
Validation of a Low-Cost Electrocardiography (ECG) System for Psychophysiological Research


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.1.1. Hardware
2.1.2. Software
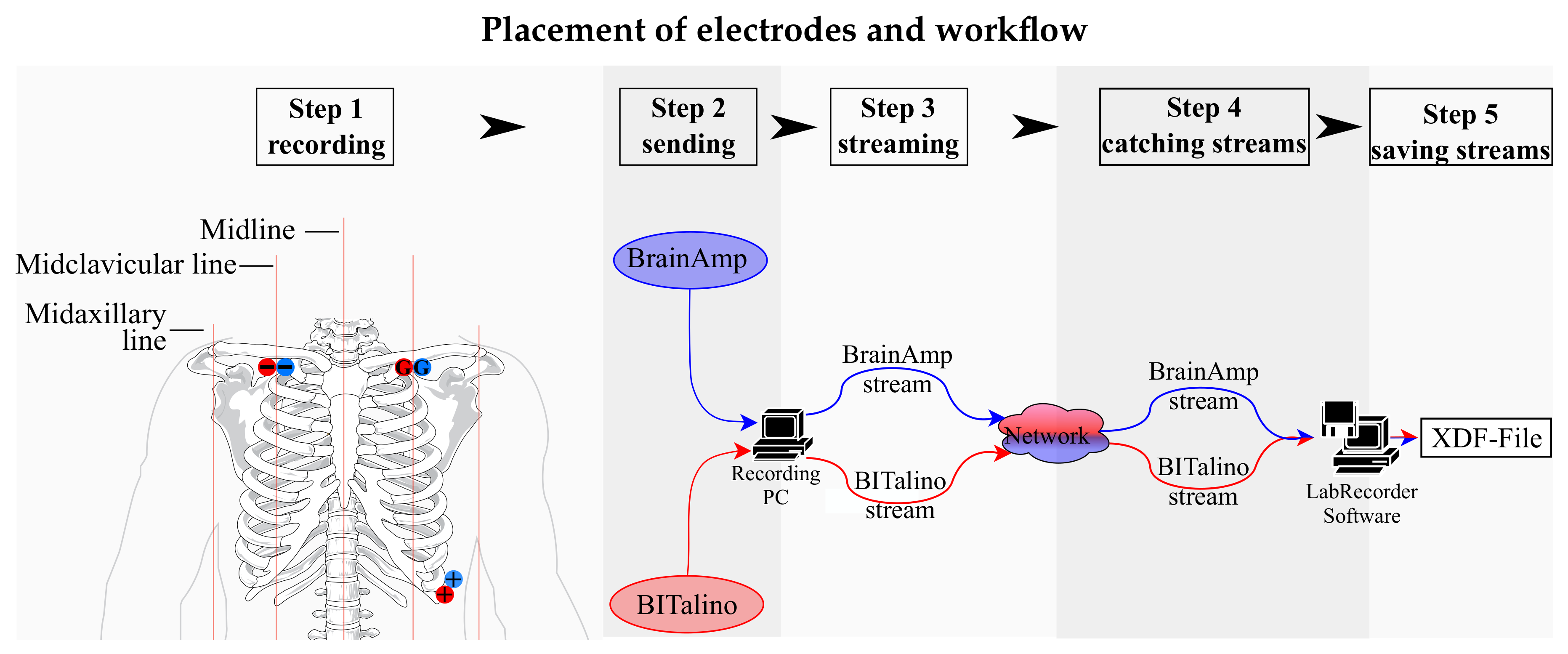
2.1.3. ECG Electrode Placement and Recording
2.2. Materials
Stimuli (IAPS)
2.3. Procedure
2.4. Data Analysis
2.4.1. Data Processing
2.4.2. Dependent Variables
3. Statistical Methods
3.1. Intraclass Correlation Coefficient (ICC)
3.2. Bland–Altman Limits of Agreement (Loa) Method
4. Results
4.1. Descriptive Results
4.2. ANOVA
4.3. Intraclass Correlation Coefficient
4.4. Bland–Altman Method
Visual Inspection of Bland–Altman Plots
5. Discussion
5.1. Overall ICC and Bland–Altman Method
5.2. ICC for Each Block
5.3. Conclusion of Method Comparison
5.4. Limitation of Comparison Methods in the Current Study
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACC | accelerometer |
| ANS | autonomic nervous system |
| API | application programming interface |
| BLE | Bluetooth Low Energy/Bluetooth 4.0 |
| Bpm/bpm | beats per minute |
| CI | confidence interval |
| DiY | do-it-yourself |
| ECG | electrocardiography |
| EDA | electrodermal activity |
| EEG | electroencephalography |
| EMG | electromyography |
| EOG | electrooculography |
| GSR | galvanic skin response |
| HF | High Frequency |
| HF(nu) | High Frequency normalized unit |
| HR | Heart Rate |
| HRV | heart rate variability |
| Hz | Hertz |
| IAPS | International Affective Picture System |
| ICC | Intraclass Correlation Coefficient |
| LF | Low Frequency |
| LF(nu) | Low Frequency normalized unit |
| LF/HF | ratio between low frequency and high frequency |
| LoA | Limits of Agreement |
| LSL | Lab Streaming Layer |
| LUX | photo transistor |
| MEG | magnetoencephalography |
| Q-Q plot | quantile-quantile plot |
| RMSSD | Root Mean Square of Successive Differences |
| SDNN | Standard deviation of the NN (R-R) intervals |
| USB | Universal Serial Bus |
| VLF | very low frequency |
| XDF | extensible data format |
References
