
A Method to Track 3D Knee Kinematics by Multi-Channel 3D-Tracked A-Mode Ultrasound

 , , , ,
, , , ,
Abstract
:1. Introduction
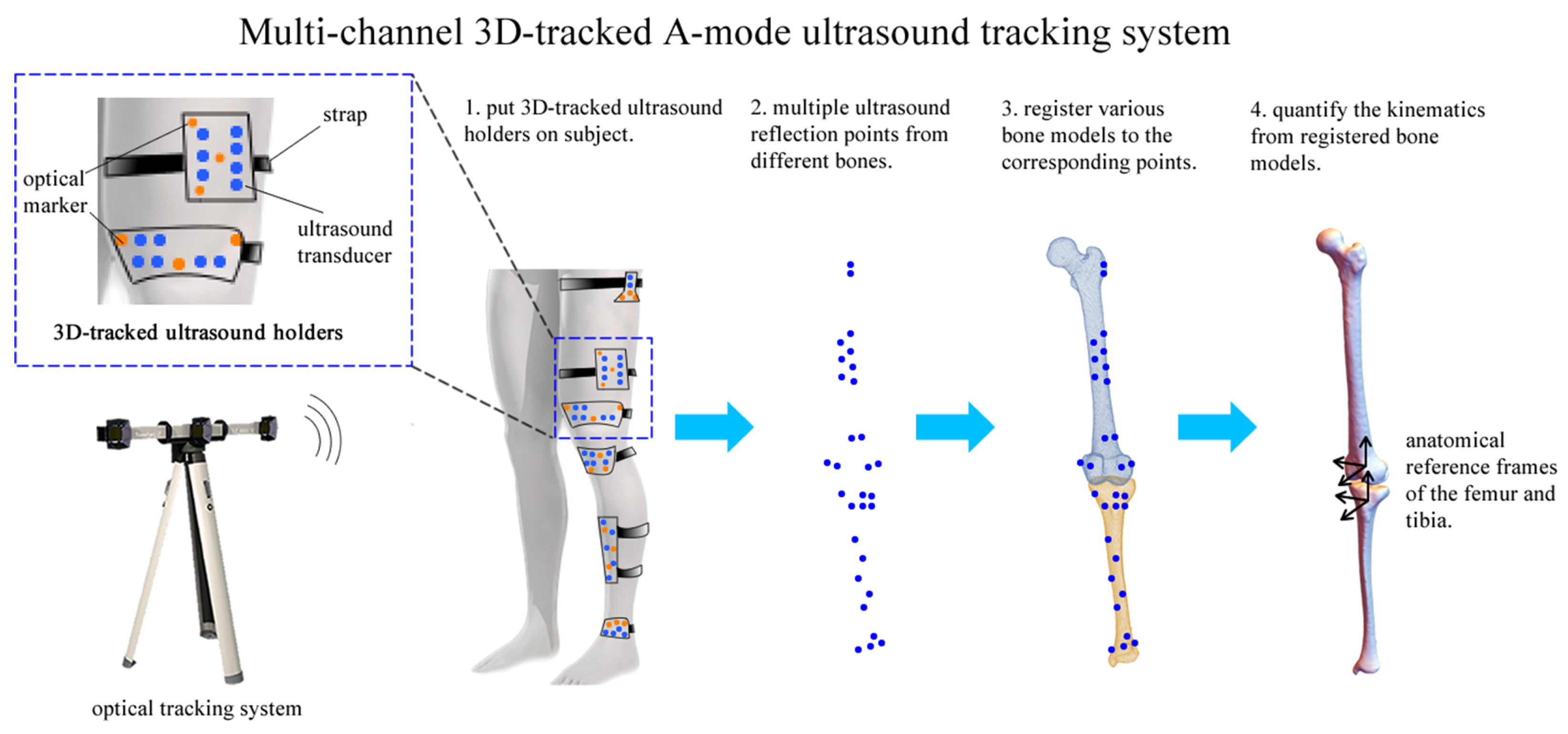
2. System Design and Method
2.1. Data Acquisition
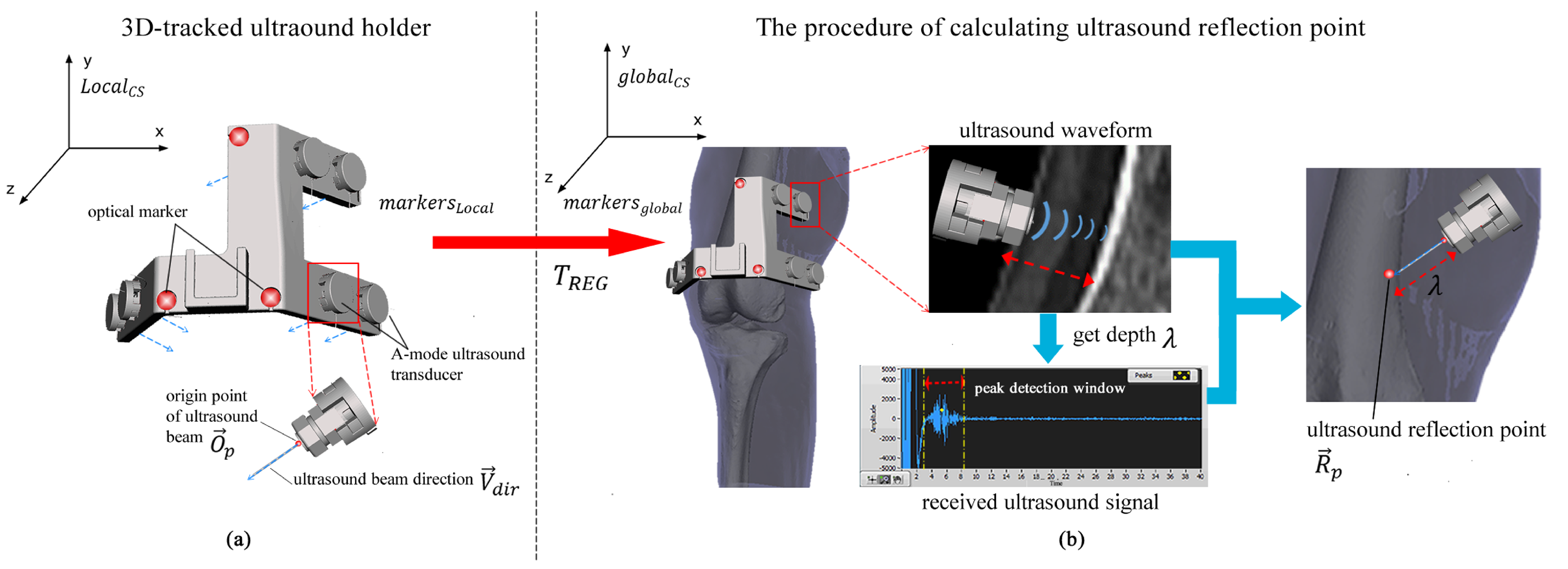
2.2. Working Principle
2.3. Ultrasound Signal Processing
2.4. Tibiofemoral Pose Estimation
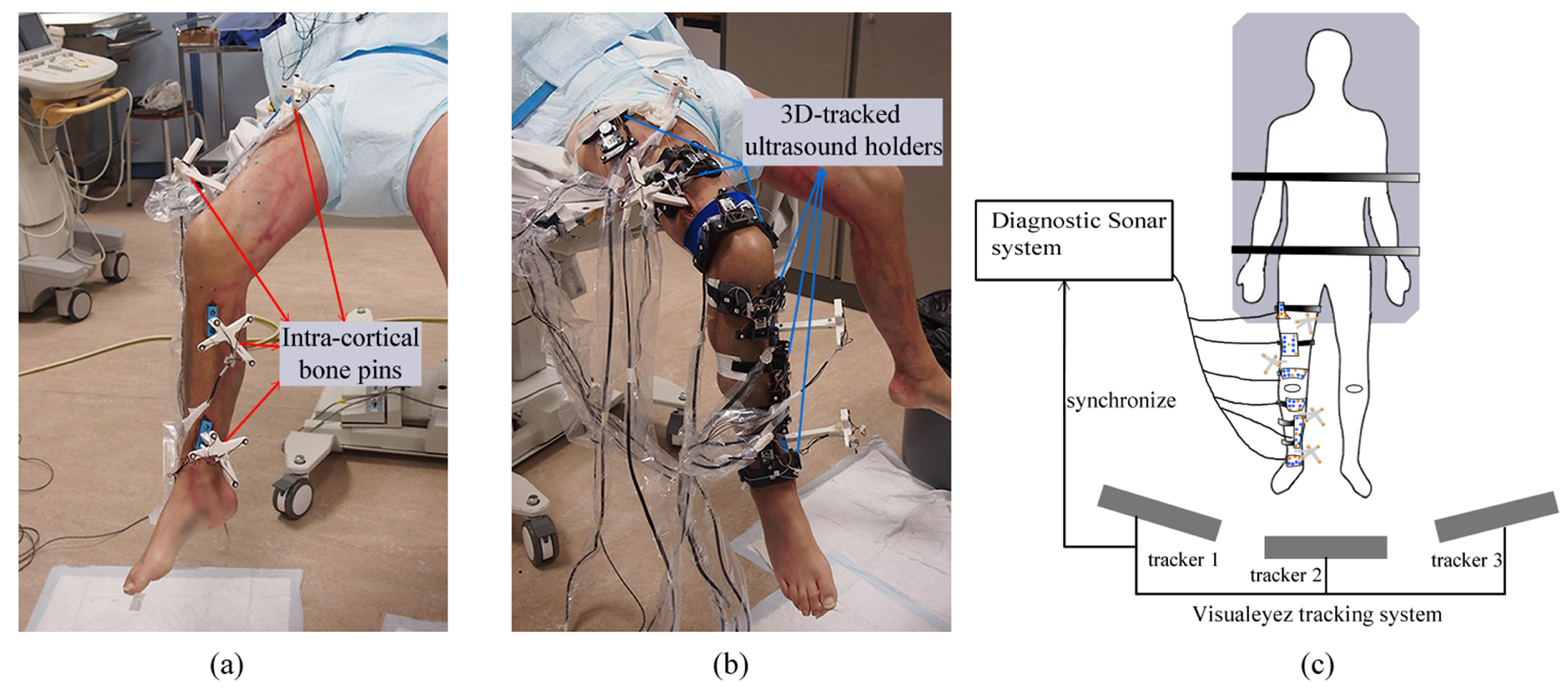
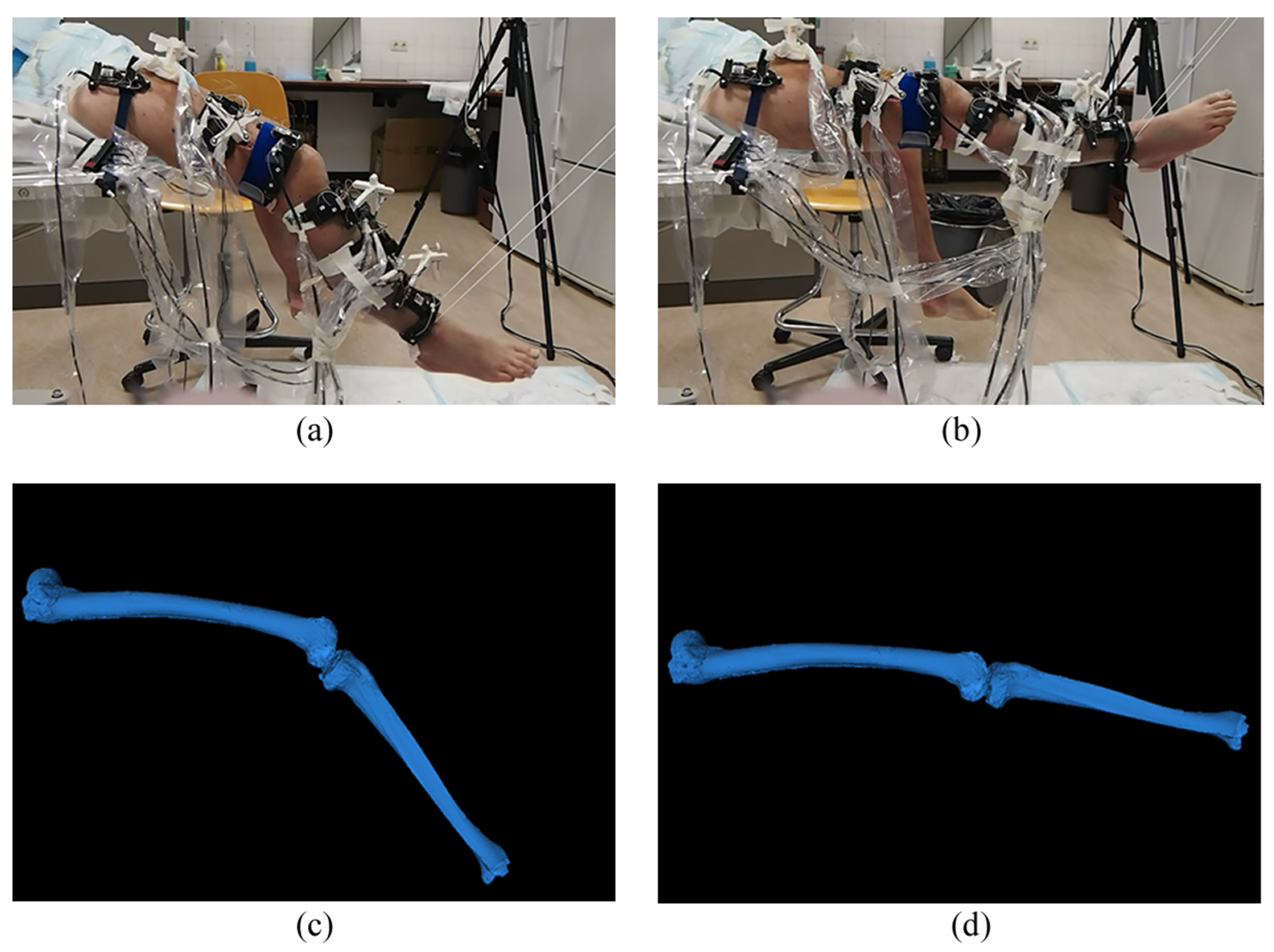
2.5. Cadaver Experiment
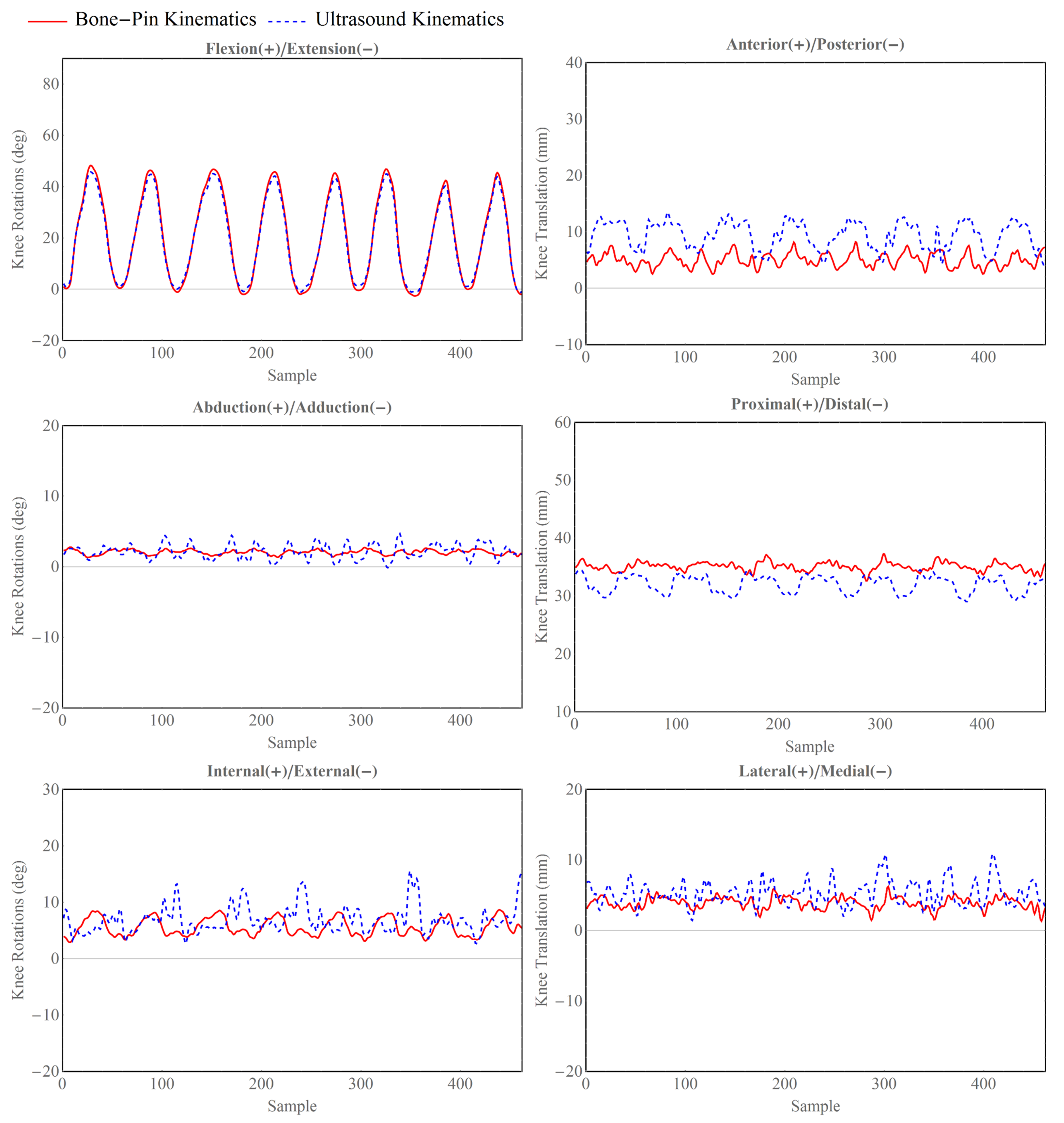
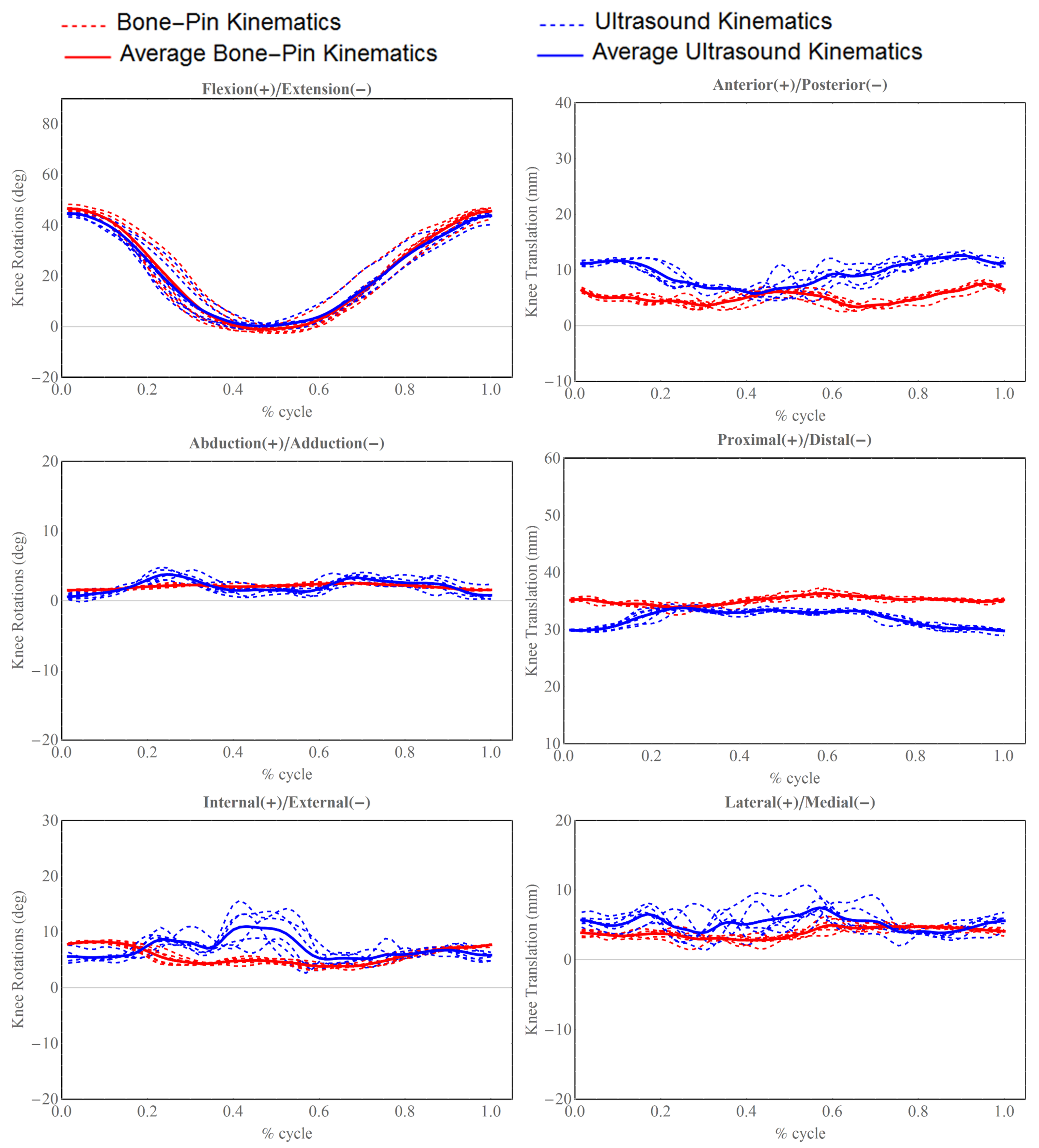
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| US | Ultrasound |
| DOF | Degrees of freedom |
| STA | Soft tissue artifact |
| SD | Standard deviation |
| RMS | Root mean square |
| Flex | Flexion rotation |
| Ext | Extension rotation |
| Add | Adduction rotation |
| Abd | Abduction rotation |
| Ext | External rotation |
| Int | Internal rotation |
| Ant | Anterior translation |
| Post | Posterior translation |
| Prox | Proximal translation |
| Dist | Distal translation |
| Lat | Lateral translation |
| Med | Medial translation |
References
- Keelson, B.; Buzzatti, L.; Ceranka, J.; Gutiérrez, A.; Battista, S.; Scheerlinck, T.; Van Gompel, G.; De Mey, J.; Cattrysse, E.; Buls, N.; et al. Automated Motion Analysis of Bony Joint Structures from Dynamic Computer Tomography Images: A Multi-Atlas Approach. Diagnostics 2021, 11, 2062. [Google Scholar] [CrossRef] [PubMed]
