
Object Weight and Hand Dominance Impact Kinematics in a Functional Reach-to-Drink Task in School-Aged Children

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
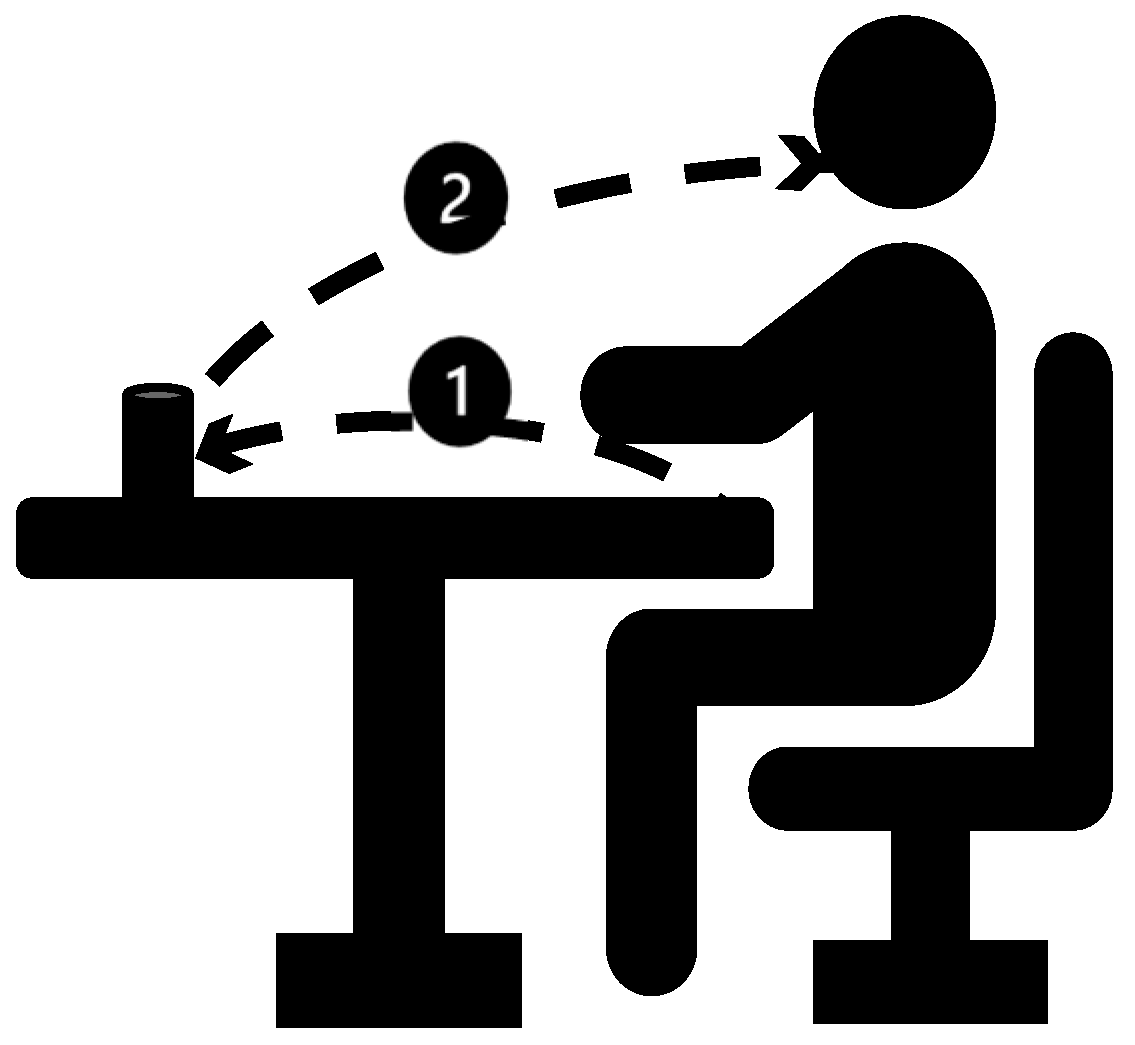
2.2. Procedure
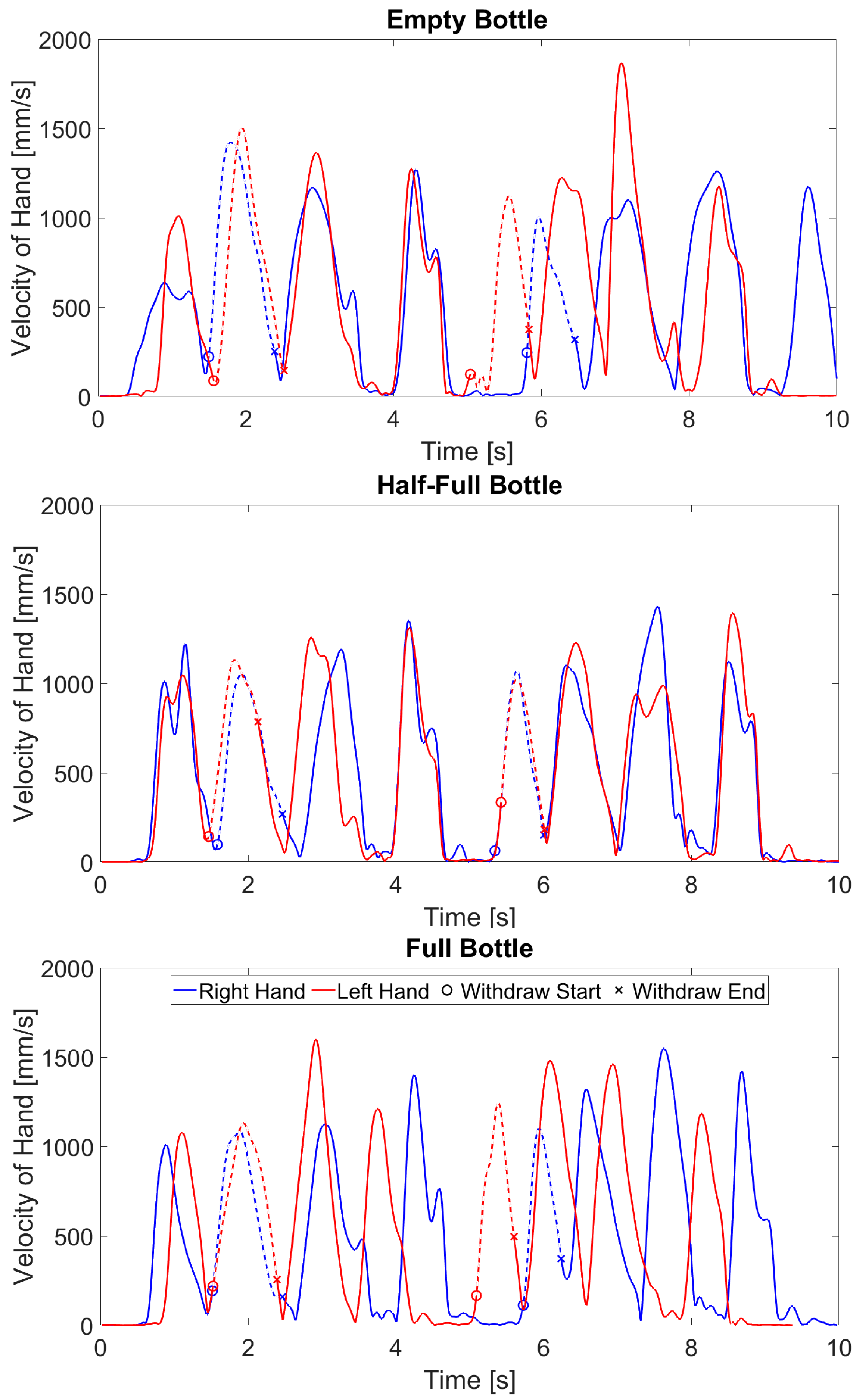
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Main Effects
4. Discussion
4.1. Object Constraints
4.2. Hand Dominance
4.3. Limitations and Future Directions
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Butler, E.E.; Ladd, A.L.; LaMont, L.E.; Rose, J. Temporal–spatial parameters of the upper limb during a Reach & Grasp Cycle for children. Gait Posture 2010, 32, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Coluccini, M.; Maini, E.S.; Martelloni, C.; Sgandurra, G.; Cioni, G. Kinematic characterization of functional reach to grasp in normal and in motor disabled children. Gait Posture 2007, 25, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Schneiberg, S.; Sveistrup, H.; McFadyen, B.; McKinley, P.; Levin, M.F. The development of coordination for reach-to-grasp movements in children. Exp. Brain Res. 2002, 146, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Domellöf, E.; Rösblad, B.; Rönnqvist, L. Impairment severity selectively affects the control of proximal and distal components of reaching movements in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2009, 51, 807–816. [Google Scholar] [CrossRef]
- van der Heide, J.C.; Begeer, C.; Fock, J.M.; Otten, B.; Stremmelaar, E.; Van Eykern, L.A.; Hadders-Algra, M. Postural control during reaching in preterm children with cerebral palsy. Dev. Med. Child Neurol. 2004, 46, 253–266. [Google Scholar] [CrossRef]
- Hung, Y.-C.; Henderson, E.R.; Akbasheva, F.; Valte, L.; Ke, W.S.; Gordon, A.M. Planning and coordination of a reach–grasp–eat task in children with hemiplegia. Res. Dev. Disabil. 2012, 33, 1649–1657. [Google Scholar] [CrossRef]
- Mackey, A.H.; Walt, S.E.; Stott, N.S. Deficits in upper-limb task performance in children with hemiplegic cerebral palsy as defined by 3-dimensional kinematics. Arch. Phys. Med. Rehabil. 2006, 87, 207–215. [Google Scholar] [CrossRef]
- Machado, L.; Heathcock, J.; Carvalho, R.; Pereira, N.; Tudella, E. Kinematic characteristics of arm and trunk when drinking from a glass in children with and without cerebral palsy. Clin. Biomech. 2019, 63, 201–206. [Google Scholar] [CrossRef]
