
Analysis of Heart Rate Variability in Individuals Affected by Amyotrophic Lateral Sclerosis

 , , ,
, , ,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
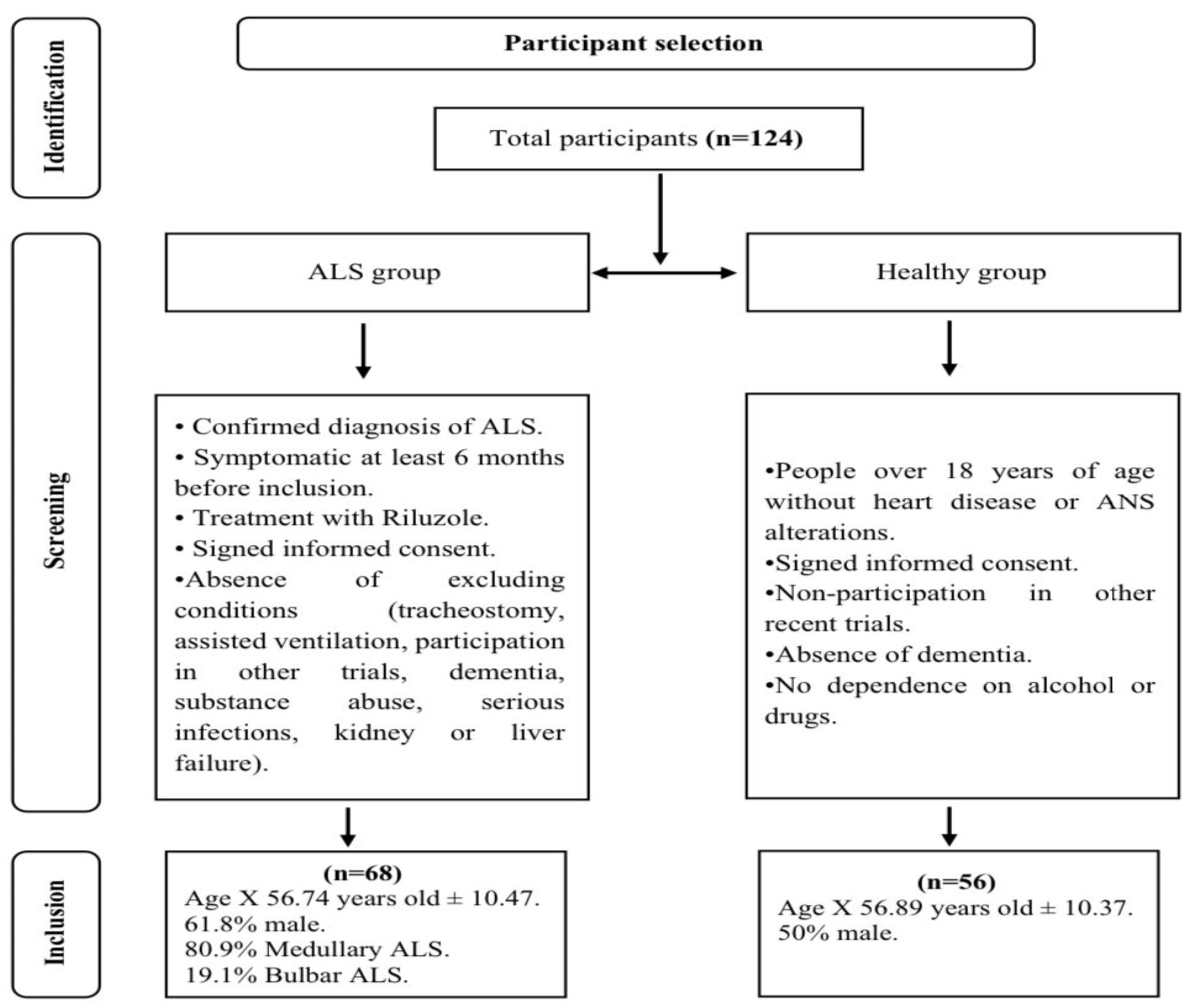
2.1. Participants
2.2. Materials and Instruments
2.3. Design
- Temporal variables:
- Frequency variables:
2.4. Procedure
2.5. HRV Analyses
2.6. Data Analysis
2.7. Ethical Concerns
3. Results
3.1. Differences in Cardiac Variability between ALS Patients and Healthy Individuals
3.2. Sex Differences in Cardiac Variability in ALS
3.3. Reference Values for Heart Rate Variability in ALS patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castro, E.; Azagra, R.; Gómez, X.; Povedano, M. La esclerosis lateral amiotrófica (ELA) desde la Atención Primaria. Epidemiología y características clínico-asistenciales. Aten. Primaria 2021, 53, 102158. [Google Scholar] [CrossRef] [PubMed]
- Camacho, A.; Esteban, J.; Paradas, C. Report by the Spanish Foundation for the Brain on the social impact of amyotrophic lateral sclerosis and other neuromuscular disorders. Neurologia 2018, 33, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Soofi, A.Y.; Bello-Haas, V.D.; Kho, M.E.; Letts, L. The Impact of Rehabilitative Interventions on Quality of Life: A Qualitative Evidence Synthesis of Personal Experiences of Individuals with Amyotrophic Lateral Sclerosis. Qual. Life Res. 2018, 27, 845–856. [Google Scholar] [CrossRef]
- Izenberg, A. Amyotrophic Lateral Sclerosis and Other Motor Neuron Diseases. Contin. (Minneap. Minn.) 2023, 29, 1538–1563. [Google Scholar] [CrossRef] [PubMed]
- Crescimanno, G.; Greco, F.; Bertini, M.; Marrone, O. Cardiovascular autonomic control during application of different modes of noninvasive ventilation in patients affected by amyotrophic lateral sclerosis. Heart Lung 2022, 56, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosc. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Geovanini, G.R.; Vasques, E.R.; De Oliveira, A.; Mill, J.; Andreão, R.; Vasques, B.; Costa, A.; Krieger, J.E. Age and Sex Differences in Heart Rate Variability and Vagal Specific Patterns—Baependi Heart Study. Glob. Heart 2020, 15, 71. [Google Scholar] [CrossRef]
- Papadopoulou, M.; Bakola, E.; Papapostolou, A.; Stefanou, M.I.; Moschovos, C.; Salakou, S.; Zis, P.; Zouvelou, V. Autonomic dysfunction in amyotrophic lateral sclerosis: A neurophysiological and neurosonology study. J. Neuroimaging 2022, 32, 710–719. [Google Scholar] [CrossRef]
