Abstract
In the rapidly evolving landscape of continuous electrocardiogram (ECG) monitoring systems, there is a heightened demand for non-invasive sensors capable of measuring ECGs and detecting heart rate variability (HRV) in diverse populations, ranging from cardiovascular patients to sports enthusiasts. Challenges like device accuracy, patient privacy, signal noise, and long-term safety impede the use of wearable devices in clinical practice. This scoping review aims to assess the performance and safety of novel multi-channel, sensor-based biopotential wearable devices in adults. A comprehensive search strategy was employed on four databases, resulting in 143 records and the inclusion of 12 relevant studies. Most studies focused on healthy adult subjects (n = 6), with some examining controlled groups with atrial fibrillation (AF) (n = 3), long QT syndrome (n = 1), and sleep apnea (n = 1). The investigated bio-sensor devices included chest-worn belts (n = 2), wrist bands (n = 2), adhesive chest strips (n = 2), and wearable textile smart clothes (n = 4). The primary objective of the included studies was to evaluate device performance in terms of accuracy, signal quality, comparability, and visual assessment of ECGs. Safety findings, reported in five articles, indicated no major side effects for long-term/continuous monitoring, with only minor instances of skin irritation. Looking forward, there are ample opportunities to enhance and test these technologies across various physical activity intensities and clinical conditions.
1. Introduction
Cardiovascular diseases (CVDs) cross geographic, socioeconomic, or gender boundaries [1]. Developed and lower-/middle-income countries have a higher prevalence of cardiovascular risk factors, incidences of CVD and stroke, and all-cause mortality [1,2]. Additionally, the 2015 Update on Heart Disease and Stroke Statistics by the American Heart Association (AHA) highlighted that both CVD and stroke are the leading causes of health and economic burden in the US and worldwide. According to the World Health Organization (WHO), CVDs are the primary cause of global mortality, with 17.9 million deaths per year. The reported number of CVD deaths is expected to reach >23.6 million by 2030, up from 17.3 million in 2015 [3].
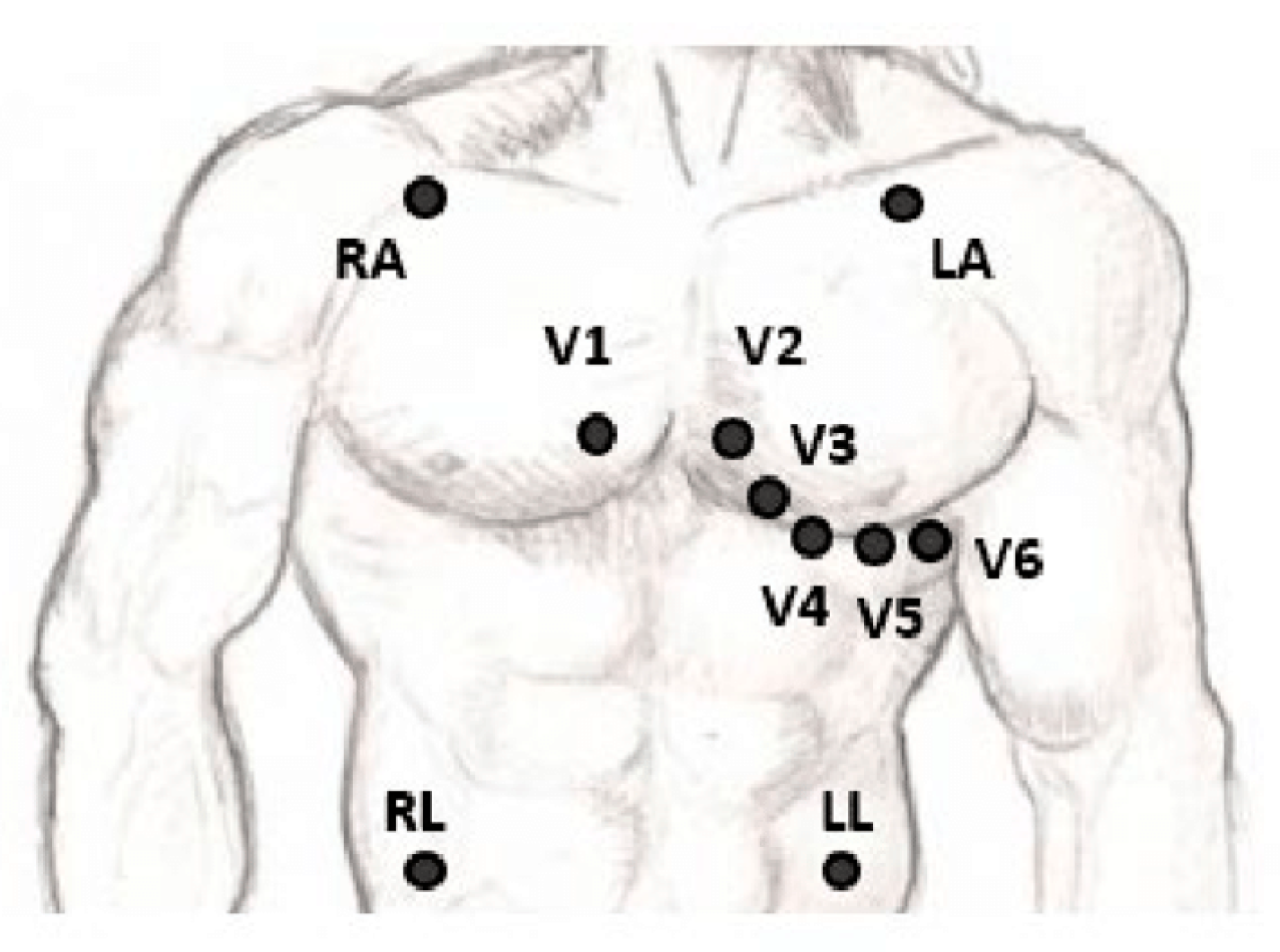
Electrocardiograms (ECGs) have become a routine part of any complete medical evaluation and have been used as a diagnostic test since their discovery over 70 years ago. As an ECG provides a waveform showing the electrical activity through the cardiac muscles, many but not all types of damage to the heart tissue can be detected by the ECG [4]. The gold standard 12-lead ECG configuration with its three bipolar limb leads (I, II, and III), three unipolar augmented leads (aVL, aVR, and aVF), six unipolar chest leads (V1–V6), and a reference electrode, as shown in Figure 1, gives spatial information about the cardiac electrical activity [5]. A vital clinical utility of ECG measurement is in detecting acute and chronic myocardial infarction, helping to differentiate coronary artery chest pain from non-cardiac chest pain. Another common diagnostic role is in the identification and management of arrhythmias localizing supraventricular and ventricular arrhythmias [6]. Other cardiovascular diseases, such as myocarditis, pericarditis, and structural deformities, and non-cardiovascular diseases, including hyperthyroidism and hypothyroidism, electrolyte imbalance, and pulmonary embolisms, can manifest as alterations of the ECG curve [7].
