
Kinocardiography Derived from Ballistocardiography and Seismocardiography Shows High Repeatability in Healthy Subjects

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
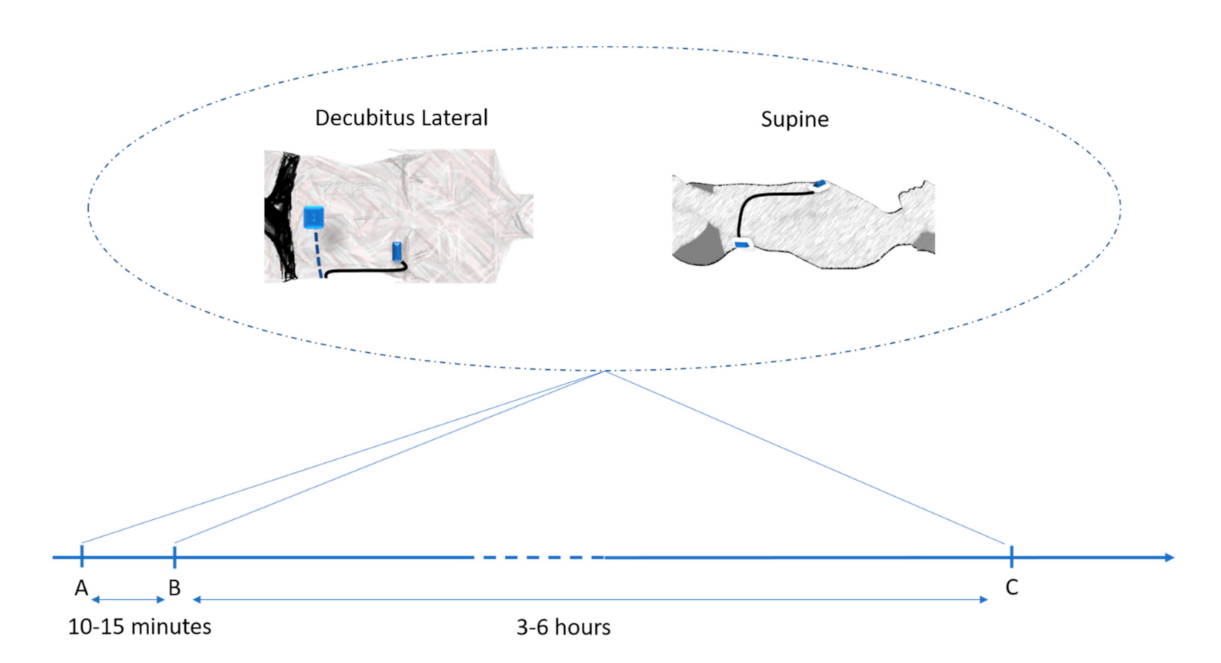
2.1. Protocols and Participants
Breathing Protocol
2.2. Portable Acquisition Device
2.3. Kinocardiography Data Analysis
2.4. Statistics
2.4.1. TRT Reliability Analysis
2.4.2. Influence of Position
3. Results
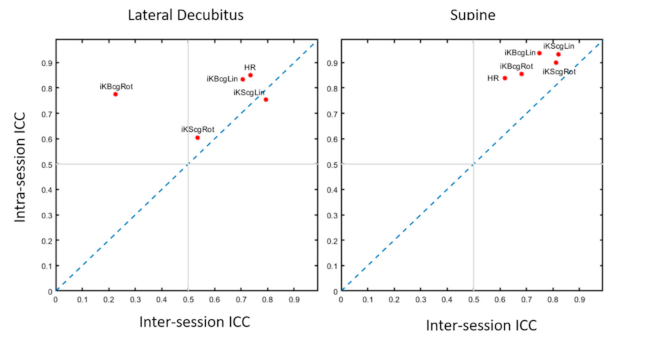
3.1. Test–Retest Reliability
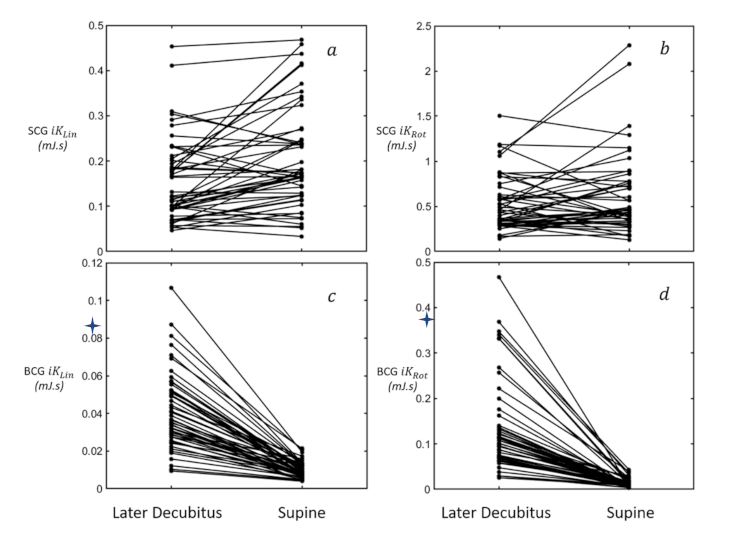
3.2. Influence of Position
4. Discussion
4.1. Main Findings
4.2. Test–Retest Reliability and Reproducibility
4.3. Postural Changes Effects
4.4. Future Directions and Perspectives
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunt, S.A.; Baker, D.W.; Chin, M.H.; Cinquegrani, M.P.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Goldstein, S.; Gregoratos, G.; Jessup, M.L.; et al. ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1995 Guidelines for the Evaluation and Management of Heart Failure): Developed in Collaboration With the International Society for Heart and Lung Transplantation; Endorsed by the Heart Failure Society of America. Circulation 2001, 104, 2996–3007. [Google Scholar]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [Green Version]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [Green Version]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Pinheiro, E.; Postolache, O.; Girão, P. Theory and Developments in an Unobtrusive Cardiovascular System Representation: Ballistocardiography. Open Biomed. Eng. J. 2010, 4, 201–216. [Google Scholar] [CrossRef] [Green Version]
- Giovangrandi, L.; Inan, O.T.; Wiard, R.M.; Etemadi, M.; Kovacs, G.T. Ballistocardiography A method worth revisiting. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; Volume 2011, pp. 4279–4282. [Google Scholar]
- Starr, I. The relation of the ballistocardiogram to cardiac function. Am. J. Cardiol. 1958, 2, 737–747. [Google Scholar] [CrossRef]
- Salernod, M.; Zanetti, J. Seismocardiography: A new technique for recording cardiac vibrations. Concept, method, and initial observations. J. Cardiovasc. Technol. 1990, 9, 111–118. [Google Scholar]
- Jaakkola, J.; Jaakkola, S.; Lahdenoja, O.; Hurnanen, T.; Koivisto, T.; Pänkäälä, M.; Knuutila, T.; Kiviniemi, T.O.; Vasankari, T.; Airaksinen, J. Mobile Phone Detection of Atrial Fibrillation with Mechanocardiography. Circulation 2018, 137, 1524–1527. [Google Scholar] [CrossRef]