- Buccino, G.; Arisi, D.; Gough, P.; Aprile, D.; Ferri, C.; Serotti, L.; Tiberti, A.; Fazzi, E. Improving upper limb motor functions through action observation treatment: A pilot study in children with cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 822–828. [Google Scholar] [CrossRef]
- Chen, Y.-P.; Pope, S.; Tyler, D.; Warren, G.L. Effectiveness of constraint-induced movement therapy on upper-extremity function in children with cerebral palsy: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2014, 28, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Friel, K.M.; Kuo, H.-C.; Fuller, J.; Ferre, C.L.; Brandão, M.; Carmel, J.B.; Bleyenheuft, Y.; Gowatsky, J.L.; Stanford, A.D.; Rowny, S.B.; et al. Skilled Bimanual Training Drives Motor Cortex Plasticity in Children With Unilateral Cerebral Palsy. Neurorehabilit. Neural Repair 2016, 30, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Hoare, B.; Wallen, M.; Thorley, M.; Jackman, M.; Carey, L.; Imms, C. Constraint-induced movement therapy in children with unilateral cerebral palsy (Review). Cochrane Database Syst. Rev. 2019, 4, CD004149. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Boyd, R.N. Efficacy of Upper Limb Therapies for Unilateral Cerebral Palsy: A Meta-analysis. Pediatrics 2014, 133, e175–e204. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Mc Namara, M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Thelen, E.; Smith, L.B. A Dynamic Systems Approach to the Development of Cognition and Action; MIT Press: Cambridge, MA, USA, 1994. [Google Scholar]
- Rönnqvist, L.; Domellöf, E. Quantitative Assessment of Right and Left Reaching Movements in Infants: A Longitudinal Study from 6 to 36 Months. Dev. Psychobiol. 2006, 48, 444–459. [Google Scholar] [CrossRef]
- Thelen, E.; Corbetta, D.; Spencer, J.P. Development of reaching during the first year: Role of movement speed. J. Exp. Psychol. Hum. Percept. Perform. 1996, 22, 1059–1076. [Google Scholar] [CrossRef]
- Bhat, A.; Galloway, J. Toy-oriented changes during early arm movements: Hand kinematics. Infant Behav. Dev. 2006, 29, 358–372. [Google Scholar] [CrossRef]
- Golenia, L.; Schoemaker, M.M.; Otten, E.; Mouton, L.J.; Bongers, R.M. What the Dynamic Systems Approach can offer for understanding development: An example of mid-childhood reaching. Front. Psychol. 2017, 8, 1774. [Google Scholar] [CrossRef]
- Rosenbaum, D.A.; Chapman, K.M.; Weigelt, M.; Weiss, D.J.; van der Wel, R. Cognition, action, and object manipulation. Psychol. Bull. 2012, 138, 924–946. [Google Scholar] [CrossRef]
