Hybrid System of Emotion Evaluation in Physiotherapeutic Procedures

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Background
2.1. Psychological Assessment
2.2. Signal-Based Measures
3. Data Acquisitions
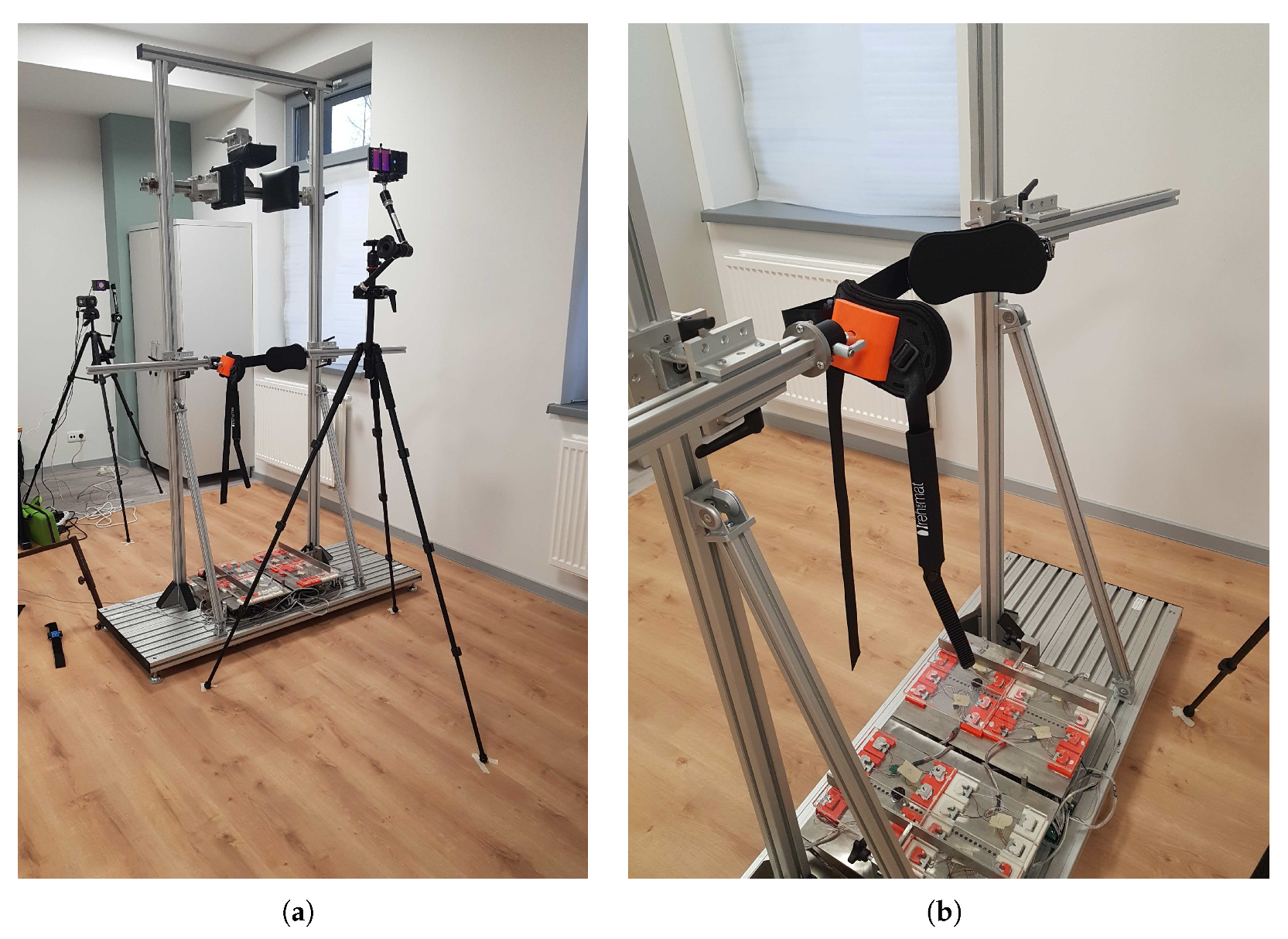
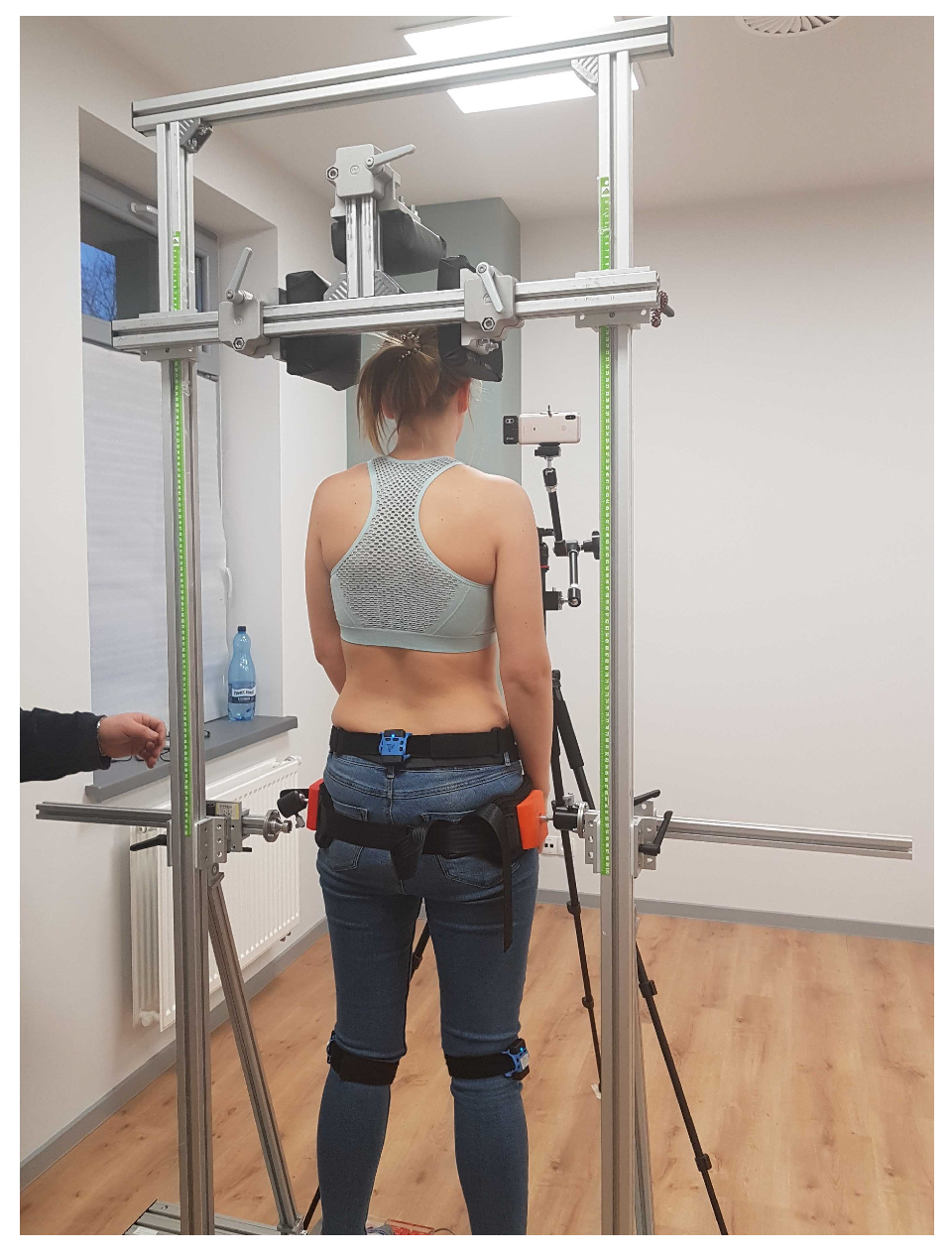
3.1. Setup
3.2. Research Protocol
- Age in the range 19–29 years (young adults),
- Be able to provide informed consent for the study,
- Without any dysfunction in auditory processing, significant visual impairment,
- Declaring physical activity in the various form of sports exercises,
- Lack of locomotor dysfunctions that may affect the measurements due to pain or limitations of mobility range,
- That he/she is not enduring psychiatric treatment and the crisis.