- Aydemir, V.B.; Fan, J.; Dowling, S.; Inan, O.T.; Rehg, J.M.; Klein, L. Ballistocardiography for Ambulatory Detection and Prediction of Heart Failure Decompensation. J. Card. Fail. 2018, 24, S116. [Google Scholar] [CrossRef] [Green Version]
- Shandhi, M.H.; Fan, J.; Heller, A.J.; Etemadi, M.; Inan, O.T.; Klein, L. Seismocardiography Can Assess Cardiopulmonary Exercise Test Parameters in Patients with Heart Failure. J. Card. Fail. 2018, 24, S124–S125. [Google Scholar] [CrossRef] [Green Version]
- Hossein, A.; Mirica, D.C.; Rabineau, J.; Del Rio, J.I.; Morra, S.; Gorlier, D.; Nonclercq, A.; Van De Borne, P.; Migeotte, P.-F. Accurate Detection of Dobutamine-induced Haemodynamic Changes by Kino-Cardiography: A Randomised Double-Blind Placebo-Controlled Validation Study. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hossein, A.; Rabineau, J.; Gorlier, D.; Pinki, F.; Van De Borne, P.; Nonclercq, A.; Migeotte, P.-F. Effects of acquisition device, sampling rate, and record length on kinocardiography during position-induced haemodynamic changes. Biomed. Eng. Online 2021, 20, 1–18. [Google Scholar] [CrossRef]
- Morra, S.; Hossein, A.; Gorlier, D.; Rabineau, J.; Chaumont, M.; Migeotte, P.-F.; Van De Borne, P. Modification of the mechanical cardiac performance during end-expiratory voluntary apnea recorded with ballistocardiography and seismocardiography. Physiol. Meas. 2019, 40, 105005. [Google Scholar] [CrossRef] [Green Version]
- Morra, S.; Hossein, A.; Gorlier, D.; Rabineau, J.; Chaumont, M.; Migeotte, P.-F.; Van De Borne, P. Ballistocardiography and seismocardiography detection of hemodynamic changes during simulated obstructive apnea. Physiol. Meas. 2020, 41, 065007. [Google Scholar] [CrossRef]
- Morra, S.; Gauthey, A.; Hossein, A.; Rabineau, J.; Racape, J.; Gorlier, D.; Migeotte, P.-F.; Waroux, J.B.L.P.D.; Van De Borne, P. Influence of sympathetic activation on myocardial contractility measured with ballistocardiography and seismocardiography during sustained end-expiratory apnea. Am. J. Physiol. Integr. Comp. Physiol. 2020, 319, R497–R506. [Google Scholar] [CrossRef]
