Did the Introduction of Biosimilars Influence Their Prices and Utilization? The Case of Biologic Disease Modifying Antirheumatic Drugs (bDMARD) in Bulgaria



Abstract
:1. Introduction
2. Results
2.1. Availability of Biosimilars in the Reimbursement Drug List
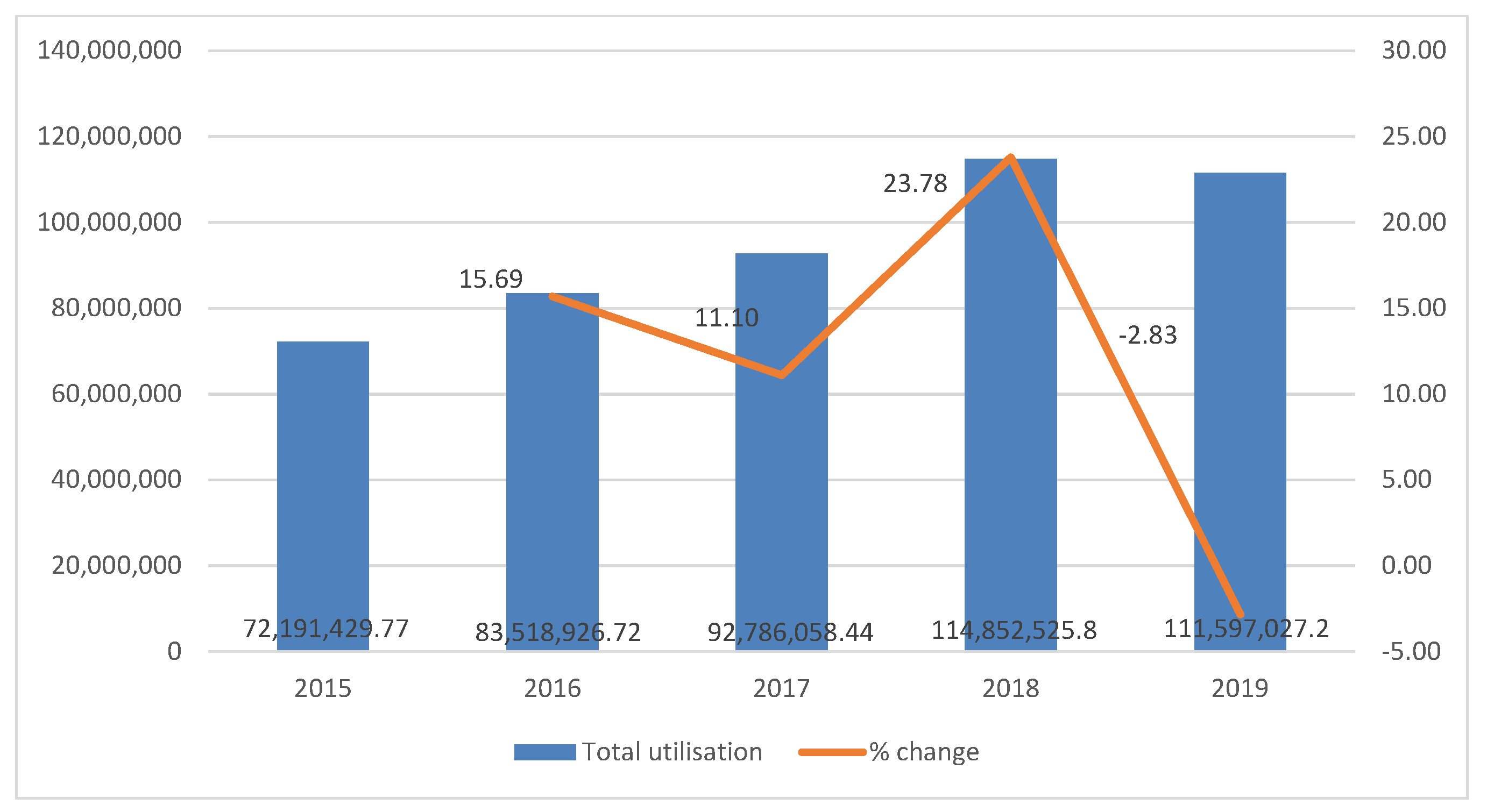
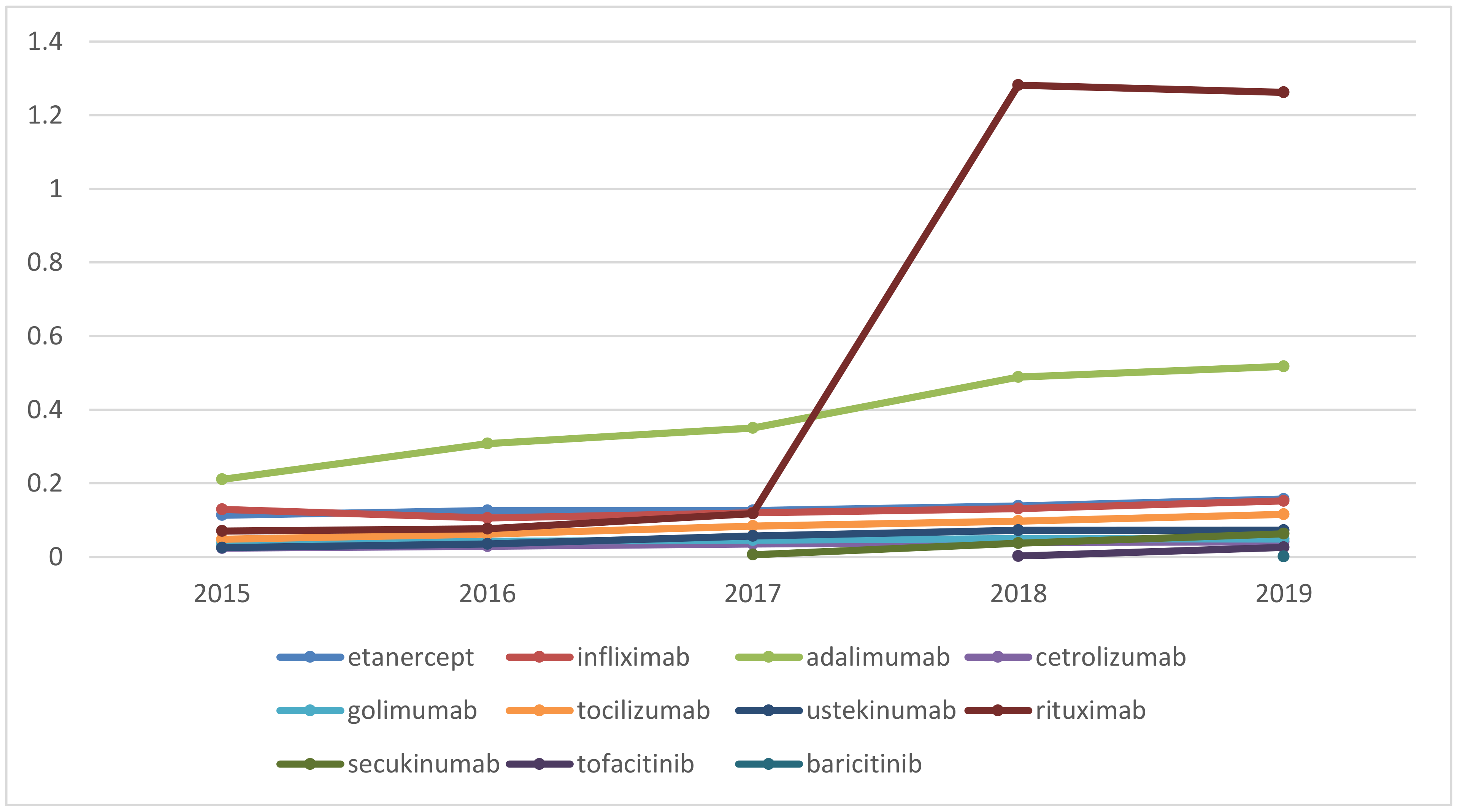
2.2. Changes in Prices and Utilization of Anti-Inflammatory Joint Diseases Medicines
3. Discussion
4. Materials and Methods
4.1. Qualitative Analysis
4.2. Quantitative Analysis
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaplan, W.A.; Ritz, L.S.; Vitello, M.; Wirtz, V.J. Policies to promote use of generic medicines in low and middle income countries: A review of published literature, 2000–2010. Health Policy 2012, 106, 211–224. [Google Scholar] [CrossRef]
- Dylst, P.; Simoens, S. Does the Market Share of Generic Medicines Influence the Price Level? PharmacoEconomics 2011, 29, 875–882. [Google Scholar] [CrossRef]
- King, D.; Kanavos, P. Encouraging the use of generic medicines: Implications for transition economies. Croat. Med. J. 2002, 43, 462–469. [Google Scholar] [PubMed]
- Gama, H.; Torre, C.; Guerreiro, J.P.; Azevedo, A.; Costa, S.; Lunet, N. Use of generic and essential medicines for prevention and treatment of cardiovascular diseases in Portugal. BMC Health Serv. Res. 2017, 17, 449. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use. OJ L 2001, 311, 67–128. Available online: http://data.europa.eu/eli/dir/2001/83/oj (accessed on 12 January 2021).
