1. Introduction
Researchers [
1,
2,
3] have been employing various two-dimensional (2D) methods to manage measurements obtained from standard photographs or X-rays in various projections [
4,
5] or directly from subjects [
6,
7]. However, the recent development of new acquisition techniques and relevant software has enabled the use of three-dimensional (3D) scans in various areas of dental medicine. These improvements include high-quality motion-fixed image capture to provide better sequential frames with landmark detection. Three-dimensional surface scanning can generate a 3D soft tissue model of the face. The scanning equipment, such as infrared laser digitisers, stereophotogrammetric cameras, or structured-light scanners, is non-invasive [
8,
9]. At the same time, some researchers employ computed tomography (CT) or cone beam computed tomography (CBCT), which emits radiation [
10]. Facial images are usually studied using anatomical landmarks (e.g., see Farkas [
11]). Each landmark is defined by three coordinates in the x, y and z spatial dimensions. The set of all landmarks representing a 3D model of the face is known as a landmark configuration or a shape, and such configurations are further analysed using the methods of geometric morphometrics. The development of software to study 3D images tends to create subgroups based on soft tissue shape differences, as opposed to traditional predefined facial characteristics used in 2D studies [
12]. The accuracy of the non-invasive facial scanners, usually 0.2 to 1 mm, is satisfactory for clinical purposes [