- Janssen, L.; Beuting, M.; Meulenbroek, R.G.J.; Steenbergen, B. Combined effects of planning and execution constraints on bimanual task performance. Exp. Brain Res. 2009, 192, 61–73. [Google Scholar] [CrossRef]
- Hughes, C.M.; Reißig, P.; Seegelke, C. Motor planning and execution in left- and right-handed individuals during a bimanual grasping and placing task. Acta Psychol. 2011, 138, 111–118. [Google Scholar] [CrossRef]
- de Bruin, N.; Sacrey, L.-A.R.; Brown, L.A.; Doan, J.; Whishaw, I.Q. Visual guidance for hand advance but not hand withdrawal in a reach-to-eat task in adult humans: Reaching is a composite movement. J. Mot. Behav. 2008, 40, 337–346. [Google Scholar] [CrossRef]
- Sacrey, L.-A.R.; Whishaw, I.Q. Subsystems of sensory attention for skilled reaching: Vision for transport and pre-shaping and somatosensation for grasping, withdrawal and release. Behav. Brain Res. 2012, 231, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, B.; Hulstijn, W.; Dortmans, S. Constraints on grip selection in cerebral palsy. Exp. Brain Res. 2000, 134, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, B. Review Activity limitation in hemiplegic cerebral palsy: Evidence for disorders in motor planning. Dev. Med. Child Neurol. 2006, 48, 780–783. [Google Scholar] [CrossRef] [PubMed]
- Flindall, J.W.; Doan, J.B.; Gonzalez, C.L.R. Manual asymmetries in the kinematics of a reach-to-grasp action. Laterality 2014, 19, 489–507. [Google Scholar] [CrossRef]
- Steenbergen, B.; Marteniuk, R.G.; Kalbfleisch, L.E. Achieving Coordination in Prehension: Joint Freezing and Postural Contributions. J. Mot. Behav. 1995, 27, 333–348. [Google Scholar] [CrossRef]
- Berthier, N.E.; Clifton, R.K.; Gullapalli, V.; McCall, D.D.; Robin, D.J. Visual Information and Object Size in the Control of Reaching. J. Mot. Behav. 1996, 28, 187–197. [Google Scholar] [CrossRef]
- Gentilucci, M. Object motor representation and reaching–grasping control. Neuropsychologia 2002, 40, 1139–1153. [Google Scholar] [CrossRef]
- Kudoh, N.; Hattori, M.; Numata, N.; Maruyama, K. An analysis of spatiotemporal variability during prehension movements: Effects of object size and distance. Exp. Brain Res. 1997, 117, 457–464. [Google Scholar] [CrossRef]
