
The Validity and Reliability of a New Intelligent Three-Dimensional Gait Analysis System in Healthy Subjects and Patients with Post-Stroke

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Odonate Conditions
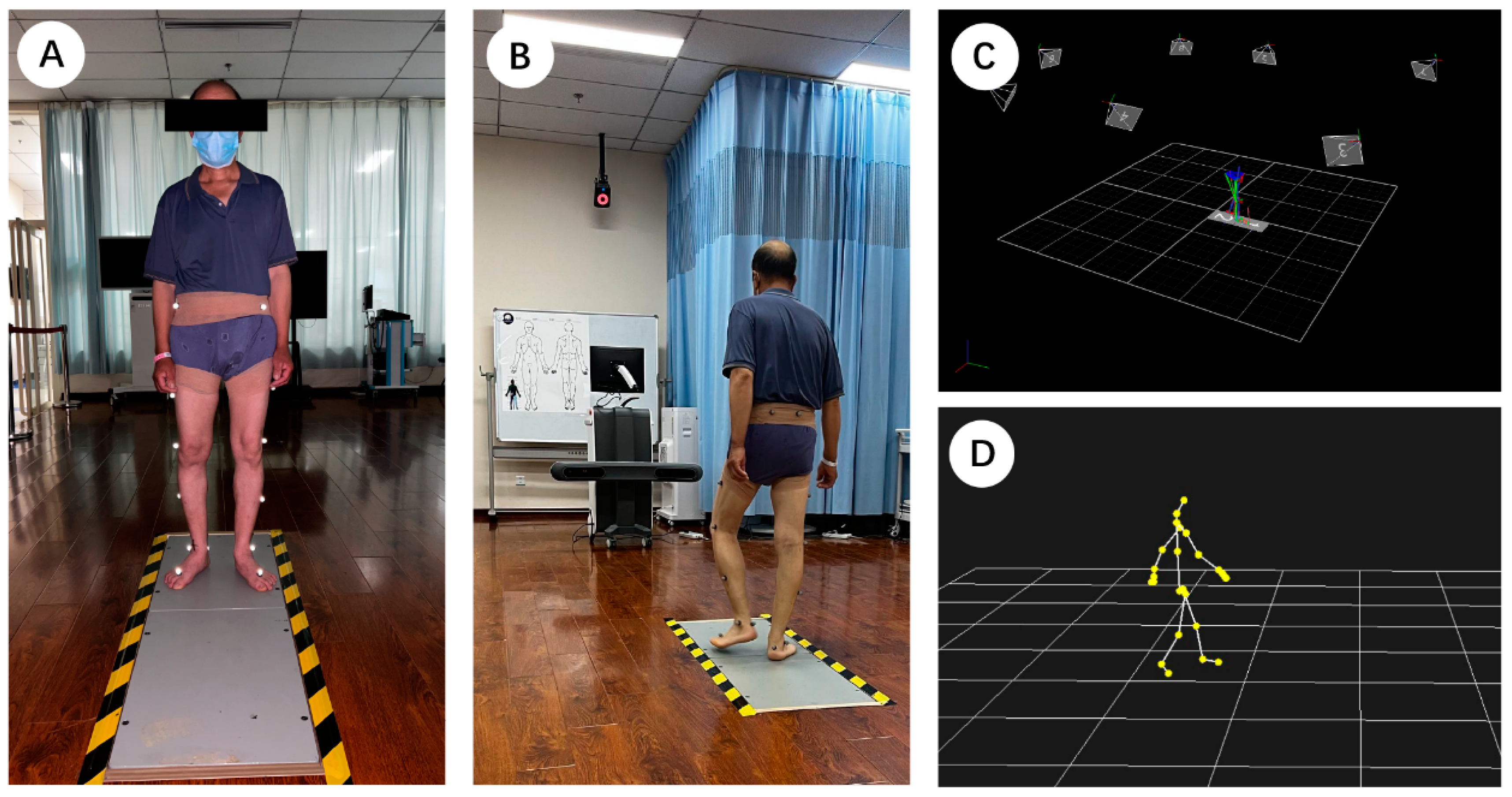
2.3. Testing Procedures
2.4. Data Processing
2.5. Statistical Analysis
3. Results
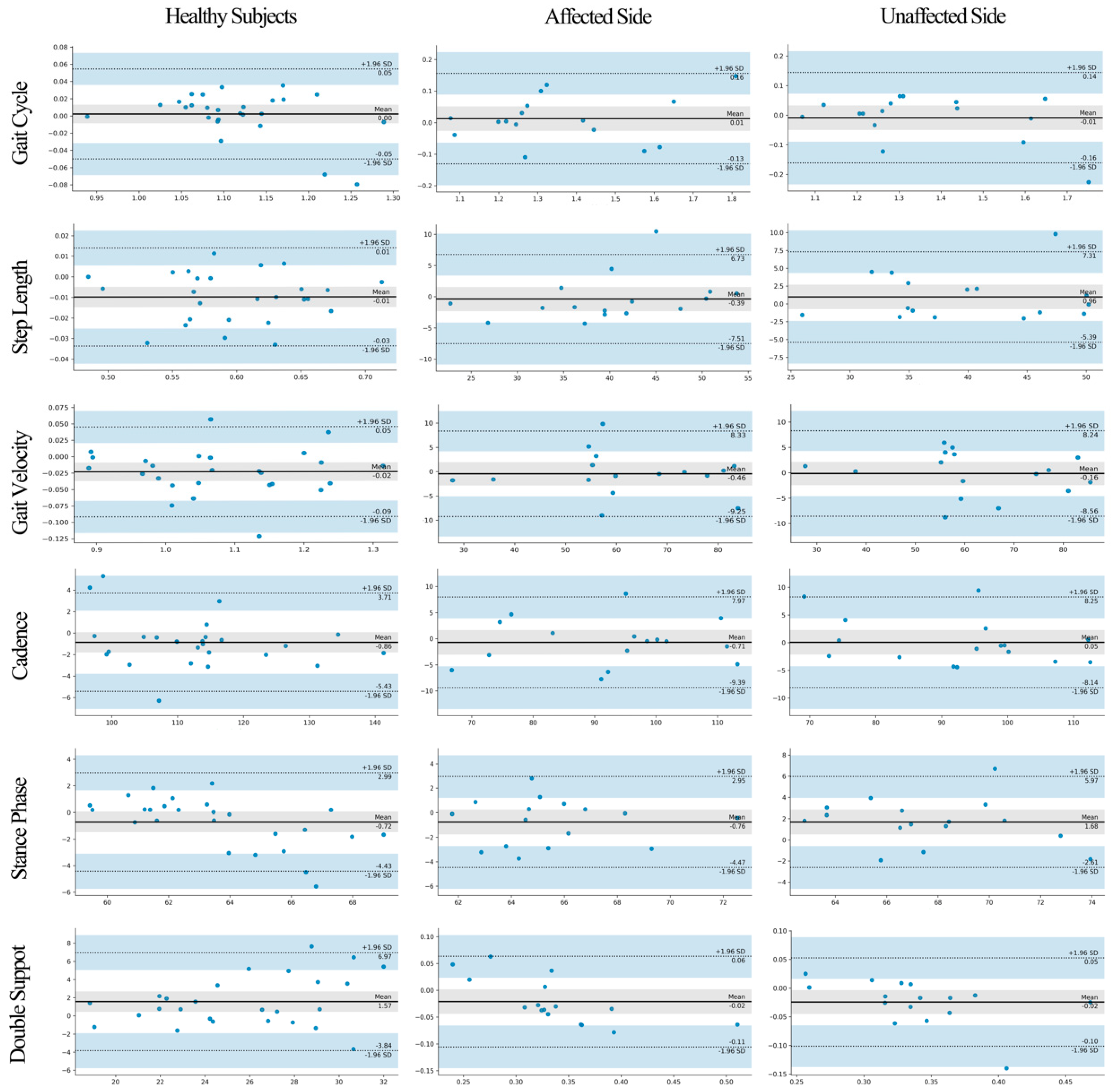
3.1. Gait Spatiotemporal Parameters
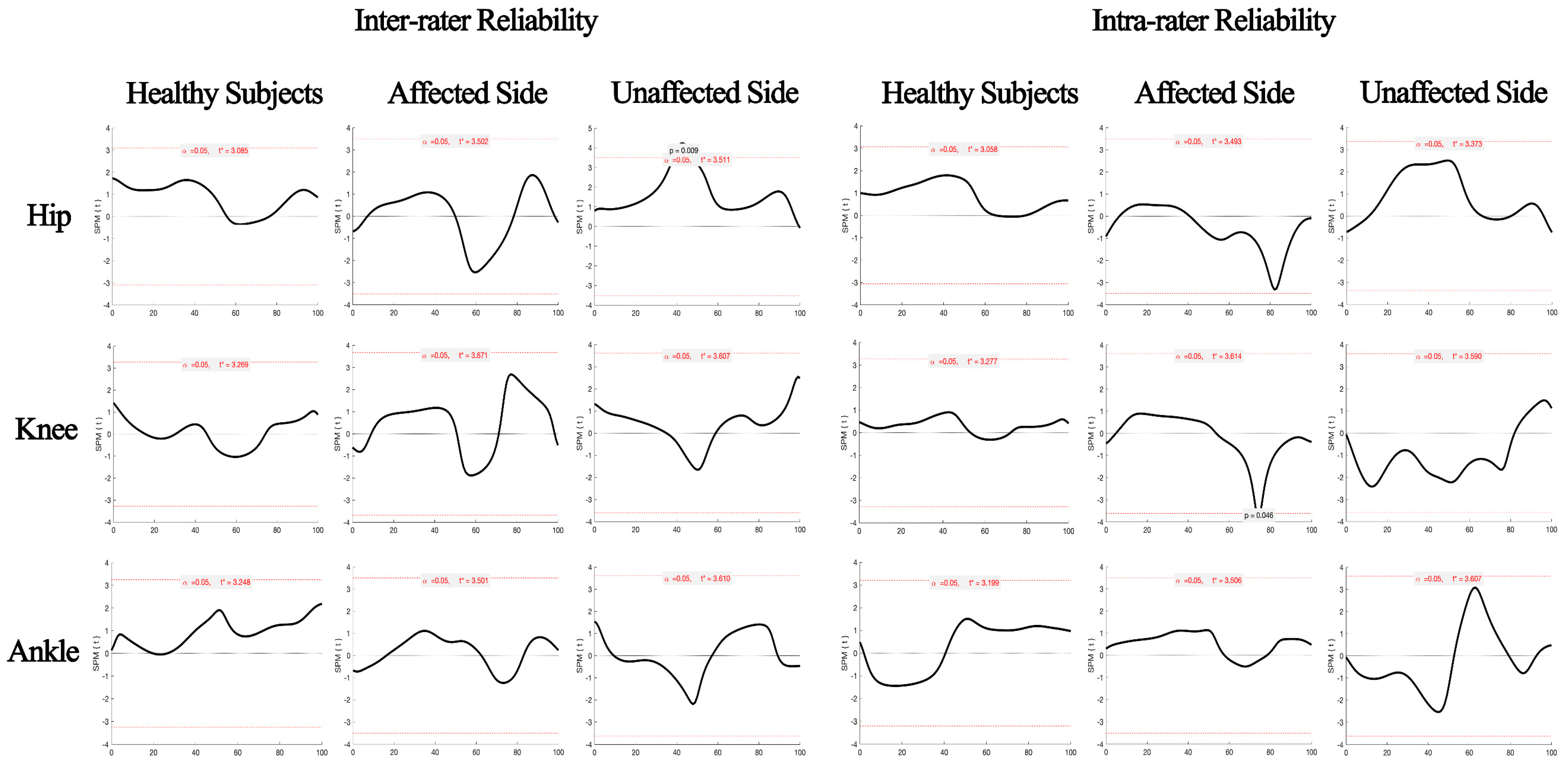
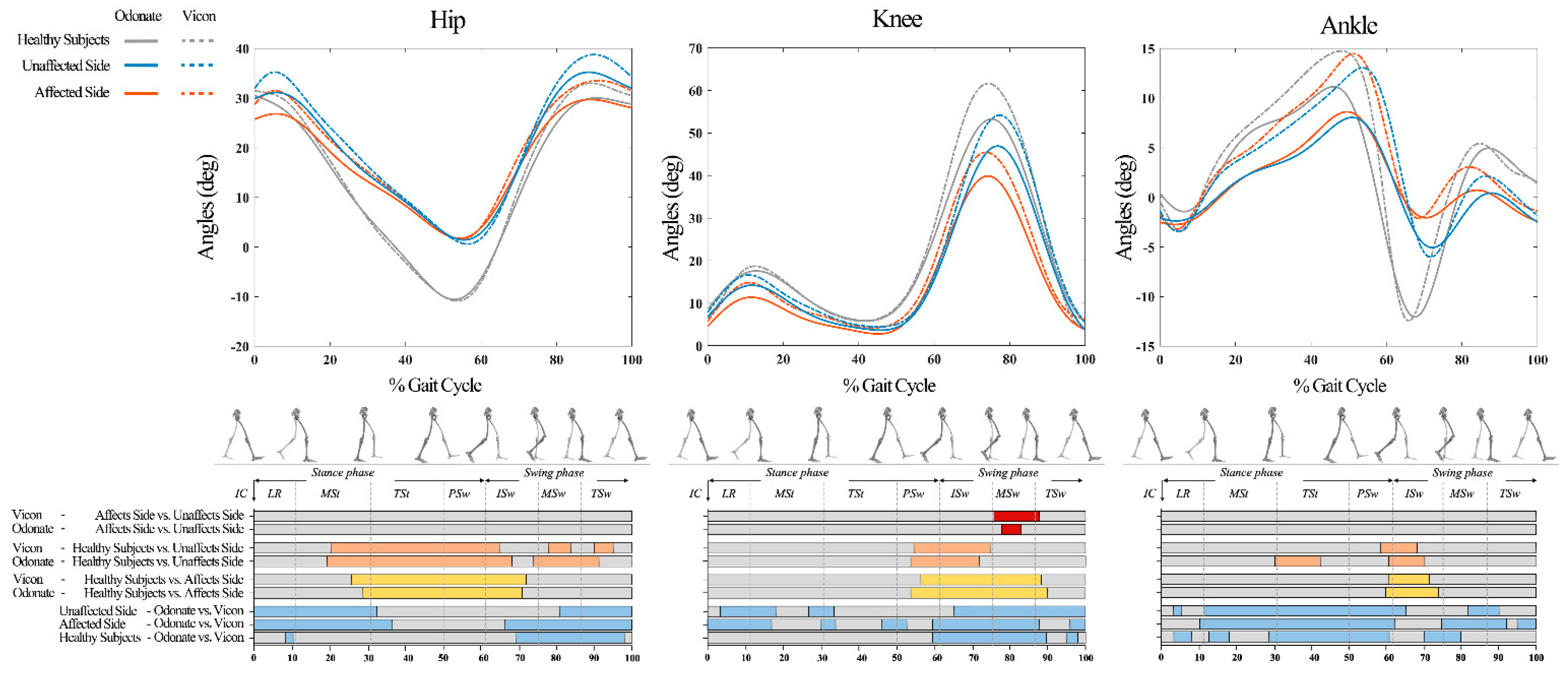
3.2. Joint Kinematics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viswanathan, A.; Sudarsky, L. Balance and gait problems in the elderly. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2012; Volume 103, pp. 623–634. [Google Scholar] [CrossRef] [PubMed]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait post-stroke: Pathophysiology and rehabilitation strategies. Neurophysiol. Clin. 2015, 45, 335–355. [Google Scholar] [CrossRef] [PubMed]
- Bawa, A.; Banitsas, K.; Abbod, M. A Review on the Use of Microsoft Kinect for Gait Abnormality and Postural Disorder Assessment. J. Healthc. Eng. 2021, 2021, 4360122. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Esquenazi, A.; Benedetti, M.G.; Desloovere, K. Gait analysis: Clinical facts. Eur. J. Phys. Rehabil. Med. 2016, 52, 560–574. [Google Scholar] [PubMed]
- Selves, C.; Stoquart, G.; Lejeune, T. Gait rehabilitation after stroke: Review of the evidence of predictors, clinical outcomes and timing for interventions. Acta Neurol. Belg. 2020, 120, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Schroder, J.; Truijen, S.; Van Criekinge, T.; Saeys, W. Feasibility and effectiveness of repetitive gait training early after stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2019, 51, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Wren, T.A.L.; Tucker, C.A.; Rethlefsen, S.A.; Gorton, G.E., 3rd; Ounpuu, S. Clinical efficacy of