- Exercise number 1 consisted in performing consecutive anterior and posterior pelvic tilt for 60 s at the frequency of one sequence (anterior/posterior) per second,
- Exercise number 2—the participant was asked to perform the internal rotation of the feet with maximum force for 10 s, during the rotation, each foot was restricted by a beam on the outside,
- Exercise number 3 consisted in performing successively the external rotation of the feet, external rotation of the knees, pelvic anterior tilt, shoulder retraction, and spine elongation. In this position, the participant was asked to remain for 10 s.
4. Data Analysis
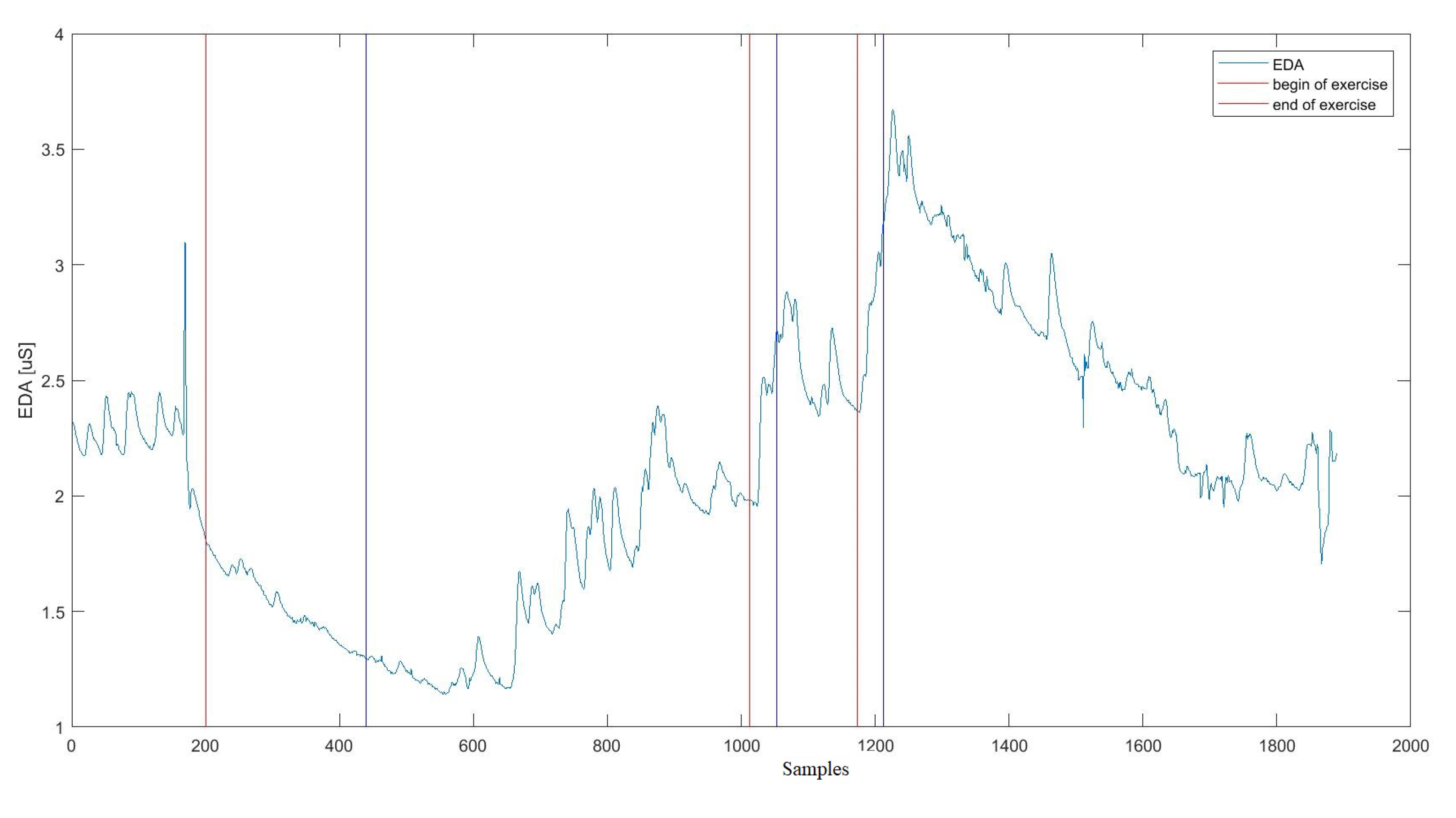
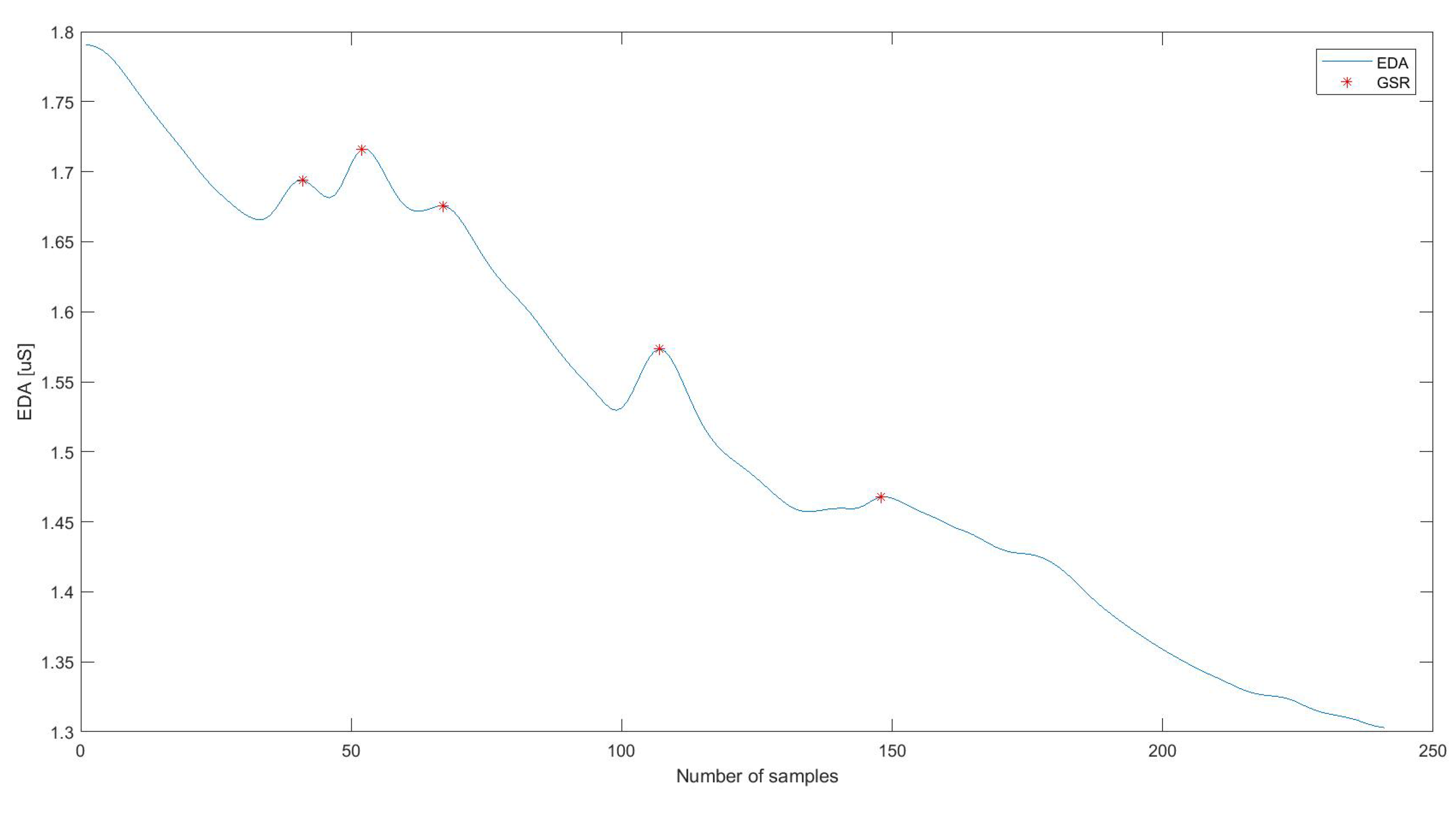
4.1. EDA Signal Preprocessing