- Dylst, P.; Vulto, A.G.; Godman, B.; Simoens, S. Generic Medicines: Solutions for a Sustainable Drug Market? Appl. Health Econ. Health Policy 2013, 11, 437–443. [Google Scholar] [CrossRef]
- Spinks, J.; Chen, G.; Donovan, L. Does generic entry lower the prices paid for pharmaceuticals in Australia? A comparison before and after the introduction of the mandatory price-reduction policy. Aust. Health Rev. 2013, 37, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Elek, P.; Harsányi, A.; Zelei, T.; Csetneki, K.; Kaló, Z. Policy objective of generic medicines from the investment perspective: The case of clopidogrel. Health Policy 2017, 121, 558–565. [Google Scholar] [CrossRef] [Green Version]
- Dylst, P.; Vulto, A.; Simoens, S. Societal value of generic medicines beyond cost-saving through reduced prices. Expert Rev. Pharm. Outcomes Res. 2015, 15, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Salmane-Kulikovska, I.; Poplavska, E.; Ceha, M.; Mezinska, S. Use of generic medicines in Latvia: Awareness, opinions and experiences of the population. J. Pharm. Policy Pract. 2019, 12, 1. [Google Scholar] [CrossRef]
- Steele, J.W. Generic Competition in Canada. Pharmacoeconomics 1994, 6, 480–482. [Google Scholar] [CrossRef]
- WHO. Guideline for National Drug Policies; World Health Organization: Geneva, Switzerland, 1988. [Google Scholar]
- Rietveld, A.H.; Haaijer-Ruskamp, F.M. Policy options for cost-containment of pharmaceuticals. Int. J. Risk Saf. Med. 2002, 15, 29–54. [Google Scholar]
- WHO. The Selection of Essential Drugs; World Health Organization: Geneva, Switzerland, 1977. [Google Scholar]
- Kemp, A.; Roughead, E.E.; Kim, D.-S.; Ong, B. Pricing policies for generic medicines in Australia, New Zealand, the Republic of Korea and Singapore: Patent expiry and influence on atorvastatin price. WHO South-East Asia J. Public Health 2018, 7, 99–106. [Google Scholar] [CrossRef]
- Miguel, P.Z. Legal and policy foundations for global generic competition: Promoting affordable drug pricing in developing societies. Glob. Public Health 2015, 10, 1–16. [Google Scholar] [CrossRef]
- Mossialos, E.; Mrazek, M.; Walley, T. Regulating Pharmaceuticals in Europe: Striving for Efficiency, Equity and Quality; Open University Press: Berkshire, UK, 2004. [Google Scholar]
- European Medicines Agency. Biosimilar Medicines. Retrieved 17 June 2015. Available online: http://www.ema.europa.eu/ema/index.jsp?curl=pages/special_topics/document_listing/document_listing_000318.jsp (accessed on 1 November 2020).