- Maiwald, C.; Arndt, A.; Nester, C.; Jones, R.; Lundberg, A.; Wolf, P. The effect of intracortical bone pin application on kinetics and tibiocalcaneal kinematics of walking gait. Gait Posture 2017, 52, 129–134. [Google Scholar] [CrossRef]
- Slater, A.A.; Hullfish, T.J.; Baxter, J.R. The impact of thigh and shank marker quantity on lower extremity kinematics using a constrained model. BMC Musculoskelet. Disord. 2018, 19, 399. [Google Scholar] [CrossRef] [PubMed]
- Niu, K.; Anijs, T.; Sluiter, V.; Homminga, J.; Sprengers, A.; Marra, M.A.; Verdonschot, N. In situ comparison of A-mode ultrasound tracking system and skin-mounted markers for measuring kinematics of the lower extremity. J. Biomech. 2018, 72, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.K.; Seth, A. Conclusion or Illusion: Quantifying Uncertainty in Inverse Analyses From Marker-Based Motion Capture due to Errors in Marker Registration and Model Scaling. Front. Bioeng. Biotechnol. 2022, 10, 874725. [Google Scholar] [CrossRef] [PubMed]
- Li, J.D.; Lu, T.W.; Lin, C.C.; Kuo, M.Y.; Hsu, H.C.; Shen, W.C. Soft tissue artefacts of skin markers on the lower limb during cycling: Effects of joint angles and pedal resistance. J. Biomech. 2017, 62, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Lu, T.W.; Li, J.D.; Kuo, M.Y.; Kuo, C.C.; Hsu, H.C. An automated three-dimensional bone pose tracking method using clinical interleaved biplane fluoroscopy systems: Application to the knee. Appl. Sci. 2020, 10, 8426. [Google Scholar] [CrossRef]