4.2. Psychological Test Analysis
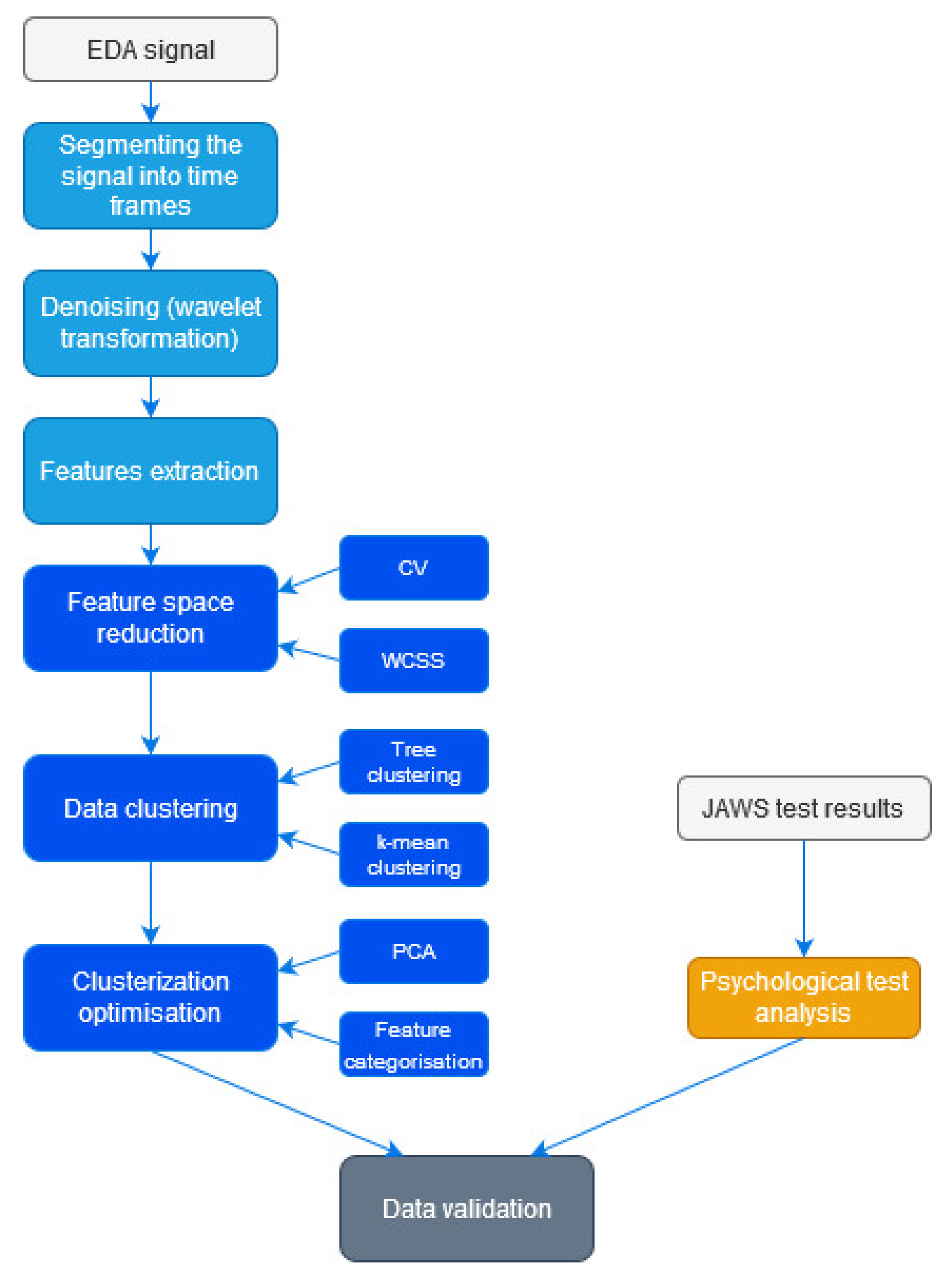
4.3. Data Classification
4.3.1. Features Reduction
- Exercise 1—standard deviation, coefficient of the slope of the regression line, number of GSRs, value of the total signal sum,
- Exercise 2—standard deviation, quartile deviation, coefficient of the slope of the regression line, GSR energy, minimum value of the signal, the 4th and 5th order moment, skewness, root of the mean square error, entropy,
- Exercise 3—standard deviation, quartile deviation, coefficient of the slope of the regression line, number and energy of GSR, a minimum value of the signal, 4th and 5th order moment, skewness, kurtosis, the root of the mean square error, entropy, and energy of signal.