- Benson, S.M.S.; Roy, E.A.; Bryden, P.J. End-state comfort in two object manipulation tasks: Investigating how the movement context influences planning in children, young adults, and older adults. Dev. Psychobiol. 2018, 60, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Scharoun, S.M.; Gonzalez, D.A.; Roy, E.A.; Bryden, P.J. End-state comfort across the lifespan: A cross-sectional investigation of how movement context influences motor planning in an overturned glass task. Mot. Control 2018, 22, 211–230. [Google Scholar] [CrossRef] [PubMed]
- Seegelke, C.; Hughes, C.M.L.; Schack, T. An investigation into manual asymmetries in grasp behavior and kinematics during an object manipulation task. Exp. Brain Res. 2011, 215, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.L.; Berthier, N.E.; Konidaris, G.D. Handedness and Reach-to-Place Kinematics in Adults: Left-Handers Are Not Reversed Right-Handers. J. Mot. Behav. 2018, 50, 381–391. [Google Scholar] [CrossRef]
- Mazzarella, J.; Richie, D.; Chaudhari, A.M.W.; Tudella, E.; Spees, C.K.; Heathcock, J.C. Task-Related Differences in End-Point Kinematics in School-Age Children with Typical Development. Behav. Sci. 2023, 13, 528. [Google Scholar] [CrossRef]
- Bryden, P.J.; Roy, E. Preferential reaching across regions of hemispace in adults and children. Dev. Psychobiol. 2006, 48, 121–132. [Google Scholar] [CrossRef]
- Annett, M. The Growth of Manual Preference and Speed. Br. J. Psychol. 1970, 61, 545–558. [Google Scholar] [CrossRef]
- Curt, F.; Maccario, J.; Dellatolas, G. Distributions of Hand Preference and Hand Skill Asymmetry in Preschool Children: Theoretical Implications. Neuropsychologia 1992, 30, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Brito, G.N.O.; Lins, M.F.C.; Paumgartten, F.J.R.; Brito, L.S.O. Hand Preference in 4- to 7-Year-Old Children: An Analysis with the Edinburgh Inventory in Brazil. Dev. Neuropsychol. 1992, 8, 59–68. [Google Scholar] [CrossRef]
- Nelson, E.L.; Konidaris, G.D.; Berthier, N.E. Hand preference status and reach kinematics in infants. Infant Behav. Dev. 2014, 37, 615–623. [Google Scholar] [CrossRef]
- Lynch, A.; Lee, H.M.; Bhat, A.; Galloway, J.C. No stable arm preference during the pre-reaching period: A comparison of right and left hand kinematics with and without a toy present. Dev. Psychobiol. 2008, 50, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Kahrs, B.A.; Jung, W.P.; Lockman, J.J. When Does Tool Use Become Distinctively Human? Hammering in Young Children. Child Dev. 2014, 85, 1050–1061. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Such-Neibar, T. Cerebral palsy diagnosis and management: The state of the art. Curr. Probl. Pediatr. Adolesc. Health Care 2003, 33, 146–169. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Tafone, S.; Lo, W.; Heathcock, J.C. Perinatal stroke causes abnormal trajectory and laterality in reaching during early infancy. Res. Dev. Disabil. 2015, 38, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, J.; McNally, M.; Chaudhari, A.M.; Pan, X.; Heathcock, J.C. Differences in coordination and timing of pre-reaching upper extremity movements may be an indicator of cerebral palsy in infants with stroke: A preliminary investigation. Clin. Biomech. 2020, 73, 181–188. [Google Scholar] [CrossRef]
- Mazzarella, J.; McNally, M.; Richie, D.; Chaudhari, A.M.W.; Buford, J.A.; Pan, X.; Heathcock, J.C. 3D Motion Capture May Detect Spatiotemporal Changes in Pre-Reaching Upper Extremity Movements with and without a Real-Time Constraint Condition in Infants with Perinatal Stroke and Cerebral Palsy: A Longitudinal Case Series. Sensors 2020, 20, 7312. [Google Scholar] [CrossRef]
- Guzzetta, A.; Pizzardi, A.; Belmonti, V.; Boldrini, A.; Carotenuto, M.; D’acunto, G.; Ferrari, F.; Fiori, S.; Gallo, C.; Ghirri, P.; et al. Hand movements at 3 months predict later hemiplegia in term infants with neonatal cerebral infarction. Dev. Med. Child Neurol. 2010, 52, 767–772. [Google Scholar] [CrossRef]
- Grosskopf, A.; Kuhtz-Buschbeck, J.P. Grasping with the left and right hand: A kinematic study. Exp. Brain Res. 2006, 168, 230–240. [Google Scholar] [CrossRef]
- Butler, E.E.; Ladd, A.L.; Louie, S.A.; LaMont, L.E.; Wong, W.; Rose, J. Three-dimensional kinematics of the upper limb during a Reach and Grasp Cycle for children. Gait Posture 2010, 32, 72–77. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; dos Santos, G.L.; Jaspers, E.; Vanderschueren, R.; Mailleux, L.; Klingels, K.; Ortibus, E.; Desloovere, K.; Feys, H. Age-related changes in upper limb motion during typical development. PLoS ONE 2018, 13, e0198524. [Google Scholar] [CrossRef]
- Vicon Motion Systems Ltd. Vicon Nexus v2; Vicon Motion Systems Ltd.: Oxford, UK, 2015. [Google Scholar]
- The MathWorks Inc. MATLAB (R2020b); The MathWorks Inc.: Natick, MA, USA, 2020. [Google Scholar]
- Balasubramanian, S.; Melendez-Calderon, A.; Burdet, E. A Robust and Sensitive Metric for Quantifying Movement Smoothness. IEEE Trans. Biomed. Eng. 2012, 59, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.; Poggiali, D.; Whitaker, K.; Marshall, T.R.; Kievit, R.A. Raincloud plots: A multi-platform tool for robust data visualization. Wellcome Open Res. 2019, 4, 63. [Google Scholar] [CrossRef] [PubMed]