- Berkowitz, S.A.; Engen, J.R.; Mazzeo, J.R.; Jones, B.G. Analytical tools for characterizing biopharmaceuticals and the implications for biosimilars. Nat. Rev. Drug Discov. 2012, 11, 527–540. [Google Scholar] [CrossRef] [Green Version]
- Harvey, R.D. Science of Biosimilars. J. Oncol. Pract. 2017, 13, 17s–23s. [Google Scholar] [CrossRef]
- Li, E.; Ramanan, S.; Green, L. Pharmacist Substitution of Biological Products: Issues and Considerations. J. Manag. Care Spéc. Pharm. 2015, 21, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Nabhan, C.; Parsad, S.; Mato, A.R.; Feinberg, B.A. Biosimilars in Oncology in the United States. JAMA Oncol. 2018, 4, 241. [Google Scholar] [CrossRef]
- Troen, P.; Newton, M.; Patel, J.; Scott, K. The Impact of Biosimilar Competition in Europe; White paper; IQVIA: Durham, NC, USA, 2019. [Google Scholar]
- Moorkens, E.; Vulto, A.G.; Huys, I.; Dylst, P.; Godman, B.; Keuerleber, S.; Claus, B.; Dimitrova, M.; Petrova, G.; Sović-Brkičić, L.; et al. Policies for biosimilar uptake in Europe: An overview. PLoS ONE 2017, 12, e0190147. [Google Scholar] [CrossRef] [Green Version]
- Cazap, E.; Jacobs, I.; McBride, A.; Popovian, R.; Sikora, K. Global Acceptance of Biosimilars: Importance of Regulatory Consistency, Education, and Trust. Oncologist 2018, 23, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Manova, M.; Savova, A.; Vasileva, M.; Terezova, S.; Kamusheva, M.; Grekova, D.; Petkova, V.; Petrova, G. Comparative Price Analysis of Biological Products for Treatment of Rheumatoid Arthritis. Front. Pharmacol. 2018, 9, 1070. [Google Scholar] [CrossRef]
- Kamusheva, M.; Manova, M.; Savova, A.T.; Petrova, G.I.; Mitov, K.; Harsányi, A.; Kaló, Z.; Márky, K.; Kawalec, P.; Angelovska, B.; et al. Comparative Analysis of Legislative Requirements About Patients’ Access to Biotechnological Drugs for Rare Diseases in Central and Eastern European Countries. Front. Pharmacol. 2018, 9, 795. [Google Scholar] [CrossRef] [Green Version]
- Stiff, K.M.; Cline, A.; Feldman, S. Tracking the price of existing biologics when drugs enter the market. Expert Rev. Pharm. Outcomes Res. 2019, 19, 375–377. [Google Scholar] [CrossRef]
- Burmester, G.-R.; Gordon, K.B.; Rosenbaum, J.T.; Arikan, D.; Lau, W.L.; Li, P.; Faccin, F.; Panaccione, R. Long-Term Safety of Adalimumab in 29,967 Adult Patients from Global Clinical Trials Across Multiple Indications: An Updated Analysis. Adv. Ther. 2019, 37, 364–380. [Google Scholar] [CrossRef] [Green Version]
- Kawalec, P.; Stawowczyk, E.; Tesar, T.; Skoupa, J.; Turcu-Stiolica, A.; Dimitrova, M.; Petrova, G.I.; Rugaja, Z.; Männik, A.; Harsanyi, A.; et al. Pricing and Reimbursement of Biosimilars in Central and Eastern European Countries. Front. Pharmacol. 2017, 8, 288. [Google Scholar] [CrossRef] [Green Version]
- Rome, B.N.; Lee, C.C.; Kesselheim, A.S. Market Exclusivity Length for Drugs with New Generic or Biosimilar Competition, 2012–2018. Clin. Pharmacol. Ther. 2020. [Google Scholar] [CrossRef]
