
A Low-Cost, Point-of-Care Test for Confirmation of Nasogastric Tube Placement via Magnetic Field Tracking


Abstract
:1. Introduction
2. Materials and Methods
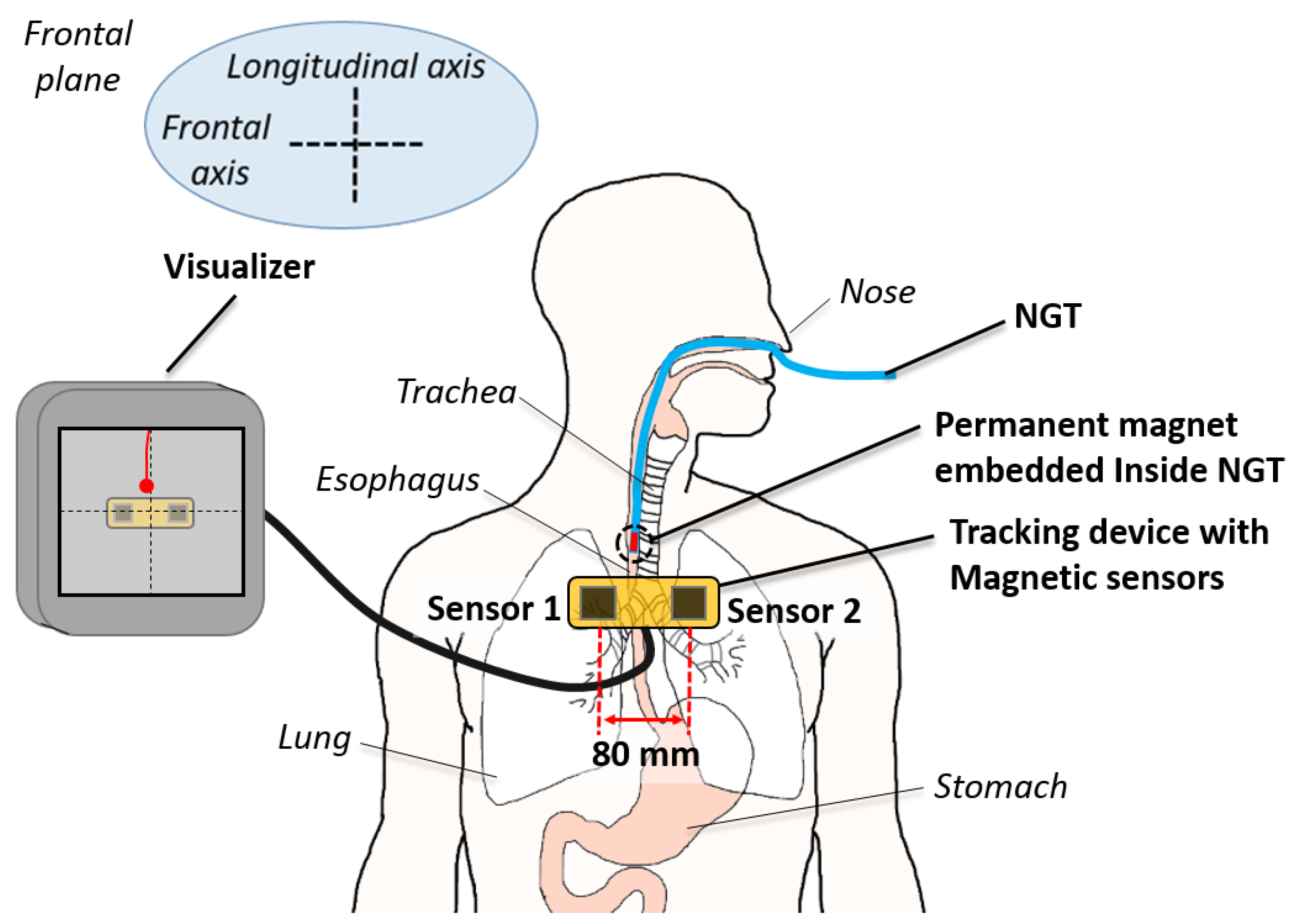
2.1. Two-Sensor Setup
2.2. Tracking Algorithm
2.2.1. Precalculation of Magnetic Field
2.2.2. Search Range
- : This region is used until the first estimation is provided. The target magnet will be out of the sensor’s sensible range at the beginning of the NGT insertion. As the insertion progresses, the tip of the tube will enter the search range always from the top. Therefore, we need to focus only on the top slice of the entire search range. Since the insertion speed and the anatomy or tilt angle of the esophagus and trachea are limited, the search ranges can be constrained as follows:where is the top end of the z search range, is the possible maximum speed of tube insertion, is the time step in between the iterations, is the first estimation of z position, and is the possible maximum pitch angle of the tube tip inside the esophagus and trachea.