instrumented gait analysis: Systematic review 2020 update. Gait Posture 2020, 80, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Kopf, A.; Pawelka, S.; Kranzl, A. Clinical gait analysis—Methods, limitations and possible applications. Acta Med. Austriaca 1998, 25, 27–32. [Google Scholar] [PubMed]
- Bonnechere, B.; Jansen, B.; Omelina, L.; Van Sint Jan, S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef]
- Zhong, R.; Rau, P.P. Are cost-effective technologies feasible to measure gait in older adults? A systematic review of evidence-based literature. Arch Gerontol. Geriatr. 2020, 87, 103970. [Google Scholar] [CrossRef] [PubMed]
- Hocking, D.R.; Ardalan, A.; Abu-Rayya, H.M.; Farhat, H.; Andoni, A.; Lenroot, R.; Kachnowski, S. Feasibility of a virtual reality-based exercise intervention and low-cost motion tracking method for estimation of motor proficiency in youth with autism spectrum disorder. J. Neuroeng. Rehabil. 2022, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Beshara, P.; Anderson, D.B.; Pelletier, M.; Walsh, W.R. The Reliability of the Microsoft Kinect and Ambulatory Sensor-Based Motion Tracking Devices to Measure Shoulder Range-of-Motion: A Systematic Review and Meta-Analysis. Sensors 2021, 21, 8186. [Google Scholar] [CrossRef] [PubMed]
- Xavier-Rocha, T.B.; Carneiro, L.; Martins, G.C.; Vilela, J.G.B.; Passos, R.P.; Pupe, C.C.B.; Nascimento, O.; Haikal, D.S.; Monteiro-Junior, R.S. The Xbox/Kinect use in poststroke rehabilitation settings: A systematic review. Arq. Neuropsiquiatr. 2020, 78, 361–369. [Google Scholar] [CrossRef]
- Wang, L.; Huynh, D.Q.; Koniusz, P. A Comparative Review of Recent Kinect-Based Action Recognition Algorithms. IEEE Trans Image Process 2020, 29, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth Analg 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Kelter, R. Analysis of Bayesian posterior significance and effect size indices for the two-sample t-test to support reproducible medical research. BMC Med. Res. Methodol. 