
Design and Evaluation of CPR Emergency Equipment for Non-Professionals

Abstract
:1. Introduction
2. Materials and Methods
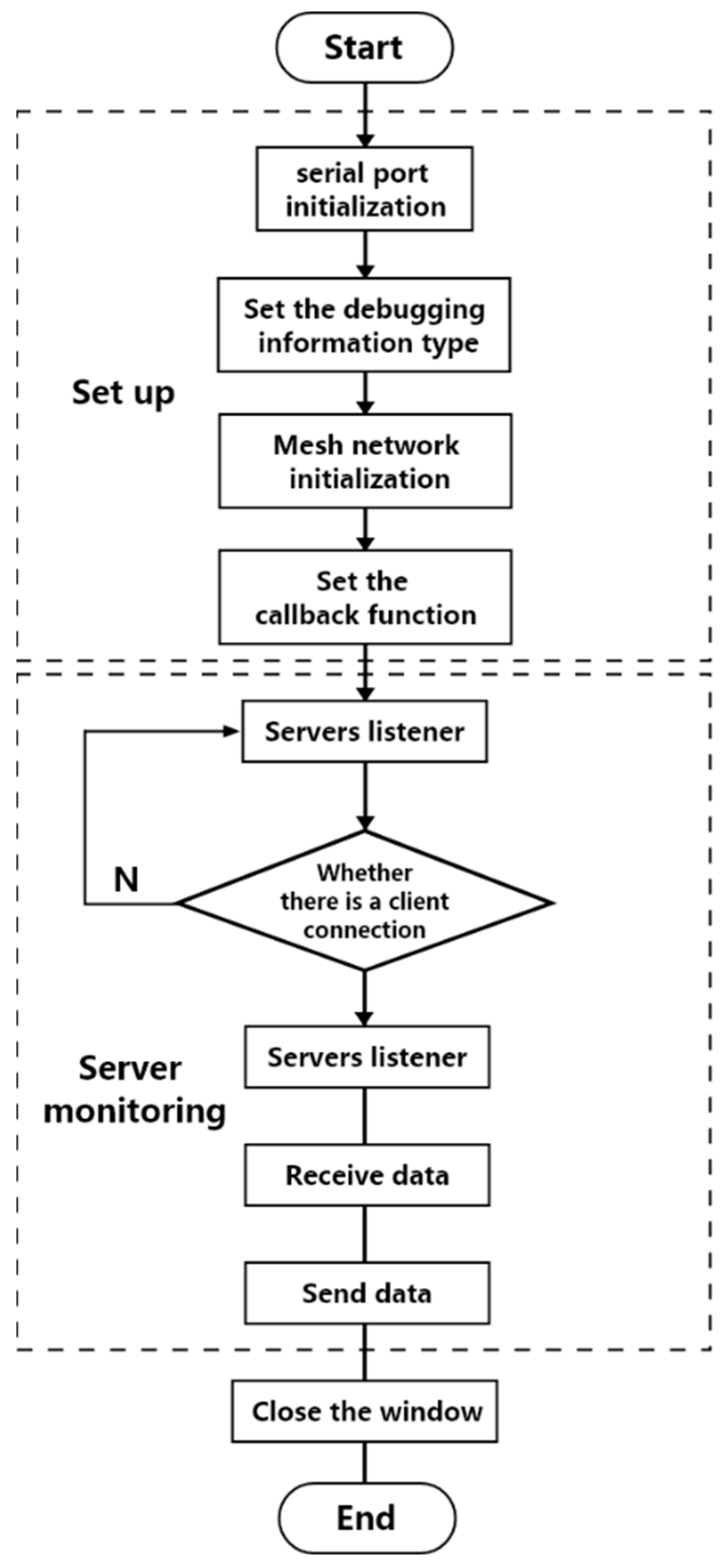
2.1. System Architecture
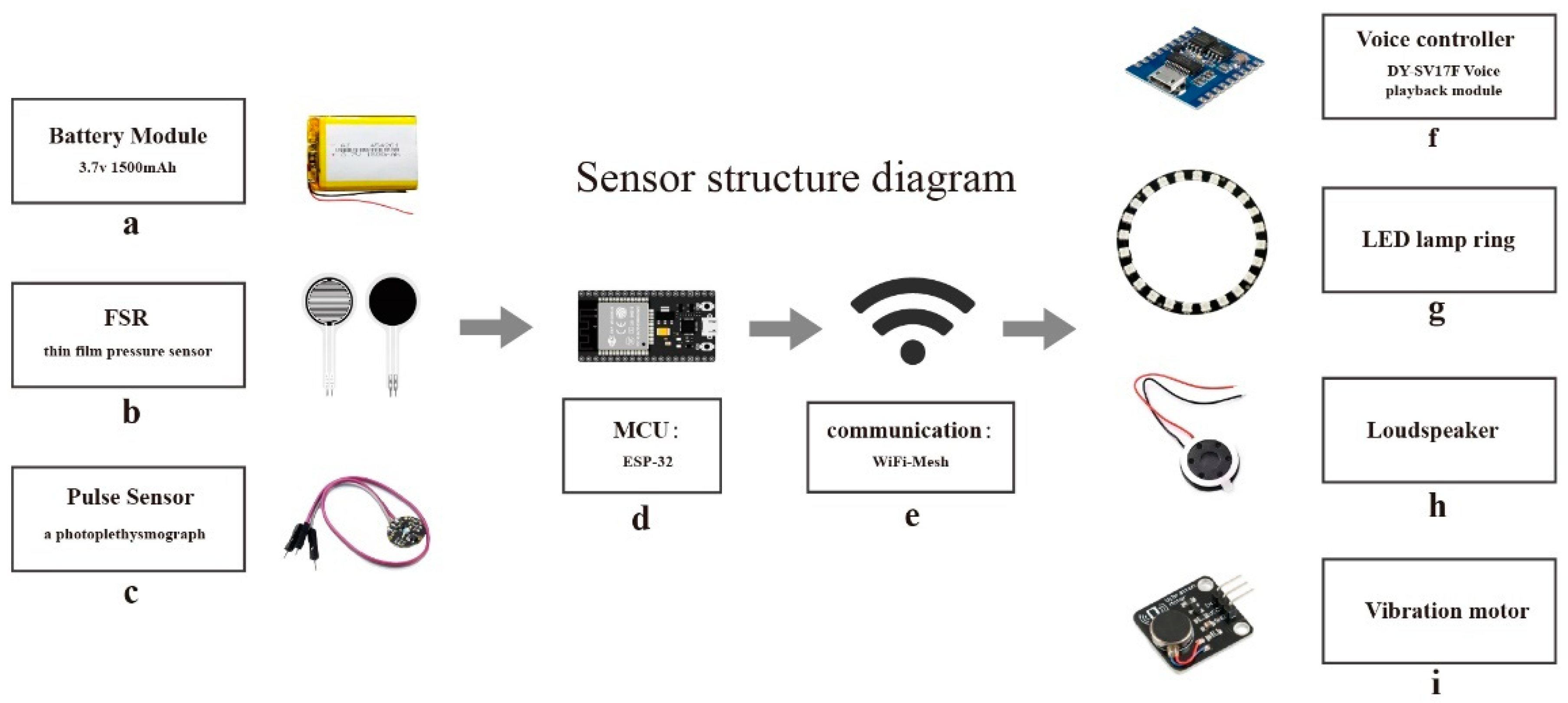
