The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy




Abstract
:1. Introduction
2. Clinical Benefits of Vonoprazan
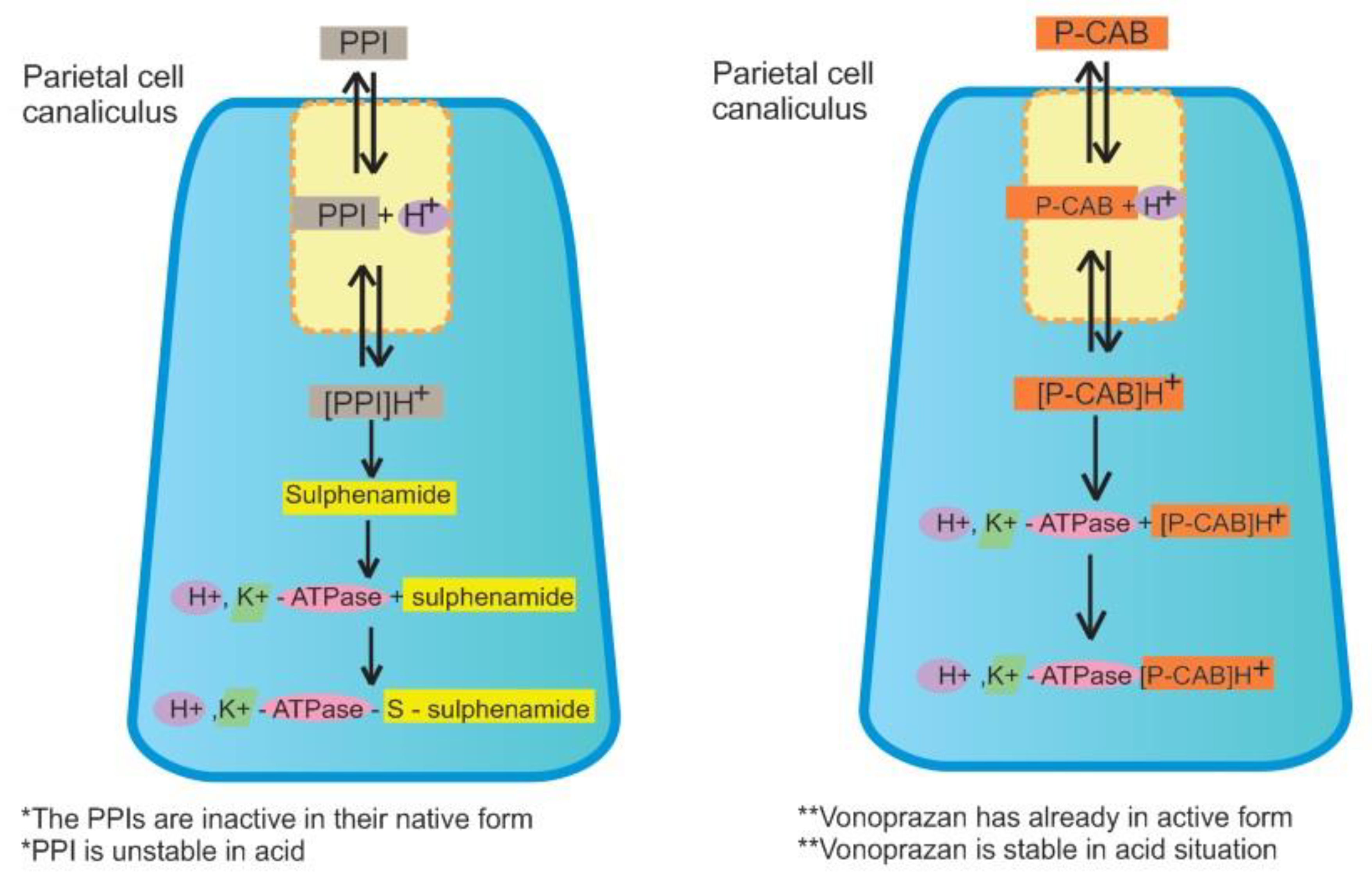
2.1. Pharmacological Aspects
2.2. Vonoprazan and H. pylori Eradication
2.3. Safety and Adverse Events
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hu, Y.; Wan, J.H.; Li, X.Y.; Zhu, Y.; Graham, D.Y.; Lu, N.H. Systematic review with meta-analysis: The global recurrence rate of Helicobacter pylori. Aliment. Pharmacol. Ther. 2017, 46, 773–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Y.; Zhou, L.Y.; Lu, H.P.; Liu, J.Z.; Guo, L.S. Recurrence of Helicobacter pylori infection: Incidence and influential factors. Chin. Med. J. (Engl.) 2019, 132, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Sjomina, O.; Pavlova, J.; Niv, Y.; Leja, M. Epidemiology of Helicobacter pylori infection. Helicobacter 2018, 23, 6–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Syam, A.F.; Miftahussurur, M.; Makmun, D.; Nusi, I.A.; Zain, L.H.; Zulkhairi; Akil, F.; Uswan, W.B.; Simanjuntak, D.; Uchida, T.; et al. Risk factors and prevalence of Helicobacter pylori in five largest islands of Indonesia: A preliminary study. PLoS ONE 2015, 10, e0140186. [Google Scholar] [CrossRef]
- Abadi, A.T.B.; Ierardi, E. Vonoprazan and Helicobacter pylori treatment: A lesson from Japan or a limited geographic phenomenon? Front. Pharmacol. 2019, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Lyu, Q.J.; Pu, Q.H.; Zhong, X.F.; Zhang, J. Efficacy and safety of vonoprazan-based versus proton pump inhibitor-based triple therapy for Helicobacter pylori eradication: A meta-analysis of randomized clinical trials. BioMed Res. Int. 2019, 2019, 9781212–9781218. [Google Scholar] [CrossRef] [Green Version]
- Floch, P.; Mégraud, F.; Lehours, P. Helicobacter pylori strains and gastric MALT lymphoma. Toxins 2017, 9, 132. [Google Scholar] [CrossRef]
- Graham, D.Y.; Miftahussurur, M. Helicobacter pylori urease for diagnosis of Helicobacter pylori infection: A mini review. J. Adv. Res. 2018, 13, 51–57. [Google Scholar] [CrossRef]
- Seta, T.; Takahashi, Y.; Noguchi, Y.; Shikata, S.; Sakai, T.; Sakai, K.; Yamashita, Y.; Nakayama, T. Effectiveness of Helicobacter pylori eradication in the prevention of primary gastric cancer in healthy asymptomatic people: A systematic review and meta-analysis comparing risk ratio with risk difference. PLoS ONE 2017, 12, e0183321. [Google Scholar] [CrossRef]
- Ford, A.; Forman, D.; Hunt, R.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication for the prevention of gastric neoplasia. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Suzuki, H.; Mori, H. World trends for H. pylori eradication therapy and gastric cancer prevention strategy by H. pylori test-and-treat. J. Gastroenterol. 2018, 53, 354–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.R.; Sachs, G.; Marcus, E.A. The role of acid inhibition in Helicobacter pylori eradication. F1000Research 2016, 5, 1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ierardi, E.; Losurdo, G.; La Fortezza, R.F.; Principi, M.; Barone, M.; Leo, A. Di Optimizing proton pump inhibitors in Helicobacter pylori treatment: Old and new tricks to improve effectiveness. World J. Gastroenterol. 2019, 25, 5097–5104. [Google Scholar] [CrossRef] [PubMed]
- Putra, B.P.; Miftahussurur, M. Vonoprazan-based therapy has lower failure rate in eradicating Helicobacter pylori compared to proton pum inhibitors-based therapy: A meta-analysis of randomized controlled trials. New Armen. Med. J. 2019, 13, 22–30. [Google Scholar]
- Graham, D.Y.; Dore, M.P. Update on the use of vonoprazan: A competitive acid blocker. Gastroenterology 2018, 154, 462–466. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Inatomi, N.; Matsukawa, J.; Sakurai, Y.; Otake, K. Potassium-competitive acid blockers: Advanced therapeutic option for acid-related diseases. Pharmacol. Ther. 2016, 168, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P.; Sunkara, T.; Ofosu, A.; Gaduputi, V. Potassium-competitive acid blockers - are they the next generation of proton pump inhibitors? World J. Gastrointest. Pharmacol. Ther. 2018, 9, 63–68. [Google Scholar] [CrossRef]