2020, 20, 88. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. (Zagreb) 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Roislien, J.; Skare, O.; Opheim, A.; Rennie, L. Evaluating the properties of the coefficient of multiple correlation (CMC) for kinematic gait data. J. Biomech. 2012, 45, 2014–2018. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Mentiplay, B.F.; Hough, E.; Pua, Y.H. Three-dimensional cameras and skeleton pose tracking for physical function assessment: A review of uses, validity, current developments and Kinect alternatives. Gait Posture 2019, 68, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Springer, S.; Yogev Seligmann, G. Validity of the Kinect for Gait Assessment: A Focused Review. Sensors 2016, 16, 194. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Mithraratne, K.; Wilson, N.C.; Wang, X.; Ma, Y.; Zhang, Y. The Validity and Reliability of a Kinect v2-Based Gait Analysis System for Children with Cerebral Palsy. Sensors 2019, 19, 1660. [Google Scholar] [CrossRef]
- Albert, J.A.; Owolabi, V.; Gebel, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. Evaluation of the Pose Tracking Performance of the Azure Kinect and Kinect v2 for Gait Analysis in Comparison with a Gold Standard: A Pilot Study. Sensors 2020, 20, 5104. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; McGorry, R.W.; Chou, L.S.; Lin, J.H.; Chang, C.C. Accuracy of the Microsoft Kinect for measuring gait parameters during treadmill walking. Gait Posture 2015, 42, 145–151. [Google Scholar] [CrossRef]