- : This region covers from the first estimated z position to the level of the carina or end of the trachea. The search ranges are constrained based on the current position, orientation, speed of the tube tip and the possible tilt angle of the tube tip inside the esophagus and the trachea.where and are the estimated z position and pitch angle at the kth iteration. is the z position of the carina. and are the uncertainties from the estimation errors. is the possible pitch rotation during one computational iteration inside the esophagus and trachea.
- : This region covers from the end of region 1 to the bottom end of the search range. The tube tip could be inside the trachea, bronchi, esophagus, or stomach. Therefore, any pitch angle is possible.where is the bottom end of z search range and the possible pitch rotation during one computational iteration inside the trachea, bronchi, esophagus and stomach.
2.2.3. Threshold Modulation
2.3. Experimental Setup
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EG | Esophagogastric |
| EM | Electromagnetic |
| EMS-EAS | Electromagnetic sensor guided enteral access system |
| GI | Gastrointestinal |
| MIBC | Magnetically inflated balloon capsule |
| NGT | Nasogastric tube |
| PD | Proportional-Derivative |
| PM | Permanent magnet |
| SD | Standard deviation |
References
- Hodin, R.A.; Bordeianou, L. Inpatient Placement and Management of Nasogastric and Nasoenteric tubes in Adults; UpToDate Inc.: Waltham, MA, USA, 2019. [Google Scholar]
- Smithard, D.; Barrett, N.A.; Hargroves, D.; Elliot, S. Electromagnetic sensor-guided enteral access systems: A literature review. Dysphagia 2015, 30, 275–285. [Google Scholar] [CrossRef] [Green Version]
- Stayner, J.L.; Bhatnagar, A.; McGinn, A.N.; Fang, J.C. Feeding tube placement: Errors and complications. Nutr. Clin. Pract. 2012, 27, 738–748. [Google Scholar] [CrossRef]
- Metheny, N.A.; Meert, K.L.; Clouse, R.E. Complications related to feeding tube placement. Curr. Opin. Gastroenterol. 2007, 23, 178–182. [Google Scholar] [CrossRef]
- Agency, N.P.S. Patient Safety Alert NPSA/2011/PSA002: Reducing the harm caused by misplaced nasogastric feeding tubes in adults, children and infants. Support. Inf. 2011. Available online: http://www.gbukenteral.com/pdf/NPSA-Alert-2011.pdf (accessed on 29 June 2021).
- Peter, S.; Gill, F. Development of a clinical practice guideline for testing nasogastric tube placement. J. Spec. Pediatr. Nurs. 2009, 14, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Allan, K.; McWilliam, H.; Manara, A.; Brown, J.; Toher, D.; Rayner, W. Confirming nasogastric tube position with electromagnetic tracking versus pH or X-ray and tube radio-opacity. Br. J. Nurs. 2014, 23, 352–358. [Google Scholar] [CrossRef]
- Ackerman, M.; Mick, D.; Bianchi, C.; Chiodo, V.; Yeager, C. The Effectiveness of the CORTRAK™ Device in Avoiding Lung Placement of Small Bore Enteral Feeding Tubes. Am. J. Crit. Care 2004, 13, 253–276. [Google Scholar]
- NICE. CORTRAK 2 Enteral Access System for Placing Nasoenteral Feeding Tubes. 2016. Available online: https://www.nice.org.uk/advice/mib48/resources/cortrak-2-enteral-access-system-for-placing-nasoenteral-feeding-tubes-pdf-63499172779717 (accessed on 21 April 2021).