- Lin, C.C.; Lu, H.L.; Lu, T.W.; Wang, C.Y.; Li, J.D.; Kuo, M.Y.; Hsu, H.C. Reconstruction of Three-Dimensional Tibiofemoral Kinematics Using Single-Plane Fluoroscopy and a Personalized Kinematic Model. Appl. Sci. 2021, 11, 9415. [Google Scholar] [CrossRef]
- List, R.; Postolka, B.; Schütz, P.; Hitz, M.; Schwilch, P.; Gerber, H.; Ferguson, S.J.; Taylor, W.R. A moving fluoroscope to capture tibiofemoral kinematics during complete cycles of free level and downhill walking as well as stair descent. PLoS ONE 2017, 12, e0185952. [Google Scholar] [CrossRef]
- Kubicek, J.; Tomanec, F.; Cerny, M.; Vilimek, D.; Kalova, M.; Oczka, D. Recent trends, technical concepts and components of computer-assisted orthopedic surgery systems: A comprehensive review. Sensors 2019, 19, 5199. [Google Scholar] [CrossRef]
- Wein, W.; Karamalis, A.; Baumgartner, A.; Navab, N. Automatic bone detection and soft tissue aware ultrasound–CT registration for computer-aided orthopedic surgery. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 971–979. [Google Scholar] [CrossRef]
- Niu, K.; Homminga, J.; Sluiter, V.I.; Sprengers, A.; Verdonschot, N. Feasibility of A-mode ultrasound based intraoperative registration in computer-aided orthopedic surgery: A simulation and experimental study. PLoS ONE 2018, 13, e0199136. [Google Scholar] [CrossRef] [PubMed]