- Kato, M.; Ota, H.; Okuda, M.; Kikuchi, S.; Satoh, K.; Shimoyama, T.; Suzuki, H.; Handa, O.; Furuta, T.; Mabe, K.; et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2016 Revised Edition. Helicobacter 2019, 24, e12597. [Google Scholar] [CrossRef]
- Mori, H.; Suzuki, H. Role of acid suppression in acid-related diseases: Proton pump inhibitor and potassium-competitive acid blocker. J. Neurogastroenterol. Motil. 2019, 25, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.J.; Son, B.K.; Kim, G.H.; Jung, H.K.; Jung, H.Y.; Chung, I.K.; Sung, I.K.; Kim, J.I.; Kim, J.H.; Lee, J.S.; et al. Randomised phase 3 trial: Tegoprazan, a novel potassium-competitive acid blocker, vs. esomeprazole in patients with erosive oesophagitis. Aliment. Pharmacol. Ther. 2019, 49, 864–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Take, Y. Tegoprazan, a novel potassium-competitive acid blocker to control gastric acid secretion and motility. J. Pharmacol. Exp. Ther. 2018, 364, 275–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwakiri, K.; Kinoshita, Y.; Habu, Y.; Oshima, T.; Manabe, N.; Fujiwara, Y.; Nagahara, A.; Kawamura, O.; Iwakiri, R.; Ozawa, S.; et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. J. Gastroenterol. 2016, 51, 751–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG clinical guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–238. [Google Scholar] [CrossRef]
- Syam, A.F.; Simadibrata, M.; Makmun, D.; Abdullah, M.; Fauzi, A.; Renaldi, K.; Maulahela, H.; Utari, A.P. National consensus on management of dyspepsia and Helicobacter pylori infection. Acta Med. Indones. 2017, 49, 279–287. [Google Scholar]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016, 151, 51–69.e4. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.Y.; Shim, K.N.; Tae, C.H.; Lee, K.E.; Lee, J.; Lee, K.H.; Moon, C.M.; Kim, S.E.; Jung, H.K.; Jung, S.A. Triple therapy versus sequential therapy for the first-line Helicobacter pylori eradication. BMC Gastroenterol. 2017, 17, 16. [Google Scholar] [CrossRef] [Green Version]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Miftahussurur, M.; Yamaoka, Y. Appropriate first-line regimens to combat Helicobacter pylori antibiotic resistance: An Asian perspective. Molecules 2015, 20, 6068–6092. [Google Scholar] [CrossRef] [Green Version]
- Miftahussurur, M.; Shrestha, P.K.; Subsomwong, P.; Sharma, R.P.; Yamaoka, Y. Emerging Helicobacter pylori levofloxacin resistance and novel genetic mutation in Nepal. BMC Microbiol. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shetty, V.; Lamichhane, B.; Tay, C.Y.; Pai, G.C.; Lingadakai, R.; Balaraju, G.; Shetty, S.; Ballal, M.; Chua, E.G. High primary resistance to metronidazole and levofloxacin, and a moderate resistance to clarithromycin in Helicobacter pylori isolated from Karnataka patients. Gut Pathog. 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Miftahussurur, M.; Waskito, L.A.; Syam, A.F.; Nusi, I.A.; Siregar, G.; Richardo, M.; Bakry, A.F.; Rezkitha, Y.A.A.; Wibawa, I.D.N.; Yamaoka, Y. Alternative eradication regimens for helicobacter pylori infection in indonesian regions with high metronidazole and levofloxacin resistance. Infect. Drug Resist. 2019, 12, 345–358. [Google Scholar] [CrossRef] [Green Version]
- Echizen, H. The first-in-class potassium-competitive acid blocker, vonoprazan fumarate: Pharmacokinetic and pharmacodynamic considerations. Clin. Pharmacokinet. 2016, 55, 409–418. [Google Scholar] [CrossRef]