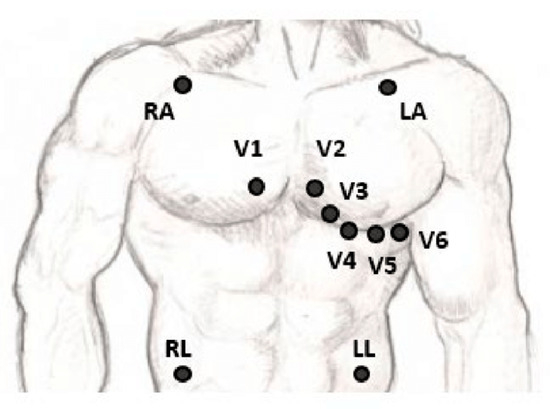
Figure 1.
The placement of the leads in a standard 12-lead ECG [5].
Currently, ECG monitoring is being used in hospitals (e.g., ICUs, wards, and clinics), homes (telemonitoring, outpatient ambulatory monitoring, and elderly people continuous monitoring at home), and remotely (real-time monitoring, self-diagnosis, and activity monitoring [8]. Some clinical indications for which short intermittent or continuous ECG monitoring has been used are medical drug monitoring, cardiac stress testing, sports performance, fetal ECG, pre-operative assessment, and in operative patients under general anesthesia [9,10,11]. ECG monitoring has been used as a tool for proactive health monitoring by tracking the physiological changes in non-clinical high-stress environments such as deep-sea explorations, wearables in construction, high-altitude environments, and long-duration space exploration missions, with the goal of leveraging ECGs for the early detection of cardiovascular issues and timely intervention [12,13].
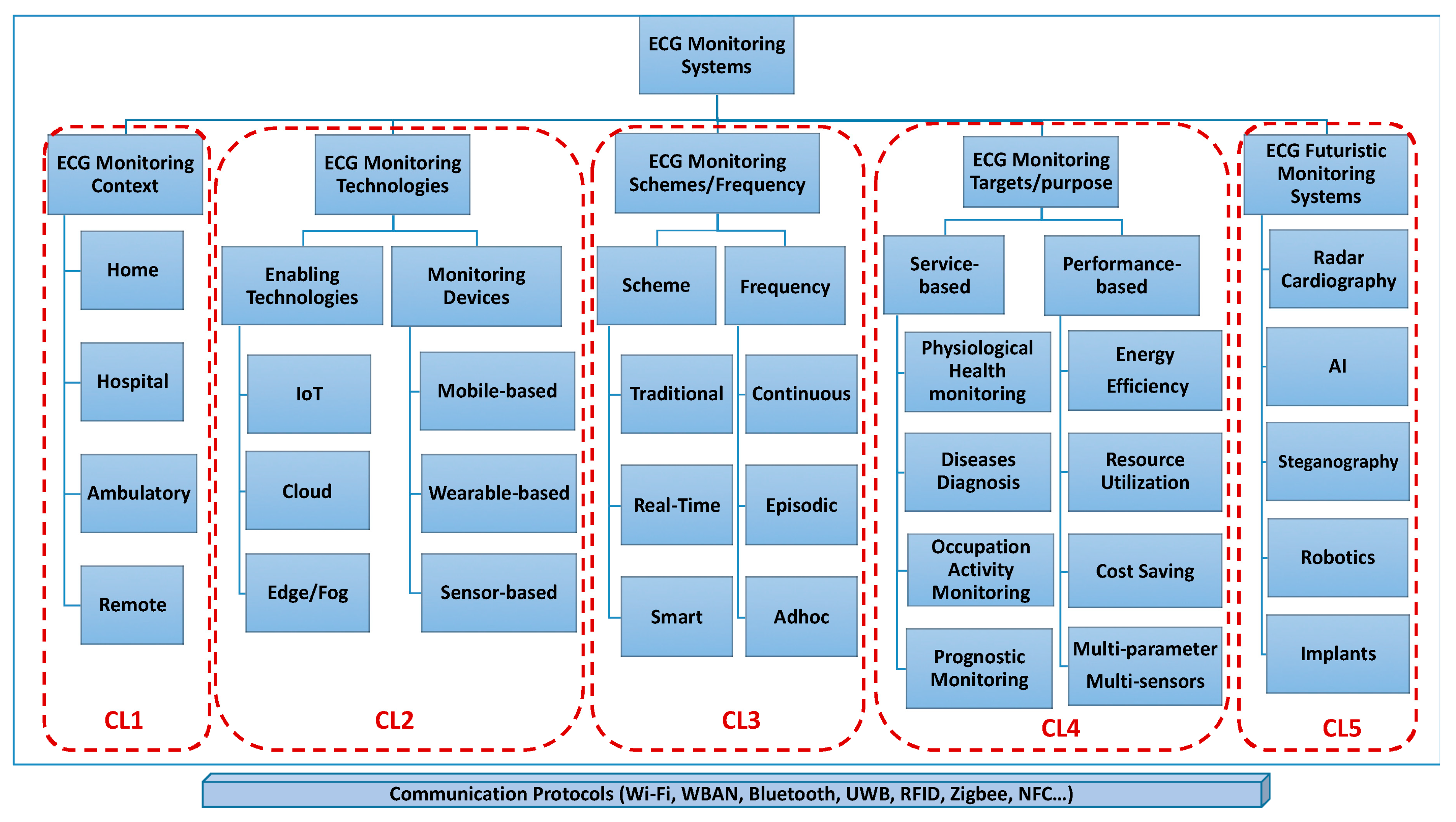
In the past few decades, ECG monitoring systems have been developed, evolved, and are widely used in the healthcare system. ECG monitoring systems are medical devices designed to record and display the electrical activity of the heart over a period of time. There is worldwide demand for a continuous health monitoring system that can detect heart rate variability through which cardiovascular diseases (accounting for 48% of non-communicable disease deaths, as per 2012 WHO Statistics) can be diagnosed and cured at an early stage [14]. Serhani et al. (2020) defined a taxonomy of ‘clusters’ for ECG monitoring systems (EMSs) as Context-aware EMS, Technology-aware EMS, EMS based on Schemes and Frequency, EMS Targets and Purposes, and Futuristic EMS, as shown in Figure 2. The second cluster of technology-aware individuals emphasized wearable devices integrated within an ambulatory, home, or patient/user setup, providing the means for the wireless monitoring of cardiovascular health [8].