- Masum, M.A.; Pickering, M.; Lambert, A.; Scarvell, J.; Smith, P. Accuracy assessment of Tri-plane B-mode ultrasound for non-invasive 3D kinematic analysis of knee joints. Biomed. Eng. Online 2014, 13, 122. [Google Scholar] [CrossRef] [PubMed]
- Hamidzada, W.A.; Osuobeni, E.P. Agreement between A-mode and B-mode ultrasonography in the measurement of ocular distances. Vet. Radiol. Ultrasound 1999, 40, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Niu, K.; Homminga, J.; Sluiter, V.; Sprengers, A.; Verdonschot, N. Measuring relative positions and orientations of the tibia with respect to the femur using one-channel 3D-tracked A-mode ultrasound tracking system: A cadaveric study. Med. Eng. Phys. 2018, 57, 61–68. [Google Scholar] [CrossRef]
- Horn, B.K. Closed-form solution of absolute orientation using unit quaternions. JOSA A 1987, 4, 629–642. [Google Scholar] [CrossRef]
- Fieten, L.; Schmieder, K.; Engelhardt, M.; Pasalic, L.; Radermacher, K.; Heger, S. Fast and accurate registration of cranial CT images with A-mode ultrasound. Int. J. Comput. Assist. Radiol. Surg. 2009, 4, 225–237. [Google Scholar] [CrossRef]
- Mozes, A.; Chang, T.C.; Arata, L.; Zhao, W. Three-dimensional A-mode ultrasound calibration and registration for robotic orthopaedic knee surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2010, 6, 91–101. [Google Scholar] [CrossRef]