- Rabineau, J.; Hossein, A.; Landreani, F.; Haut, B.; Mulder, E.; Luchitskaya, E.; Tank, J.; Caiani, E.G.; van de Borne, P.; Migeotte, P.F. Cardiovascular adaptation and countermeasure efficacy assessed by ballistocardiography and seismocardiography during 60 days of simulated microgravity in head-down bed rest. Sci. Rep. 2020, 10, 1–13. [Google Scholar]
- Holloszy, J.O.; Skinner, J.S.; Barry, A.J.; Cureton, T.K. Effect of physical conditioning on cardiovascular function. Am. J. Cardiol. 1964, 14, 761–770. [Google Scholar] [CrossRef]
- Jackson, D.H.; Lane, N.E.; Wherry c, R.J., Jr. A Study of the Ballistocardiographic Test-Retest Reliability; U.S. Naval Aerospace Medical Institute: Pensacola, MI, USA; Naval Aviation Medical Center: Pensacola, MI, USA, 1969. [Google Scholar]
- Alametsä, J.; Palomäki, A.; Viik, J. Short and longer term repeatability of ballistocardiography in a sitting position with EMFi sensor. Med Biol. Eng. Comput. 2011, 49, 881–889. [Google Scholar] [CrossRef]
- Zakeri, V.; Tavakolian, K.; Blaber, A.P.; Bauer, E.P.; Dehkordi, P.; Khosrow-Khavar, F. The repeatability of estimated systolic time intervals in healthy subjects using seismocardiogram and electrocardiogram. Physiol. Meas. 2020, 41, 02NT01. [Google Scholar] [CrossRef]
- De Lalla, V.; Brown, H.R. Respiratory variation of the ballistocardiogram. Am. J. Med. 1950, 9, 728–733. [Google Scholar] [CrossRef]
- Martin-Yebra, A.; Landreani, F.; Casellato, C.; Pavan, E.E.; Migeotte, P.-F.; Frigo, C.A.; Martínez, J.P.; Caiani, E.G. Evaluation of respiratory- and postural-induced changes on the ballistocardiogram signal by time warping averaging. Physiol. Meas. 2017, 38, 1426–1440. [Google Scholar] [CrossRef]
- Inan, O.T.; Migeotte, P.-F.; Park, K.-S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.M.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2014, 19, 1414–1427. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420. [Google Scholar]
- McGraw, K.O.; Wong, S.P. Forming inferences about some intraclass correlation coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Abdi, H.; Salkind, N. Coefficient of Variation. Encycl. Res. Des. 2012, 1, 169–171. [Google Scholar] [CrossRef]
- Inan, O.T.; Etemadi, M.; Wiard, R.M.; Giovangrandi, L.; Kovacs, G.T.A. Robust ballistocardiogram acquisition for home monitoring. Physiol. Meas. 2009, 30, 169–185. [Google Scholar] [CrossRef]
- Rowland, T.W.; Melanson, E.L.; Popowski, B.E.; Ferrone, L.C. Test–Retest Reproducibility of Maximum Cardiac Output by Doppler Echocardiography. Am. J. Cardiol. 1998, 81, 1228–1230. [Google Scholar] [CrossRef]