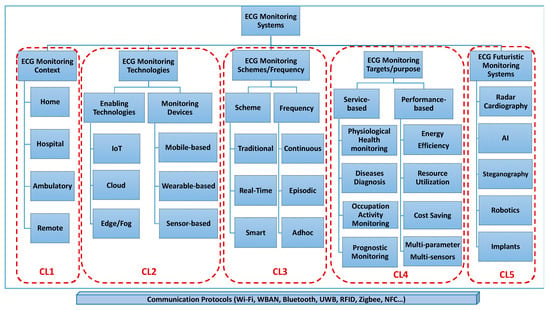
Figure 2.
ECG monitoring system clustering (used with permission) [8].
Wearable ECG devices could be in the form of an ‘on-body patch’ or a contact-less sensor as a smart watch, ‘textile-base’ vest, or capacitive sensors integrated within patients’ stretchers, beds, and wheelchairs [8]. Regardless of the type of sensor, these EMSs integrate with the device to record and retrieve the ECG signals and conduct processing to present a trackable outcome. Prieto-Avalos et al. (2022) reviewed the commercial and non-commercial wearable devices for the physical monitoring of the heart, and they concluded that the majority of such devices have ECG monitoring capacity along with other data; however, improvement in the user’s health is limited without healthy personal habits [15]. Table 1 categorizes these wearable devices with ECG monitoring capacity using either single-lead or multi-lead continuous or real-time ECG. Heart rate during rest and activity can be calculated through the ECG or photoplethysmography (PPG) sensors by calculating beat-to-beat time intervals.

Table 1.
Commercial wearable devices for ECG measurement and their FDA status [15,16].
The wearable wireless ECG devices are designed as a system of electrodes, an analog front-end (AFE), a data acquisition (DAQ) system, a digital signal processing (DSP) unit, wireless communication technology such as Bluetooth, IR, WiFi, and power consumption [8,17,18]. Although many ambulatory ECG monitoring systems have been commercialized to date, a major problem is still faced due to patients/athletes performing motion-related activities that introduce unwanted signal noise that makes monitoring less effective [19]. The frequency spectrum of the motion artifact overlaps the ECG; therefore, it is the most difficult form of noise to be removed [20]. A recent systematic review discussed the challenges of the present monitoring systems, which are rich in diversity and variability. The key challenges identified were manual static screening, the need to learn device operations at the user’s end, the effect on signal quality during real-time long-term monitoring, data processing, analysis and interpretation for the amount of data generated, sensor type and size and designs to keep it user-friendly, and being biocompatible for long-term monitoring [8,17]. Moreover, advances in mobile operating systems and the emergence of artificial intelligence bring their own benefits and challenges [15].
A scoping review is the best choice when the research questions are broad-identifying main concepts, theories, and knowledge gaps in a body of literature and systematically reviewing the data qualitatively [18,21]. We chose to go with the scoping review methodology to review and summarize the evidence on the performance and safety of multi-channel, sensor-based biopotential wearable devices in adults, providing direction for our future research work, where ‘performance’ will be defined based on accuracy, signal quality, comparability to the gold standard, visual assessment, and ‘safety’ as any side effect or adverse reaction on short- or long-term monitoring.
2. Methods
This scoping review used the framework provided by Tricco et al. as the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [21]. We initiated the review process by developing a review protocol stating the objectives and screening strategies. The Methods Section is organized into five steps: (1) identifying the research question; (2) identifying the relevant studies; (3) study selection; (4) charting the data; and (5) clinical data appraisal, collating, summarizing, and reporting results.
2.1. Identifying Research Questions
What is the extent of the scientific literature on monitoring ECGs with multichannel biopotential wearable devices in adults?
We sought to gather information based on the following research questions: (i) determine how the new technologies were designed; (ii) are these devices validated against the gold standard (12-lead ECG); and (iii) screen the selected research for performance and safety outcomes.
2.2. Identifying the Relevant Studies
The evaluation was carried out to provide a broader search of the existing literature and a comprehensive description of a given theme, allowing for the identification of gaps in scientific knowledge. The literature was assessed to determine whether the evidential data were sufficient for clinical evaluation. A P.I.C.O. strategy was defined as follows:
- Population: adults (>19 years), all genders, with or without cardiac irregularities.
- Intervention: Multichannel biopotential wearable device (Datalogger).
- Context/comparison: 12-lead ECGs or other variants of ECGs.
- Outcome (endpoints): ECG and heart rate variability (HRV).