- Pham, D.; Aziz, S.M. A real-time localization system for an endoscopic capsule using magnetic sensors. Sensors 2014, 14, 20910–20929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.; Li, B.; Qiao, W.; Hu, C.; Ren, H.; Yu, H.; Zhang, Q.; Meng, M.Q.H.; Xu, G. 6-D magnetic localization and orientation method for an annular magnet based on a closed-form analytical model. IEEE Trans. Magn. 2014, 50, 1–11. [Google Scholar] [CrossRef]
- Dai, H.; Yang, W.; Xia, X.; Su, S.; Ma, K. A three-axis magnetic sensor array system for permanent magnet tracking. In Proceedings of the 2016 IEEE International Conference on Multisensor Fusion and Integration for Intelligent Systems (MFI), Baden-Baden, Germany, 19–21 September 2016; pp. 476–480. [Google Scholar]
- Hu, C.; Ren, Y.; You, X.; Yang, W.; Song, S.; Xiang, S.; He, X.; Zhang, Z.; Meng, M.Q.H. Locating intra-body capsule object by three-magnet sensing system. IEEE Sens. J. 2016, 16, 5167–5176. [Google Scholar] [CrossRef]
- Wu, X.; Hou, W.; Peng, C.; Zheng, X.; Fang, X.; He, J. Wearable magnetic locating and tracking system for MEMS medical capsule. Sens. Act. A Phys. 2008, 141, 432–439. [Google Scholar] [CrossRef]
- Sun, Z.; Foong, S.; Maréchal, L.; Tan, U.X.; Teo, T.H.; Shabbir, A. A non-invasive real-time localization system for enhanced efficacy in nasogastric intubation. Ann. Biomed. Eng. 2015, 43, 2941–2952. [Google Scholar] [CrossRef]
- Burdett, E.; Mitchell, V. Anatomy of the larynx, trachea and bronchi. Anaesth. Intensive Care Med. 2011, 12, 335–339. [Google Scholar] [CrossRef]
- Miyasaka, M.; Tiong, A.M.H.; Phan, P.T.; Huang, Y.; Kaan, H.L.; Ho, K.Y.; Phee, S.J. Two Magnetic Sensor Based Real-Time Tracking of Magnetically Inflated Swallowable Intragastric Balloon. Ann. Biomed. Eng. 2021, 1–12. [Google Scholar] [CrossRef]
- Bleys, R.L.; Weijs, T.J. Surgical anatomy of esophagus. In Minimally Invasive Surgery for Upper Abdominal Cancer; Springer: Berlin/Heidelberg, Germany, 2017; pp. 11–20. [Google Scholar]
- Jaeger, J.M.; Titus, B.J.; Blank, R.S. Essential anatomy and physiology of the respiratory system and the pulmonary circulation. In Principles and Practice of Anesthesia for Thoracic Surgery; Springer: Berlin/Heidelberg, Germany, 2019; pp. 65–92. [Google Scholar]
- Ball, M.; Falkson, S.R.; Adigun, O.O. Anatomy, angle of Louis 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459336/ (accessed on 29 June 2021).