- Jenkins, H.; Sakurai, Y.; Nishimura, A.; Okamoto, H.; Hibberd, M.; Jenkins, R.; Yoneyama, T.; Ashida, K.; Ogama, Y.; Warrington, S. Randomised clinical trial: Safety, tolerability, pharmacokinetics and pharmacodynamics of repeated doses of TAK-438 (vonoprazan), a novel potassium-competitive acid blocker, in healthy male subjects. Aliment. Pharmacol. Ther. 2015, 41, 636–648. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, Y.; Nishimura, A.; Kennedy, G.; Hibberd, M.; Jenkins, R.; Okamoto, H.; Yoneyama, T.; Jenkins, H.; Ashida, K.; Irie, S.; et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of single rising Tak-438 (Vonoprazan) doses in healthy male Japanese/Non-Japanese Subjects. Clin. Transl. Gastroenterol. 2015, 6, e94. [Google Scholar] [CrossRef]
- Shin, J.M.; Inatomi, N.; Munson, K.; Strugatsky, D.; Tokhtaeva, E.; Vagin, O.; Sachs, G. Characterization of a Novel Potassium-Competitive Acid Blocker of the Gastric H,K-ATPase, 1-[5-(2-Fluorophenyl)-1-(pyridin-3-ylsulfonyl)-1H-pyrrol-3-yl]-N-methylmethanamine Monofumarate (TAK-438). J. Pharmacol. Exp. Ther. 2011, 339, 412–420. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Li, Y.; Sun, Y.; Zhang, M.; Guo, C.; Mirza, I.A.; Li, Y.Q. Vonoprazan: A novel and potent alternative in the treatment of acid-related diseases. Dig. Dis. Sci. 2018, 63, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, C.; Wang, S.; Zhou, Q.; Dai, D.; Shi, J.; Xu, X.; Luo, Q. Cytochrome P450-based drug-drug interactions of vonoprazan in vitro and in vivo. Front. Pharmacol. 2020, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, H.; Jenkins, R.; Patat, A. Effect of multiple oral doses of the potent CYP3A4 inhibitor clarithromycin on the pharmacokinetics of a single oral dose of vonoprazan: A phase I, open-label, sequential design study. Clin. Drug Investig. 2017, 37, 311–316. [Google Scholar] [CrossRef]
- Kagami, T.; Sahara, S.; Ichikawa, H.; Uotani, T.; Yamade, M.; Sugimoto, M.; Hamaya, Y.; Iwaizumi, M.; Osawa, S.; Sugimoto, K.; et al. Potent acid inhibition by vonoprazan in comparison with esomeprazole, with reference to CYP2C19 genotype. Aliment. Pharmacol. Ther. 2016, 43, 1048–1059. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Ishimura, N.; Ishihara, S. Advantages and disadvantages of long-term proton pump inhibitor use. J. Neurogastroenterol. Motil. 2018, 24, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Arai, E.; Taki, M.; Kondo, T.; Tomita, T.; Fukui, H.; Watari, J.; Miwa, H. Randomised clinical trial: Vonoprazan versus lansoprazole for the initial relief of heartburn in patients with erosive oesophagitis. Aliment. Pharmacol. Ther. 2019, 49, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oshima, T.; Miwa, H. Potent potassium-competitive acid blockers: A new era for the treatment of acid-related diseases. J. Neurogastroenterol. Motil. 2018, 24, 334–344. [Google Scholar] [CrossRef]
- Akazawa, Y.; Fukuda, D.; Fukuda, Y. Vonoprazan-based therapy for Helicobacter pylori eradication: Experience and clinical evidence. Therap. Adv. Gastroenterol. 2016, 9, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Sugano, K. Vonoprazan fumarate, a novel potassium-competitive acid blocker, in the management of gastroesophageal reflux disease: Safety and clinical evidence to date. Therap. Adv. Gastroenterol. 2018, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.; Smolka, A.J. Gastric parietal cell physiology and Helicobacter pylori–induced disease. Gastroenterology 2019, 156, 2158–2173. [Google Scholar] [CrossRef] [Green Version]
- Garnock-Jones, K.P. Vonoprazan: First global approval. Drugs 2015, 75, 439–443. [Google Scholar] [CrossRef]
- Cheng, Y.; Liu, J.; Tan, X.; Dai, Y.; Xie, C.; Li, X.; Lu, Q.; Kou, F.; Jiang, H.; Li, J. Direct comparison of the efficacy and safety of vonoprazan versus proton-pump inhibitors for gastroesophageal reflux disease: A systematic review and meta-analysis. Dig. Dis. Sci. 2020. [Google Scholar] [CrossRef]
- Ashida, K.; Sakurai, Y.; Hori, T.; Kudou, K.; Nishimura, a.; Hiramatsu, N.; Umegaki, E.; Iwakiri, K. Randomised clinical trial: Vonoprazan, a novel potassium-competitive acid blocker, vs. lansoprazole for the healing of erosive oesophagitis. Aliment. Pharmacol. Ther. 2016, 43, 240–251. [Google Scholar] [CrossRef]