- Oprisan, A.; Popescu, B.O. Dysautonomia in Amyotrophic Lateral Sclerosis. Int. J. Mol. Sci. 2023, 24, 14927. [Google Scholar] [CrossRef]
- Pavlovic, S.; Stevic, Z.; Mikovanovic, B.; Milicic, B.; Rakocevic, V.; Lavrnic, D.; Apostolski, S. Impairment of cardiac autonomic control in patients with amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2010, 11, 272–276. [Google Scholar] [CrossRef]
- Alvarado, V.; Camacho, S.; Monge, S.L.; Rodríguez, D.; Fernández, A.V. Detection heart rate variability as an indicator of autonomic nervous system activation: Implicantions in exercise and pathologies. Rev. Med. UCR 2017, 11, 48–64. [Google Scholar]
- Veloza, L.; Jiménez, C.; Quiñones, D.; Polanía, F.; Pachón-Valero, L.C.; Rodríguez-Triviño, C.Y. Heart rate variability as a predictive factor of cardiovascular disease. Rev. Colomb. Cardiol. 2019, 26, 205–210. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Moya-Ramon, M.; Mateo-March, M.; Peña-González, I.; Zabala, M.; Javaloyes, A. Validity and reliability of different smartphones applications to measure HRV during short and ultra-short measurements in elite athletes. Comput. Methods Programs Biomed. 2022, 217, 106696. [Google Scholar] [CrossRef] [PubMed]
- İşcan, D.; Karaaslan, M.B.; Deveci, O.S.; Akıllı, R.; Koç, F. The importance of heart rate variability in predicting cardiac autonomic dysfunction in patients with amyotrophic lateral sclerosis. Int. J. Clin. Pract. 2021, 75, e14536. [Google Scholar] [CrossRef] [PubMed]
- Umetani, K.; Singer, D.H.; McCraty, R.; Atkinson, M. Twenty-Four Hour Time Domain Heart Rate Variability and Heart Rate: Relations to Age and Gender Over Nine Decades. JACC 1998, 31, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.; Menze, I.; Moritz, C.; Metelmenn, T.B.; Woost, J.C.; Johann, O.P. Multimodal assessment of autonomic dysfunction in amyotrophic lateral sclerosis. Eur. J. Neurol. 2021, 29, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research—Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 20, 213. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart Rate Variability as an Index of Regulated Emotional Responding. Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef]