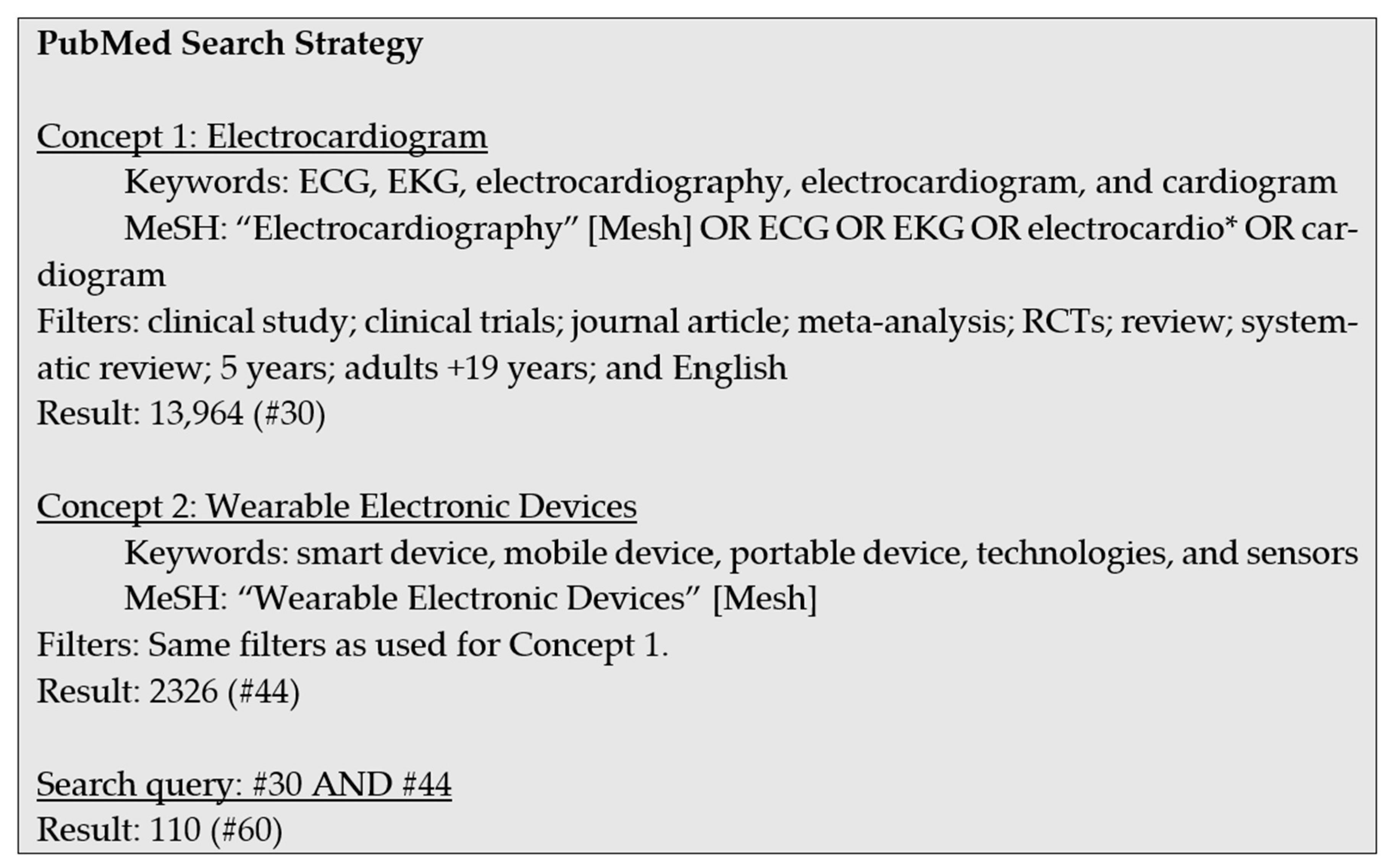
The literature search methodology was based on the identified PICO strategy. The search was conducted in January 2021. The search was made from databases such as PubMed, Cochrane, EMBASE, and CINAHL. For each database, concepts were identified, and the possible keywords were included in the search. The search queries were based on the Medical Subject Headings (MeSH) terms and the keywords. The limits or filters were selected to make a concise list of results. The focus was on the past five years, journal articles, and reviews published in English. The search strategy for the PubMed database with the keywords, MeSH terms, and filters is presented in Figure 3 as an example.
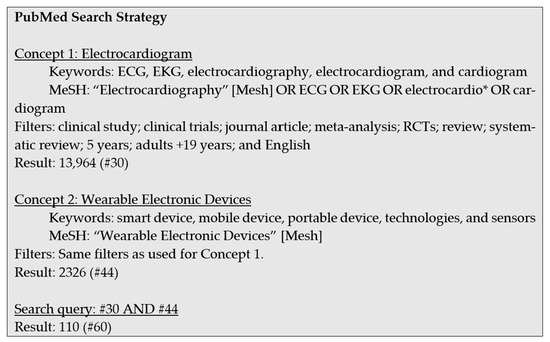
Figure 3.
Search strategies for the PubMed database.
2.3. Selecting the Studies
We exported records from each database into a master EndNote library and removed duplicates. Articles were selected based on the inclusion and exclusion criteria. The database search retrieved a total of 143 records, and 18 articles were selected that examined the performance and safety of novel concepts of measuring biopotential with a multichannel device and validated them against the gold standard 12-lead ECG or another variant. To have a wider inclusion window, articles/trials with healthy adults as well as those directed towards any cardiovascular condition were selected. Also, commentary and editorials were included if they aligned with the overall objectives. Out of the 18 articles included, three were reviews on wearable devices, which were not included in this scoping review but for a general overview of the current developments. A total of 12 articles (four which were clinical trials) were selected and reviewed in detail. Based on outcomes and the presence of strong evidence, six articles presented the data for device performance only and zero for device safety only (note: some of the literature addressed issues of both performance and safety). The main reasons for the exclusion of articles were duplication, non-availability of full articles, devices working on the principle of optical photoplethysmography (PPG) in smartwatches, or out-of-scope (as defined by the PICO strategy). After retrieving the full-text articles, two authors independently reviewed each paper based on the approved inclusion criteria, and the selected articles were discussed with the team.
2.4. Charting the Data
A summary table abstracting the data from the selected articles was drafted by one researcher. The information recorded in the final extraction included: sample characteristics (size, type of study population), publication year, study location, study design, study objective, type of device, comparative device, and study outcome. Discussion sections from these articles were reviewed to identify their common themes, limitations, and future research directions.