- Latash, M.L.; Jaric, S. Organization of Drinking: Postural Characteristics of Arm-Head Coordination. J. Mot. Behav. 2002, 34, 139–150. [Google Scholar] [CrossRef]
- Gonzalez, C.L.R.; Ganel, T.; Goodale, M.A. Hemispheric Specialization for the Visual Control of Action Is Independent of Handedness. J. Neurophysiol. 2006, 95, 3496–3501. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, B.; Meulenbroek, R.G.; Rosenbaum, D.A. Constraints on grip selection in hemiparetic cerebral palsy: Effects of lesional side, end-point accuracy, and context. Cogn. Brain Res. 2004, 19, 145–159. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Bottle Size (Diameter × Height (cm)) | Weight (g) |
|---|---|---|
| Empty | 6.2 × 14 | 31.5 |
| Half | 187.9 | |
| Full | 346.5 |
| Variable | Units | Description | Calculation |
|---|---|---|---|
| Average Speed | mm/s | Average velocity during the withdrawal movement | Velocity was calculated at each position of the hand marker cluster using a 4-point central difference numerical differentiation, then averaged across the movement |
| Peak Velocity | mm/s | Peak velocity reached during the withdrawal movement | Velocity was calculated at each position of the hand marker cluster using a 4-point central difference numerical differentiation |
| Straightness Ratio | ratio | a value closer to one indicates a straighter movement | Hand path length/straight line distance from start to end of the movement |
| Number of Velocity Peaks | count | Fewer velocity peaks indicate a smoother movement | Number of velocity peaks in a movement, with a peak defined as a change > 100 mm/s |
| Log Dimensionless Jerk | no units | Measures smoothness of movement, with less negative values indicating a smoother movement | The negative natural logarithm of the squared absolute value of jerk multiplied with the trial duration to the power of three and divided by the squared peak velocity [55] |
| Effects | Bottle Fill | Hand | Bottle Fill * Hand | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Num DF | 2 | 1 | 2 | ||||||
| Den DF | 60 | 30 | 60 | ||||||
| Variables | F | Sig | η2p | F | Sig | η2p | F | Sig | η2p |
| Average Velocity (mm/s) | 4.58 | 0.01 * | 0.13 | 5.80 | 0.02 * | 0.28 | 0.01 | 0.99 | 0.0003 |
| Peak Velocity (mm/s) | 5.34 | 0.007 * | 0.15 | 7.31 | 0.01 * | 0.33 | 1.69 | 0.19 | 0.05 |
| Straightness Ratio | 0.73 | 0.48 | 0.02 | 0.01 | 0.93 | 0.001 | 0.66 | 0.52 | 0.02 |