- Aubert, A.; Seps, B.; Beckers, F. Heart Rate Variability in Athletes. Sports Med. 2003, 33, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Hayano, J.; Yuda, E. Assessment of autonomic function using long-term heart rate variability: Beyond the classical framework of LF and HF measurements. J. Physiol. Anthr. 2021, 40, 21. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. Heart Rate Variability? A Historical Perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef] [PubMed]
- Marek, C. Electrophysiology Task Force. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation. Eur. Heart J. 1996, 93, 1043–1065. [Google Scholar]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- West, S.G.; Finch, J.F.; Curran, P.J. Structural equation models with nonnormal variables: Problems and remedies. In Structural Equation Modeling: Concepts, Issues, and Applications; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1995; pp. 56–75. [Google Scholar]
- Cohen, J. Quantitative methods in psychology. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; Pinto, A.; De Carvalho, M. Decreased heart rate variability predicts death in amyotrophic lateral sclerosis. Muscle Nerve 2012, 46, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Silveira, A.C.; Moraes, Í.; Vidigal, G.P.; Simcsik, A.O.; Rosa, R.M.; Favero, F.M.; Fernandes, S.; Garner, D.; Araújo, B.M.; Taiar, R. Cardiac Autonomic Modulation in Subjects with Amyotrophic Lateral Sclerosis (ALS) during an Upper Limb Virtual Reality Task: A Prospective Control Trial. BioMed Res. Int. 2022, 9, 4439681. [Google Scholar] [CrossRef]
- Moore, J. Normative HRV Scores by Age and Gender [Heart Rate Variability Chart]. Elite HRV. 2021. Available online: https://elitehrv.com/normal-heart-rate-variability-age-gender (accessed on 2 February 2024).
- Gąsior, J.S.; Sacha, J.; Jeleń, P.J.; Zieliński, J.; Przybylski, J. Heart Rate and Respiratory Rate Influence on Heart Rate Variability Repeatability: Effects of the Correction for the Prevailing Heart Rate. Front. Physiol. 2016, 18, 356. [Google Scholar] [CrossRef]
- Brown, A.A.; Ferguson, B.J.; Jones, V.; Green, B.E.; Pearre, J.D.; Anunoby, I.A.; Beversdorf, D.; Barohn, R.; Cirstea, C. Pilot Study of Real-World Monitoring of the Heart Rate Variability in Amyotrophic Lateral Sclerosis. Front. Artif. Intell. 2022, 5, 910049. [Google Scholar] [CrossRef] [PubMed]