2.5. Clinical Data Appraisal, Collating, Summarizing, and Reporting
To ensure a systematic and unbiased appraisal of the data, the researchers set up an appraisal plan that describes the procedure and the criteria to be used for the appraisal. Table 2 shows appraisal criteria based on suitability and data contribution. Based on the defined appraisal plan, the selected articles were graded and categorized as to whether the data addressed the performance or safety of the device in question. The data were then ranked according to the importance of their contribution to establishing the safety and performance of the device and any specific claims about performance or safety. Grades 1–4 were assigned to evidence on both performance and safety, evidence only on performance, evidence only on safety, and no evidence on either parameter, respectively. The summary of the included articles was collated and summarized to report the study characteristics, different study designs, new technologies, and identified themes.
Table 2.
Appraisal plan for suitability.
3. Results
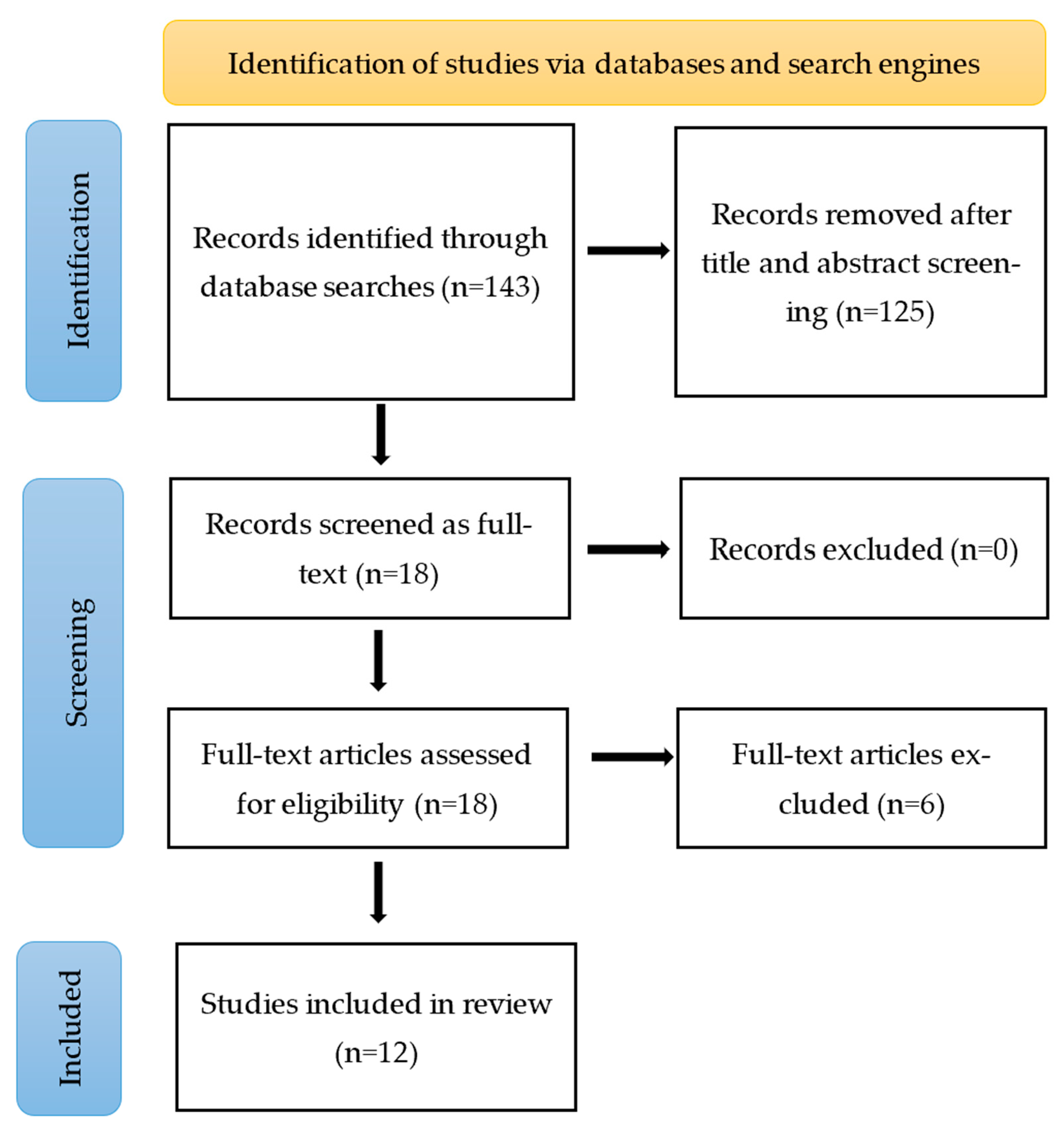
Figure 4 introduces the PRISMA-based flowchart search strategy and the outcome. It includes the number of records excluded after the title and abstract screening, the number of articles retrieved as full-text and excluded after reviewing, and the total number of studies included in the scoping review. We have searched four databases—PubMed, Cochrane, EMBASE, and CINAHL. Removing 125 articles after the title and abstract review left us with 18 full-text articles to review as per the eligibility criteria. At this point, 12 articles met the criteria and were added to this scoping review.
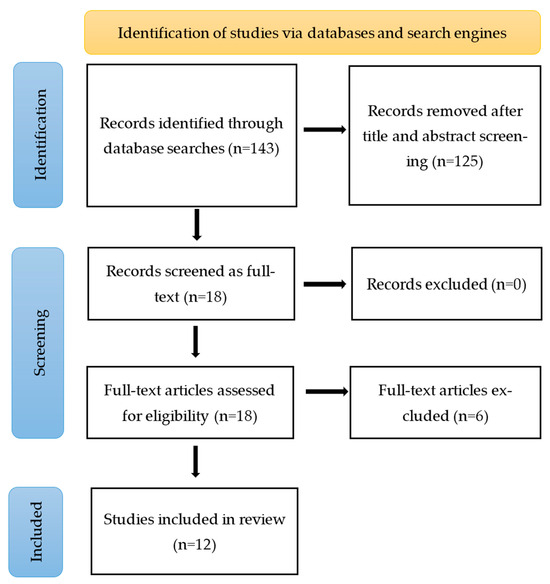
Figure 4.