- Barratt, D.C.; Penney, G.P.; Chan, C.S.; Slomczykowski, M.; Carter, T.J.; Edwards, P.J.; Hawkes, D.J. Self-calibrating 3D-ultrasound-based bone registration for minimally invasive orthopedic surgery. IEEE Trans. Med. Imaging 2006, 25, 312–323. [Google Scholar] [CrossRef]
- Besl, P.J.; McKay, N.D. Method for registration of 3-D shapes. In Proceedings of the Sensor Fusion IV: Control Paradigms and Data Structures, Boston, MA, USA, 14–15 November 1991; SPIE: Bellingham, WA, USA, 1992; Volume 1611, pp. 586–606. [Google Scholar]
- Ma, B.; Ellis, R.E. Robust registration for computer-integrated orthopedic surgery: Laboratory validation and clinical experience. Med. Image Anal. 2003, 7, 237–250. [Google Scholar] [CrossRef]
- Maurer, C.R.; Maciunas, R.J.; Fitzpatrick, J.M. Registration of head CT images to physical space using a weighted combination of points and surfaces [image-guided surgery]. IEEE Trans. Med. Imaging 1998, 17, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Miranda, D.L.; Rainbow, M.J.; Leventhal, E.L.; Crisco, J.J.; Fleming, B.C. Automatic determination of anatomical coordinate systems for three-dimensional bone models of the isolated human knee. J. Biomech. 2010, 43, 1623–1626. [Google Scholar] [CrossRef] [PubMed]
- Grood, E.; Suntay, W. A joint coordinate system for the clinical description of three-dimensional motions: Application to the knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef]