- Pisano, F.; Miscio, G.; Mazzuero, G.; Lanfranchi, P.; Colombo, R.; Pinelli, P. Decreased heart rate variability in amyotrophic lateral sclerosis. Muscle Nerve 1995, 18, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Dalla Vecchia, L.; De Maria, B.; Marinou, K.; Sideri, R.; Lucini, A.; Porta, A.; Mora, G. Cardiovascular neural regulation is impaired in amyotrophic lateral sclerosis patients. A study by spectral and complexity analysis of cardiovascular oscillations. Physiol. Meas. 2015, 36, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Merico, A.; Cavinato, M. Autonomic dysfunction in the early stage of ALS with bulbar involvement. Amyotroph. Lateral Scler. 2011, 12, 363–367. [Google Scholar] [CrossRef] [PubMed]
- De Maria, B.; Bari, V.; Marchi, A.; Barbic, F.; Furlan, R.; Mora, G.; Dalla, L.; Porta, A. Cardiovascular control indexes in amyotrophic lateral sclerosis patients and their relation with clinical markers. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Milan, Italy, 25–29 August 2015; pp. 2055–2058. [Google Scholar] [CrossRef]
- Rosenbohm, A.; Schmid, B.; Buckert, D.; Rottbauer, W.; Kassubek, J.; Ludolph, A.C.; Bernhardt, P. Cardiac Findings in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Imaging Study. Front. Neurol. 2017, 8, 479. [Google Scholar] [CrossRef]
- Chrousos, G.P.; Gold, P.W. The concepts of stress and stress system disorders. Overview of physical and behavioral homeostasis. JAMA 1992, 267, 1244–1252. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| M | SD | Skewness | Kurtosis | |
|---|---|---|---|---|
| Age | 56.81 | 10.39 | −0.13 | −0.39 |
| HRV index | 46.70 | 12.77 | 0.16 | 0.20 |
| HRV RMSSD ms | 30.87 | 30.43 | 2.60 * | 8.09 * |
| HRV LN RMSSD ms | 3.08 | 0.84 | 0.04 | 0.10 |
| HRV SDNN ms | 42.81 | 38.80 | 2.96 * | 10.91 * |
| HRV PNN50 | 8.56 | 13.97 | 2.39 * | 6.17 * |
| LF Power ms2 | 833.47 | 1703.79 | 3.50 * | 13.07 * |
| HF Power ms2 | 633.23 | 1847.79 | 4.63 * | 22.99 * |
| LF HF ratio | 4.07 | 5.59 | 3.26 * | 13.18 * |
| HF Peak HZ | 0.26 | 0.09 | 0.77 | −0.07 |
| HR Average | 76.66 | 13.73 | 0.80 | 0.3 |
| Group | M | SD | Differences in Means | d Cohen | |
|---|---|---|---|---|---|
| HRV index | ALS | 42.33 | 12.21 | t123 = 4.7, p < 0.001 | 0.82 |
| Healthy | 52.07 | 11.39 | |||
| HRV RMSSD ms | ALS | 22.00 | 22.28 | U = 952.00, p < 0.001 | 0.86 |
| Healthy | 41.65 | 35.37 | |||
| HRV LN RMSSD ms | ALS | 2.76 | 0.81 | t121 = 5.14, p < 0.001 | 0.93 |
| Healthy | 3.47 | 0.71 | |||
| HRV SDNN ms | ALS | 30.07 | 25.28 | U = 81.50, p < 0.001 | 0.99 |
| Healthy | 58.28 | 46.30 | |||
| HRV PNN50 | ALS | 4.79 | 10.57 | U = 1014.00, p < 0.001 | 0.84 |
| Healthy | 13.14 | 16.17 | |||