PRISMA flow diagram of the search strategy.
3.1. Study Characteristics
The included studies were published between 2018 and 2020 and were spread across the Pacific, Asian, and European regions. The main locations were the USA (n = 3), Taiwan (n = 2), Italy (n = 2), and one each for Switzerland, Canada, China, Japan, and Brazil. The majority of studies included healthy adult subjects (n = 6), while others had healthy control to compare with the patients with atrial fibrillation (n = 3), long QT syndrome (LQTS) (n = 1), and sleep apnea (n = 1). One of the articles was a proof-of-concept for a multi-channel mechanocardiogram (MCG/ECG) to predict left ventricular ejection fraction (LVEF) (W. Y. Lin et al., 2018) [22]. The classification was established based on a variety of biosensing devices utilized for ECG measurement, encompassing all devices utilizing available sensing technologies such as chest-worn (dry-sensing), adhesive (gel-sensing), and textile-based (capacitive-sensing) options. The selected 12 articles investigated different bio-sensor devices categorized as chest-worn belts (Polar H10, Zephyr™ BioHarness™, BLE HR monitor), wrist bands (Kardia Band), adhesive chest strips (BodyGuardian™, Zio Patch), and wearable textile smart clothes (multi-channel mechanocardiogram (MCG)/ECG smart clothes, wearable textile ECG-belt, Omsignal system garment, textile nano-fibers coated with poly (3, 4-ethylene dioxythiophene) (PEDOT)-poly(styrene sulfonate) (PSS) polymer [23,24,25,26,27,28,29,30,31,32,33].
3.2. Appraisal of the Clinical Data
Based on the defined appraisal plan shown in Table 2, the selected articles were graded and categorized to determine whether the data addressed the performance or safety of the device in question. Table 3 presents the appraisal grading for the selected articles. As the PICO search strategy included all populations healthy and with any health conditions, most of these studies had appropriate population/patient groups. The data were rated as of high quality with an appropriate study design. The outcomes were aligned with the intended performance of the device. Four out of twelve studies did study long-term monitoring. The data provided were statistically analyzed and sufficient to compare and validate the devices with their respective controls/gold standards. As the devices were not aimed to induce any treatment effect clinically, the papers were graded as C3 (not applicable).
Table 3.
Appraisal grading for the selected articles as per the appraisal plan.
3.3. Evaluation of Performance Outcomes
The majority of the selected articles (n = 10) had the objective of evaluating the performance of the device under investigation. The two articles that did not account for these were assessing the applicability of a mobile application. The devices (chest straps) that these articles included were commercially available and validated against the gold standard. The purpose of including them in the report was to get an insight into different aspects of the project, such as Bluetooth connection and processing. The remaining 10 articles were ranked based on the similarity in the technology, material, and functions used for the current investigational device, i.e., the Datalogger.
From the ranking given in Table 4, the most important articles that contributed to the demonstration of the overall performance of the device are those with ranks 1–5 [29,31,32,34]. The evidence provided in papers on performance ranged from several outcomes, such as accuracy, signal quality, comparability, and visual assessment of ECG measurements by clinicians/electrophysiologists was sufficient. The statistical analysis performed on the data recorded with the devices evaluated has answered the respective objectives. These reviewed papers can serve as an important baseline to guide the extent of validation and test experiments to be conducted for evaluating the performance of the investigational devices in the future.
Table 4.
Summary of the included articles.
3.4. Evaluation of Safety Outcomes
The safety outcomes involved evaluating for any side effects and adverse effects of the wearable devices, either physical or mechanical, used in short- or long-term settings. A total of five papers provided direct or indirect evidence of safety for the device they investigated; thus, they have been ranked higher. The outcomes were related to long-term and continuous monitoring and/or skin irritation in the case of wearable textiles or patch electrodes. Whether the ECG sensors were made up of textile or silicone, there were no reported side effects for the devices reviewed. Steinberg et al. (2019) reported that the garments used for OM signals had a minimal risk of skin irritation compared to conventional Ag/AgCl electrodes (7% vs. 47%) [31]. The rest of the included paper did not assess safety parameters as an objective, mainly because the device was worn for a short period or because the device in question has been validated and assessed previously as supported by the literature. Some of these reviewed devices were commercially available and, therefore, have undergone extensive investigation for safety. A detailed summary of these articles is given in Table 4.
4. Discussion
The studies under scrutiny exhibited a diverse array of participant profiles and research objectives. While six studies focused on healthy adult subjects, others introduced controlled groups to compare individuals with specific conditions such as atrial fibrillation (AF), long QT syndrome, and sleep apnea. Notably, one article presented a proof-of-concept for a multi-channel mechanocardiogram aimed at predicting left ventricular ejection fraction (LVEF). This diversity underscores the evolving landscape of ECG monitoring and its application in various clinical contexts. The examined bio-sensor devices showcased a range of wearable forms, including chest-worn belts, wrist bands, adhesive chest strips, and innovative wearable textile smart clothes. The different types of wearable device approaches reflect the ongoing efforts to enhance user comfort, increase accessibility, and integrate ECG monitoring seamlessly into individuals’ daily lives. As technology continues to evolve, it opens avenues for novel wearable designs that can cater to specific user preferences and clinical requirements.
Interestingly, the evidence regarding safety considerations emerged from only five articles among those reviewed. Nonetheless, a noteworthy finding is that regardless of the type of ECG sensor employed, none of the studies reported any adverse effects associated with long-term or continuous monitoring. This is an encouraging indication that wearable ECG technology appears to be well-tolerated by users, at least within the scope of the studies analyzed. While only a limited number of articles addressed safety considerations, the collective evidence indicated a reassuring trend.
The WHO has indicated that more than 25% of adults do not meet the criteria for being physically active and are at a 20% to 30% higher risk of adult mortality [35]. The introduction of activity-tracing wearable devices has promoted physical activity and has been received with great enthusiasm by consumers and the research community. However, this comes with caution as these devices are not medical devices, and very few have only been regulated by the Food and Drug Administration and other regulatory authorities.