2.2. Hardware Design
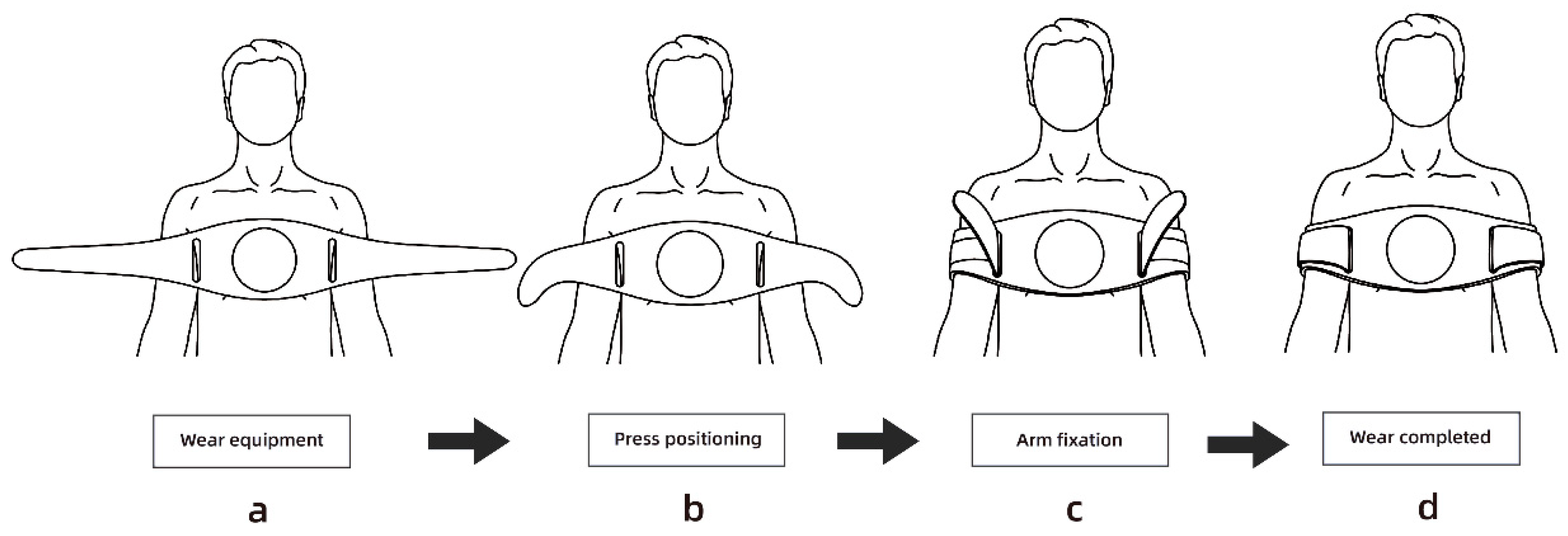
2.2.1. Emergency Clothing Design
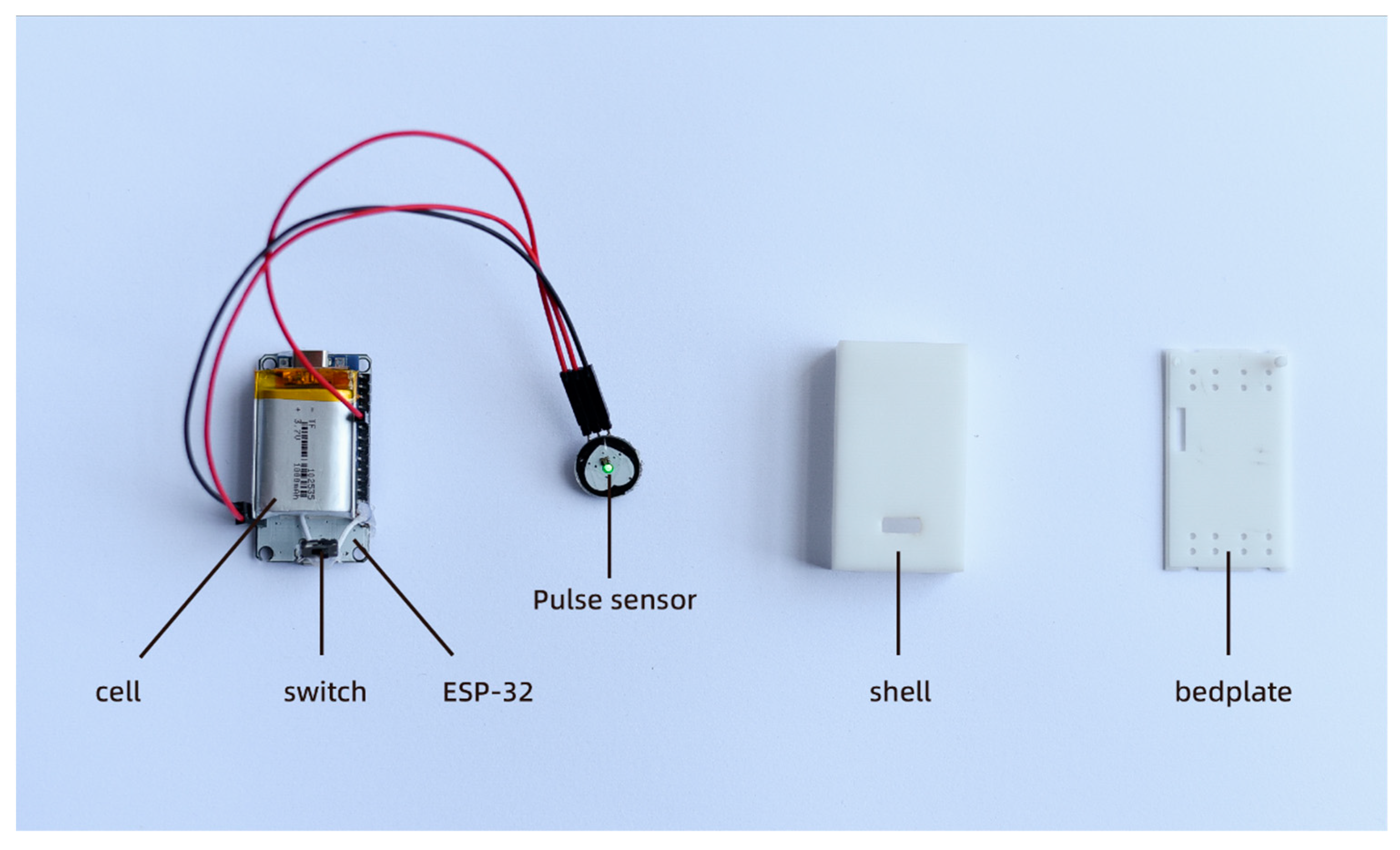
2.2.2. Design of Vital Signs Detector
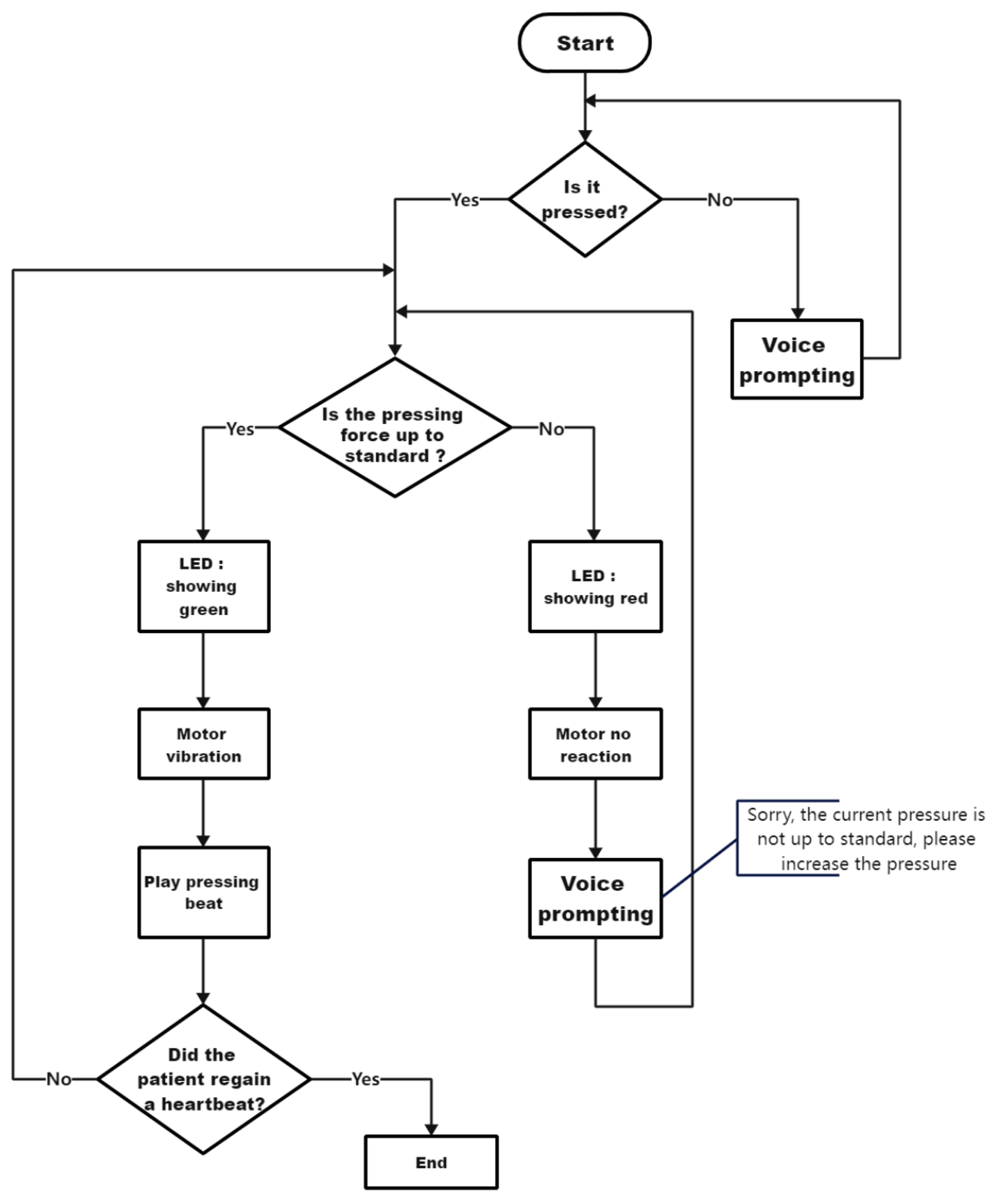
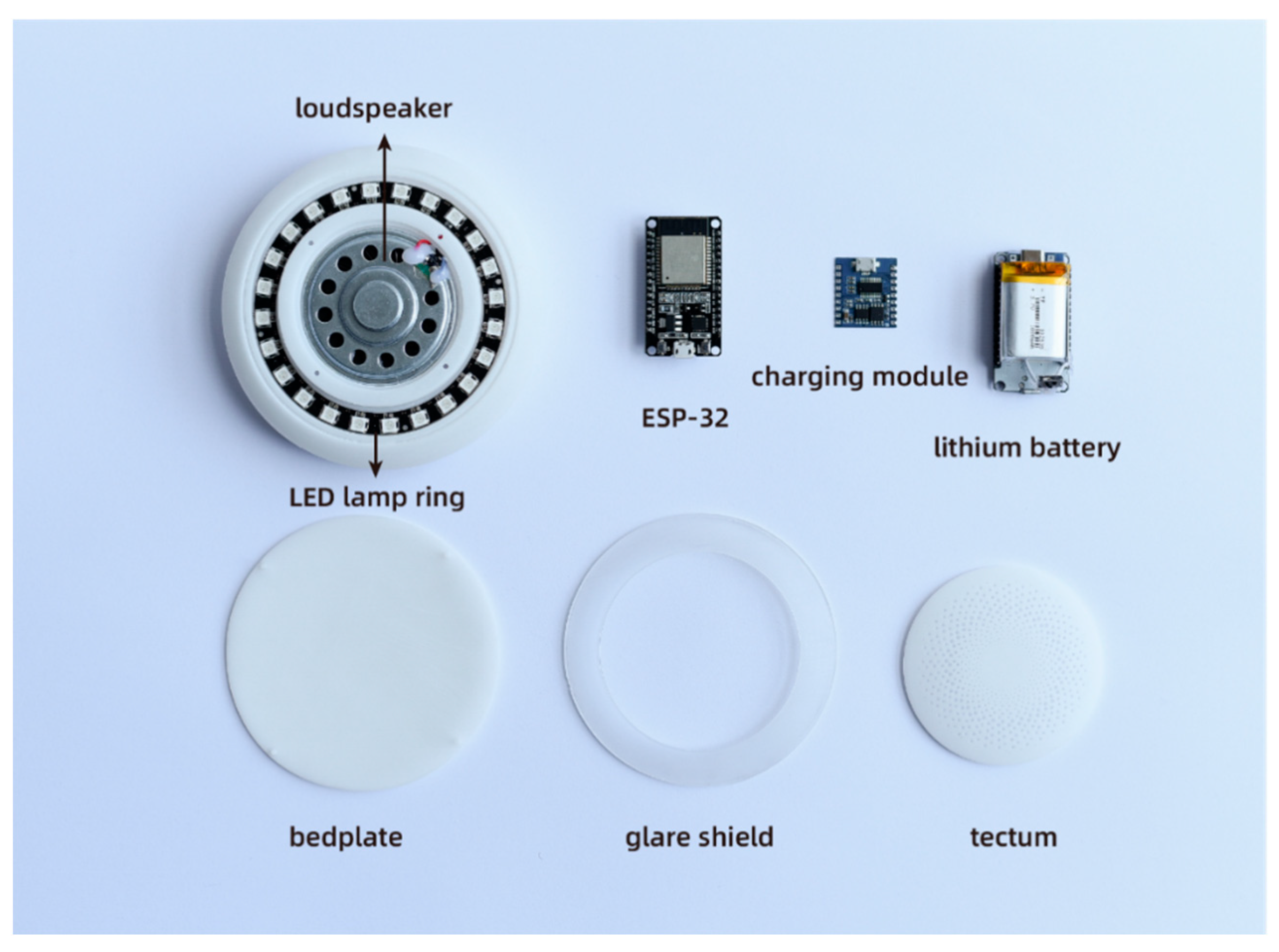