- Soames, R.W.; Atha, J. Three-dimensional ballistocardiographic responses to changes of posture. Clin. Phys. Physiol. Meas. 1982, 3, 169–177. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Vaini, E.; Castiglioni, P.; Merati, G.; Meriggi, P.; Parati, G.; Faini, A.; Rizzo, F. Wearable seismocardiography: Towards a beat-by-beat assessment of cardiac mechanics in ambulant subjects. Auton. Neurosci. 2013, 178, 50–59. [Google Scholar] [CrossRef]
- Taebi, A.; Solar, B.E.; Bomar, A.J.; Sandler, R.H.; Mansy, H.A. Recent Advances in Seismocardiography. Vibration 2019, 2, 64–86. [Google Scholar] [CrossRef] [Green Version]
- Nakao, S.; Come, P.C.; Miller, M.J.; Momomura, S.; Sahagian, P.; Ransil, B.J.; Grossman, W. Effects of supine and lateral positions on cardiac output and intracardiac pressures: An experimental study. Circulation 1986, 73, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Profant, J.; Dimsdale, J.E. Race and Diurnal Blood Pressure Patterns. Hypertension 1999, 33, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Fagard, R.H. Dipping Pattern of Nocturnal Blood Pressure in Patients with Hypertension. Medscape. Available online: http://www.medscape.com/viewarticle/705780 (accessed on 13 November 2020).
- Starr, I.; Friedland, C.K. On the Cause of The Respiratory Variation of The Ballistocardiogram, with a Note on Sinus Arrhythmia. J. Clin. Investig. 1946, 25, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Jain, P.K.; Tiwari, A.K. A novel method for suppression of motion artifacts from the seismocardiogram signal. In Proceedings of the 2016 IEEE International Conference on Digital Signal Processing (DSP), Beijing, China, 16–18 October 2016; pp. 6–10. [Google Scholar]
- Yu, S.; Liu, S. A Novel Adaptive Recursive Least Squares Filter to Remove the Motion Artifact in Seismocardiography. Sensors 2020, 20, 1596. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Tavassolian, N. Motion Artifact Cancellation of Seismocardiographic Recording from Moving Subjects. IEEE Sens. J. 2016, 16, 5702–5708. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | (µJ·s) | (µJ·s) | SCG (µJ·s) | SCG (µJ·s) | HR (bpm) | BPsys (mmHg) | BPdia (mmHg) | |
|---|---|---|---|---|---|---|---|---|
| Beginning (A) | Sup | 9.7 ± 3.5 | 11.9 ± 6.3 | 195.3 ± 99.4 | 564.6 ± 316.8 | 67.1 ± 9.1 | 128.3 ± 11.9 | 77.6 ± 9.2 |