Despite the positive findings on clinical performance and safety, it is essential to acknowledge certain limitations in the current state of wearable technology. The reviewed literature provides a foundational understanding of device capabilities and limitations, yet it also reveals areas requiring further investigation for research and development. Several reviews and journal articles have pointed out the inaccuracy of measurements during some activities [23,36]. For instance, while the studies assessed the accuracy of the devices, there remains a need to explore their performance across different levels of physical activity intensities and various clinical conditions. Such investigations are crucial to understand how these factors may impact the quality and reliability of ECG signals, thereby influencing the diagnostic potential of the devices.
Future Challenges
Furthermore, future challenges in the realm of wearable ECG monitoring systems encompass a multifaceted landscape. With the invention of artificial intelligence and its integration into ECG monitoring and data analysis, its interpretation, security, and sovereignty pose both opportunities and challenges. Striking a balance between continuous long-term monitoring and efficient battery usage without compromising device performance would be imperative. It would be a challenge for the research community, healthcare professionals, regulators, and industries to design an intuitive user interface that is cost-effective and affordable, establish a clinical validation process fostering standards, and adhere to regulatory frameworks for the seamless integration of wearable ECG devices into mainstream healthcare.
5. Conclusions
This scoping review contributes a comprehensive understanding of the performance and safety aspects of novel multi-channel, sensor-based biopotential wearable devices for ECG monitoring in adults. The analyzed studies highlight the strides made in device accuracy and signal quality assessment, while also revealing the promising safety profile of these devices. The evolving landscape offers prospects for refining technology, broadening clinical applications, and advancing personalized health management. As wearable ECG technology continues to shape the future of cardiovascular care, collaboration between researchers, clinicians, and industry partners will be instrumental in unlocking its full potential.
Author Contributions
Conceptualization, E.S.D. and A.L.; methodology, E.S.D.; investigation, E.S.D.; writing—original draft preparation, E.S.D. and A.M.K.; writing—review and editing, A.L. and G.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Business, Innovation, and Employment, New Zealand.
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data was created.
Conflicts of Interest
There are no conflict of interest to disclose.
References
- Deaton, C.; Froelicher, E.S.; Wu, L.H.; Ho, C.; Shishani, K.; Jaarsma, T. The global burden of cardiovascular disease. Eur. J. Cardiovasc. Nurs. 2011, 10 (Suppl. S2), S5–S13. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Krishnamurthi, R.V.; Barker-Collo, S.; McPherson, K.M.; Barber, P.A.; Parag, V.; Arroll, B.; Bennett, D.A.; Tobias, M.; Jones, A. 30-year trends in stroke rates and outcome in Auckland, New Zealand (1981–2012): A multi-ethnic population-based series of studies. PLoS ONE 2015, 10, e0134609. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- Delano, M.K. A Long Term Wearable Electrocardiogram (ECG) Measurement System. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2012. [Google Scholar]
- Kalra, A.; Lowe, A.; Al-Jumaily, A. Critical review of electrocardiography measurement systems and technology. Meas. Sci. Technol. 2018, 30, 012001. [Google Scholar] [CrossRef]
- Rafie, N.; Kashou, A.H.; Noseworthy, P.A. ECG interpretation: Clinical relevance, challenges, and advances. Hearts 2021, 2, 505–513. [Google Scholar] [CrossRef]
- Stracina, T.; Ronzhina, M.; Redina, R.; Novakova, M. Golden standard or obsolete method? Review of ECG applications in clinical and experimental context. Front. Physiol. 2022, 13, 867033. [Google Scholar] [CrossRef]
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Nujum Navaz, A. ECG Monitoring Systems: Review, Architecture, Processes, and Key Challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef]
- Drew, B.J.; Califf, R.M.; Funk, M.; Kaufman, E.S.; Krucoff, M.W.; Laks, M.M.; Macfarlane, P.W.; Sommargren, C.; Swiryn, S.; Van Hare, G.F. Practice standards for electrocardiographic monitoring in hospital settings: An American Heart Association scientific statement from the Councils on Cardiovascular Nursing, Clinical Cardiology, and Cardiovascular Disease in the Young: Endorsed by the International Society of Computerized Electrocardiology and the American Association of Critical-Care Nurses. Circulation 2004, 110, 2721–2746. [Google Scholar]
- Khunti, K. Accurate interpretation of the 12-lead ECG electrode placement: A systematic review. Health Educ. J. 2014, 73, 610–623. [Google Scholar] [CrossRef]
- Lilly, L.S. Pathophysiology of Heart Disease: A Collaborative Project of Medical Students and Faculty; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Abuwarda, Z.; Mostafa, K.; Oetomo, A.; Hegazy, T.; Morita, P. Wearable devices: Cross benefits from healthcare to construction. Autom. Constr. 2022, 142, 104501. [Google Scholar] [CrossRef]
- Vinetti, G.; Lopomo, N.F.; Taboni, A.; Fagoni, N.; Ferretti, G. The current use of wearable sensors to enhance safety and performance in breath-hold diving: A systematic review. Diving Hyperb. Med. 2020, 50, 54. [Google Scholar] [CrossRef] [PubMed]