- Mi, W.; Zhang, C.; Wang, H.; Cao, J.; Li, C.; Yang, L.; Guo, F.; Wang, X.; Yang, T. Measurement and analysis of the tracheobronchial tree in Chinese population using computed tomography. PLoS ONE 2015, 10, e0123177. [Google Scholar] [CrossRef] [Green Version]
- García, H.F.; Valencia Orgaz, O.; López Vicente, R.; Gutiérrez Vidal, S.E. Airway anatomy for the bronchoscopist: An anesthesia approach. Rev. Colomb. Anestesiol. 2014, 42, 192–198. [Google Scholar] [CrossRef]
- Seneterre, E.; Paganin, F.; Bruel, J.; Michel, F.; Bousquet, J. Measurement of the internal size of bronchi using high resolution computed tomography (HRCT). Eur. Respir. J. 1994, 7, 596–600. [Google Scholar] [CrossRef]
- Sehgal, I.S.; Dhooria, S.; Ram, B.; Singh, N.; Aggarwal, A.N.; Gupta, D.; Behera, D.; Agarwal, R. Foreign body inhalation in the adult population: Experience of 25,998 bronchoscopies and systematic review of the literature. Respir. Care 2015, 60, 1438–1448. [Google Scholar] [CrossRef]
- Bellemare, F.; Jeanneret, A.; Couture, J. Sex differences in thoracic dimensions and configuration. Am. J. Respir. Crit. Care Med. 2003, 168, 305–312. [Google Scholar] [CrossRef]
- Chubar, O.; Elleaume, P.; Chavanne, J. A 3D Magnetostatics Computer Code For Insertion Devices, SRI97 Conf. Aug. 1997. J. Synchrotron Rad 1998, 5, 481–484. [Google Scholar] [CrossRef]
- Elleaume, P.; Chubar, O.; Chavanne, J. Computing 3D magnetic fields from insertion devices. In Proceedings of the 1997 Particle Accelerator Conference (Cat. No. 97CH36167), Baden-Baden, Germany, 19–21 September 2016; Volume 3, pp. 3509–3511. [Google Scholar]
- Berkelman, P.; Bozlee, S.; Miyasaka, M. Interactive rigid-body dynamics and deformable surface simulations with co-located maglev haptic and 3D graphic display. Int. J. Adv. Intell. Syst. 2013, 6, 289–299. [Google Scholar]
- Berkelman, P.; Miyasaka, M.; Anderson, J. Co-located 3D graphic and haptic display using electromagnetic levitation. In Proceedings of the 2012 IEEE Haptics Symposium (HAPTICS), Vancouver, BC, Canada, 4–7 March 2012; pp. 77–81. [Google Scholar]
- Berkelman, P.; Bozlee, S.; Miyasaka, M. Interactive dynamic simulations with co-located maglev haptic and 3d graphic display. In Proceedings of the International Conference Advances in Computer-Human Interactions, Nice, France, 24 February–1 March 2013; pp. 324–329. [Google Scholar]
- Miyasaka, M.; Berkelman, P. Magnetic levitation with unlimited omnidirectional rotation range. Mechatronics 2014, 24, 252–264. [Google Scholar] [CrossRef]
- Ferhatoglu, M.F.; Kıvılcım, T. Anatomy of esophagus. In Esophageal Abnormalities; IntechOpen: London, UK, 2017. [Google Scholar] [CrossRef] [Green Version]