13]. However, there are differences between various scanning techniques and manufacturers [
14,
15]. Nevertheless, the advancement in scanning technology and computational methods have made non-invasive scanners available at affordable prices, which could facilitate and further promote research and clinical application of 3D models. Additionally, independent initiatives in software development help verify the application of commercially available low-cost equipment. Analysing patients’ soft tissues and the effect of various dental procedures on their facial physiognomy is quite demanding. The operator performing manual physical measurements must possess sufficient knowledge and exhibit considerable caution to the patient. Because there is direct contact between the soft tissue and the instrument, the process can cause discomfort for the patient, especially after certain procedures that may result in swelling and pain. In addition, it is time-consuming for both the patient and the examiner.
To minimise discomfort and simplify the process, we performed facial scanning and computer measurement of experimentally determined demarcation lines. Demarcation lines are virtual boundaries or lines that separate different areas or connect two different anatomical points on the face. Demarcation lines used in this research are chosen based on previous research for the assessment of the post-surgery oedema [
4,
5,
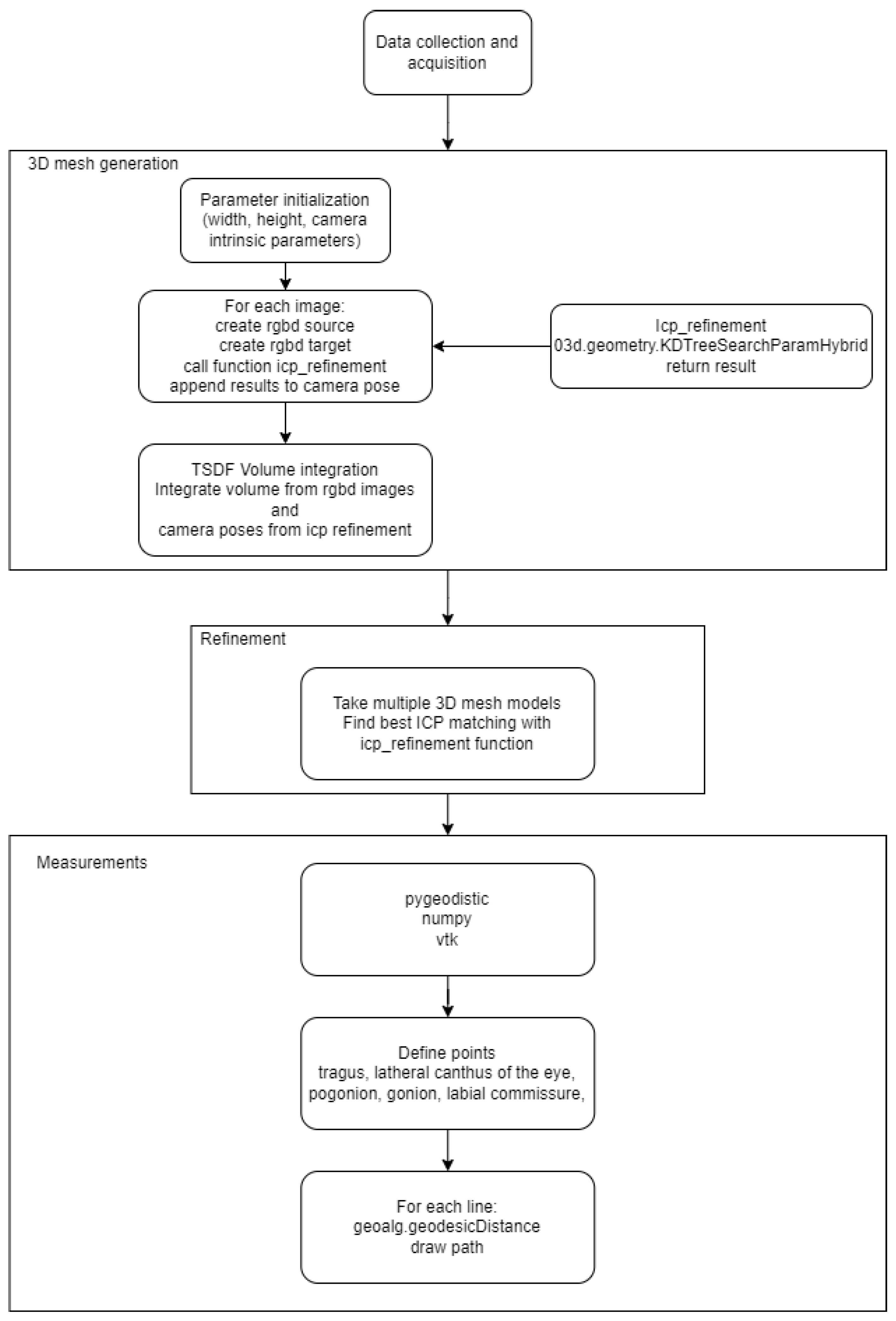