| Frequency LF Power ms2 | ALS | 461.62 | 1231.02 | U = 1014.00, p < 0.001 | 0.81 |
| Healthy | 1285.00 | 2065.76 | |||
| Frequency HF Power ms2 | ALS | 366.00 | 1250.29 | U = 1067.00, p < 0.001 | 0.76 |
| Healthy | 957.72 | 2352.85 | |||
| Frequency LF HF ratio | ALS | 3.94 | 5.48 | U = 1792.00, p = 0.574 | 0.10 |
| Healthy | 4.22 | 5.77 | |||
| Frequency HF Peak HZ | ALS | 0.27 | 0.09 | t122 = 0.98, p = 0.330 | 0.18 |
| Healthy | 0.25 | 0.08 | |||
| HR Average | ALS | 79.30 | 14.11 | t123 = 2.24, p = 0.016 | 0.44 |
| Healthy | 73.41 | 12.62 |
| Group | M | SD | Differences in Means | d Cohen | |
|---|---|---|---|---|---|
| HRV index | Male | 41.12 | 11.64 | t66 = 0.78, p = 0.440 | 0.20 |
| Female | 43.48 | 12.49 | |||
| HRV RMSSD ms | Female | 18.70 | 12.37 | U = 512.00, p = 0.866 | 0.04 |
| Male | 24.35 | 26.50 | |||
| HRV LN RMSSD ms | Female | 2.69 | 0.77 | t64 = 0.67, p = 0.508 | 0.17 |
| Male | 2.82 | 0.83 | |||
| HRV SDNN ms | Female | 24.90 | 15.85 | U = 425.00, p = 0.195 | 0.33 |
| Male | 33.67 | 29.25 | |||
| HRV PNN50 | Female | 3.32 | 7.05 | U = 487.00, p = 0.575 | 0.14 |
| Male | 5.79 | 12.28 | |||
| Frequency LF Power ms2 | Female | 195.69 | 284.21 | U = 396.00, p = 0.094 | 0.42 |
| Male | 629.76 | 1533.91 | |||
| Frequency HF Power ms2 | Female | 134.35 | 230.96 | U = 446.00, p = 0.306 | 0.26 |
| Male | 512.41 | 1570.20 | |||
| Frequency LF HF ratio | Female | 3.16 | 3.09 | U = 466.50, p = 0.448 | 0.19 |
| Male | 4.35 | 6.55 | |||
| Frequency HF Peak HZ | Female | 0.31 | 0.09 | t65 = 3.06, p = 0.003 | 0.77 |
| Male | 0.24 | 0.08 | |||
| HR Average | Female | 81.92 | 14.43 | t66 = 1.34, p = 0.186 | 0.34 |
| Varón | 77.26 | 13.67 |
| Centile | Zn | T | HRV Index | ZHRV Index | HRV RMSSD ms | ZRMSSD ms | HRV LN RMSSD ms | ZHRV LN RMSSD ms | HRV SDNN ms | ZSDNN ms | HRV PNN50 | ZHRV PNN50 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | −2.33 | 26.70 | 9.00 | −2.73 | 1.82 | −0.91 | 0.60 | −2.67 | 5.74 | −0.96 | 0.00 | −0.45 | ||||||||||||||||||
| 5 | −1.64 | 33.60 | 23.00 | −1.58 | 4.45 | −0.79 | 1.45 | −1.61 | 8.23 | −0.86 | 0.00 | −0.45 | ||||||||||||||||||
| 10 | −1.28 | 37.20 | 26.00 | −1.34 | 5.52 | −0.74 | 1.71 | −1.30 | 10.01 | −0.79 | 0.00 | −0.45 | ||||||||||||||||||
| 15 | −1.04 | 39.60 | 30.50 | −0.97 | 7.10 | −0.67 | 1.94 | −1.01 | 11.86 | −0.72 | 0.00 | −0.45 | ||||||||||||||||||
| 20 | −0.84 | 41.60 | 32.00 | −0.85 | 8.09 | −0.62 | 2.09 | −0.83 | 13.64 | −0.65 | 0.00 | −0.45 | ||||||||||||||||||