2.2.3. Audio-Visual Integrated Terminal Design
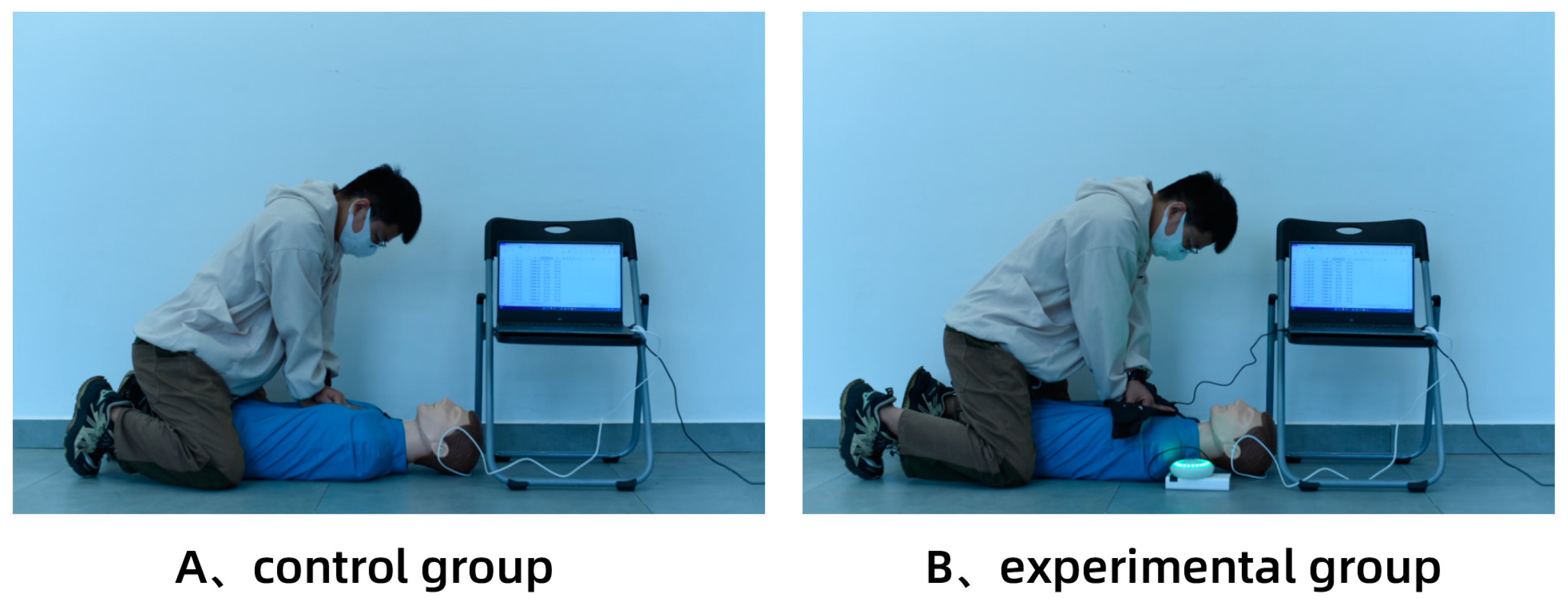
2.3. Research Program
2.4. Measurements
2.5. Usability and Availability Evaluation of Devices
- I will often use this product;
- I think the product is unnecessarily complex;
- I think the product is good;
- I think I need technical support to learn how to use this product;
- I think the functions of the product are well integrated;
- I think there are many inconsistencies in the performance of the product;
- I think most people will learn to use this product soon;
- I think this product is uncomfortable to use;
- I have full confidence in using this product;
- I need to learn a lot before continuing to use the product.