- Sator, P. Safety and tolerability of adalimumab for the treatment of psoriasis: A review summarizing 15 years of real-life experience. Ther. Adv. Chronic Dis. 2018, 9, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Atzinger, C.B.; Guo, J.J. Biologic Disease-Modifying Antirheumatic Drugs in a National, Privately Insured Population: Utilization, Expenditures, and Price Trends. Am. Health Drug Benefits 2017, 10, 27–36. [Google Scholar]
- Lee, H.-J.; Han, E.; Kim, H. Comparison of Utilization Trends between Biosimilars and Generics: Lessons from the Nationwide Claims Data in South Korea. Appl. Health Econ. Health Policy 2020, 18, 557–566. [Google Scholar] [CrossRef]
- Dutcher, S.K.; Fazio-Eynullayeva, E.; Eworuke, E.; Carruth, A.; Dee, E.C.; Blum, M.D.; Nguyen, M.D.; Toh, S.; Panozzo, C.A.; Lyons, J.G. Understanding utilization patterns of biologics and biosimilars in the United States to support postmarketing studies of safety and effectiveness. Pharmacoepidemiol. Drug Saf. 2020, 29, 786–795. [Google Scholar] [CrossRef]
- Dutta, B.; Huys, I.; Vulto, A.G.; Simoens, S. Identifying Key Benefits in European Off-Patent Biologics and Biosimilar Markets: It is Not Only about Price! BioDrugs 2020, 34, 159–170. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kwon, H.-Y.; Godman, B.; Moorkens, E.; Simoens, S.; Bae, S. Uptake of Biosimilar Infliximab in the UK, France, Japan, and Korea: Budget Savings or Market Expansion Across Countries? Front. Pharmacol. 2020, 11, 970. [Google Scholar] [CrossRef]
- O’Callaghan, J.; Barry, S.P.; Bermingham, M.; Morris, J.M.; Griffin, B.T. Regulation of biosimilar medicines and current perspectives on interchangeability and policy. Eur. J. Clin. Pharmacol. 2018, 75, 1–11. [Google Scholar] [CrossRef]
- Rémuzat, C.; Dorey, J.; Cristeau, O.; Ionescu, D.; Radière, G.; Toumi, M. Key drivers for market penetration of biosimilars in Europe. J. Mark. Access Health Policy 2017, 5, 1272308. [Google Scholar] [CrossRef] [Green Version]
- Ministry Council. Regulation on the Conditions, Rules and Order of Regulating and Registering of the Prices of Medicinal Product; State Gazette No 40/2013; Last amended: State Gazette 19/2020; Council of Ministers: Sofia, Bulgaria, 2020. [Google Scholar]
- EMA. Science, Medicines, Health. Biosimilar Medicines: Marketing Authorization. Available online: https://www.ema.europa.eu/en/human-regulatory/marketing-authorisation/biosimilar-medicines-marketing-authorisation (accessed on 12 January 2021).
- National Council of Prices and Reimbursement. Electronic Registries. Available online: http://portal.ncpr.bg/registers/pages/register/list-medicament.xhtml (accessed on 12 January 2021).
- WHO. Essential Medicines and Health Products. DDD Indicators. Available online: https://www.who.int/medicines/regulation/medicines-safety/toolkit_indicators/en/index1.html (accessed on 12 January 2021).



{kind=link}
{kind=link}
| INN | Authorized Biosimilars in Europe (n) | Biosimilars Available on the National Market (n) | Authorisation Date in Europe | Date of Inclusions into the Positive Drug List (PDL) | Time Lag |