6]. The image acquisition was carried out with a low-cost 3D scanner which requires many consecutive recordings of the object for the best results. RGBD integration was used for merging frames into a 3D object [
16]. For correct comparison, the resulting images need to be registered together, which is usually performed with Ransac [
17] and ICP [
18] based techniques. We used the slower but more precise ICP method [
19]. The measurements on 3D images can be performed using exact or approximate distances. With approximate distances, it is assumed that the path between two close points can be approximated by Euclidian distance (neglecting the effect of the curvature). With a more accurate approach, a kind of exact measurement, one subdivides the path into several portions; the algorithm is similar to that of Dijkstra (e.g., see Mitchel and Mount [
20]).
This study aimed to evaluate the accuracy and repeatability of facial scans obtained with a low-cost 3D camera and compare the direct measurements from patients’ faces with measurements from 3D facial images for use in dental medicine research.
Hypotheses are:
- (1)
Three dimensional (3D) facial scans are reproducible with high accuracy;
- (2)
The actual and computed measurements are consistent and interchangeable.
4. Discussion
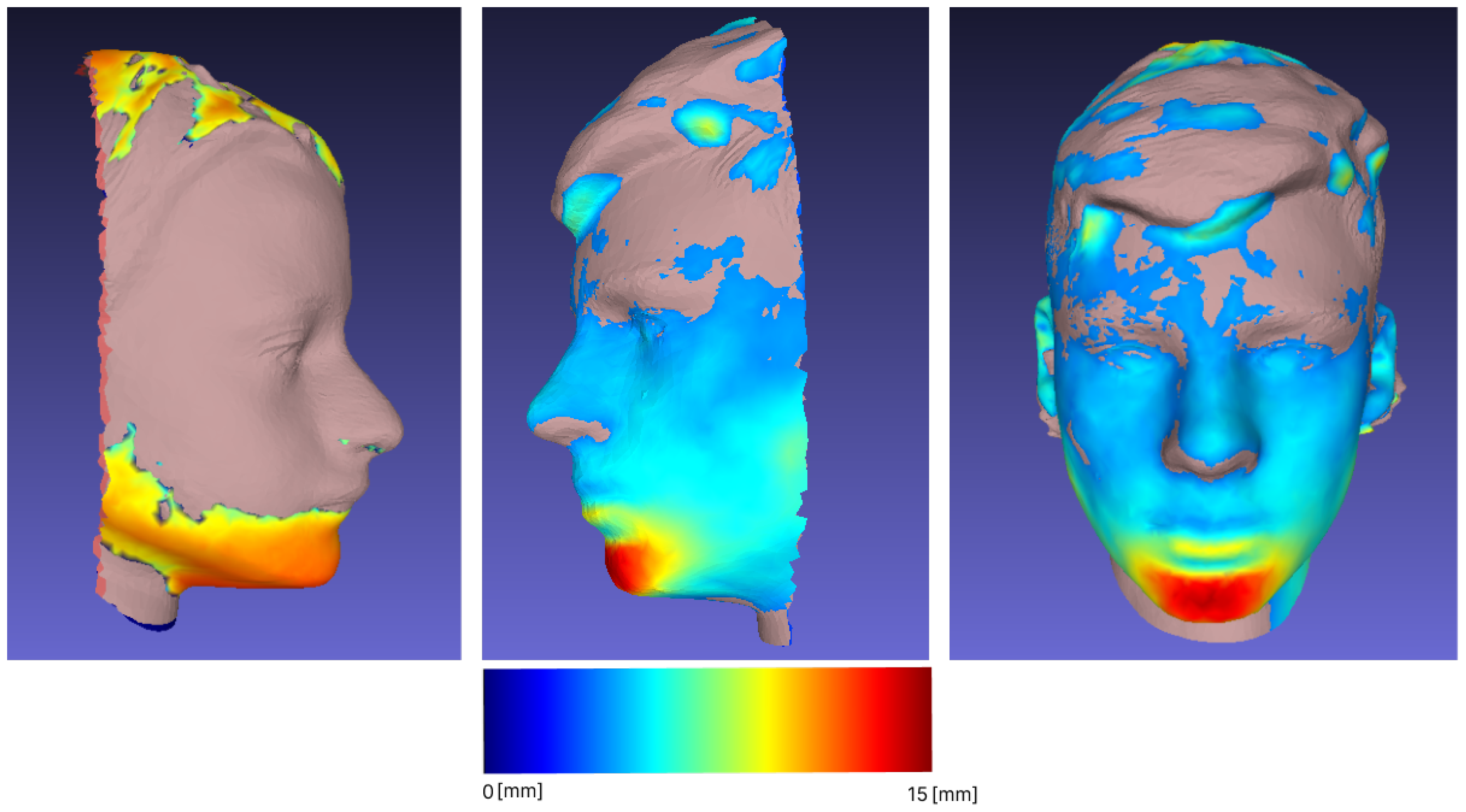
Our research has shown that 3D facial scans from low-cost scanners are reproducible with high accuracy (mean difference between repeated scans < 1%), our initial hypothesis was confirmed. Previous research [