2.6. Statistical Analysis
2.7. Sample Size Determination
3. Results
3.1. Basic Characteristics of Subjects
3.2. Main Evaluation Results
3.3. Results of the Equipment Learnability and Usability Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehra, R. Global public health problem of sudden cardiac death. J. Electrocardiol. 2007, 40, S118–S122. [Google Scholar] [CrossRef]
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; et al. American Heart Association Statistics Committee; Stroke Statistics Subcommittee: Heart Disease and Stroke Statistics—2016 update: A report from the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar]
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.P.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef]
- Berg, K.M.; Soar, J.; Andersen, L.W.; Böttiger, B.W.; Cacciola, S.; Callaway, C.W.; Couper, K.; Cronberg, T.; D’Arrigo, S.; Deakin, C.D.; et al. Adult Advanced Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2020, 156, A80–A119. [Google Scholar] [CrossRef]
- Abella, B.S.; Edelson, D.P.; Kim, S.; Retzer, E.; Myklebust, H.; Barry, A.M.; O’Hearn, N.; Hoek, T.L.V.; Becker, L.B. CPR quality improvement during in-hospital cardiac arrest using a real-time audiovisual feedback system. Resuscitation 2007, 73, 54–61. [Google Scholar] [CrossRef]
- Gallagher, E.J.; Lombardi, G.; Gennis, P. Effectiveness of bystander cardiopulmonary resuscitation and survival following out-of-hospital cardiac arrest. JAMA 1995, 274, 1922–1925. [Google Scholar] [CrossRef]
- Van Hoeyweghen, R.J.; Bossaert, L.L.; Mullie, A.; Calle, P.; Martens, P.; Buylaert, W.A.; Delooz, H. Quality and efficiency of bystander CPR. Belgian Cerebral Resuscitation Study Group. Resuscitation 1993, 26, 47–52. [Google Scholar] [CrossRef]
- Wik, L.; Steen, P.A.; Bircher, N.G. Quality of bystander cardiopulmonary resuscitation influences outcome after prehospital cardiac arrest. Resuscitation 1994, 28, 195–203. [Google Scholar] [CrossRef]
- Safar, P.; Brown, T.C.; Holtey, W.J.; Wilder, R.J. Ventilation and circulation with closed-chest cardiac massage in man. J. Amer. Med. Assoc. 1961, 176, 574–576. [Google Scholar] [CrossRef]
- SOS-KANTO Study Group. Cardiopulmonary resuscitation by bystanders with chest compression only (SOS-KANTO): An observational study. Lancet 2007, 369, 920–926. [Google Scholar] [CrossRef]
- Rea, T.D.; Fahrenbruch, C.; Culley, L.; Donohoe, R.T.; Hambly, C.; Innes, J.; Bloomingdale, M.; Subido, C.; Romines, S.; Eisenberg, M.S. CPR with chest compression alone or with rescue breathing. N. Engl. J. Med. 2010, 363, 423–433. [Google Scholar] [PubMed] [Green Version]
- Wik, L.; Kramer-Johansen, J.; Myklebust, H.; Sørebø, H.; Svensson, L.; Fellows, B.; Steen, P.A. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. JAMA 2005, 293, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Stiell, I.G.; Brown, S.P.; Christenson, J.; Cheskes, S.; Nichol, G.; Powell, J.; Bigham, B.; Morrison, L.J.; Larsen, J.; Hess, E.; et al. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Crit. Care Med. 2012, 40, 1192–1198. [Google Scholar] [CrossRef] [Green Version]
- Aufderheide, T.P.; Pirrallo, R.G.; Yannopoulos, D.; Klein, J.P.; Von Briesen, C.; Sparks, C.W.; Deja, K.A.; Conrad, C.J.; Kitscha, D.J.; Provo, T.A.; et al. Incomplete chest wall decompression: A clinical evaluation of CPR performance by EMS personnel and assessment of alternative manual chest compression–decompression techniques. Resuscitation 2005, 64, 353–362. [Google Scholar] [CrossRef]
- Smereka, J.; Szarpak, L.; Czekajlo, M.; Abelson, A.; Zwolinski, P.; Plusa, T.; Dunder, D.; Dabrowski, M.; Wiesniewska, Z.; Robak, O.; et al. The TrueCPR device in the process of teaching cardiopulmonary resuscitation: A randomized simulation trial. Medicine 2019, 98, e15995. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Aufderheide, T.P.; Eigel, B.; Hickey, R.W.; Longstreth, W.T., Jr.; Nadkarni, V.; Nichol, G.; Sayre, M.R.; Sommargren, C.E.; Hazinski, M.F. Reducing barriers for implementation of bystander-initiated cardiopulmonary resuscitation: A scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation. Circulation 2008, 117, 704–709. [Google Scholar] [PubMed] [Green Version]
- Bobrow, B.J.; Spaite, D.W.; Berg, R.A.; Stolz, U.; Sanders, A.B.; Kern, K.B.; Vadeboncoeur, T.F.; Clark, L.L.; Gallagher, J.V.; Stapczynski, J.S.; et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA 2010, 304, 1447–1454. [Google Scholar] [CrossRef] [Green Version]