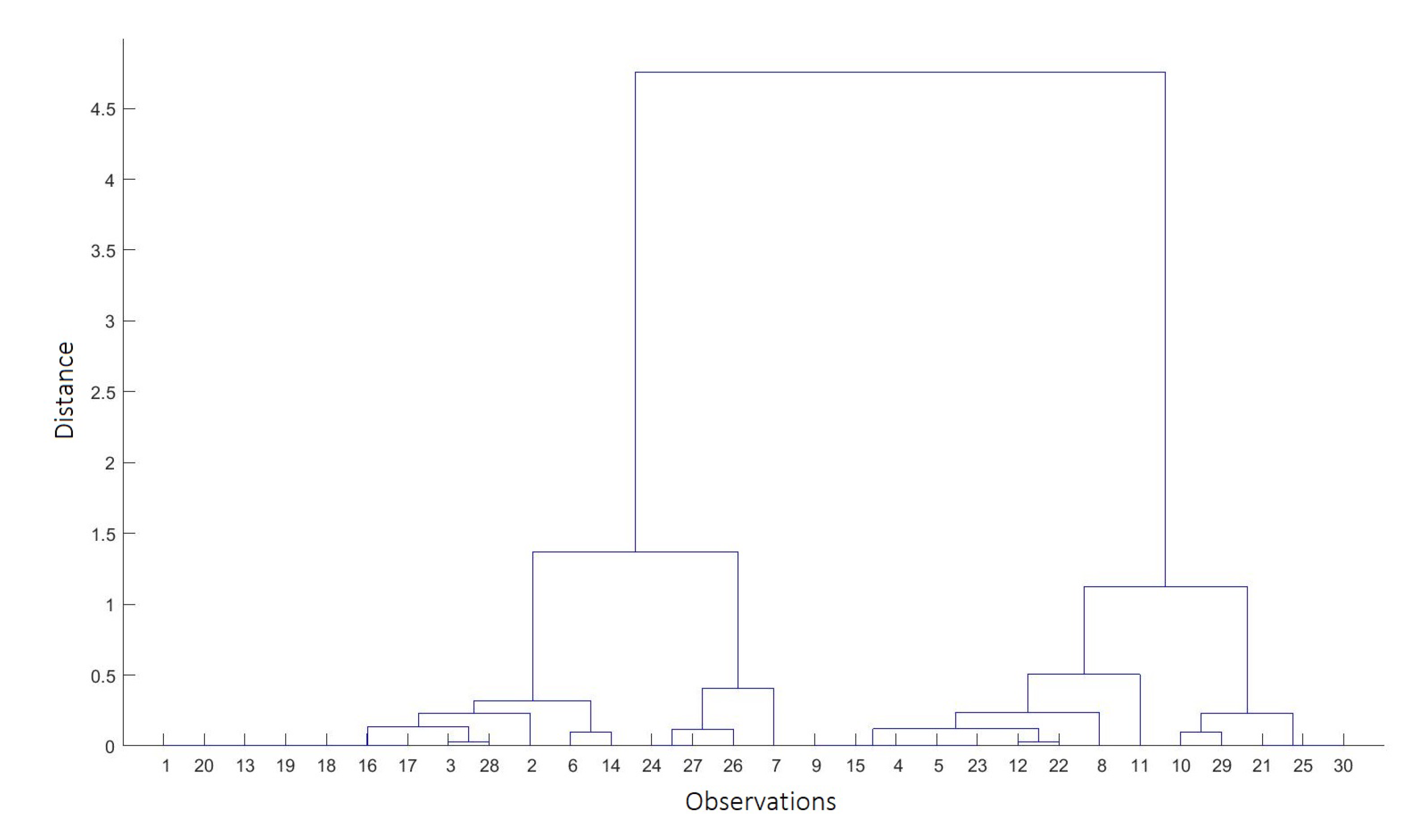
4.3.2. Data Clustering
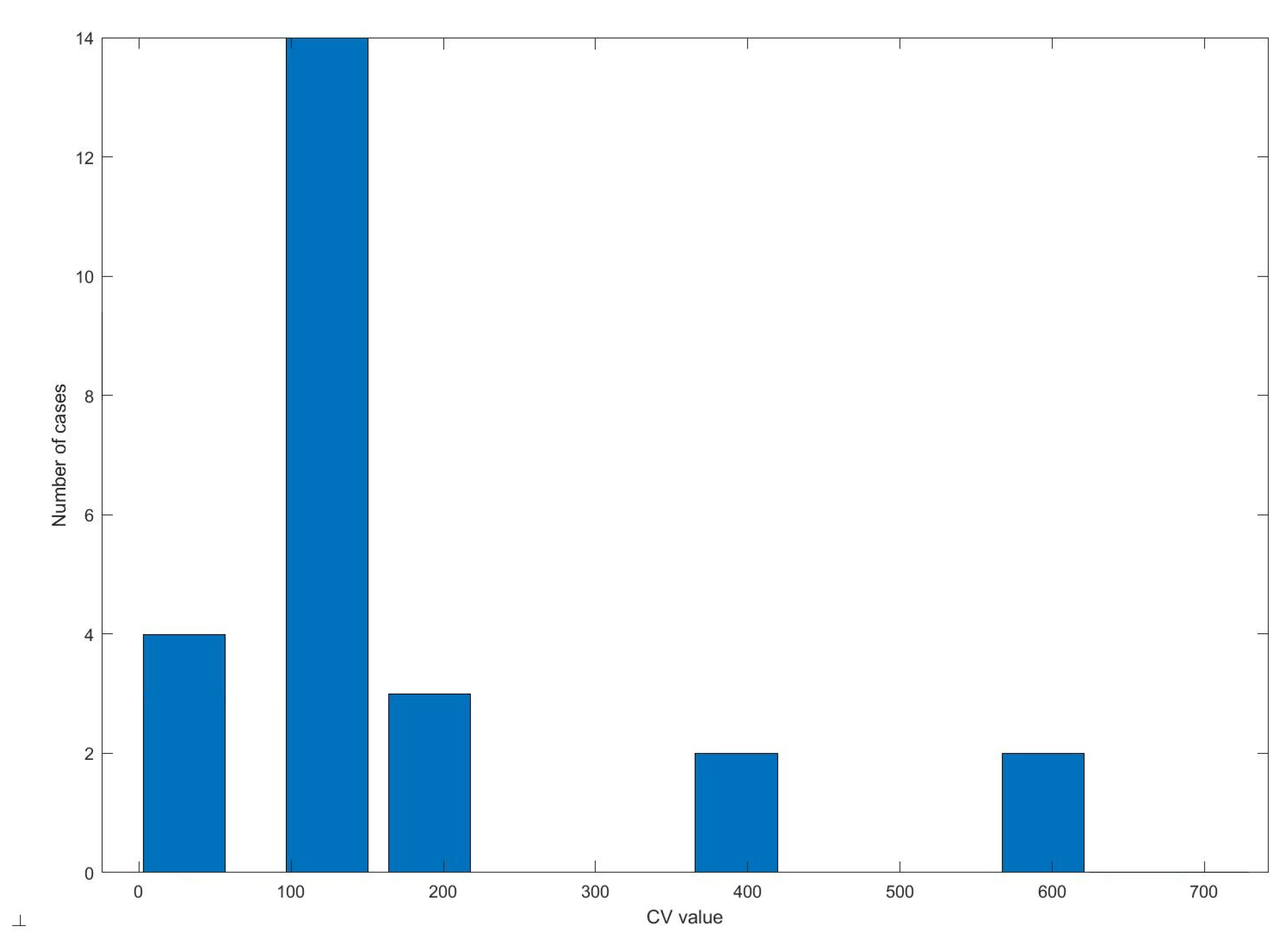
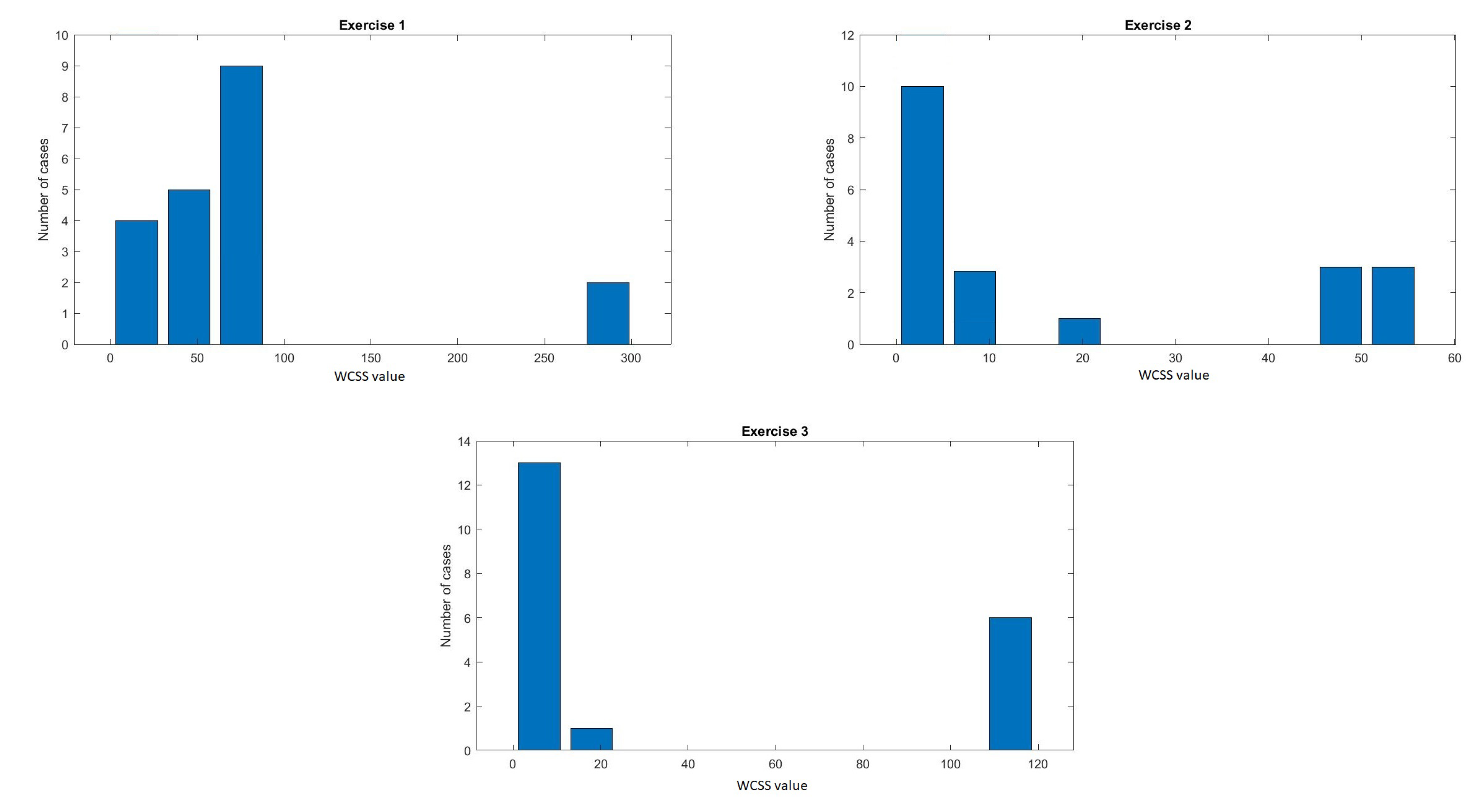
4.3.3. Clustering Optimisation
- Statistical set: standard deviation, quartile deviation, skewness, kurtosis, coefficient of the slope of the regression line,
- Signal set: number of GSRs, energy of GSR, minimum, total sum,
- Error set: 4th order moment, 5th order moment, rms, entropy.