- Mizokami, Y.; Oda, K.; Funao, N.; Nishimura, A.; Soen, S.; Kawai, T.; Ashida, K.; Sugano, K. Vonoprazan prevents ulcer recurrence during long-term NSAID therapy: Randomised, lansoprazole-controlled non-inferiority and single-blind extension study. Gut 2018, 67, 1042–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miwa, H.; Uedo, N.; Watari, J.; Mori, Y.; Sakurai, Y.; Takanami, Y.; Nishimura, a.; Tatsumi, T.; Sakaki, N. Randomised clinical trial: Efficacy and safety of vonoprazan vs. lansoprazole in patients with gastric or duodenal ulcers–results from two phase 3, non-inferiority randomised controlled trials. Aliment. Pharmacol. Ther. 2017, 45, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Oda, K.; Funao, N.; Nishimura, A.; Matsumoto, Y.; Mizokami, Y.; Ashida, K.; Sugano, K. Vonoprazan prevents low-dose aspirin-associated ulcer recurrence: Randomised phase 3 study. Gut 2018, 67, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Poonsombudlert, K.; Ungprasert, P. Vonoprazan versus proton-pump inhibitors for gastric endoscopic submucosal dissection-induced ulcers: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1416–1421. [Google Scholar] [CrossRef]
- Sugimoto, M.; Yamaoka, Y. Role of vonoprazan in Helicobacter pylori eradication therapy in Japan. Front. Pharmacol. 2019, 9, 1–15. [Google Scholar] [CrossRef]
- Waskito, L.A.; Miftahussurur, M.; Lusida, M.I.; Syam, A.F.; Suzuki, R.; Subsomwong, P.; Uchida, T.; Hamdan, M.; Nasronudin; Yamaoka, Y. Distribution and clinical associations of integrating conjugative elements and cag pathogenicity islands of Helicobacter pylori in Indonesia. Sci. Rep. 2018, 8, 6073. [Google Scholar] [CrossRef]
- Doohan, D.; Miftahussurur, M.; Matsuo, Y.; Kido, Y.; Akada, J.; Matsuhisa, T.; Yee, T.T.; Htet, K.; Aftab, H.; Vilaichone, R.K.; et al. Characterization of a novel Helicobacter pylori East Asian-type CagA ELISA for detecting patients infected with various cagA genotypes. Med. Microbiol. Immunol. 2020, 209, 29–40. [Google Scholar] [CrossRef]
- Subsomwong, P.; Miftahussurur, M.; Uchida, T.; Vilaichone, R.K.; Ratanachu-Ek, T.; Mahachai, V.; Yamaoka, Y. Prevalence, risk factors, and virulence genes of Helicobacter pylori among dyspeptic patients in two different gastric cancer risk regions of Thailand. PLoS ONE 2017, 12, e0187113. [Google Scholar] [CrossRef]
- Li, M.; Oshima, T.; Horikawa, T.; Tozawa, K.; Tomita, T.; Fukui, H.; Watari, J.; Miwa, H. Systematic review with meta-analysis: Vonoprazan, a potent acid blocker, is superior to proton-pump inhibitors for eradication of clarithromycin-resistant strains of Helicobacter pylori. Helicobacter 2018, 23, 1–8. [Google Scholar] [CrossRef]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, M.; Tanaka, N.; Kubota, D.; Miyajima, M.; Kimura, T.; Tokutake, K.; Imai, R.; Fujisawa, T.; Mori, H.; Matsuda, Y.; et al. Vonoprazan-based regimen is more useful than PPI-based one as a first-line Helicobacter pylori eradication: A randomized controlled trial. Can. J. Gastroenterol. Hepatol. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sue, S.; Ogushi, M.; Arima, I.; Kuwashima, H.; Nakao, S.; Naito, M.; Komatsu, K.; Kaneko, H.; Tamura, T.; Sasaki, T.; et al. Vonoprazan- vs proton-pump inhibitor-based first-line 7-day triple therapy for clarithromycin-susceptible Helicobacter pylori: A multicenter, prospective, randomized trial. Helicobacter 2018, 23, e12456. [Google Scholar] [CrossRef]
- Ozaki, H.; Harada, S.; Takeuchi, T.; Kawaguchi, S.; Takahashi, Y.; Kojima, Y.; Ota, K.; Hongo, Y.; Ashida, K.; Sakaguchi, M.; et al. Vonoprazan, a novel potassium-competitive acid blocker, should be used for the Helicobacter pylori eradication therapy as first choice: A large sample study of vonoprazan in real world compared with our randomized control trial using second-generation pro. Digestion 2018, 97, 212–218. [Google Scholar] [CrossRef]