- Grassl, K.; Leidel, B.A.; Stegmaier, J.; Bogner, V.; Huppertz, T.; Kanz, K.G. Quality of chest compressions in lay person cardiopulmonary resuscitation. Use of a real-time audiovisual feedback system. Notf. Rett. 2009, 12, 117–122. [Google Scholar]
- Yeung, J.; Meeks, R.; Edelson, D.; Gao, F.; Soar, J.; Perkins, G.D. The use of CPR feedback/prompt devices during training and CPR performance: A systematic review. Resuscitation 2009, 80, 743–751. [Google Scholar] [CrossRef] [Green Version]
- Pozner, C.N.; Almozlino, A.; Elmer, J.; Poole, S.; McNamara, D.; Barash, D. Cardiopulmonary resuscitation feedback improves the quality of chest compression provided by hospital health care professionals. Am. J. Emerg. Med. 2011, 29, 618–625. [Google Scholar] [CrossRef]
- Skorning, M.H.; Beckers, S.K.; Brokmann, J.C.; Rörtgen, D.C.; Bergrath, S.; Veiser, T.; Heussen, N.; Rossaint, R. New visual feedback device improves performance of chest compressions by professionals in simulated cardiac arrest. Resuscitation 2010, 81, 53–58. [Google Scholar] [CrossRef]
- Kern, K.B.; Sanders, A.B.; Raife, J.; Milander, M.M.; Otto, C.W.; Ewy, G.A. A study of chest compression rates during cardiopulmonary resuscitation in humans: The importance of rate-directed chest compressions. Arch. Intern. Med. 1992, 152, 145–149. [Google Scholar] [CrossRef]
- Chung, T.N.; Bae, J.; Kim, E.C.; Cho, Y.K.; You, J.S.; Choi, S.W.; Kim, O.J. Induction of a shorter compression phase is correlated with a deeper chest compression during metronome-guided cardiopulmonary resuscitation: A manikin study. Emerg. Med. J. 2013, 30, 551–554. [Google Scholar] [CrossRef]
- Kurowski, A.; Szarpak, Ł.; Bogdański, Ł.; Zaśko, P.; Czyżewski, Ł. The effectiveness of cardiopulmonary resuscitation using CPR feedback devices. Kardiol. Pol. 2015, 73, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Lai, H.Y.; Hsieh, T.C.; Wu, W.R. Using real-time device-based visual feedback in CPR recertification programs: A prospective randomised controlled study. Nurse Educ. Today 2023, 124, 105755. [Google Scholar] [CrossRef] [PubMed]
- Kahsay, D.T.; Peltonen, L.M.; Rosio, R.; Tommila, M.; Salanterä, S. The effect of standalone audio-visual feedback devices on the quality of chest compressions during laypersons’ CPR training: A Systematic review and meta-analysis. Eur. J. Cardiovasc. Nurs. 2023, zvad041. [Google Scholar] [CrossRef] [PubMed]
- Ahn, C.; Lee, S.; Lee, J.; Oh, J.; Song, Y.; Kim, I.Y.; Kang, H. Impact of a Smart-Ring-Based Feedback System on the Quality of Chest Compressions in Adult Cardiac Arrest: A Randomized Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 5408. [Google Scholar] [CrossRef]
- Song, Y.; Oh, J.; Chee, Y. A New Chest Compression Depth Feedback Algorithm for High-Quality CPR Based on Smartphone. Telemed. J. E-Health 2014, 21, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Iskrzycki, L.; Smereka, J.; Rodriguez-Nunez, A.; Furelos, R.B.; Gomez, C.A.; Kaminska, H.; Wieczorek, W.; Szarpak, L.; Nadolny, K.; Galazkowski, R.; et al. The impact of the use of CPRMeter monitor on the chest compressions quality: A prospective randomized trial, cross-simulation. Kardiol. Pol. 2018, 76, 574–579. [Google Scholar] [CrossRef] [Green Version]
- Majer, J.; Madziala, A.; Dabrowska, A.; Dabrowski, M. The place of TrueCPR feedback device in cardiopulmonary resuscitation. Should we use it? A randomized pilot study. Disaster Emerg. Med. J. 2018, 3, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Buléon, C.; Parienti, J.J.; Morilland-Lecoq, E.; Halbout, L.; Cesaréo, E.; Dubien, P.Y.; Jardel, B.; Boyer, C.; Husson, K.; Andriamirado, F.; et al. Impacts of chest compression cycle length and real-time feedback with a CPRmeter® on chest compression quality in out-of-hospital cardiac arrest: Study protocol for a multicenter randomized controlled factorial plan trial. Trials 2020, 21, 627. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Augré, C.; Rogers, H.; Allan, M.; Thickett, D.R. CPREzy: An evaluation during simulated cardiac arrest on a hospital bed. Resuscitation 2005, 64, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Zapletal, B.; Greif, R.; Stumpf, D.; Nierscher, F.J.; Frantal, S.; Haugk, M.; Ruetzler, K.; Schlimp, C.; Fischer, H. Comparing three CPR feedback devices and standard BLS in a single rescuer scenario: A randomised simulation study. Resuscitation 2013, 85, 560–566. [Google Scholar] [CrossRef]