13] reported accuracy between 0.2–1 mm for expensive scanners. In contrast, Gibelli et al. [
15] found that an inexpensive scanner they tested did not have satisfactory reproducibility (RMS point-to-point distances averaged 0.65 mm), but comparison of the volumes obtained was considered unsatisfactory. In all the aforementioned articles, the scans were manually or semi-manually adjusted before analysis. Usually, the part of the scan that contained the hair was cut off, and landmarks were manually placed on each scan or on each subject before scanning [
12,
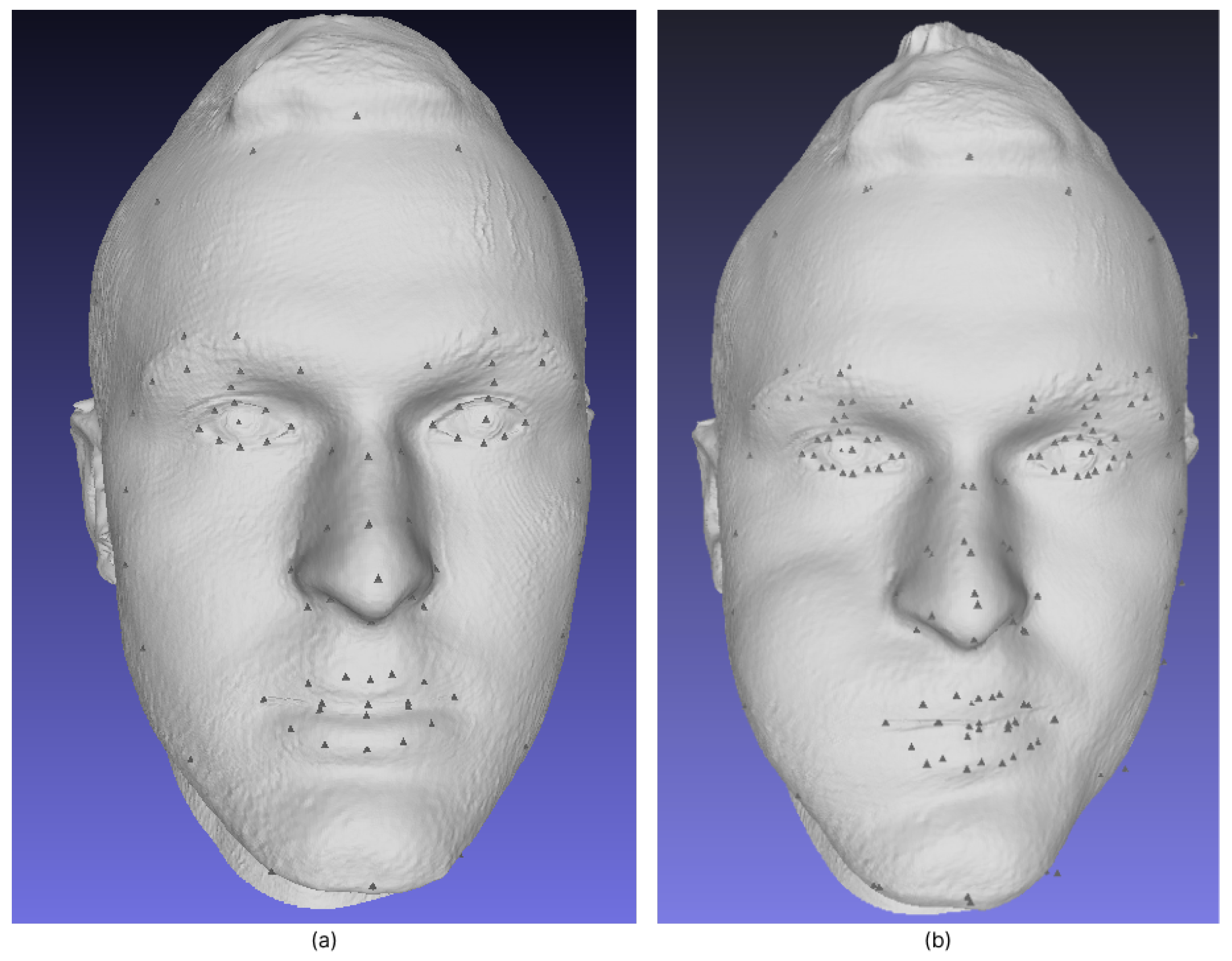
33]. Because these procedures can be time consuming, we attempted to analyse the scans with automated landmark tracking. Automated landmark tracking saves significant time. The tested 3D Bellus software sets a total of over 100 landmarks (ten landmarks for each eye, six landmarks for each eyebrow, fourteen landmarks for the nose, eighteen landmarks for the mouth, ten landmarks for the oblique line of the face, three landmarks for the chin, the trichion hair line, the gonial angle, and the soft tissue throat, and an additional six landmarks for the outer hairline and ten for each ear). As expected, the results became even more accurate when hair was excluded (from initial to after hair removal). Therefore, the use of a hair cover would improve the results without increasing the time needed for the analysis.
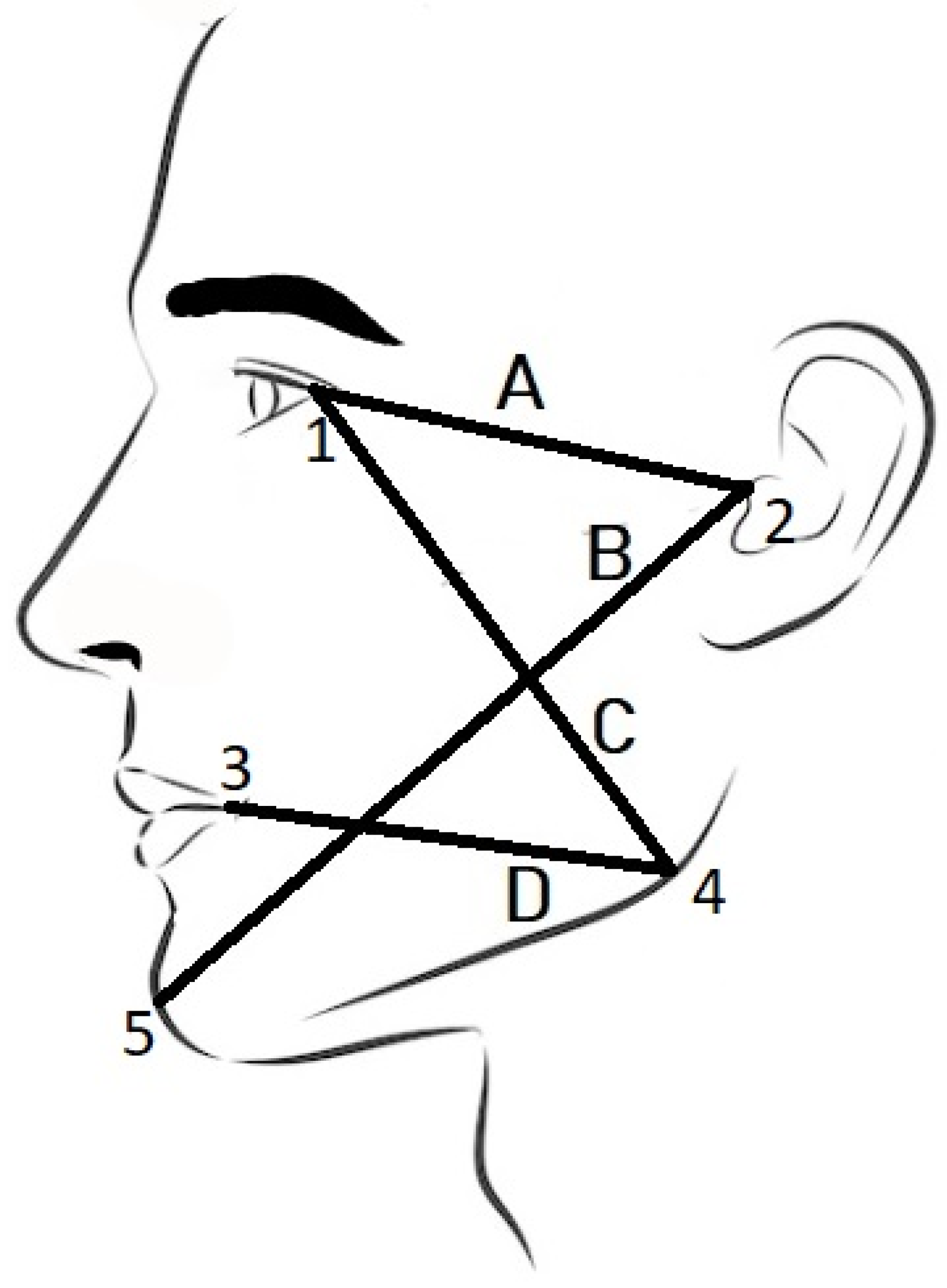
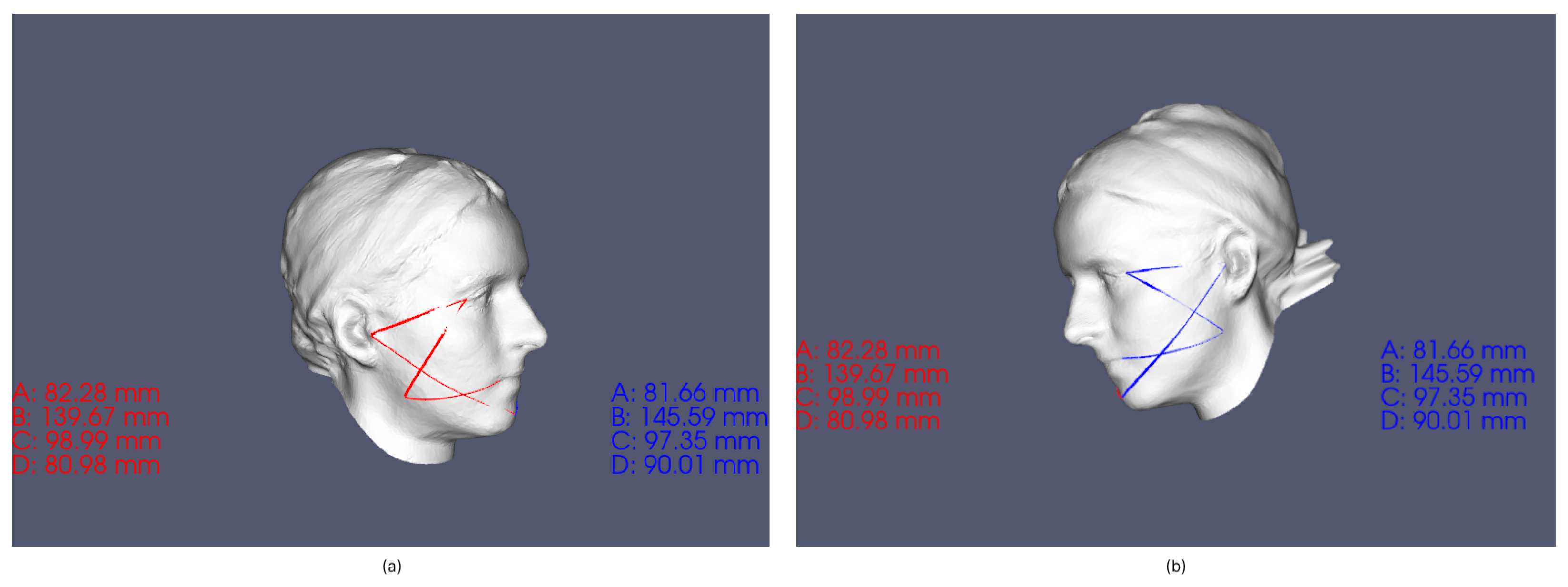
