consensus. J. Am. Geriatr. Soc. 2005, 53, 1618–1622. [Google Scholar] [CrossRef]
- Yang, L.; Ren, Y.; Zhang, W. 3D depth image analysis for indoor fall detection of elderly people. Digit. Commun. Netw. 2016, 2, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.Y.; Liu, K.C.; Huang, C.N.; Chu, W.C.; Chan, C.T. Novel Hierarchical Fall Detection Algorithm Using a Multiphase Fall Model. Sensors 2017, 17, 307. [Google Scholar] [CrossRef] [PubMed]
- Bourke, A.K.; Lyons, G.M. A threshold-based fall-detection algorithm using a bi-axial gyroscope sensor. Med. Eng. Phys. 2008, 30, 84–90. [Google Scholar] [CrossRef]
- Lee, J.K.; Robinovitch, S.N.; Park, E.J. Inertial sensing-based pre-impact detection of falls involving near-fall scenarios. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 258–266. [Google Scholar] [CrossRef]
- Fortino, G.; Gravina, R. (Eds.) Fall-MobileGuard: A smart real-time fall detection system. In Proceedings of the BodyNets ‘15 the 10th EAI International Conference on Body Area Networks, Sydney, Australia, 28–30 September 2015. [Google Scholar]
- Bourke, A.K.; Klenk, J.; Schwickert, L.; Aminian, K.; Ihlen, E.A.F.; Mellone, S. Fall detection algorithms for real–world falls harvested from lumbar sensors in the elderly population: A machine learning approach. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3712–3715. [Google Scholar]
- Boyle, J.; Karunanithi, M. Simulated fall detection via accelerometers. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 1274–1277. [Google Scholar]
- Naranjo-Hernández, D.; Roa, L.M.; Reina-Tosina, J.; Estudillo-Valderrama, M.A. Personalization and adaptation to the medium and context in a fall detection system. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Preece, J. Best Fall Detection Sensors of 2019. Available online: https://www.toptenreviews.com/health/senior-care/best-fall-detection-sensors/ (accessed on 9 March 2019).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | First Phase | Second Phase |
|---|---|---|
| Number of participants | 11 * | 18 * |
| Gender (m/f) (% female) | 4/7 (64) | 6/12 (67) |
| Age (years) (mean ± SD) | 85.64 ± 7.81 | 87.50 ± 5.65 |
| Falls history 6 months before study (mean ± SD) | 11.45 ± 11.1 | 7.28 ± 8.87 |
| MoCA score (mean ± SD) | 10.64 ± 9.34 | 6.35 ± 7.52 |
| Katz score (mean ± SD) | 1.91 ± 1.38 | 2.11 ± 1.88 |
| Morse Fall Scale score (mean ± SD) | 80.45 ± 8.50 | 79.44 ± 9.22 |
| First Phase | Second Phase | |
|---|---|---|
| Study duration in days | 59 | 66 |
| Amount of data collected (one-minute slices) | 675,390 | 735,872 |
| Number of features used in algorithm | 3 | 15 |
| Real falls documented in event protocol | 18 | 23 |
| Sensor recorded falls | 11 | 20 |
| False alarms documented in event protocol | 29 | 12 |
| True Positive (correctly classified falls) | 3 | 16 |
| True Negative (correctly classified non-falls) | 675,350 | 735,840 |
| False Positive (wrongly classified non-falls) | 29 | 12 |
| False Negative (wrongly classified falls) | 8 | 4 |
| Sensitivity | 27.273% | 80.0% |
| Specificity | 99.995% | 99.998% |
| Accuracy | 99.994% | 99.997% |
| Precision | 9.375% | 57.143% |
| F-measure | 13.953% | 66.666% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheurer, S.; Koch, J.; Kucera, M.; Bryn, H.; Bärtschi, M.; Meerstetter, T.; Nef, T.; Urwyler, P. Optimization and Technical Validation of the AIDE-MOI Fall Detection Algorithm in a Real-Life Setting with Older Adults. Sensors 2019, 19, 1357. https://doi.org/10.3390/s19061357
Scheurer S, Koch J, Kucera M, Bryn H, Bärtschi M, Meerstetter T, Nef T, Urwyler P. Optimization and Technical Validation of the AIDE-MOI Fall Detection Algorithm in a Real-Life Setting with Older Adults. Sensors. 2019; 19(6):1357. https://doi.org/10.3390/s19061357
Chicago/Turabian StyleScheurer, Simon, Janina Koch, Martin Kucera, Hȧkon Bryn, Marcel Bärtschi, Tobias Meerstetter, Tobias Nef, and Prabitha Urwyler. 2019. "Optimization and Technical Validation of the AIDE-MOI Fall Detection Algorithm in a Real-Life Setting with Older Adults" Sensors 19, no. 6: 1357. https://doi.org/10.3390/s19061357
APA StyleScheurer, S., Koch, J., Kucera, M., Bryn, H., Bärtschi, M., Meerstetter, T., Nef, T., & Urwyler, P. (2019). Optimization and Technical Validation of the AIDE-MOI Fall Detection Algorithm in a Real-Life Setting with Older Adults. Sensors, 19(6), 1357. https://doi.org/10.3390/s19061357