|---|---|---|---|---|---|
| Outpatient Practice | |||||
| insulin glargine | 2 | 1 | 8/09/2014 | 24/08/2015 | 11 months |
| adalimumab | 8 | 1 | 20/03/2017 | 22/10/2018 | 1 year 5 months |
| 1 | 15/09/2018 | 22/03/2019 | 6 months | ||
| 1 | 25/07/2018 | 18/03/2019 | 6 months | ||
| 1 | 16/09/2018 | 20/02/2020 | 2 year 6 months | ||
| infliximab | 4 | 1 | 9/09/2013 | 27/11/2013 | 2 months |
| 1 | 8/09/2013 | 27/11/2013 | 2 months | ||
| 1 | 17/05/2018 | 28/03/2019 | 10 months | ||
| etanercept | 2 | 1 | 22/06/2017 | 19/06/2020 | 3 year |
| rituximab | 5 | 1 | 16/02/2017 | 30/03/2018 2/11/2020 (excluded) | 11 months 2 year |
| epoetin alfa | 3 | 1 | 26/08/2007 | 20.03.2013 2.10.2014 (excluded) | 4 year 6 months 1 year 7 months |
| 1 | 22/08/2007 | 26/09/2016 | 9 year | ||
| epoetin zeta | 3 | 1 | 17/12/2007 | 15/06/2012 | 4 year 5 months |
| teriparatide | 3 | 1 | 10/01/2017 | 8/11/2019 2/04/2020 (excluded) | 1.9 year 6 months |
| somatropin | 1 | 1 | 11/04/2006 | 3/12/2011 | 4 year 8 months |
| Inpatient Practice | |||||
| follitropin alfa | 2 | 1 | 25/03/2014 | 01/03/2015 | 1 year |
| filgrastim | 6 | 1 | 16/09/2014 | 01/02/2018 | 3 year 5 months |
| 1 | 6/06/2010 | 22/08/2011 8/09/2012 (excluded) | 1 year 2 months 1 year | ||
| 1 | 14/09/2008 | 21/08/2012 16/06/2014 (excluded) | 4 year 2 year | ||
| 1 | 5/02/2009 | 19/09/2011 | 2 year 7 months | ||
| pegfilgrastim | 6 | 1 | 25/04/2019 | 27/03/2020 | 11 months |
| 1 | 20/09/2018 | 01/03/2019 | 5 months | ||
| 1 | 21/11/2018 | 01/03/2019 | 4 months | ||
| trastuzumab | 5 | 1 | 7/02/2018 | 12/10/2018 2/11/2020 (excluded) | 8 months 2 year |
| 1 | 15/05/2018 | 2/02/2019 | 9 months | ||
| 1 | 11/12/2018 | 13/03/2019 | 3 months | ||
| 1 | 14/11/2017 | 21/02/2020 | 2 year 3 months | ||
| 1 | 25/07/2018 | 13/03/2019 | 6 months | ||
| bevacizumam | 2 | 1 | 14/01/2018 | 28/09/2020 | 1 year 9 months |
| INN | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | % Change (2020 to 2015) | Fisher Test |
|---|---|---|---|---|---|---|---|---|
| etanercept | 67.08 | 60.49 | 58.69 | 54.55 | 53.75 | 34.39 * | 48.72 | p < 0.0001 |
| infliximab | 30.61 *,* | 28.68 | 27.018 | 27.02 | 17.92 * | 17.92 | 41.47 | |
| adalimumab | 72.39 | 66.08 | 66.08 | 50.01* | 38.13 * | 38.13 *,* | 47.33 | |
| cetrolizumab | 63.67 | 57.29 | 57.29 | 53.10 | 53.11 | 50.03 | 21.43 | |
| golimumab | 65.56 | 65.24 | 62.05 | 57.50 | 57.50 | 53.34 | 18.63 | |
| ustekinumab | 73.70 | 73.24 | 65.53 | 60.65 | 60.65 | 60.65 | 17.71 | |
| tocilizumab | 71.21 | 70.91 | 60.58 | 60.58 | 59.22 | 54.69 | 23.19 | |
| rituximab | 4.97 | 4.97 | 4.94 | 3.65 * | 3.13 | 3.39 ↓ | 31.66 | |
| secukinumab | 81.04 | 80.88 | 73.08 | 72,58 | 10.44 | |||
| tofacitinib | 55.51 | 52.94 | 52.94 | 4.63 | ||||
| baricitinib | 77.16 | 77.16 | 0% |
| INN | 2015 | 2016 | 2017 | 2018 | 2019 | % Change (2019 to 2015) | Fisher Test |
|---|---|---|---|---|---|---|---|
| Etanercept | 15.87 | 15.78 | 15.27 | 15.47 | 17.19 | 7.69 | p < 0.0001 |