The second part of our research deals with the comparison between the computational and the physical measurement of demarcation lines. We chose four lines for measurement, shown in
Figure 2, namely
tragus—
lateral canthus of the eye (A);
tragus—
pogonion (B);
gonion—
lateral canthus of the eye (C);
gonion—
labial commissure (D). The physical measurements on the subjects showed excellent repeatability only for one demarcation line (tragus-pogonion). It was suggested that this demarcation line could be used in the evaluation of the post-operative swelling of the face, rather than a variety of the demarcation lines [
22], because of the long span across the area of the most pronounced swelling. Previous studies have shown that repeatability is better when longer spans are measured [
34]. Other demarcation lines showed lower repeatability, which could be due to the effect of facial expressions (slight movements are almost always present, especially in the eye and mouth areas) [
35,
36]. Additionally, discomfort due to physical contact between the subject’s skin (eye and mouth corners) and the measurement tape must have affected the repeatability; it is also more challenging to place the gonion landmark correctly. Furthermore, measurement of the left side of the face proved even more difficult for the right-handed operator; the poorest repeatability was reported for the demarcation lines of the left side of the face. Any discomfort caused by contact of the tape measure with the sensitive, hypersensitive skin at the corners of the eyes and mouth (resulting in blink reflexes and pinching of the lips) could be avoided by using virtual measurements on the 3D facial scans. However, involuntary blinking and lip curling may still occur during scanning. In these cases, the scanning process should be repeated. To our knowledge, there are no previous reports of measurement error on living subjects who participated in the studies of postoperative swelling after third molar surgery [
5,
37]. Repeated physical measurement showed deviations in the range of 0–10 [mm]. Although with considerable deviations, we took these measurements as a reference (ground truth). For the exact computational measurement over a triangular mesh, we used the “continuous” Dijsktra method proposed in [
20].
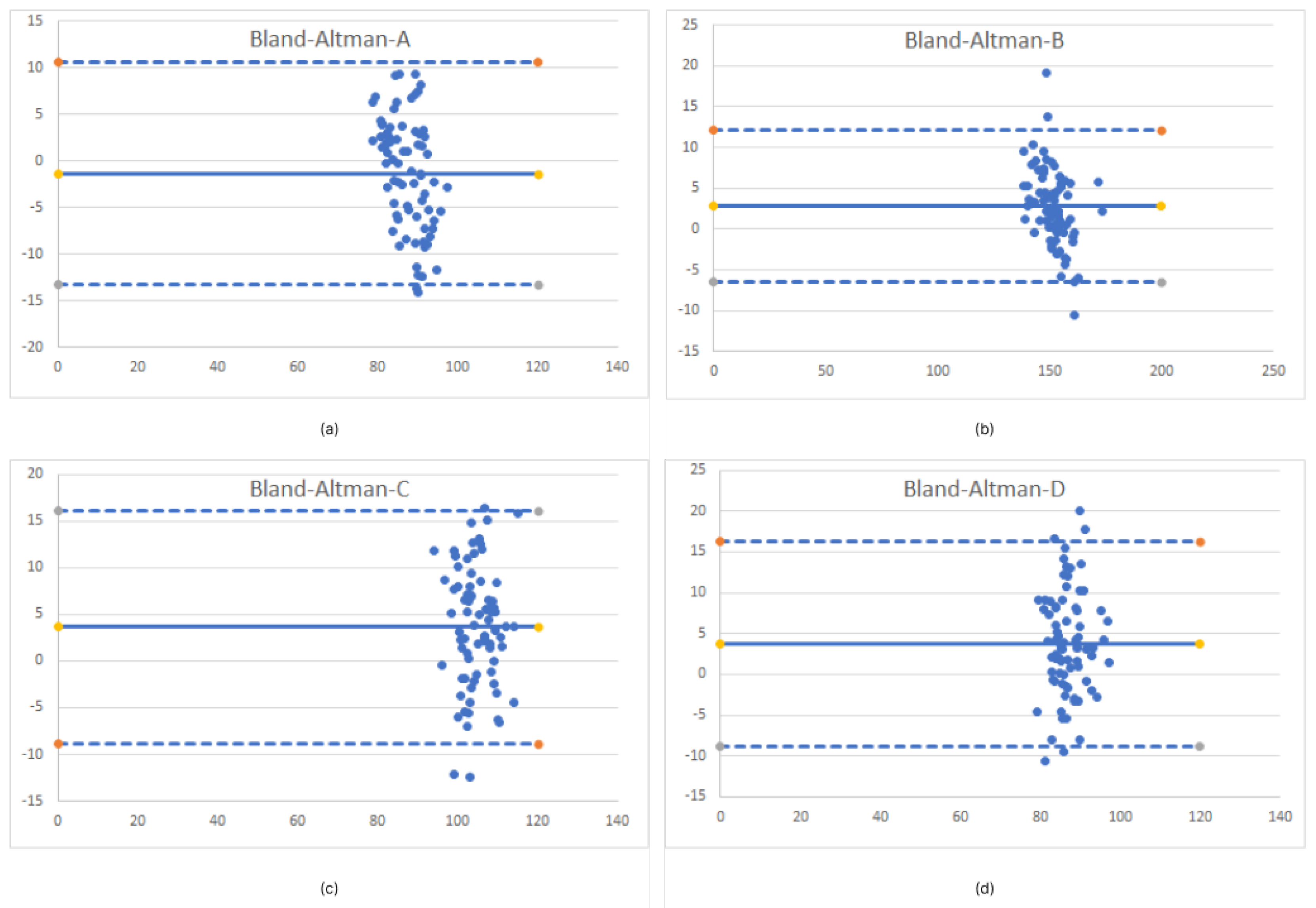
Our results for the computational measurement show a difference of <1 cm for demarcation lines A, B, and C. The largest deviation of >1cm from the ground truth measurement is for the D line. The lowest accuracy is limited not only by reflex movement of the lips, but also due to a lower quality selection of the gonion location; rather than a computer measurement error. The gonial angle is a location where the lower mandibular body meets the posterior border of the ramus [
38]. Due to the influence of the shape of the face and the amount of fat tissue, it can be challenging to choose an exact gonion position. Considering the experimental results obtained and taking into account the more demanding selection of the gonion location, we can conclude that the computer-based method provides reasonable accuracy. Furthermore, a big part of the measurement error is caused by initial settings. Initial measurement errors are represented by the number of triangles that build a 3D polygonal structure. If the mesh model is created from a smaller number of polygons, the lines that builds the surface area do not describe the real surface curvature. Therefore, it is desirable to have 3D meshes made of a greater number of polygons. Additionally, the precise selection of the source and destination points is also crucial step for computational measurement accuracy. To determine differences between the computational and physical measurements, we performed a two-tailed t-test. The result for the
p value of 0.31 shows that there is no statistical difference between the two groups and correlation of 0.973 strong association between two measurements. The limits of the agreements are determined for each of the four demarcation lines of the computational measurement. The visualization of such boundaries, here presented with the Bland–Altman diagram (shown in
Figure 5), brings us to conclusion that computer-aided measurement provides sufficient accuracy to provide clinically relevant results. The graph shows the less stringent limits for measuring the D line (the aforementioned challenges of actual measurement must be also taken into account, when discussing comparison of the two measurement methods).