- Eltoukhy, M.; Kuenze, C.; Oh, J.; Jacopetti, M.; Wooten, S.; Signorile, J. Microsoft Kinect can distinguish differences in over-ground gait between older persons with and without Parkinson’s disease. Med. Eng. Phys. 2017, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Kubota, T.; Yamasaki, T.; Higashi, A. Validity of the total body centre of gravity during gait using a markerless motion capture system. J. Med. Eng. Technol. 2018, 42, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C.; Robinson, M.A.; Vanrenterghem, J. Vector field statistical analysis of kinematic and force trajectories. J. Biomech. 2013, 46, 2394–2401. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C.; Robinson, M.A.; Vanrenterghem, J. Region-of-interest analyses of one-dimensional biomechanical trajectories: Bridging 0D and 1D theory, augmenting statistical power. PeerJ 2016, 4, e2652. [Google Scholar] [CrossRef]
- Pataky, T.C.; Vanrenterghem, J.; Robinson, M.A. The probability of false positives in zero-dimensional analyses of one-dimensional kinematic, force and EMG trajectories. J. Biomech. 2016, 49, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C.; Vanrenterghem, J.; Robinson, M.A. Zero- vs. one-dimensional, parametric vs. non-parametric, and confidence interval vs. hypothesis testing procedures in one-dimensional biomechanical trajectory analysis. J. Biomech. 2015, 48, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Eltoukhy, M.; Oh, J.; Kuenze, C.; Signorile, J. Improved kinect-based spatiotemporal and kinematic treadmill gait assessment. Gait Posture 2017, 51, 77–83. [Google Scholar] [CrossRef]
- Oh, J.; Kuenze, C.; Jacopetti, M.; Signorile, J.F.; Eltoukhy, M. Validity of the Microsoft KinectTM in assessing spatiotemporal and lower extremity kinematics during stair ascent and descent in healthy young individuals. Med. Eng. Phys. 2018, 60, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Timmi, A.; Coates, G.; Fortin, K.; Ackland, D.; Bryant, A.L.; Gordon, I.; Pivonka, P. Accuracy of a novel marker tracking approach based on the low-cost Microsoft Kinect v2 sensor. Med. Eng. Phys. 2018, 59, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Yeung, L.F.; Yang, Z.; Cheng, K.C.; Du, D.; Tong, R.K. Effects of camera viewing angles on tracking kinematic gait patterns using Azure Kinect, Kinect v2 and Orbbec Astra Pro v2. Gait Posture 2021, 87, 19–26. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spatiotemporal Parameters | Odonate-Reliability | ICC3,1 (95%CI) | Odonate-Validity | Cohen’s d | r | ICC2,1 (95%CI) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Day1-A | Day1-B | Day2-A | Inter-Rater | Intra-Rater | Odonate | Vicon | |||||
| healthy subjects | |||||||||||
| Gait Cycle (s) | 1.111 ± 0.067 | 1.114 ± 0.079 | 1.114 ± 0.073 | 0.955 (0.899, 0.980) | 0.968 (0.928, 0.986) | 1.118 ± 0.070 | 1.115 ± 0.081 | 0.029 | 0.947 | 0.968 (0.929, 0.986) | |
| Step Length (m) | 0.599 ± 0.057 | 0.602 ± 0.054 | 0.597 ± 0.051 | 0.974 (0.942, 0.988) | 0.955 (0.899, 0.980) | 0.594 ± 0.055 | 0.600 ± 0.055 | 0.167 | 0.956 | 0.977 (0.950, 0.990) | |
| Gait Velocity (m/s) | 1.077 ± 0.117 | 1.081 ± 0.129 | 1.074 ± 0.111 | 0.985 (0.965, 0.993) | 0.981 (0.958, 0.992) | 1.069 ± 0.118 | 1.079 ± 0.112 | 0.186 | 0.974 | 0.987 (0.971, 0.994) | |
| Cadence (step/min) | 113.481 ± 11.431 | 113.477 ± 11.662 | 112.951 ± 11.710 | 0.988 (0.974, 0.995) | 0.988 (0.973, 0.995) | 112.385 ± 11.196 | 113.245 ± 11.763 | 0.075 | 0.981 | 0.990 (0.977, 0.995) | |
| Stance Phase (%) | 63.442 ± 2.546 | 62.726 ± 2.569 | 63.216 ± 2.260 | 0.942 (0.871, 0.974) | 0.801 (0.555, 0.911) | 63.262 ± 2.196 | 63.979 ± 3.304 | 0.256 | 0.838 | 0.872 (0.714, 0.943) | |
| Swing Phase (%) | 36.558 ± 2.546 | 37.274 ± 2.569 | 36.784 ± 2.260 | 0.942 (0.871, 0.974) | 0.801 (0.555, 0.911) | 36.738 ± 2.196 | 36.020 ± 3.304 | 0.256 | 0.838 | 0.872 (0.714, 0.943) | |
| Double Support (%) | 26.911 ± 5.073 | 25.431 ± 4.669 a | 26.573 ± 4.742 | 0.931 (0.845, 0.969) | 0.872 (0.714, 0.943) | 26.525 ± 4.374 | 24.960 ± 3.516 b | 0.395 | 0.776 | 0.863 (0.694, 0.938) | |
| Affected Side | |||||||||||