- Suzuki, S.; Gotoda, T.; Kusano, C.; Iwatsuka, K.; Moriyama, M. The efficacy and tolerability of a triple therapy containing a potassium-competitive acid blocker compared with a 7-day PPI-based low-dose clarithromycin triple therapy. Am. J. Gastroenterol. 2016, 111, 949–956. [Google Scholar] [CrossRef]
- Shinozaki, S.; Nomoto, H.; Kondo, Y.; Sakamoto, H.; Hayashi, Y.; Yamamoto, H.; Lefor, A.K.; Osawa, H. Comparison of vonoprazan and proton pump inhibitors for eradication of Helicobacter pylori. Kaohsiung J. Med. Sci. 2016, 32, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Shichijo, S.; Hirata, Y.; Niikura, R.; Hayakawa, Y.; Yamada, A.; Mochizuki, S.; Matsuo, K.; Isomura, Y.; Seto, M.; Suzuki, N.; et al. Vonoprazan versus conventional proton pump inhibitor-based triple therapy as first-line treatment against Helicobacter pylori: A multicenter retrospective study in clinical practice. J. Dig. Dis. 2016, 17, 670–675. [Google Scholar] [CrossRef]
- Noda, H.; Noguchi, S.; Yoshimine, T.; Goji, S.; Adachi, K.; Tamura, Y.; Izawa, S.; Ebi, M.; Yamamoto, S.; Ogasawara, N.; et al. A novel potassium-competitive acid blocker improves the efficacy of clarithromycin-containing 7-day triple therapy against helicobacter pylori. J. Gastrointest. Liver Dis. 2016, 25, 283–288. [Google Scholar] [CrossRef]
- Matsumoto, H.; Shiotani, A.; Katsumata, R.; Fujita, M.; Nakato, R.; Murao, T.; Ishii, M.; Kamada, T.; Haruma, K.; Graham, D.Y. Helicobacter pylori eradication with proton pump inhibitors or potassium-competitive acid blockers: The effect of clarithromycin resistance. Dig. Dis. Sci. 2016, 61, 3215–3220. [Google Scholar] [CrossRef]
- Yamada, S.; Kawakami, T.; Nakatsugawa, Y.; Suzuki, T.; Fujii, H.; Tomatsuri, N.; Nakamura, H.; Sato, H.; Okuyama, Y.; Kimura, H.; et al. Usefulness of vonoprazan, a potassium ion-competitive acid blocker, for primary eradication of Helicobacter pylori. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 550. [Google Scholar] [CrossRef]
- Tsujimae, M.; Yamashita, H.; Hashimura, H.; Kano, C.; Shimoyama, K.; Kanamori, A.; Matsumoto, K.; Koizumi, A.; Momose, K.; Eguchi, T.; et al. A comparative study of a new class of gastric acid suppressant agent named vonoparazan versus esomeprazole for the eradication of Helicobacter pylori. Digestion 2017, 94, 240–246. [Google Scholar] [CrossRef]
- Kajihara, Y.; Shimoyama, T.; Mizuki, I. Analysis of the cost-effectiveness of using vonoprazan–amoxicillin–clarithromycin triple therapy for first-line Helicobacter pylori eradication. Scand. J. Gastroenterol. 2017, 52, 238–241. [Google Scholar] [CrossRef]
- Sakurai, K.; Suda, H.; Ido, Y.; Takeichi, T.; Okuda, A.; Hasuda, K.; Hattori, M. Comparative study: Vonoprazan and proton pump inhibitors in Helicobacter pylori eradication therapy. World J. Gastroenterol. 2017, 23, 668–675. [Google Scholar] [CrossRef]
- Sue, S.; Kuwashima, H.; Iwata, Y.; Oka, H.; Arima, I.; Fukuchi, T.; Sanga, K.; Inokuchi, Y.; Ishii, Y.; Kanno, M.; et al. The superiority of vonoprazan-based first-line triple therapy with clarithromycin: A prospective multi-center cohort study on Helicobacter pylori eradication. Intern. Med. 2017, 56, 1277–1285. [Google Scholar] [CrossRef] [Green Version]
- Nishizawa, T.; Suzuki, H.; Hibi, T. Quinolone-based therapy for Helicobacter pylori eradication. J. Clin. Biochem. Nutr. 2009, 44, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, H.; Yoshino, K.; Ando, K.; Nomura, Y.; Ohta, K.; Satoh, K.; Ichiishi, E.; Ishizuka, A.; Otake, T.; Kohgo, Y.; et al. Vonoprazan-based triple therapy is non-inferior to susceptibility-guided proton pump inhibitor-based triple therapy for Helicobacter pylori eradication. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 1–7. [Google Scholar] [CrossRef]
- Shinozaki, S.; Shinozaki, S.; Kobayashi, Y.; Osawa, H.; Sakamoto, H.; Hayashi, Y.; Yamamoto, H.; Lefor, A.K. Effectiveness and safety of vonoprazan versus proton pump inhibitors for second-line Helicobacter pylori eradication therapy: Systematic review and meta-analysis. Digestion 2020, 3223, 1–7. [Google Scholar] [CrossRef]