- Guan, S.; Gray, H.A.; Schache, A.G.; Feller, J.; de Steiger, R.; Pandy, M.G. In vivo six-degree-of-freedom knee-joint kinematics in overground and treadmill walking following total knee arthroplasty. J. Orthop. Res. 2017, 35, 1634–1643. [Google Scholar] [CrossRef] [PubMed]
- Gray, H.A.; Guan, S.; Pandy, M.G. Accuracy of mobile biplane X-ray imaging in measuring 6-degree-of-freedom patellofemoral kinematics during overground gait. J. Biomech. 2017, 57, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Guan, S.; Gray, H.A.; Keynejad, F.; Pandy, M.G. Mobile biplane X-ray imaging system for measuring 3D dynamic joint motion during overground gait. IEEE Trans. Med. Imaging 2015, 35, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Matsumura, N.; Yamada, Y.; Yamada, M.; Yokoyama, Y.; Miyamoto, A.; Nakamura, M.; Nagura, T.; Jinzaki, M. Three-Dimensional Quantitative Evaluation of the Scapular Skin Marker Movements in the Upright Posture. Sensors 2022, 22, 6502. [Google Scholar] [CrossRef] [PubMed]
- Ancillao, A.; Aertbeliën, E.; De Schutter, J. Effect of the soft tissue artifact on marker measurements and on the calculation of the helical axis of the knee during a gait cycle: A study on the CAMS-Knee data set. Hum. Mov. Sci. 2021, 80, 102866. [Google Scholar] [CrossRef]
- Niu, K.; Sluiter, V.; Homminga, J.; Sprengers, A.; Verdonschot, N. A novel ultrasound-based lower extremity motion tracking system. In Intelligent Orthopaedics: Artificial Intelligence and Smart Image-Guided Technology for Orthopaedics; Springer: Singapore, 2018; pp. 131–142. [Google Scholar]