| LD | 37.6 ± 17.5 | 108.9 ± 73.9 | 131.7 ± 64.0 | 489.0 ± 264.5 | 68.2 ± 9.8 | 128.4 ± 12.2 | 77.0 ± 9.6 | |
| 10 to 15 min later (B) | Sup | 10.4 ± 4.2 | 13.8 ± 9.0 | 196.5 ± 110.6 | 609.5 ± 390.0 | 65.0 ± 8.7 | 128.5 ± 12.1 | 77.1 ± 9.2 |
| LD | 34.0 ± 14.1 | 89.2 ± 44.9 | 102.1 ± 42.1 | 383.0 ± 159.3 | 64.7 ± 9.1 | 128.0 ± 11.8 | 77.2 ± 9.4 | |
| 3 to 6 h later (C) | Sup | 11.8 ± 4.4 | 18.3 ± 9.9 | 206.3 ± 88.6 | 827.1 ± 549.1 | 66.0 ± 10.5 | 130.0 ± 9.5 | 80.6 ± 8.3 |
| LD | 37.8 ± 19.4 | 103.0 ± 63.2 | 134.9 ± 74.3 | 479.7 ± 289.5 | 69.0 ± 9.9 | 129.5 ± 9.8 | 80.2 ± 8.6 | |
| Measurements | HR | BPsys | BPdia | |||||
|---|---|---|---|---|---|---|---|---|
| Short-term TRT (A vs. B) | CV Sup (%) | 2.85 | 3.48 | 4.54 | 3.98 | 1.77 | NA | NA |
| CV LD (%) | 4.35 | 5.07 | 1.82 | 5.34 | 1.1 | NA | NA | |
| ICCc Sup ([90% CI]) | 0.94 [0.91;0.96] | 0.86 [0.79;0.91] | 0.93 [0.90;0.96] | 0.90 [0.85;0.94] | 0.84 [0.69;0.91] | NA | NA | |
| ICCc LD ([90% CI]) | 0.84 [0.76;0.89] | 0.77 [0.66;0.85] | 0.80 [0.70;0.87] | 0.61 [0.45;0.73] | 0.85 [0.52;0.93] | NA | NA | |
| Long-term TRT (A vs. C) | ICCc Sup ([90% CI]) | 0.76 [0.65;0.84] | 0.70 [0.56;0.80] | 0.82 [0.73;0.88] | 0.82 [0.73;0.88] | 0.62 [0.46;0.74] | 0.31 [0.09;0.50] | 0.50 [0.31;0.65] |
| ICCc LD ([90% CI]) | 0.70 [0.57;0.80] | 0.22 [0.00;0.42] | 0.79 [0.69;0.86] | 0.53 [0.35;0.68] | 0.74 [0.61;0.82] | 0.40 [0.19;0.57] | 0.44 [0.24;0.60] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hossein, A.; Rabineau, J.; Gorlier, D.; Del Rio, J.I.J.; van de Borne, P.; Migeotte, P.-F.; Nonclercq, A. Kinocardiography Derived from Ballistocardiography and Seismocardiography Shows High Repeatability in Healthy Subjects. Sensors 2021, 21, 815. https://doi.org/10.3390/s21030815
Hossein A, Rabineau J, Gorlier D, Del Rio JIJ, van de Borne P, Migeotte P-F, Nonclercq A. Kinocardiography Derived from Ballistocardiography and Seismocardiography Shows High Repeatability in Healthy Subjects. Sensors. 2021; 21(3):815. https://doi.org/10.3390/s21030815
Chicago/Turabian StyleHossein, Amin, Jérémy Rabineau, Damien Gorlier, Jose Ignacio Juarez Del Rio, Philippe van de Borne, Pierre-François Migeotte, and Antoine Nonclercq. 2021. "Kinocardiography Derived from Ballistocardiography and Seismocardiography Shows High Repeatability in Healthy Subjects" Sensors 21, no. 3: 815. https://doi.org/10.3390/s21030815