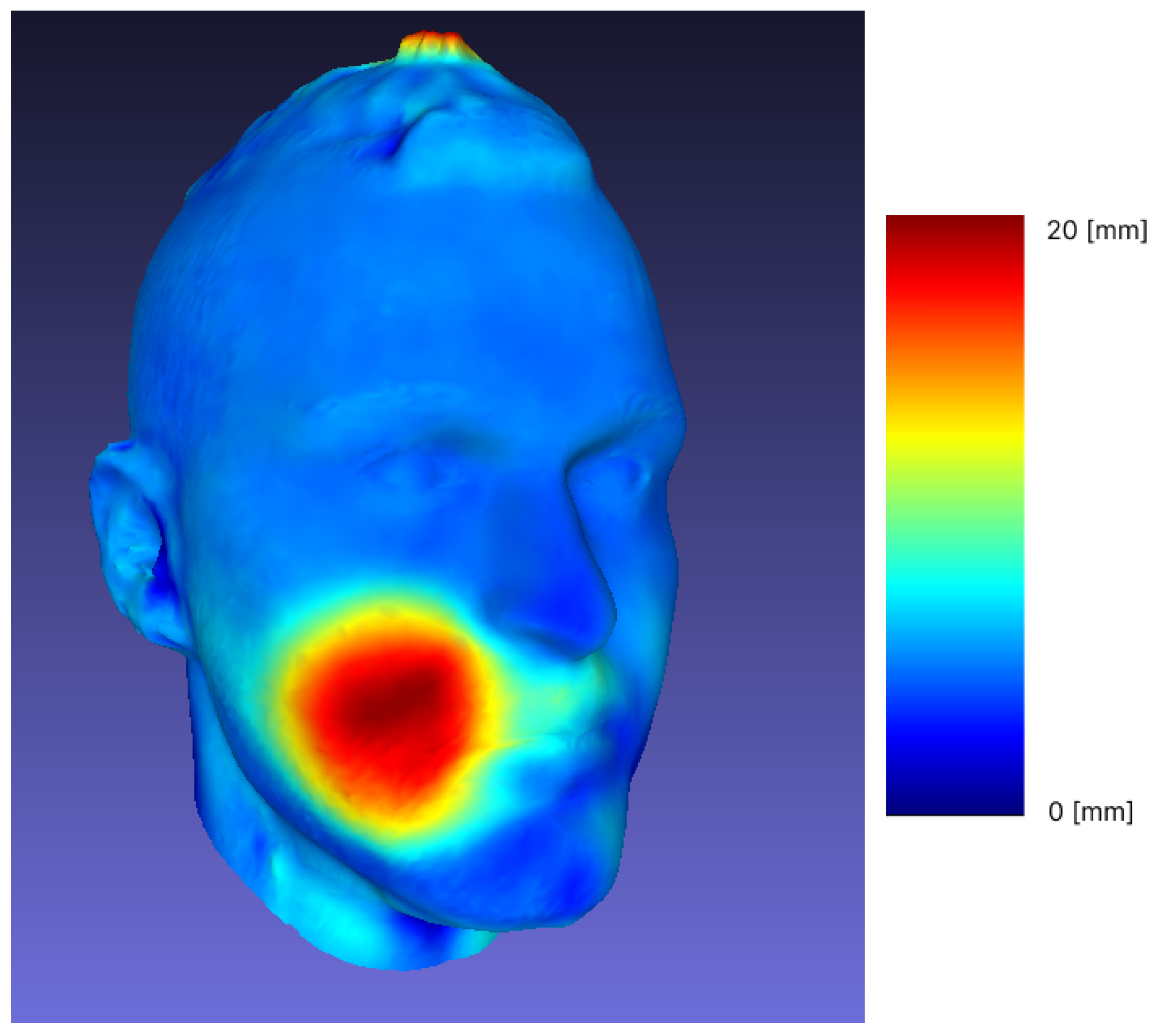
In the third part of our study, we examined the procedure of the Frankel manoeuvre (FM). The procedure of the projection of dental class I occlusion in the dental class II patients is called the Fränkel Manoeuvre (FM), and is often used in clinical decision making [
39]. If a soft tissue profile becomes more straight (from convex to less convex or straight, but not towards concave), it is advisable to try to gain, as much as possible, forward growth of the mandible with functional orthodontic appliances during the peak pubertal growth [
40]. Recording the initial state and comparing it to the projected goal (scanned FM) will enable better evaluation of the end result (after the treatment), also in comparison with the desired outcome (the FM). It is easier to monitor the change with a series of non-invasive 3D facial scans, as opposed to X-ray imaging [
4]. The overlap and matching (shown in
Figure 6) of different scans of the same individual subjected to FM show a significant change in the forward movement of the mandible, allowing further comparison and tracking of treatment progress, which would not be possible if we were limited to visualization with X-rays. At each follow-up of different dental procedures and for monitoring the changes, the 3D facial scans could be used and measurements could be taken with a minimum of additional time and discomfort for the patients, as the physical contact of the measuring tape with sensitive, prone to reflex contractions and potentially painful parts of the facial soft tissue is reduced.
5. Conclusions
The low-cost 3D facial scans are reproducible with high accuracy (mean difference between repeated scans <1%).
The physical measurements are dependent on landmark positioning, sensitivity of the measured area of skin, the measured length and the skill of the operator, but are still considered to be the ground truth; a comparison of computer and physical measurement results shows reasonable accuracy. Facial scans and computed measurements can be used instead of physical measurements.
Further advances for the future use of 3D facial scans are: contactless data acquisition and measuring, better non-invasive visualization in multiple time-points for various dental procedures influencing changes of the facial soft tissues.

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}