| Gait Cycle (s) | 1.346 ± 0.204 | 1.350 ± 0.191 | 1.365 ± 0.213 | 0.983 (0.953, 0.994) | 0.932 (0.805, 0.976) | 1.367 ± 0.219 | 1.354 ± 0.205 | 0.059 | 0.942 | 0.969 (0.912, 0.989) | |
| Step Length (m) | 0.401 ± 0.088 | 0.404 ± 0.076 | 0.400 ± 0.085 | 0.973 (0.923, 0.991) | 0.980 (0.944, 0.993) | 0.400 ± 0.092 | 0.403 ± 0.081 | 0.045 | 0.920 | 0.954 (0.869, 0.984) | |
| Gait Velocity (m/s) | 0.622 ± 0.160 | 0.6112 ± 0.160 | 0.616 ± 0.166 | 0.983 (0.951, 0.994) | 0.984 (0.954, 0.994) | 0.614 ± 0.159 | 0.618 ± 0.163 | 0.028 | 0.962 | 0.980 (0.944, 0.993) | |
| Cadence (step/min) | 93.393 ± 14.693 | 92.837 ± 13.937 | 92.126 ± 14.455 | 0.984 (0.955, 0.995) | 0.958 (0.881, 0.985) | 92.122 ± 14.493 | 92.832± 14.333 | 0.049 | 0.953 | 0.976 (0.931, 0.992) | |
| Stance Phase (%) | 65.614± 2.290 | 64.932 ± 2.484 | 65.689 ± 3.248 | 0.855 (0.585, 0.949) | 0.837 (0.533, 0.943) | 65.176 ± 2.861 | 65.936 ± 2.869 | 0.265 | 0.782 | 0.877 (0.649, 0.957) | |
| Swing Phase (%) | 34.386 ± 2.288 | 35.068 ± 2.484 | 34.311 ± 3.248 | 0.855 (0.585, 0.949) | 0.837 (0.533, 0.943) | 34.824 ± 2.861 | 34.064 ± 2.869 | 0.265 | 0.782 | 0.877 (0.649, 0.957) | |
| Double Support (%) | 35.062 ± 5.499 | 33.063 ± 6.304 a | 36.465 ± 5.994 | 0.889 (0.681, 0.961) | 0.832 (0.518, 0.941) | 32.689 ± 4.995 | 34.806 ± 7.912 | 0.320 | 0.873 | 0.881 (0.660, 0.959) | |
| Unaffected Side | |||||||||||
| Gait Cycle (s) | 1.350 ± 0.204 | 1.367 ± 0.216 | 1.346 ± 0.188 | 0.967 (0.905, 0.988) | 0.971 (0.916, 0.990) | 1.355 ± 0.188 | 1.363 ± 0.219 | 0.043 | 0.938 | 0.962 (0.891, 0.987) | |
| Step Length (m) | 0.398 ± 0.092 | 0.396 ± 0.084 | 0.387 ± 0.071 | 0.979 (0.938, 0.992) | 0.840 (0.543, 0.944) | 0.403 ± 0.077 | 0.393 ± 0.075 | 0.126 | 0.910 | 0.953 (0.865, 0.984) | |
| Gait Velocity (m/s) | 0.613 ± 0.161 | 0.609 ± 0.160 | 0.627 ± 0.163 | 0.980 (0.943, 0.993) | 0.987 (0.962, 0.995) | 0.618 ± 0.156 | 0.620 ± 0.163 | 0.010 | 0.965 | 0.982 (0.947, 0.994) | |