- Benoit, D.L.; Ramsey, D.K.; Lamontagne, M.; Xu, L.; Wretenberg, P.; Renström, P. Effect of skin movement artifact on knee kinematics during gait and cutting motions measured in vivo. Gait Posture 2006, 24, 152–164. [Google Scholar] [CrossRef]
- Afshari, P.; Zakian, C.; Ntziachristos, V. Improving ultrasound images with elevational angular compounding based on acoustic refraction. Sci. Rep. 2020, 10, 18173. [Google Scholar] [CrossRef]
- Patey, S.J.; Corcoran, J.P. Physics of ultrasound. Anaesth. Intensive Care Med. 2021, 22, 58–63. [Google Scholar] [CrossRef]
- Chang, T.; Mozes, A.; Arata, L.; Zhao, W. A-Mode Ultrasound Bone Registration for Computer-Assisted Knee Surgery: Calibration and Robustness Test. In Proceedings of the 25th Southern Biomedical Engineering Conference 2009, Miami, FL, USA, 15–17 May 2009; Springer: Berlin/Heidelberg, Germany, 2009; pp. 97–100. [Google Scholar]
- Zhang, Q.; Iyer, A.; Sun, Z.; Kim, K.; Sharma, N. A dual-modal approach using electromyography and sonomyography improves prediction of dynamic ankle movement: A case study. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1944–1954. [Google Scholar] [CrossRef] [PubMed]