| Number of Velocity Peaks | 3.00 | 0.06 | 0.09 | 0.88 | 0.36 | 0.06 | 0.67 | 0.51 | 0.02 |
| Log Dimensionless Jerk | 1.90 | 0.16 | 0.06 | 1.01 | 0.32 | 0.06 | 0.55 | 0.58 | 0.02 |
| Bottle Fill | |||||
|---|---|---|---|---|---|
| Variable | Hand | Empty | Half | Full | Average of Fills |
| Average Velocity (mm/s) 1,2 | Dominant | 540.4 (147.0) | 503.6 (149.1) | 531.5 (124.1) | 525.2 (140.7) 1 |
| Non-dominant | 560.3 (137.3) | 520.6 (142.6) | 549.4 (154.6) | 543.5 (145.2) 1 | |
| Average of Both Hands | 550.4 (142.0) 2 | 512.1 (145.6) 2 | 540.5 (139.9) | ||
| Peak Velocity (mm/s) 1,2 | Dominant | 885.5 (234.3) | 829.0 (212.9) | 877.9 (175.0) | 864.1 (209.2) 1 |
| Non-dominant | 947.0 (231.6) | 856.4 (183.4) | 886.2 (195.9) | 896.5 (207.0) 1 | |
| Average of Both Hands | 916.3 (234.0) 2 | 842.7 (198.4) 2 | 882.0 (185.0) | ||
| Straightness Ratio | Dominant | 1.042 (0.035) | 1.050 (0.049) | 1.045 (0.038) | 1.045 (0.041) |
| Non-dominant | 1.047 (0.046) | 1.048 (0.052) | 1.040 (0.040) | 1.045 (0.046) | |
| Average of Both Hands | 1.044 (0.041) | 1.049 (0.050) | 1.042 (0.039) | ||
| Number of Velocity Peaks | Dominant | 1.19 (0.43) | 1.29 (0.52) | 1.21 (0.45) | 1.23 (0.47) |
| Non-dominant | 1.22 (0.45) | 1.40 (0.58) | 1.19 (0.43) | 1.27 (0.50) | |
| Average of Both Hands | 1.21 (0.44) | 1.34 (0.55) | 1.20 (0.44) | ||
| Log Dimensionless Jerk | Dominant | −10.36 (0.72) | −10.60 (0.95) | −10.47 (0.80) | −10.48 (0.83) |
| Non-dominant | −10.51 (0.87) | −10.66 (0.92) | −10.45 (0.89) | −10.54 (0.90) | |
| Average of Both Hands | −10.41 (0.80) | −10.63 (0.93) | −10.46 (0.84) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzarella, J.; Richie, D.; Chaudhari, A.M.W.; Pan, X.; Tudella, E.; Spees, C.K.; Heathcock, J.C. Object Weight and Hand Dominance Impact Kinematics in a Functional Reach-to-Drink Task in School-Aged Children. Sensors 2024, 24, 5421. https://doi.org/10.3390/s24165421
Mazzarella J, Richie D, Chaudhari AMW, Pan X, Tudella E, Spees CK, Heathcock JC. Object Weight and Hand Dominance Impact Kinematics in a Functional Reach-to-Drink Task in School-Aged Children. Sensors. 2024; 24(16):5421. https://doi.org/10.3390/s24165421
Chicago/Turabian StyleMazzarella, Julia, Daniel Richie, Ajit M. W. Chaudhari, Xueliang Pan, Eloisa Tudella, Colleen K. Spees, and Jill C. Heathcock. 2024. "Object Weight and Hand Dominance Impact Kinematics in a Functional Reach-to-Drink Task in School-Aged Children" Sensors 24, no. 16: 5421. https://doi.org/10.3390/s24165421