| Cadence (step/min) | 93.123 ± 14.365 | 92.041 ± 14.486 | 92.991 ± 13.540 | 0.982 (0.948, 0.994) | 0.984 (0.954, 0.994) | 92.386 ± 13.160 | 92.332 ± 14.559 | 0.004 | 0.960 | 0.977 (0.934, 0.992) | |
| Stance Phase (%) | 68.054 ± 3.737 | 68.344 ± 3.914 | 67.452 ± 3.598 | 0.946 (0.846, 0.981) | 0.887 (0.678, 0.961) | 68.521 ± 3.196 | 66.842 ± 3.562 b | 0.496 | 0.795 | 0.883 (0.665, 0.959) | |
| Swing Phase (%) | 31.946 ± 3.737 | 31.656 ± 3.914 | 32.548 ± 3.598 | 0.946 (0.846, 0.981) | 0.887 (0.678, 0.961) | 34.479 ± 3.196 | 33.158 ± 3.562 b | 0.496 | 0.795 | 0.883 (0.665, 0.959) | |
| Double Support (%) | 35.113 ± 5.815 | 32.543 ± 5.532 a | 33.328 ± 5.532 | 0.905 (0.729, 0.967) | 0.837 (0.532, 0.943) | 32.820 ± 4.521 | 35.257 ± 6.384 b | 0.441 | 0.792 | 0.855 (0.586, 0.949) | |
| Variable | Inter-Rater Reliability | Intra-Rater Reliability | Validity |
|---|---|---|---|
| Healthy Subjects | |||
| Hip | 0.999 | 0.996 | 0.989 |
| Knee | 0.999 | 0.995 | 0.977 |
| Ankle | 0.983 | 0.977 | 0.917 |
| Affected Side | |||
| Hip | 0.982 | 0.987 | 0.977 |
| Knee | 0.953 | 0.963 | 0.978 |
| Ankle | 0.946 | 0.909 | 0.868 |
| Unaffected Side | |||
| Hip | 0.989 | 0.985 | 0.988 |
| Knee | 0.982 | 0.980 | 0.976 |
| Ankle | 0.934 | 0.950 | 0.917 |
| Authors | Systems | Subjects | Conditions | Consistency | Kinematics | Values |
|---|---|---|---|---|---|---|
| Ma et al. [24] | Kinect v2 VS. Motion Analysis | 10 children with cerebral palsy | Walk | CMC | Hip flexion/extension | 0.75 to 0.81 |
| Knee flexion/extension | 0.85 to 0.87 | |||||
| Ankle dorsi/plantarflexion | 0 to 0.43 | |||||
| Eltoukhy et al. [27] | Kinect v2 VS. BTS System | 11 healthy subjects and 8 patients with Parkinson’s Disease | Walk | ICC (Consistency and Agreement) | Hip ROM | 0.86 to 0.98 |
| Knee ROM | 0.69 to 0.98 | |||||
| Ankle ROM | 0.13 to 0.28 | |||||