- Muhendra, R.; Rinaldi, A.; Budimana, M.; Khairurrijal. Development of WiFi Mesh Infrastructure for Internet of Things applications. Procedia Eng. 2017, 170, 332–337. [Google Scholar] [CrossRef]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlář, A.; Wyllie, J.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef]
- Parak, J.; Korhonen, I. Evaluation of wearable consumer heart rate monitors based on photopletysmography. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 3670–3673. [Google Scholar]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult basic and advanced life support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S366–S468. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Intl. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- McLellan, S.; Muddimer, A.; Peres, S.C. The effect of experience on System Usability Scale ratings. J. Usability Stud. 2012, 7, 56–67. [Google Scholar]
- Brooke, J. Usability Evaluation in Industry; Taylor & Francis Ltd.: London, UK, 1996; pp. 4–7. [Google Scholar]
- Semeraro, F.; Frisoli, A.; Loconsole, C.; Bannò, F.; Tammaro, G.; Imbriaco, G.; Marchetti, L.; Cerchiari, E.L. Motion detection technology as a tool for cardiopulmonary resuscitation (CPR) quality training: A randomised crossover mannequin pilot study. Resuscitation 2012, 84, 501–507. [Google Scholar] [CrossRef]
- Ashton, A.; McCluskey, A.; Gwinnutt, C.L.; Keenan, A.M. Effect of rescuer fatigue on performance of continuous external chest compressions over 3 min. Resuscitation 2002, 55, 151–155. [Google Scholar] [CrossRef]
- Heidenreich, J.W.; Berg, R.A.; Higdon, T.A.; Ewy, G.A.; Kern, K.B.; Sanders, A.B. Rescuer fatigue: Standard versus continuous chest-compression cardiopulmonary resuscitation. Acad. Emerg. Med. 2006, 13, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Hightower, D.; Thomas, S.H.; Stone, C.K.; Dunn, K.; March, J.A. Decay in quality of closed-chest compressions over time. Ann. Emerg. Med. 1995, 26, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, F.J.; Ramalle-Gomara, E.; Lisa, V.; Saralegui, I. The effect of rescuer fatigue on the quality of chest compressions. Resuscitation 1998, 37, 149–152. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Experimenter (n = 32) |
|---|---|
| Gender (female) | 16/32 |
| Age | 23.72 ± 1.97 |
| Height (cm) | 170 ± 6.21 |
| Weight (kg) | 60.53 ± 11.36 |
| BMI (kg/m2) | 20.82 ± 2.76 |
| Result | A (Control Group) | B (Experimental Group) | Standard CPR | p-Value |
|---|---|---|---|---|
| CC Depth (mm) | 50.2 ± 2.2 | 51.5 ± 1.3 | 55 ± 7 | 0.012 |
| CC Rate (times/min) | 100.4 ± 6.6 | 110.1 ± 6.2 | 113 ± 12 | p < 0.001 |
| Precise depth of CC ratio (%) | 63.25 | 82.11 | 100 | 0.066 |
| Precise rate of CC ratio (%) | 56.52 | 93.75 | 100 | 0.024 |
| NO | Question | Mean | SD 1 |
|---|---|---|---|
| 1 | I will often use this product | 4.16 | 0.15 |
| 2 | I think the product is unnecessarily complex | 1.72 | 0.15 |
| 3 | I think the product is good | 4.31 | 0.122 |
| 4 | I think I need technical support to learn how to use this product | 2.00 | 0.168 |
| 5 | I think the functions of the product are well integrated. | 4.22 | 0.125 |
| 6 | I think there are many inconsistencies in the performance of the product | 1.94 | 0.142 |
| 7 | I think most people will learn to use this product soon. | 4.50 | 0.110 |
| 8 | I think this product is uncomfortable to use. | 1.66 | 0.139 |
| 9 | I have full confidence in using this product | 3.69 | 0.171 |
| 10 | I need to learn a lot before continuing to use the product. | 2.13 | 0.166 |
| aggregate score | 78.594 | 2.652 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, J.; Wu, Q. Design and Evaluation of CPR Emergency Equipment for Non-Professionals. Sensors 2023, 23, 5948. https://doi.org/10.3390/s23135948
Xie J, Wu Q. Design and Evaluation of CPR Emergency Equipment for Non-Professionals. Sensors. 2023; 23(13):5948. https://doi.org/10.3390/s23135948
Chicago/Turabian StyleXie, Jiayu, and Qun Wu. 2023. "Design and Evaluation of CPR Emergency Equipment for Non-Professionals" Sensors 23, no. 13: 5948. https://doi.org/10.3390/s23135948
APA StyleXie, J., & Wu, Q. (2023). Design and Evaluation of CPR Emergency Equipment for Non-Professionals. Sensors, 23(13), 5948. https://doi.org/10.3390/s23135948