| 25 | −0.67 | 43.30 | 35.00 | −0.60 | 9.84 | −0.55 | 2.24 | −0.64 | 14.98 | −0.60 | 0.00 | −0.45 | ||||||||||||||||||
| 30 | −0.52 | 44.80 | 36.00 | −0.52 | 10.49 | −0.52 | 2.32 | −0.54 | 16.30 | −0.54 | 0.00 | −0.45 | ||||||||||||||||||
| 35 | −0.39 | 46.10 | 38.00 | −0.35 | 12.25 | −0.44 | 2.47 | −0.35 | 18.31 | −0.47 | 0.00 | −0.45 | ||||||||||||||||||
| 40 | −0.25 | 47.50 | 39.00 | −0.27 | 12.70 | −0.42 | 2.54 | −0.27 | 20.32 | −0.39 | 0.00 | −0.45 | ||||||||||||||||||
| 45 | −0.13 | 48.70 | 39.50 | −0.23 | 13.21 | −0.39 | 2.57 | −0.23 | 22.54 | −0.30 | 0.00 | −0.45 | ||||||||||||||||||
| 50 | 0.00 | 50.00 | 41.00 | −0.11 | 14.78 | −0.32 | 2.68 | −0.10 | 23.85 | −0.25 | 0.00 | −0.45 | ||||||||||||||||||
| 55 | 0.13 | 51.30 | 43.00 | 0.05 | 16.12 | −0.26 | 2.80 | 0.04 | 25.81 | −0.17 | 0.00 | −0.45 | ||||||||||||||||||
| 60 | 0.25 | 52.50 | 44.00 | 0.14 | 17.61 | −0.20 | 2.87 | 0.14 | 28.30 | −0.07 | 0.00 | −0.45 | ||||||||||||||||||
| 65 | 0.39 | 53.90 | 45.50 | 0.26 | 19.98 | −0.09 | 3.03 | 0.34 | 31.00 | 0.04 | 1.00 | −0.36 | ||||||||||||||||||
| 70 | 0.52 | 55.20 | 49.00 | 0.55 | 24.79 | 0.13 | 3.23 | 0.58 | 33.59 | 0.14 | 3.30 | −0.14 | ||||||||||||||||||
| 75 | 0.67 | 56.70 | 51.00 | 0.71 | 27.98 | 0.27 | 3.33 | 0.70 | 34.69 | 0.18 | 4.75 | 0.00 | ||||||||||||||||||
| 80 | 0.84 | 58.40 | 52.00 | 0.79 | 29.29 | 0.33 | 3.38 | 0.77 | 38.50 | 0.33 | 7.20 | 0.23 | ||||||||||||||||||
| 85 | 1.04 | 60.40 | 54.50 | 1.00 | 34.76 | 0.57 | 3.55 | 0.97 | 44.04 | 0.55 | 10.00 | 0.49 | ||||||||||||||||||
| 90 | 1.28 | 62.80 | 58.00 | 1.28 | 43.98 | 0.99 | 3.78 | 1.26 | 57.49 | 1.08 | 15.40 | 1.00 | ||||||||||||||||||
| 95 | 1.64 | 66.40 | 66.50 | 1.98 | 75.34 | 2.39 | 4.33 | 1.93 | 70.64 | 1.60 | 32.10 | 2.58 | ||||||||||||||||||
| 99 | 2.33 | 73.30 | 66.50 | 1.98 | 75.34 | 2.39 | 4.33 | 1.93 | 70.64 | 1.60 | 32.10 | 2.58 | ||||||||||||||||||
| Mean | 0.00 | 50.00 | 42.33 | 0.00 | 22.00 | 0.00 | 2.76 | 0.00 | 30.07 | 0.00 | 4.79 | 0.00 | ||||||||||||||||||
| DT | 1.00 | 10.00 | 12.21 | 1.00 | 22.28 | 1.00 | 0.81 | 1.00 | 25.28 | 1.00 | 10.57 | 1.00 | ||||||||||||||||||
| Centile | Zn | T | Frequency LF Power ms2 | Z Frequency LF Power ms2 | Frequency HF Power ms2 | Z Frequency HF Power ms2 | Frequency LF HF ratio | Z Frequency LF HR ratio | Frequency HF Peak HZ | Z Frequency HF Peak Hz | Frequency HF Peak HZ (Female) | Z Frequency HF Peak Hz (Female) | Frequency HF Peak HZ (Male) | Z Frequency HF Peak Hz (Male) | HR Average | ZHR Average | ||||||||||||||