| Infliximab | 8.25 | 6.30 | 6.65 | 7.24 | 5.54 | −48.77 | |
| Adalimumab | 31.86 | 42.24 | 47.70 | 49.99 | 40.08 | 20.51 | |
| Cetrolizumab | 3.19 | 3.45 | 4.17 | 4.32 | 4.43 | 27.98 | |
| Golimumab | 4.98 | 5.71 | 5.82 | 5.85 | 5.71 | 12.89 | |
| Tocilizumab | 7.15 | 9.06 | 10.46 | 12.00 | 13.91 | 48.58 | |
| Rituximab | 0.89 | 0.97 | 1.49 | 11.96 | 10.06 | 91.12 | |
| Secukinimab | 1.23 | 7.72 | 11.74 | 89.56 | |||
| Tofacitinib | 0.28 | 2.80 | 89.87 | ||||
| Baricitinib | 0.12 | 0 |
| 2015 | % of Overall Utilization | 2016 | % of Overall Utilization | 2017 | % of Overall Utilization | 2018 | % of Overall Utilization | 2019 | % of Overall Utilization | |
|---|---|---|---|---|---|---|---|---|---|---|
| etanercept | 0.1133 | 17.25 | 0.1258 | 16.04 | 0.1263 | 13.41 | 0.1387 | 5.93 | 0.1575 | 6.41 |
| infliximab | 0.129 | 19.63 | 0.1059 | 13.50 | 0.1197 | 12.71 | 0.1312 | 5.61 | 0.1524 | 6.20 |
| adalimmab | 0.2107 | 32.07 | 0.3082 | 39.29 | 0.3506 | 37.22 | 0.489 | 20.91 | 0.5178 | 21.07 |
| cetrolizumab | 0.0239 | 3.64 | 0.0291 | 3.71 | 0.0353 | 3.75 | 0.0398 | 1.70 | 0.041 | 1.67 |
| golimumab | 0.0363 | 5.53 | 0.0423 | 5.39 | 0.0456 | 4.84 | 0.0497 | 2.13 | 0.0489 | 1.99 |
| tocilizumab | 0.0481 | 7.32 | 0.0616 | 7.85 | 0.0839 | 8.91 | 0.0969 | 4.14 | 0.1157 | 4.71 |
| rituximab | 0.0254 | 36.13 | 0.0352 | 4.49 | 0.0567 | 6.02 | 0.072 | 3.08 | 0.0726 | 2.95 |
| secukinumab | 0.0703 | 10.70 | 0.0764 | 9.74 | 0.1179 | 12.52 | 1.2817 | 54.80 | 1.2619 | 51.35 |
| ustekinumab | 0.0059 | 0.63 | 0.0374 | 1.60 | 0.0629 | 2.56 | ||||
| tofacitinib | 0.0024 | 0.10 | 0.026 | 1.06 | ||||||
| baricitinib | 0.0007 | 0.03 | ||||||||
| total utilization | 0.66 | 132.26 | 0.78 | 100.00 | 0.94 | 100.00 | 2.34 | 100.00 | 2.46 | 100.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tachkov, K.; Mitkova, Z.; Boyadzieva, V.; Petrova, G. Did the Introduction of Biosimilars Influence Their Prices and Utilization? The Case of Biologic Disease Modifying Antirheumatic Drugs (bDMARD) in Bulgaria. Pharmaceuticals 2021, 14, 64. https://doi.org/10.3390/ph14010064
Tachkov K, Mitkova Z, Boyadzieva V, Petrova G. Did the Introduction of Biosimilars Influence Their Prices and Utilization? The Case of Biologic Disease Modifying Antirheumatic Drugs (bDMARD) in Bulgaria. Pharmaceuticals. 2021; 14(1):64. https://doi.org/10.3390/ph14010064
Chicago/Turabian StyleTachkov, Konstantin, Zornitsa Mitkova, Vladimira Boyadzieva, and Guenka Petrova. 2021. "Did the Introduction of Biosimilars Influence Their Prices and Utilization? The Case of Biologic Disease Modifying Antirheumatic Drugs (bDMARD) in Bulgaria" Pharmaceuticals 14, no. 1: 64. https://doi.org/10.3390/ph14010064
APA StyleTachkov, K., Mitkova, Z., Boyadzieva, V., & Petrova, G. (2021). Did the Introduction of Biosimilars Influence Their Prices and Utilization? The Case of Biologic Disease Modifying Antirheumatic Drugs (bDMARD) in Bulgaria. Pharmaceuticals, 14(1), 64. https://doi.org/10.3390/ph14010064