- Hayward, J.; Chansin, G. Wearable Sensors 2015–2025: Market Forecasts, Technologies, Players; IDTechEx: Cambridge, UK, 2015. [Google Scholar]
- Prieto-Avalos, G.; Cruz-Ramos, N.A.; Alor-Hernández, G.; Sánchez-Cervantes, J.L.; Rodríguez-Mazahua, L.; Guarneros-Nolasco, L.R. Wearable devices for physical monitoring of heart: A review. Biosensors 2022, 12, 292. [Google Scholar] [CrossRef] [PubMed]
- Bayoumy, K.; Gaber, M.; Elshafeey, A.; Mhaimeed, O.; Dineen, E.H.; Marvel, F.A.; Martin, S.S.; Muse, E.D.; Turakhia, M.P.; Tarakji, K.G. Smart wearable devices in cardiovascular care: Where we are and how to move forward. Nat. Rev. Cardiol. 2021, 18, 581–599. [Google Scholar] [CrossRef] [PubMed]
- Cosoli, G.; Spinsante, S.; Scardulla, F.; D’Acquisto, L.; Scalise, L. Wireless ECG and cardiac monitoring systems: State of the art, available commercial devices and useful electronic components. Measurement 2021, 177, 109243. [Google Scholar] [CrossRef]
- Sequeira, L.; Perrotta, S.; LaGrassa, J.; Merikangas, K.; Kreindler, D.; Kundur, D.; Courtney, D.; Szatmari, P.; Battaglia, M.; Strauss, J. Mobile and wearable technology for monitoring depressive symptoms in children and adolescents: A scoping review. J. Affect. Disord. 2020, 265, 314–324. [Google Scholar] [CrossRef]
- Yan, L.; Yoo, J.; Kim, B.; Yoo, H.-J. A 0.5-μ Vrms 12-μ W Wirelessly Powered Patch-Type Healthcare Sensor for Wearable Body Sensor Network. IEEE J. Solid-State Circuits 2010, 45, 2356–2365. [Google Scholar]
- Kim, D.-H.; Lu, N.; Ma, R.; Kim, Y.-S.; Kim, R.-H.; Wang, S.; Wu, J.; Won, S.M.; Tao, H.; Islam, A. Epidermal electronics. Science 2011, 333, 838–843. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Lin, W.Y.; Ke, H.L.; Chou, W.C.; Chang, P.C.; Tsai, T.H.; Lee, M.Y. Realization and Technology Acceptance Test of a Wearable Cardiac Health Monitoring and Early Warning System with Multi-Channel MCGs and ECG. Sensors 2018, 18, 3538. [Google Scholar] [CrossRef]
- Boudreaux, B.D.; Hebert, E.P.; Hollander, D.B.; Williams, B.M.; Cormier, C.L.; Naquin, M.R.; Gillan, W.W.; Gusew, E.E.; Kraemer, R.R. Validity of Wearable Activity Monitors during Cycling and Resistance Exercise. Med. Sci. Sports Exerc. 2018, 50, 624–633. [Google Scholar] [CrossRef]
- Bumgarner, J.M.; Lambert, C.T.; Hussein, A.A.; Cantillon, D.J.; Baranowski, B.; Wolski, K.; Lindsay, B.D.; Wazni, O.M.; Tarakji, K.G. Smartwatch Algorithm for Automated Detection of Atrial Fibrillation. J. Am. Coll. Cardiol. 2018, 71, 2381–2388. [Google Scholar] [CrossRef]
- Castelletti, S.; Dagradi, F.; Goulene, K.; Danza, A.I.; Baldi, E.; Stramba-Badiale, M.; Schwartz, P.J. A wearable remote monitoring system for the identification of subjects with a prolonged QT interval or at risk for drug-induced long QT syndrome. Int. J. Cardiol. 2018, 266, 89–94. [Google Scholar] [CrossRef]
- Pereira, R.D.A.; Alves, J.L.D.B.; Silva, J.H.D.C.; Costa, M.D.S.; Silva, A.S. Validity of a Smartphone Application and Chest Strap for Recording RR Intervals at Rest in Athletes. Int. J. Sports Physiol. Perform. 2020, 15, 896–899. [Google Scholar] [CrossRef]
- Fontana, P.; Martins, N.R.A.; Camenzind, M.; Rossi, R.M.; Baty, F.; Boesch, M.; Schoch, O.D.; Brutsche, M.H.; Annaheim, S. Clinical Applicability of a Textile 1-Lead ECG Device for Overnight Monitoring. Sensors 2019, 19, 2436. [Google Scholar] [CrossRef]
- Lin, I.M. Effects of a cardiorespiratory synchronization training mobile application on heart rate variability and electroencephalography in healthy adults. Int. J. Psychophysiol. 2018, 134, 168–177. [Google Scholar] [CrossRef]
- Peng, S.; Xu, K.; Chen, W. Comparison of Active Electrode Materials for Non-Contact ECG Measurement. Sensors 2019, 19, 3585. [Google Scholar] [CrossRef]
- Reverberi, C.; Rabia, G.; De Rosa, F.; Bosi, D.; Botti, A.; Benatti, G. The RITMIA™ Smartphone App for Automated Detection of Atrial Fibrillation: Accuracy in Consecutive Patients Undergoing Elective Electrical Cardioversion. BioMed Res. Int. 2019, 2019, 4861951. [Google Scholar] [CrossRef]
- Steinberg, C.; Philippon, F.; Sanchez, M.; Fortier-Poisson, P.; O’Hara, G.; Molin, F.; Sarrazin, J.F.; Nault, I.; Blier, L.; Roy, K.; et al. A Novel Wearable Device for Continuous Ambulatory ECG Recording: Proof of Concept and Assessment of Signal Quality. Biosensors 2019, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, Y.T.; Tokita, M.; Murata, H.; Hirasawa, Y.; Yodogawa, K.; Iwasaki, Y.K.; Asai, K.; Shimizu, W.; Kasai, N.; Nakashima, H.; et al. Validation of wearable textile electrodes for ECG monitoring. Heart Vessel. 2019, 34, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.J.; Roetker, N.S.; Folsom, A.R.; Alonso, A.; Heckbert, S.R.; Chen, L.Y. Feasibility of using a leadless patch monitor in community cohort studies: The Multi-ethnic Study of Atherosclerosis. Pacing Clin. Electrophysiol. 2018, 41, 1389–1390. [Google Scholar] [CrossRef] [PubMed]
- Fontana, P.; Martins, N.R.A.; Camenzind, M.; Boesch, M.; Baty, F.; Schoch, O.D.; Brutsche, M.H.; Rossi, R.M.; Annaheim, S. Applicability of a Textile ECG-Belt for Unattended Sleep Apnoea Monitoring in a Home Setting. Sensors 2019, 19, 3367. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization. Physical Activity. Available online: https://www.who.int/en/news-room/fact-sheets/detail/physical-activity (accessed on 31 July 2021).
- Bai, Y.; Welk, G.J.; Nam, Y.H.; Lee, J.A.; Lee, J.-M.; Kim, Y.; Meier, N.F.; Dixon, P.M. Comparison of consumer and research monitors under semistructured settings. Med. Sci. Sports Exerc. 2016, 48, 151–158. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).