- Mobarak, R.; Tigrini, A.; Verdini, F.; Al-Timemy, A.H.; Fioretti, S.; Burattini, L.; Mengarelli, A. A Minimal and Multi-Source Recording Setup for Ankle Joint Kinematics Estimation During Walking using only Proximal Information from Lower Limb. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Mendez, J.; Murray, R.; Gabert, L.; Fey, N.P.; Liu, H.; Lenzi, T. A-mode ultrasound-based prediction of transfemoral amputee prosthesis walking kinematics via an artificial neural network. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 1511–1520. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Joint Rotational Errors (°) | Joint Translational Errors (mm) | ||||
|---|---|---|---|---|---|
| Flex/Ext | Add/Abd | Ext/Int | Ant/Post | Prox/Dist | |
| Mean | 1.32 | 0.71 | 2.49 | 4.55 | 3.08 |
| SD | 0.73 | 0.52 | 2.14 | 2.17 | 1.57 |
| RMS | 1.51 | 0.88 | 3.28 | 5.04 | 3.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niu, K.; Sluiter, V.; Lan, B.; Homminga, J.; Sprengers, A.; Verdonschot, N. A Method to Track 3D Knee Kinematics by Multi-Channel 3D-Tracked A-Mode Ultrasound. Sensors 2024, 24, 2439. https://doi.org/10.3390/s24082439
Niu K, Sluiter V, Lan B, Homminga J, Sprengers A, Verdonschot N. A Method to Track 3D Knee Kinematics by Multi-Channel 3D-Tracked A-Mode Ultrasound. Sensors. 2024; 24(8):2439. https://doi.org/10.3390/s24082439
Chicago/Turabian StyleNiu, Kenan, Victor Sluiter, Bangyu Lan, Jasper Homminga, André Sprengers, and Nico Verdonschot. 2024. "A Method to Track 3D Knee Kinematics by Multi-Channel 3D-Tracked A-Mode Ultrasound" Sensors 24, no. 8: 2439. https://doi.org/10.3390/s24082439