| 1 | −2.33 | 26.70 | 7.70 | −0.37 | 0.91 | −0.29 | 0.08 | −0.70 | 0.16 | −1.24 | 0.16 | −1.08 | 0.17 | −1.52 | 54.00 | −1.79 | ||||||||||||||
| 5 | −1.64 | 33.60 | 14.18 | −0.36 | 3.82 | −0.29 | 0.25 | −0.67 | 0.16 | −1.24 | 0.16 | −1.08 | 0.17 | −1.50 | 58.00 | −1.51 | ||||||||||||||
| 10 | −1.28 | 37.20 | 21.18 | −0.36 | 7.94 | −0.29 | 0.57 | −0.62 | 0.16 | −1.24 | 0.16 | −1.08 | 0.18 | −1.38 | 64.00 | −1.08 | ||||||||||||||
| 15 | −1.04 | 39.60 | 26.44 | −0.35 | 12.21 | −0.28 | 0.73 | −0.59 | 0.17 | −1.06 | 0.16 | −1.08 | 0.20 | −1.19 | 66.00 | −0.94 | ||||||||||||||
| 20 | −0.84 | 41.60 | 35.64 | −0.35 | 16.09 | −0.28 | 0.98 | −0.54 | 0.19 | −0.90 | 0.16 | −1.08 | 0.25 | −0.66 | 68.00 | −0.80 | ||||||||||||||
| 25 | −0,67 | 43.30 | 43.88 | −0.34 | 20.88 | −0.28 | 1.08 | −0.52 | 0.19 | −0.86 | 0.17 | −0.88 | 0.25 | −0.66 | 69.00 | −0.73 | ||||||||||||||
| 30 | −0.52 | 44.80 | 64.31 | −0.32 | 25.57 | −0.27 | 1.24 | −0.49 | 0.20 | −0.71 | 0.19 | −0,68 | 0.25 | −0.66 | 70.00 | −0.66 | ||||||||||||||
| 35 | −0.39 | 46.10 | 74.52 | −0.31 | 27.94 | −0.27 | 1.59 | −0.43 | 0.22 | −0.54 | 0.20 | −0.598 | 0.27 | −0.48 | 72.50 | −0.48 | ||||||||||||||
| 40 | −0.25 | 47.50 | 82.61 | −0.31 | 34.80 | −0.26 | 1.82 | −0.39 | 0.22 | −0.54 | 0.21 | −0.45 | 0.27 | −0.48 | 74.00 | −0.38 | ||||||||||||||
| 45 | −0.13 | 48.70 | 98.02 | −0.30 | 38.97 | −0.26 | 2.07 | −0.34 | 0.25 | −0.19 | 0.22 | −0.29 | 0.28 | −0.36 | 75.50 | −0.27 | ||||||||||||||
| 50 | 0.00 | 50.00 | 124.13 | −0.27 | 43.20 | −0.26 | 2.40 | −0.28 | 0.25 | −0.19 | 0.22 | −0.29 | 0.30 | −0.13 | 76.00 | −0.23 | ||||||||||||||
| 55 | 0.13 | 51.30 | 145.97 | −0.26 | 59.90 | −0.24 | 2.65 | −0.24 | 0.27 | −0.02 | 0.22 | −0.29 | 0.30 | −0.08 | 78.50 | −0.06 | ||||||||||||||
| 60 | 0.25 | 52.50 | 172.95 | −0.23 | 77.65 | −0.23 | 2.88 | −0.19 | 0.27 | −0.01 | 0.25 | 0.10 | 0.31 | 0.04 | 81.00 | 0.12 | ||||||||||||||
| 65 | 0.39 | 53.90 | 205.63 | −0.21 | 10.79 | −0.20 | 3.43 | −0.09 | 0.28 | 0.15 | 0.25 | 0.10 | 0.33 | 0.19 | 83.00 | 0.26 | ||||||||||||||
| 70 | 0.52 | 55.20 | 253.59 | −0.17 | 124.83 | −0.19 | 3.80 | −0.03 | 0.30 | 0.38 | 0.27 | 0.30 | 0.35 | 0.46 | 86.00 | 0.47 | ||||||||||||||
| 75 | 0.67 | 56.70 | 308.25 | −0.12 | 155.01 | −0.17 | 4.26 | 0.06 | 0.33 | 0.67 | 0.29 | 0.53 | 0.38 | 0.82 | 88.50 | 0.65 | ||||||||||||||