| Eltoukhy et al. [33] | Kinect v2 VS. BTS System | 10 healthy subjects | Walk with different speeds | ICC (Consistency and Agreement) | Hip ROM | 0.77 to 0.86 |
| Knee ROM | 0.68 to 0.82 | |||||
| Ankle ROM | –0.39 to 0.05 | |||||
| Oh et al. [34] | Kinect v2 VS. BTS System | 12 healthy subjects | Stair ascent and descent | ICC (Consistency and Agreement) | Peak hip angle | 0.86 to 0.97 |
| Peak knee angle | 0.54 to 0.95 | |||||
| Peak ankle angle | –0.26 to 0.33 | |||||
| Timmi et al. [35] | Kinect v2 VS. Vicon | 20 healthy subjects | Fast walk | Range of LOA | Hip marker coordinates (x,y,z) | (7.7, 10, 8.3) mm |
| Knee marker coordinates (x,y,z) | (8.7, 12.3, 11.6) mm | |||||
| Ankle marker coordinates (x,y,z) | (10.8, 15.1, 26.2) mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Tang, R.; Wang, H.; Yu, X.; Li, Y.; Wang, C.; Wang, L.; Qie, S. The Validity and Reliability of a New Intelligent Three-Dimensional Gait Analysis System in Healthy Subjects and Patients with Post-Stroke. Sensors 2022, 22, 9425. https://doi.org/10.3390/s22239425
Wang Y, Tang R, Wang H, Yu X, Li Y, Wang C, Wang L, Qie S. The Validity and Reliability of a New Intelligent Three-Dimensional Gait Analysis System in Healthy Subjects and Patients with Post-Stroke. Sensors. 2022; 22(23):9425. https://doi.org/10.3390/s22239425
Chicago/Turabian StyleWang, Yingpeng, Ran Tang, Hujun Wang, Xin Yu, Yingqi Li, Congxiao Wang, Luyi Wang, and Shuyan Qie. 2022. "The Validity and Reliability of a New Intelligent Three-Dimensional Gait Analysis System in Healthy Subjects and Patients with Post-Stroke" Sensors 22, no. 23: 9425. https://doi.org/10.3390/s22239425
APA StyleWang, Y., Tang, R., Wang, H., Yu, X., Li, Y., Wang, C., Wang, L., & Qie, S. (2022). The Validity and Reliability of a New Intelligent Three-Dimensional Gait Analysis System in Healthy Subjects and Patients with Post-Stroke. Sensors, 22(23), 9425. https://doi.org/10.3390/s22239425