4.4. Psychological Data Compliance
5. Results
5.1. Psychological Test
5.2. Data Classification
5.2.1. Feature Reduction
5.2.2. Clustering and Optimisation
5.3. Psychological Data Compliance
6. Discussion
7. Summary
Author Contributions
Funding

Conflicts of Interest
Ethical Statements
References
- Adam, K.; Peters, S.; Chipchase, L. Knowledge, skills and professional behaviours required by occupational therapist and physiotherapist beginning practitioners in work-related practice: A systematic review. Aust. Occup. Ther. J. 2013, 60, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Dyer, T.A.; Owens, J.; Robinson, P.G. The acceptability of healthcare: From satisfaction to trust. Community Dent. Health 2016, 33, 242–251. [Google Scholar] [PubMed]
- Jensen, M.P.; Turner, J.A.; Romano, J.M. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J. Consult. Clin. Psychol. 2001, 69, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984; pp. 150–153. [Google Scholar]
- Pinto, G.; Carvalho, J.M.; Barros, F.; Soares, S.C.; Pinho, A.J.; Brás, S. Multimodal Emotion Evaluation: A Physiological Model for Cost-Effective Emotion Classification. Sensors 2020, 20, 3510. [Google Scholar] [CrossRef]
- Salovey, P.; Rothman, A.J.; Detweiler, J.B.; Steward, W.T. Emotional states and physical health. Am. Psychol. 2000, 55, 110–121. [Google Scholar] [CrossRef]
- Folkman, S.; Moskowitz, J.T. Stress, positive emotion, and coping. Curr. Dir. Psychol. Sci. 2000, 9, 115–118. [Google Scholar] [CrossRef]
- Nourbakhsh, N.; Chen, F.; Wang, Y.; Calvo, R.A. Detecting users’ cognitive load by galvanic skin response with affective interference. ACM Trans. Interact. Intell. Syst. 2017, 7, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Folkman, S. Positive psychological states and coping with severe stress. Soc. Sci. Med. 1997, 45, 1207–1221. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; McGuire, L.; Robles, T.F.; Glaser, R. Emotions, morbidity, and mortality: New perspectives from psychoneuroimmunology. Annu. Rev. Psychol. 2002, 53, 83–107. [Google Scholar] [CrossRef] [Green Version]
- Epel, E.S.; McEwen, B.S.; Ickovics, J.R. Embodying psychological thriving: Physical thriving in response to stress. J. Soc. Issues 1998, 54, 301–322. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Mancuso, R.A.; Branigan, C.; Tugade, M.M. The undoing effect of positive emotions. Motiv. Emot. 2000, 24, 237–258. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Progress on a cognitive-motivational-relational theory of emotion. Am. Psychol. 1991, 46, 819. [Google Scholar] [CrossRef]
- Ito, T.A.; Larsen, J.T.; Smith, N.K.; Cacioppo, J.T. Negative information weighs more heavily on the brain: The negativity bias in evaluative categorizations. J. Personal. Soc. Psychol. 1998, 75, 887–900. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Losada, M.F. Positive affect and the complex dynamics of human flourishing. Am. Psychol. 2005, 60, 678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Yperen, N.W.; Hagedoorn, M. Do high job demands increase intrinsic motivation or fatigue or both? The role of job control and job social support. Acad. Manag. J. 2003, 46, 339–348. [Google Scholar]
- Ekman, P.; Levenson, R.W.; Friesen, W.V. Autonomic nervous system activity distinguishes among emotions. Science 1983, 221, 1208–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poh, M.Z.; Swenson, N.C.; Picard, R.W. A wearable sensor for unobtrusive, long-term assessment of electrodermal activity. IEEE Trans. Biomed. Eng. 2010, 57, 1243–1252. [Google Scholar] [PubMed] [Green Version]
- Brancaccio, G.; Russo, T. Anatomy and Physiology of Sweat Glands. In Hyperhidrosis; Springer: Cham, Switzerland, 2016; pp. 1–5. [Google Scholar]
- Asahina, M.; Suzuki, A.; Mori, M.; Kanesaka, T.; Hattori, T. Emotional sweating response in a patient with bilateral amygdala damage. Int. J. Psychophysiol. 2003, 47, 87–93. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in Electrodermal Activity Data Collection and Signal Processing: A Systematic Review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef] [Green Version]
- Visnovcova, Z.; Calkovska, A.; Tonhajzerova, I. Heart rate variability and electrodermal activity as noninvasive indices of sympathovagal balance in response to stress. Acta Medica Martiniana 2013, 13, 5–13. [Google Scholar] [CrossRef]
- Hovsepian, K.; Al’Absi, M.; Ertin, E.; Kamarck, T.; Nakajima, M.; Kumar, S. Stress: Towards a Gold Standard for Continuous Stress Assessment in the Mobile Environment. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Osaka, Japan, 7–11 September 2015; pp. 493–504. [Google Scholar]
- Sarker, H.; Tyburski, M.; Rahman, M.M.; Hovsepian, K.; Sharmin, M.; Epstein, D.H.; Preston, K.L.; Furr-Holden, C.D.; Milam, A.; Nahum-Shani, I.; et al. Finding Significant Stress Episodes in a Discontinuous Time Series of Rapidly Varying Mobile Sensor Data. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 4489–4501. [Google Scholar]
- Samadiani, N.; Huang, G.; Cai, B.; Luo, W.; Chi, C.H.; Xiang, Y.; He, J. A Review on Automatic Facial Expression Recognition Systems Assisted by Multimodal Sensor Data. Sensors 2019, 19, 1863. [Google Scholar] [CrossRef] [Green Version]
- Gjoreski, M.; Luštrek, M.; Gams, M.; Gjoreski, H. Monitoring stress with a wrist device using context. J. Biomed. Inform. 2017, 73, 159–170. [Google Scholar] [CrossRef]
- Kalimeri, K.; Saitis, C. Exploring multimodal biosignal features for stress detection during indoor mobility. In Proceedings of the 18th ACM International Conference on Multimodal Interaction, Tokyo Japan, 12–16 October 2016; pp. 53–60. [Google Scholar]