| 80 | 0.84 | 58.40 | 400.82 | −0.05 | 200.64 | −0.13 | 5.98 | 0.37 | 0.34 | 0.85 | 0.33 | 1.15 | 0.39 | 0.91 | 91.00 | 0.83 | ||||||||||||||
| 85 | 1.04 | 60.40 | 595.04 | 0.11 | 279.69 | −0.07 | 8.38 | 0.81 | 0.37 | 1.13 | 0.34 | 1.27 | 0.43 | 1.29 | 92.00 | 0.90 | ||||||||||||||
| 90 | 1.28 | 62.80 | 995.53 | 0.43 | 467.56 | 0.08 | 8.96 | 0.92 | 0.39 | 1.41 | 0.36 | 1.46 | 0.47 | 1.74 | 98.00 | 1.33 | ||||||||||||||
| 95 | 1.64 | 66.40 | 2486.67 | 1.65 | 1947.23 | 1.26 | 9.75 | 1.06 | 0.47 | 2.25 | 0.42 | 2.17 | 0.48 | 1.94 | 109.00 | 2.10 | ||||||||||||||
| 99 | 2.33 | 73.30 | 2486.67 | 1.65 | 1947.23 | 1.26 | 9.75 | 1.06 | 0.47 | 2.25 | 0.42 | 2.17 | 0.48 | 1.94 | 109.00 | 2.10 | ||||||||||||||
| Mean | 0.00 | 50.00 | 461.62 | 0.00 | 366.00 | 0.00 | 3.94 | 0.00 | 0.27 | 0.00 | 0.24 | 0.00 | 0.31 | 0.00 | 79.30 | 0.00 | ||||||||||||||
| DT | 1.00 | 10.00 | 1231.02 | 1.00 | 1250.29 | 1.00 | 5.48 | 1.00 | 0.09 | 1.00 | 0.08 | 1.00 | 0.09 | 1.00 | 14.11 | 1.00 | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maset-Roig, R.; Caplliure-Llopis, J.; de Bernardo, N.; Privado, J.; Alarcón-Jiménez, J.; Martín-Ruiz, J.; Botella-Navas, M.; Villarón-Casales, C.; Sancho-Cantus, D.; de la Rubia Ortí, J.E. Analysis of Heart Rate Variability in Individuals Affected by Amyotrophic Lateral Sclerosis. Sensors 2024, 24, 2355. https://doi.org/10.3390/s24072355
Maset-Roig R, Caplliure-Llopis J, de Bernardo N, Privado J, Alarcón-Jiménez J, Martín-Ruiz J, Botella-Navas M, Villarón-Casales C, Sancho-Cantus D, de la Rubia Ortí JE. Analysis of Heart Rate Variability in Individuals Affected by Amyotrophic Lateral Sclerosis. Sensors. 2024; 24(7):2355. https://doi.org/10.3390/s24072355
Chicago/Turabian StyleMaset-Roig, Rosa, Jordi Caplliure-Llopis, Nieves de Bernardo, Jesús Privado, Jorge Alarcón-Jiménez, Julio Martín-Ruiz, Marta Botella-Navas, Carlos Villarón-Casales, David Sancho-Cantus, and José Enrique de la Rubia Ortí. 2024. "Analysis of Heart Rate Variability in Individuals Affected by Amyotrophic Lateral Sclerosis" Sensors 24, no. 7: 2355. https://doi.org/10.3390/s24072355
APA StyleMaset-Roig, R., Caplliure-Llopis, J., de Bernardo, N., Privado, J., Alarcón-Jiménez, J., Martín-Ruiz, J., Botella-Navas, M., Villarón-Casales, C., Sancho-Cantus, D., & de la Rubia Ortí, J. E. (2024). Analysis of Heart Rate Variability in Individuals Affected by Amyotrophic Lateral Sclerosis. Sensors, 24(7), 2355. https://doi.org/10.3390/s24072355