- Jimenez-Molina, A.; Retamal, C.; Lira, H. Using psychophysiological sensors to assess mental workload during web browsing. Sensors 2018, 18, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzey, D.; Luz, M.; Mueller, S.; Dietz, A.; Meixensberger, J.; Strauss, G. Automation in surgery: The impact of navigated-control assistance on performance, workload, situation awareness, and acquisition of surgical skills. Hum. Factors 2011, 53, 584–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, H.P.; Fred, A.; Martins, R. Biosignals for Everyone. IEEE Pervasive Comput. 2014, 13, 64–71. [Google Scholar] [CrossRef]
- Carreiras, C.; Lourenço, A.; Silva, H.; Fred, A. Comparative Study of Medical-grade and Off-the-Person ECG Systems. In Proceedings of the International Congress on Cardiovascular Technologies—IWoPE (CARDIOTECHNIX), Vilamoura, Portugal, 20–21 September 2013; INSTICC, SciTePress: Setúbal, Portugal, 2013; pp. 115–120. [Google Scholar] [CrossRef]
- Ishaque, S.; Khan, N.; Krishnan, S. Trends in Heart-Rate Variability Signal Analysis. Front. Digit. Health 2021, 3, 13. [Google Scholar] [CrossRef]
- Baek, H.J.; Shin, J. Effect of missing inter-beat interval data on heart rate variability analysis using wrist-worn wearables. J. Med. Syst. 2017, 41, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Morelli, D.; Rossi, A.; Cairo, M.; Clifton, D.A. Analysis of the impact of interpolation methods of missing RR-intervals caused by motion artifacts on HRV features estimations. Sensors 2019, 19, 3163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, G.D.; Tarassenko, L. Quantifying errors in spectral estimates of HRV due to beat replacement and resampling. IEEE Trans. Biomed. Eng. 2005, 52, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. International Affective Picture System (IAPS): Affective Ratings of Pictures and Instruction Manual; Technical Report A-8; Technical Report; The Center for the Study of Emotion and Attention (CSEA): Gainesville, FL, USA, 2008. [Google Scholar]
- Bota, P.J.; Wang, C.; Fred, A.L.; Da Silva, H.P. A review, current challenges, and future possibilities on emotion recognition using machine learning and physiological signals. IEEE Access 2019, 7, 140990–141020. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.; Aggarwal, R. Common pitfalls in statistical analysis: Measures of agreement. Perspect. Clin. Res. 2017, 8, 187. [Google Scholar] [CrossRef]
- Team, M.I.C.T. BITalino Toolbox-File Exchange-MATLAB Central. 2018. Available online: https://ww2.mathworks.cn/matlabcentral/fileexchange/53983-bitalino-toolbox?requestedDomain=zh (accessed on 2 June 2021).