- Setz, C.; Arnrich, B.; Schumm, J.; La Marca, R.; Tröster, G.; Ehlert, U. Discriminating stress from cognitive load using a wearable EDA device. IEEE Trans. Inf. Technol. Biomed. 2009, 14, 410–417. [Google Scholar] [CrossRef]
- Shi, Y.; Ruiz, N.; Taib, R.; Choi, E.; Chen, F. Galvanic skin response (GSR) as an index of cognitive load. In CHI’07 Extended Abstracts on Human Factors in Computing Systemsm; Association for Computing Machinery: New York, NY, USA, 2007; pp. 2651–2656. [Google Scholar]
- Ikehara, C.S.; Crosby, M.E. Assessing cognitive load with physiological sensors. In Proceedings of the 38th Annual Hawaii International Conference on System Sciences, Big Island, HI, USA, 6 January 2005; p. 295a. [Google Scholar]
- Visnovcova, Z.; Bona Olexova, L.; Sekaninova, N.; Ondrejka, I.; Hrtanek, I.; Cesnekova, D.; Kelcikova, S.; Farsky, I.; Tonhajzerova, I. Spectral and Nonlinear Analysis of Electrodermal Activity in Adolescent Anorexia Nervosa. Appl. Sci. 2020, 10, 4514. [Google Scholar] [CrossRef]
- TaheriNejad, N.; Pollreisz, D. Assessment of physiological signals during happiness, sadness, pain or anger. In Proceedings of the International Conference on Wireless Mobile Communication and Healthcare, Milan, Italy, 14 November 2016; pp. 107–114. [Google Scholar]
- Liu, M.; Fan, D.; Zhang, X.; Gong, X. Human emotion recognition based on galvanic skin response signal feature selection and svm. In Proceedings of the 2016 International Conference on Smart City and Systems Engineering (ICSCSE), Hunan, China, 25–26 November 2016; pp. 157–160. [Google Scholar]
- Nakasone, A.; Prendinger, H.; Ishizuka, M. Emotion recognition from electromyography and skin conductance. In Proceedings of the 5th International Workshop on Biosignal Interpretation, Tokyo, Japan, 6–8 September 2005; pp. 219–222. [Google Scholar]
- Feng, H.; Golshan, H.M.; Mahoor, M.H. A wavelet-based approach to emotion classification using EDA signals. Expert Syst. Appl. 2018, 112, 77–86. [Google Scholar] [CrossRef]
- Szurmik, T.; Bibrowicz, K.; Lipowicz, A.; Mitas, A.W. Methods of Therapy of Scoliosis and Technical Functionalities of DISC4SPINE (D4S) Diagnostic and Therapeutic System. In Information Technology in Biomedicine; Springer: Cham, Switzerland, 2020; pp. 201–212. [Google Scholar]
- Bibrowicz, K.; Szurmik, T.; Lipowicz, A.; Mitas, A.W. Application of Original System to Support Specialist Physiotherapy D4S in Correction of Postural Defects as Compared to Other Methods—A Review. In Information Technology in Biomedicine; Springer: Cham, Switzerland, 2020; pp. 187–199. [Google Scholar]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Rigo, M.; Weiss, H.R. Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis 2006, 1, 4. [Google Scholar] [CrossRef] [Green Version]
- Romaniszyn, P.; Kania, D.; Bugdol, M.N.; Pollak, A.; Mitas, A.W. Behavioral and Physiological Profile Analysis While Exercising—Case Study. In Information Technology in Biomedicine; Springer: Cham, Switzerland, 2020; pp. 161–173. [Google Scholar]
- Mańka, A.; Romaniszyn, P.; Bugdol, M.N.; Mitas, A.W. Methods for Assessing the Subject’s Multidimensional Psychophysiological State in Terms of Proper Rehabilitation. In Information Technology in Biomedicine; Springer: Cham, Switzerland, 2020; pp. 213–225. [Google Scholar]
- E4 Wristband User’s Manual 20150608; Empatica: Milano, Italy, 2015; pp. 5–16. Available online: https://empatica.app.box.com/v/E4-User-Manual (accessed on 1 November 2020).
- Van Katwyk, P.T.; Fox, S.; Spector, P.E.; Kelloway, E.K. Using the Job-Related Affective Well-Being Scale (JAWS) to investigate affective responses to work stressors. J. Occup. Health Psychol. 2000, 5, 219–230. [Google Scholar] [CrossRef]
- McDonald Roderick, P. Test Theory: A Unified Treatment; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999. [Google Scholar]
- Hornowska, E. Testy psychologiczne. In Teoria i praktyka; Wydawnictwo Naukowe Scholar: Warszawa, PL, USA, 2009. [Google Scholar]
- Kreibig, S.D. Autonomic nervous system activity in emotion: A review. Biol. Psychol. 2010, 84, 394–421. [Google Scholar] [CrossRef]
- Storm, H. Changes in skin conductance as a tool to monitor nociceptive stimulation and pain. Curr. Opin. Anesthesiol. 2008, 21, 796–804. [Google Scholar] [CrossRef]
- Nourbakhsh, N.; Wang, Y.; Chen, F.; Calvo, R.A. Using galvanic skin response for cognitive load measurement in arithmetic and reading tasks. In Proceedings of the 24th Australian Computer-Human Interaction Conference, Melbourne, Australia, 26–30 November 2012; pp. 420–423. [Google Scholar]
- Ferdinando, H.; Alasaarela, E. Emotion recognition using cvxEDA-based features. J. Telecommun. Electron. Comput. Eng. 2018, 10, 19–23. [Google Scholar]
- Bianco, S.; Napoletano, P. Biometric Recognition Using Multimodal Physiological Signals. IEEE Access 2019, 7, 83581–83588. [Google Scholar] [CrossRef]
- Nielsen, O.M. Wavelets in Scientific Computing. Ph.D. Thesis, Technical University of Denmark, Lyngby, Denmark, 1998. [Google Scholar]
- Boucsein, W. Electrodermal Activity; Springer Science & Business Media: New York, NY, USA, 2012. [Google Scholar]
- Greco, A.; Valenza, G.; Lanata, A.; Scilingo, E.P.; Citi, L. cvxEDA: A convex optimization approach to electrodermal activity processing. IEEE Trans. Biomed. Eng. 2015, 63, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Job-Related Affective Well-Being Scale, JAWS. Available online: http://shell.cas.usf.edu/~pspector/scales/jawsscor.html (accessed on 1 November 2020).