- Nishizawa, T.; Suzuki, H.; Fujimoto, A.; Kinoshita, H.; Yoshida, S.; Isomura, Y.; Toyoshima, A.; Kanai, T.; Yahagi, N.; Toyoshima, O. Effects of patient age and choice of antisecretory agent on success of eradication therapy for Helicobacter pylori infection. J. Clin. Biochem. Nutr. 2017, 60, 208–210. [Google Scholar] [CrossRef]
- Sue, S.; Shibata, W.; Sasaki, T.; Kaneko, H.; Irie, K.; Kondo, M.; Maeda, S. Randomized trial of vonoprazan-based versus proton-pump inhibitor-based third-line triple therapy with sitafloxacin for Helicobacter pylori. J. Gastroenterol. Hepatol. 2019, 34, 686–692. [Google Scholar] [CrossRef]
- Saito, Y.; Konno, K.; Sato, M.; Nakano, M.; Kato, Y.; Saito, H.; Serizawa, H. Vonoprazan-based third-line therapy has a higher eradication rate against sitafloxacin-resistant. Cancers 2019, 11, 116. [Google Scholar] [CrossRef] [Green Version]
- Kiyotoki, S.; Nishikawa, J.; Sakaida, I. Efficacy of vonoprazan for helicobacter pylori eradication. Intern. Med. 2020, 59, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Okamura, T.; Suga, T.; Nagaya, T.; Arakura, N.; Matsumoto, T.; Nakayama, Y.; Tanaka, E. Antimicrobial resistance and characteristics of eradication therapy of Helicobacter pylori in Japan: A multi-generational comparison. Helicobacter 2014, 19, 214–220. [Google Scholar] [CrossRef]
- Miftahussurur, M.; Aftab, H.; Shrestha, P.K.; Sharma, R.P.; Subsomwong, P.; Waskito, L.A.; Doohan, D.; Fauzia, K.A.; Yamaoka, Y. Effective therapeutic regimens in two South Asian countries with high resistance to major Helicobacter pylori antibiotics. Antimicrob. Resist. Infect. Control. 2019, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, P.H.; Tawar, M.G. Pharmacognostic and phytopharmacological overview on Bombax ceiba. Syst. Rev. Pharm. 2019, 10, 20–25. [Google Scholar] [CrossRef]
- Ratnasari, N.; Rezkitha, Y.A.A.; Adnyana, I.K.; Alfaray, R.I.; Fauzia, K.A.; Doohan, D.; Panjaitan, A.; Priskila, Y.; Yulinah, E.; Khomsan, A.; et al. Anti-helicobacter pylori effects of propolis ethanol extract on clarithromycin and metronidazole resistant strains. Syst. Rev. Pharm. 2020, 11, 429–434. [Google Scholar] [CrossRef]
- Scott, D.R.; Munson, K.B.; Marcus, E.A.; Lambrecht, N.W.G.; Sachs, G. The binding selectivity of vonoprazan (TAK-438) to the gastric H+,K+-ATPase. Aliment. Pharmacol. Ther. 2015, 42, 1315–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundell, L.; Vieth, M.; Gibson, F.; Nagy, P.; Kahrilas, P.J. Systematic review: The effects of long-term proton pump inhibitor use on serum gastrin levels and gastric histology. Aliment. Pharmacol. Ther. 2015, 42, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Sundaresan, S.; Kang, A.J.; Merchant, J.L. Pathophysiology of gastric NETs: Role of gastrin and menin. Curr. Gastroenterol. Rep. 2017, 19, 1–12. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Fossmark, R.; Waldum, H.L. The phylogeny and biological function of gastric juice—Microbiological consequences of removing gastric acid. Int. J. Mol. Sci. 2019, 20, 6031. [Google Scholar] [CrossRef] [Green Version]
- Bruno, G.; Zaccari, P.; Rocco, G.; Scalese, G.; Panetta, C.; Porowska, B.; Pontone, S.; Severi, C. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J. Gastroenterol. 2019, 25, 2706–2719. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J. Proton pump inhibitors and risk of vitamin and mineral deficiency: Evidence and clinical implications. Ther. Adv. Drug Saf. 2013, 4, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Kristanto, A.; Adiwinata, R.; Rasidi, J.; Phang, B.B.; Adiwinata, S.; Richard, T.; Uwan, W.B.; Syam, A.F. Long-term risks of proton pump inhibitor administration: A literature review. Indones. J. Gastroenterol. Hepatol. Dig. Endosc. 2017, 18, 169–176. [Google Scholar] [CrossRef]