- Breatnach, E.; Abbott, G.C.; Fraser, R.G. Dimensions of the normal human trachea. Am. J. Roentgenol. 1984, 142, 903–906. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Son, J.S.; Choi, J.W.; Han, Y.J.; Lee, J.R. The comparison of the lengths and diameters of main bronchi measured from two-dimensional and three-dimensional images in the same patients. Korean J. Anesthesiol. 2014, 66, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, M.; Kallam, R.; Flindall, I.; Gatt, M.; Macfie, J. Use of Cortrak®—An electromagnetic sensing device in placement of enteral feeding tubes. Proc. Nutr. Soc. 2008, 67. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.J.; Allan, K.; McWilliam, H.; Toher, D. Nasogastric tube depth: The ‘NEX’guideline is incorrect. Br. J. Nurs. 2014, 23, 641–644. [Google Scholar] [CrossRef] [Green Version]
- Williamson, S.J.; Kaufman, L. Biomagnetism. J. Magn. Magn. Mater. 1981, 22, 129–201. [Google Scholar] [CrossRef]
- Kaan, H.L.; Phan, P.T.; Tiong, A.M.H.; Miyasaka, M.; Phee, S.J.; Ho, K.Y. First-in-man feasibility study of a novel ingestible magnetically inflated balloon capsule for treatment of obesity. Endosc. Int. Open 2020, 8, E607. [Google Scholar] [CrossRef] [Green Version]
- Phan, P.T.; Tiong, A.M.H.; Miyasaka, M.; Cao, L.; Kaan, H.L.; Ho, K.Y.; Phee, S.J. EndoPil: A magnetically actuated swallowable capsule for weight management: Development and trials. Ann. Biomed. Eng. 2020, 49, 1–11. [Google Scholar]
- Mateen, H.; Basar, R.; Ahmed, A.U.; Ahmad, M.Y. Localization of wireless capsule endoscope: A systematic review. IEEE Sens. J. 2017, 17, 1197–1206. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| 0 mm | |
| 250 mm | |
| 100 mm | |
| 80 mm | |
| 100 mm/s | |
| 10 mm | |
| 0 | 120 |
| (0, 20] | 100 |
| (20, 80] | 70 |
| (80, 120] | 80 |
| (120, 180] | 40 |
| (180, 220] | 80 |
| (220, 290] | 90 |
| greater than 290 | 100 |
| Condition | x, y, z, and | |
|---|---|---|
| Components | Component | |
| 0 ≤ < 2.5 | 0.4 | 0.8 |
| or < 100 | 1.25 | 2.5 |
| and < 500 | 1 | 2 |
| 500 < | 0.5 | 1 |
| 100 < ≤ 500 | 0.75 | 1.5 |
| 50 < ≤ 100 | 1 | 2 |
| 0 < ≤ 50 | 1.75 | 3.5 |
| = 0 | 2.5 | 5 |
| y | z | y | z | ||
|---|---|---|---|---|---|
| [mm] | [mm] | [mm] | [mm] | ||
| (Excluding z = 250 mm) | |||||
| L [mm] | 80 | 2.60 | 3.55 | 2.47 | 1.44 |
| 100 | 2.83 | 5.50 | 2.62 | 1.84 | |
| Proposed | Ref [15] | |
|---|---|---|
| # of sensors | 2 | 11 |
| Volume [mm3] | 100 × 120 × 250 | 100 × 100 × 200 |
| Magnet size [mm] | 3.2 × L9.6 | 3.2 × L9.6 |
| RMSE in 1D [mm] | 2.60 − 5.50 | 0.92 − 4.05 |
| (1.44 − 2.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyasaka, M.; Li, H.; Tay, K.V.; Phee, S.J. A Low-Cost, Point-of-Care Test for Confirmation of Nasogastric Tube Placement via Magnetic Field Tracking. Sensors 2021, 21, 4491. https://doi.org/10.3390/s21134491
Miyasaka M, Li H, Tay KV, Phee SJ. A Low-Cost, Point-of-Care Test for Confirmation of Nasogastric Tube Placement via Magnetic Field Tracking. Sensors. 2021; 21(13):4491. https://doi.org/10.3390/s21134491
Chicago/Turabian StyleMiyasaka, Muneaki, Hao Li, Kon Voi Tay, and Soo Jay Phee. 2021. "A Low-Cost, Point-of-Care Test for Confirmation of Nasogastric Tube Placement via Magnetic Field Tracking" Sensors 21, no. 13: 4491. https://doi.org/10.3390/s21134491
APA StyleMiyasaka, M., Li, H., Tay, K. V., & Phee, S. J. (2021). A Low-Cost, Point-of-Care Test for Confirmation of Nasogastric Tube Placement via Magnetic Field Tracking. Sensors, 21(13), 4491. https://doi.org/10.3390/s21134491