- Odic, D.; Im, H.Y.; Eisinger, R.; Ly, R.; Halberda, J. PsiMLE: A maximum-likelihood estimation approach to estimating psychophysical scaling and variability more reliably, efficiently, and flexibly. Behav. Res. Methods 2016, 48, 445–462. [Google Scholar] [CrossRef]
- Duong, K.C.; Vrain, C. Constrained minimum sum of squares clustering by constraint programming. In Proceedings of the International Conference on Principles and Practice of Constraint Programming, Cork, Ireland, 4 September 2015; pp. 557–573. [Google Scholar]
- Day, W.H.; Edelsbrunner, H. Efficient algorithms for agglomerative hierarchical clustering methods. J. Classif. 1984, 1, 7–24. [Google Scholar] [CrossRef]
- Hartigan, J.A.; Wong, M.A. A K-means clustering algorithm. Applied Statistics. Appl. Stat. 1979, 28, 51. [Google Scholar] [CrossRef]
- Ku, W.; Storer, R.H.; Georgakis, C. Disturbance detection and isolation by dynamic principal component analysis. Chemom. Intell. Lab. Syst. 1995, 30, 179–196. [Google Scholar] [CrossRef]
- Schreiber, T. Measuring information transfer. Phys. Rev. Lett. 2000, 85, 461. [Google Scholar] [CrossRef] [Green Version]
- Trevethan, R. Sensitivity, specificity, and predictive values: Foundations, pliabilities, and pitfalls in research and practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Threshold | Range | Cluster 1 | Cluster 2 | |
|---|---|---|---|---|
| JAWS | 44.5 | 12–60 | Positive (n = 21) | Negative (m = 20) |
| JAWS_pos | 18.5 | 6–30 | Positive (n = 19) | Neutral (m = 22) |
| JAWS_neg | 10 | 6–30 | Negative (n = 15) | Neutral (m = 26) |
| Variable | JAWS | JAWS_poz | JAWS_neg |
|---|---|---|---|
| Mean | 44.39 | 18.29 | 9.90 |
| Standard deviation | 5.25 | 5.51 | 3.51 |
| Median | 45 | 18 | 9 |
| Min | 33 | 6 | 6 |
| Max | 57 | 27 | 21 |
| Possible range | 12–60 | 6–30 | 6-30 |
| Feature | Exercise 1 | Exercise 2 | Exercise 3 |
|---|---|---|---|
| Standard deviation | 0.232 | 0.103 | 0.102 |
| Quartile deviation | 0.341 | 0.184 | 0.167 |
| Coefficient of the slope of the regression line | 0.002 | 0.005 | 0.004 |
| Number of GSRs | 7.634 | 1.683 | 1.341 |
| Energy of GSR | 3.898 | 4.482 | 4.513 |
| Minimum value | 3.510 | 4.563 | 4.972 |
| 4th order moment | 1.348 | 0.044 | 0.047 |
| 5th order moment | 2.739 | 0.043 | |
| Skewness | 0.303 | 0.206 | 0.129 |
| Kurtosis | 3.256 | 4.707 | 5.109 |
| Root mean square | 3.885 | 4.707 | 5.109 |
| Entropy | 0.952 | 0.426 | 0.502 |
| Exercise 1 | Exercise 2 | Exercise 3 | ||||
|---|---|---|---|---|---|---|
| Classifier | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] |
| Cluster tree Euclidean | 51.22 | 60.98 | 39.02 | 60.98 | 39.02 | 60.98 |
| Cluster tree Spearman | 31.71 | 36.59 | 51.22 | 51.22 | 58.54 | 41.46 |
| Cluster tree Correlation | 19.51 | 36.59 | 21.95 | 36.59 | 48.29 | 48.78 |
| K-mean | 41.46 | 68.29 | 68.29 | 70.73 | 70.73 | 80.49 |
| Exercise 1 | Exercise 2 | Exercise 3 | ||||
|---|---|---|---|---|---|---|
| without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | |
| ACC | 41.46 | 68.29 | 68.29 | 70.73 | 70.73 | 80.49 |
| TPR | 80.00 | 96.29 | 88.89 | 70.83 | 70.83 | 80.64 |
| TNR | 12.50 | 14.29 | 35.71 | 64.71 | 73.33 | 80.00 |
| Exercise 3 + JAWS_pos | Exercise 3 + JAWS_neg | |||
|---|---|---|---|---|
| without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | |
| ACC | 60.98 | 78.05 | 60.98 | 80.49 |
| TPR | 75.00 | 92.00 | 78.95 | 95.45 |
| TNR | 30.77 | 56.25 | 45.45 | 63.13 |
| Feature Set | EDA+JAWS | EDA+JAWS_pos | EDA+JAWS_neg | ||||
|---|---|---|---|---|---|---|---|
| Coefficient | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | |
| set 1 | ACC | 63.41 | 73.17 | 53.65 | 78.05 | 46.34 | 68.29 |
| TPR | 78.26 | 91.67 | 57.14 | 84.62 | 48.00 | 91.30 | |
| TNR | 44.44 | 52.94 | 50.00 | 66.67 | 43.75 | 38.89 | |
| set 2 | ACC | 58.53 | 68.29 | 51.22 | 78.05 | 60.98 | 78.05 |
| TPR | 76.19 | 84 | 70.00 | 88.89 | 64.71 | 81.15 | |
| TNR | 31.58 | 43.75 | 45.16 | 68.56 | 58.33 | 71.43 | |
| set 3 | ACC | 78.05 | 85.37 | 58.54 | 68.29 | 78.05 | 85.37 |
| TPR | 96.30 | 95.45 | 66.67 | 77.78 | 91.30 | 88.46 | |
| TNR | 42.86 | 73.68 | 42.11 | 66.67 | 68.75 | 80.00 | |
| JAWS | JAWS_pos | JAWS_neg | ||||
|---|---|---|---|---|---|---|
| without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | without PCA [%] | with PCA [%] | |
| ACC | 65.85 | 73.17 | 60.98 | 73.17 | 63.41 | 78.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romaniszyn-Kania, P.; Pollak, A.; Danch-Wierzchowska, M.; Kania, D.; Myśliwiec, A.P.; Piętka, E.; Mitas, A.W. Hybrid System of Emotion Evaluation in Physiotherapeutic Procedures. Sensors 2020, 20, 6343. https://doi.org/10.3390/s20216343
Romaniszyn-Kania P, Pollak A, Danch-Wierzchowska M, Kania D, Myśliwiec AP, Piętka E, Mitas AW. Hybrid System of Emotion Evaluation in Physiotherapeutic Procedures. Sensors. 2020; 20(21):6343. https://doi.org/10.3390/s20216343
Chicago/Turabian StyleRomaniszyn-Kania, Patrycja, Anita Pollak, Marta Danch-Wierzchowska, Damian Kania, Andrzej P. Myśliwiec, Ewa Piętka, and Andrzej W. Mitas. 2020. "Hybrid System of Emotion Evaluation in Physiotherapeutic Procedures" Sensors 20, no. 21: 6343. https://doi.org/10.3390/s20216343