- Maes, M.L.; Fixen, D.R.; Linnebur, S.A. Adverse effects of proton-pump inhibitor use in older adults: A review of the evidence. Ther. Adv. Drug Saf. 2017, 8, 273–297. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Singh, A.; Habib, A.; Najmi, A.K. Proton pump inhibitors use and risk of chronic kidney disease: Evidence-based meta-analysis of observational studies. Clin. Epidemiol. Glob. Health 2019, 7, 46–52. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| American College of Gastroenterology [25] Indonesian Society of Gastroenterology [26] | Japanese Society for Helicobacter Research [20] | The Toronto Consensus [27] | The Maastricht V/Florence Consensus Report [17] | |
|---|---|---|---|---|
| First Line | If Clarithromycin-resistant strains < 20% PPI * Amoxicillin Clarithromycin If Clarithromycin-resistant strains > 20% PPI * Bismuth subsalicylate Metronidazole Tetracycline | PPI * or Vonoprazan Amoxicillin Clarithromycin | If Clarithromycin-resistant strains < 15% PPI * Amoxicillin/Metronidazole Clarithromycin If Clarithromycin-resistant strains > 15% PPI * Amoxicillin Metronidazole Clarithromycin or PPI * Bismuth Metronidazole Tetracycline | If Clarithromycin-resistant strains < 15% PPI * Amoxicillin Clarithromycin If Clarithromycin-resistant strains > 15% PPI * Amoxicillin Metronidazole |
| Second Line | PPI * Bismuth subsalicylate Metronidazole or PPI * Amoxicillin Levofloxacin | PPI * Amoxicillin Metronidazole | PPI * Amoxicillin Levofloxacin or PPI * Bismuth Metronidazole Tetracycline | PPI * Amoxicillin Levofloxacin or PPI * Bismuth Metronidazole Tetracycline |
| Third Line | PPI * Amoxicillin Levofloxacin Rifabutin | PPI * Amoxicillin/Metronidazole Sitafloxacin | PPI * Amoxicillin Rifabutin | Regimens based on the bacterial culture susceptibility test |
| Parameter | PPI | Vonoprazan | |
|---|---|---|---|
| First Generation PPI | Second Generation PPI | ||
| Acid activation | Yes | No | |
| Active drug | No | Yes | |
| Acid Stability | No | Yes | |
| Main P450 metabolizer | CYP2C19 | CYP3A4 | |
| Meal’s influence | Yes | No | |
| Mechanism of Action | Covalent bond to gastric proton pump | Potassium ion competitive reversible inhibitor to gastric proton pump | |
| Days required for reaching maximal acid suppression | 3–5 | 1 | |
| pH > 4 holding time (%) | OMZ 30.4 LPZ 39.1 | ESO 43.1 RPZ 42.8 | 10 mg 38.4–43.1 20 mg 62.7–63.3 |
| Time Needed to Reach Maximum Plasma Concentration (h) | OMZ 1–4 LPZ 1.2–2.1 | ESO 1–3.5 RPZ 1.14 | 10 mg 1.75 20 mg 1.50 |
| Half-life (h) | OMZ 0.5–1.2 LPZ 0.9–2.1 | ESO 1.3–1.6 RPZ 0.6–1.4 | 10 mg 6.95 ± 1.03 20 mg 6.85 ± 0.80 |
| Cmax (μmol/L) | OMZ 0.23–23.2 LPZ 1.62–3.25 | ESO 2.1–2.4 RPZ 1.14 | 10 mg 9.7 ± 2.1 μg/L 20 mg 25.0 ± 5.6 μg/L |
| AUC (μmol.h/L) | OMZ 0.58–3.47 LPZ 4.60–13.5 | ESO 4.2 RPZ 2.22 | 10 mg 60.1 ± 9.0 μg.h/L 20 mg 160.3 ± 38.6 μg.h/L |
| Study | VPZ-Based Regimen | PPI-Based Regimen | ||
|---|---|---|---|---|
| Regimen | Eradication Rate | Regimen | Eradication Rate | |
| RCT | ||||
| Murakami et al., 2016 [60] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 90.9% | LPZ: 30 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 75.1% |
| Maruyama et al., 2017 [61] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 95.8% | LPZ: 30 mg bid or RPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 69.6% |
| Sue et al., 2017 [62] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 87.3% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 76.5% |
| Ozaki et al., 2018 [63] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 90.9% | RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 72.8% |
| Non-RCT | ||||
| Suzuki et al., 2016 [64] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 89.0% | LPZ: 30 mg bid or RPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 74.2% |
| Shinozaki et al., 2016 [65] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 82.9% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 73.9% |
| Shichijo et al., 2016 [66] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 87.2% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 72.4% |