- Kothe, C.; Brunner, C. Extensible Data Format (XDF); Swartz Center for Computational Neuroscience (SCCN), University of California: San Diego, CA, USA, 2018. [Google Scholar]
- Brouwer, A.M.; van Wouwe, N.; Mühl, C.; van Erp, J.; Toet, A. Perceiving blocks of emotional pictures and sounds: Effects on physiological variables. Front. Hum. Neurosci. 2013, 7. [Google Scholar] [CrossRef] [Green Version]
- Greenwald, M.K.; Cook, E.W.; Lang, P.J. Affective judgment and psychophysiological response: Dimensional covariation in the evaluation of pictorial stimuli. J. Psychophysiol. 1989, 3, 51–64. [Google Scholar]
- Bradley, M.M.; Cuthbert, B.N.; Lang, P.J. Startle Reflex Modification: Emotion or Attention? Psychophysiology 1990, 27, 513–522. [Google Scholar] [CrossRef]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. Emotion, motivation, and anxiety: Brain mechanisms and psychophysiology. Biol. Psychiatry 1998, 44, 1248–1263. [Google Scholar] [CrossRef]
- Bradley, M.M.; Lang, P.J. Affective reactions to acoustic stimuli. Psychophysiology 2000, 37, 204–215. [Google Scholar] [CrossRef]
- Anttonen, J.; Surakka, V. Emotions and heart rate while sitting on a chair. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; ACM Press: Portland, OR, USA, 2005; pp. 491–499. [Google Scholar] [CrossRef] [Green Version]
- Codispoti, M.; De Cesarei, A. Arousal and attention: Picture size and emotional reactions. Psychophysiology 2007, 44, 680–686. [Google Scholar] [CrossRef]
- Sokhadze, E.M. Effects of Music on the Recovery of Autonomic and Electrocortical Activity After Stress Induced by Aversive Visual Stimuli. Appl. Psychophysiol. Biofeedback 2007, 32, 31–50. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and Others. Heart Rate Variability: Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Gramann, K.; Schandry, R. Psychophysiologie: Körperliche Indikatoren Psychischen Geschehens, 4th ed.; vollst. überarb. aufl, Ed.; Beltz PVU: Weinheim, Germany, 2009. [Google Scholar]
- Hare, R.; Wood, K.; Britain, S.; Shadman, J. Autonomic Responses to Affective Visual Stimulation. Psychophysiology 1970, 7, 408–417. [Google Scholar] [CrossRef]
- Libby, W.L.; Lacey, B.C.; Lacey, J.I. Pupillary and Cardiac Activity During Visual Attention. Psychophysiology 1973, 10, 270–294. [Google Scholar] [CrossRef]
- Winton, W.M.; Putnam, L.E.; Krauss, R.M. Facial and autonomic manifestations of the dimensional structure of emotion. J. Exp. Soc. Psychol. 1984, 20, 195–216. [Google Scholar] [CrossRef]
- Lang, P.J.; Greenwald, M.K.; Bradley, M.M.; Hamm, A.O. Looking at pictures: Affective, facial, visceral, and behavioral reactions. Psychophysiology 1993, 30, 261–273. [Google Scholar] [CrossRef]
- Müller, R.; Büttner, P. A critical discussion of intraclass correlation coefficients. Stat. Med. 1994, 13, 2465–2476. [Google Scholar] [CrossRef]
- Pinna, G.; Maestri, R.; Torunski, A.; Danilowicz-Szymanowicz, L.; Szwoch, M.; La Rovere, M.; Raczak, G. Heart rate variability measures: A fresh look at reliability. Clin. Sci. 2007, 113, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Lee, J.; Koh, D.; Ong, C.N. Statistical evaluation of agreement between two methods for measuring a quantitative variable. Comput. Biol. Med. 1989, 19, 61–70. [Google Scholar] [CrossRef]
- McGraw, K.O.; Wong, S.P. Forming inferences about some intraclass correlation coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. Statistician 1983, 32, 307. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Comparing Methods of Clinical Measurement-A Citation-Classic Commentary on Statistical-Methods for Assessing Agreement between 2 Methods of Clinical Measurment. Curr. Contents 1992, 40, 8. [Google Scholar]
- Ryan, T.P.; Woodall, W.H. The most-cited statistical papers. J. Appl. Stat. 2005, 32, 461–474. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Agreement Between Methods of Measurement with Multiple Observations Per Individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Weippert, M.; Kumar, M.; Kreuzfeld, S.; Arndt, D.; Rieger, A.; Stoll, R. Comparison of three mobile devices for measuring R-R intervals and heart rate variability: Polar S810i, Suunto t6 and an ambulatory ECG system. Eur. J. Appl. Physiol. 2010, 109, 779–786. [Google Scholar] [CrossRef]