| Noda et al., 2016 [67] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 400 mg bid | 89.7% | OMZ: 20 mg bid, LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 73.9% |
| Matsumoto et al., 2016 [68] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 89.6% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 71.9% |
| Yamada et al., 2016 [69] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 85.7% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 73.2% |
| Tsujimae et al., 2016 [70] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 84.6% | ESO: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 79.1% |
| Kajihara et al., 2016 [71] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 400 mg bid | 94.6% | RPZ: 10 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 86.7% |
| Sakurai et al., 2017 [72] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 87.9% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 66.9% |
| Sue et al., 2017 [73] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 84.9% | OMZ: 20 mg bid, LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 78.8% |
| Nishizawa et al., 2017 [74] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 62.3% | LPZ: 30 mg bid or RPZ: 10 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 47.1% |
| Tanabe et al., 2018 [75] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 91.5% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 79.4% |
| Study | VPZ-Based Regimen | PPI-Based Regimen | ||
|---|---|---|---|---|
| Regimen | Eradication Rate | Regimen | Eradication Rate | |
| RCT | ||||
| Murakami et al., 2016 [60] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 82.0% | LPZ: 30 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 40.0% |
| Non-RCT | ||||
| Noda et al., 2016 [67] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 400 mg bid | 87.5% | OMZ: 20 mg bid, LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 53.8% |
| Matsumoto et al., 2016 [68] | VPZ: 20 mg bid AMX: 750 mg bid CLR: 200 mg bid | 76.1% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid CLR: 200 or 400 mg bid | 40.2% |
| Study | VPZ-Based Regimen | PPI-Based Regimen | ||
|---|---|---|---|---|
| Regimen | Eradication Rate | Regimen | Eradication Rate | |
| Yamada et al., 2016 [69] | VPZ: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 89.6% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 89.9% |
| Tsujimae et al., 2016 [70] | VPZ: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 89.1% | ESO: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 83.3% |
| Sakurai et al., 2017 [72] | VPZ: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 96.1% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 89.7% |
| Sue et al., 2017 [73] | VPZ: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 80.5% | LPZ: 30 mg bid, RPZ: 10 mg bid or ESO: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 81.5% |
| Nishizawa et al., 2017 [77] | VPZ: 20 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 71.8% | LPZ: 30 mg bid or RPZ: 10 mg bid AMX: 750 mg bid MNZ: 250 mg bid | 73.7% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miftahussurur, M.; Pratama Putra, B.; Yamaoka, Y. The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy. Pharmaceuticals 2020, 13, 276. https://doi.org/10.3390/ph13100276
Miftahussurur M, Pratama Putra B, Yamaoka Y. The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy. Pharmaceuticals. 2020; 13(10):276. https://doi.org/10.3390/ph13100276
Chicago/Turabian StyleMiftahussurur, Muhammad, Boby Pratama Putra, and Yoshio Yamaoka. 2020. "The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy" Pharmaceuticals 13, no. 10: 276. https://doi.org/10.3390/ph13100276
APA StyleMiftahussurur, M., Pratama Putra, B., & Yamaoka, Y. (2020). The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy. Pharmaceuticals, 13(10), 276. https://doi.org/10.3390/ph13100276