- Sandercock, G.R.H.; Shelton, C.; Bromley, P.; Brodie, D.A. Agreement between three commercially available instruments for measuring short-term heart rate variability. Physiol. Meas. 2004, 25, 1115–1124. [Google Scholar] [CrossRef]
- Nunan, D.; Donovan, G.; Jakovljevic, D.G.; Hodges, L.D.; Sandercock, G.R.H.; Brodie, D.A. Validity and Reliability of Short-Term Heart-Rate Variability from the Polar S810. Med. Sci. Sport. Exerc. 2009, 41, 243–250. [Google Scholar] [CrossRef]
- Da Silva, H.P.; Carreiras, C.; Lourenço, A.; Fred, A.; das Neves, R.C.; Ferreira, R. Off-the-person electrocardiography: Performance assessment and clinical correlation. Health Technol. 2015, 4, 309–318. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BrainAmp | BITalino | |
|---|---|---|
| high-pass filter | 0.016 Hz * | 0.5 Hz |
| low-pass filter | 250 Hz | 40 Hz |
| sampling rate | 1000 Hz | 1000 Hz |
| HR Measures | HR | Heart Rate | [bpm] | |
|---|---|---|---|---|
| root mean | ||||
| time domain | RMSSD | square of | [ms] | |
| successive differences | ||||
| HRV measures | LF | low frequency | ||
| frequency domain | HF | high frequency | [ms] | |
| LF/HF | ratio between LF and HF |
| BITalino | BrainAmp | BITalino | BrainAmp | ||
|---|---|---|---|---|---|
| Mean | Mean | SD | SD | ||
| HR | |||||
| Fixation Cross | 73.065 | 73.025 | 10.190 | 10.205 | |
| Pleasant | 72.624 | 72.625 | 10.274 | 10.276 | |
| Unpleasant | 71.515 | 71.504 | 9.379 | 9.381 | |
| RMSSD | |||||
| Fixation Cross | 0.045 | 0.045 | 0.025 | 0.025 | |
| Pleasant | 0.043 | 0.043 | 0.025 | 0.025 | |
| Unpleasant | 0.044 | 0.044 | 0.023 | 0.022 | |
| ratio LF/HF | |||||
| Fixation Cross | 3.109 | 2.973 | 3.970 | 3.797 | |
| Pleasant | 2.993 | 2.988 | 4.220 | 4.204 | |
| Unpleasant | 3.081 | 3.078 | 4.889 | 4.875 | |
| Dependent Variable | Main Factor “Condition” | |
|---|---|---|
| HR | * | * |
| RMSSD | ||
| HRV LF | * | * |
| HRV HF | ||
| HRV LF/HF | * | * |
| Overall | B1 | B2 | B3 | B4 | B5 | B6 | B7 | |
|---|---|---|---|---|---|---|---|---|
| Fix 1 | P 1 | UP 1 | Fix 2 | P 2 | UP 2 | Fix 3 | ||
| HR | 100.0% | 100.0% | 100.0% | 100.0% | 99.9% | 100.0% | 100.0% | 100.0% |
| RMSSD | 99.6% | 99.9% | 100.0% | 100.0% | 97.4% | 99.8% | 100.0% | 100.0% |
| HRV LF | 100.0% | 100.0% | 100.0% | 100.0% | 99.9% | 100.0% | 100.0% | 100.0% |
| HRV HF | 99.6% | 99.9% | 99.8% | 100.0% | 97.3% | 99.9% | 100.0% | 99.9% |
| HRV LF/HF | 98.8% | 100.0% | 100.0% | 100.0% | 83.6% | 100.0% | 100.0% | 99.8% |
| Overall | B1 | B2 | B3 | B4 | B5 | B6 | B7 | |
|---|---|---|---|---|---|---|---|---|
| Fix 1 | P 1 | UP 1 | Fix 2 | P 2 | UP 2 | Fix 3 | ||
| HR | 100.0% | 100.0% | 100.0% | 100.0% | 99.8% | 100.0% | 100.0% | 100.0% |
| RMSSD | 99.4% | 99.8% | 100.0% | 100.0% | 94.0% | 99.6% | 100.0% | 99.8% |
| HRV LF | 99.9% | 99.9% | 100.0% | 100.0% | 99.8% | 100.0% | 100.0% | 100.0% |
| HRV HF | 99.4% | 99.8% | 100.0% | 100.0% | 93.8% | 99.7% | 100.0% | 99.9% |
| HRV LF/HF | 98.4% | 99.9% | 100.0% | 100.0% | 65.6% | 100.0% | 100.0% | 99.6% |
| LoA | |||||
|---|---|---|---|---|---|
| Measure | Bias | Lower LoA | - | Upper LoA | Outlier (in %) |
| HR | −0.01990803 | −0.33662671 | - | 0.29681066 | 4.83% |
| RMSSD | 0.00003761 | −0.00439510 | - | 0.00447032 | 3.22% |
| HRV LF | −0.00000880 | −0.00011612 | - | 0.00009852 | 4.83% |
| HRV HF | 0.00000290 | −0.00019657 | - | 0.00020236 | 4.83% |
| HRV LF/HF | −0.06054003 | −1.32977327 | - | 1.20869321 | 3.22% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, R.E.; Plácido da Silva, H.; Gramann, K. Validation of a Low-Cost Electrocardiography (ECG) System for Psychophysiological Research. Sensors 2021, 21, 4485. https://doi.org/10.3390/s21134485
Wagner RE, Plácido da Silva H, Gramann K. Validation of a Low-Cost Electrocardiography (ECG) System for Psychophysiological Research. Sensors. 2021; 21(13):4485. https://doi.org/10.3390/s21134485
Chicago/Turabian StyleWagner, Ruth Erna, Hugo Plácido da Silva, and Klaus Gramann. 2021. "Validation of a Low-Cost Electrocardiography (ECG) System for Psychophysiological Research" Sensors 21, no. 13: 4485. https://doi.org/10.3390/s21134485