
Combinatorial Regimen of Carbamazepine and Imipramine Exhibits Synergism against Grandmal Epilepsy in Rats: Inhibition of Pro-Inflammatory Cytokines and PI3K/Akt/mTOR Signaling Pathway

 ,
,  , and
, and
Abstract
:1. Introduction
2. Results
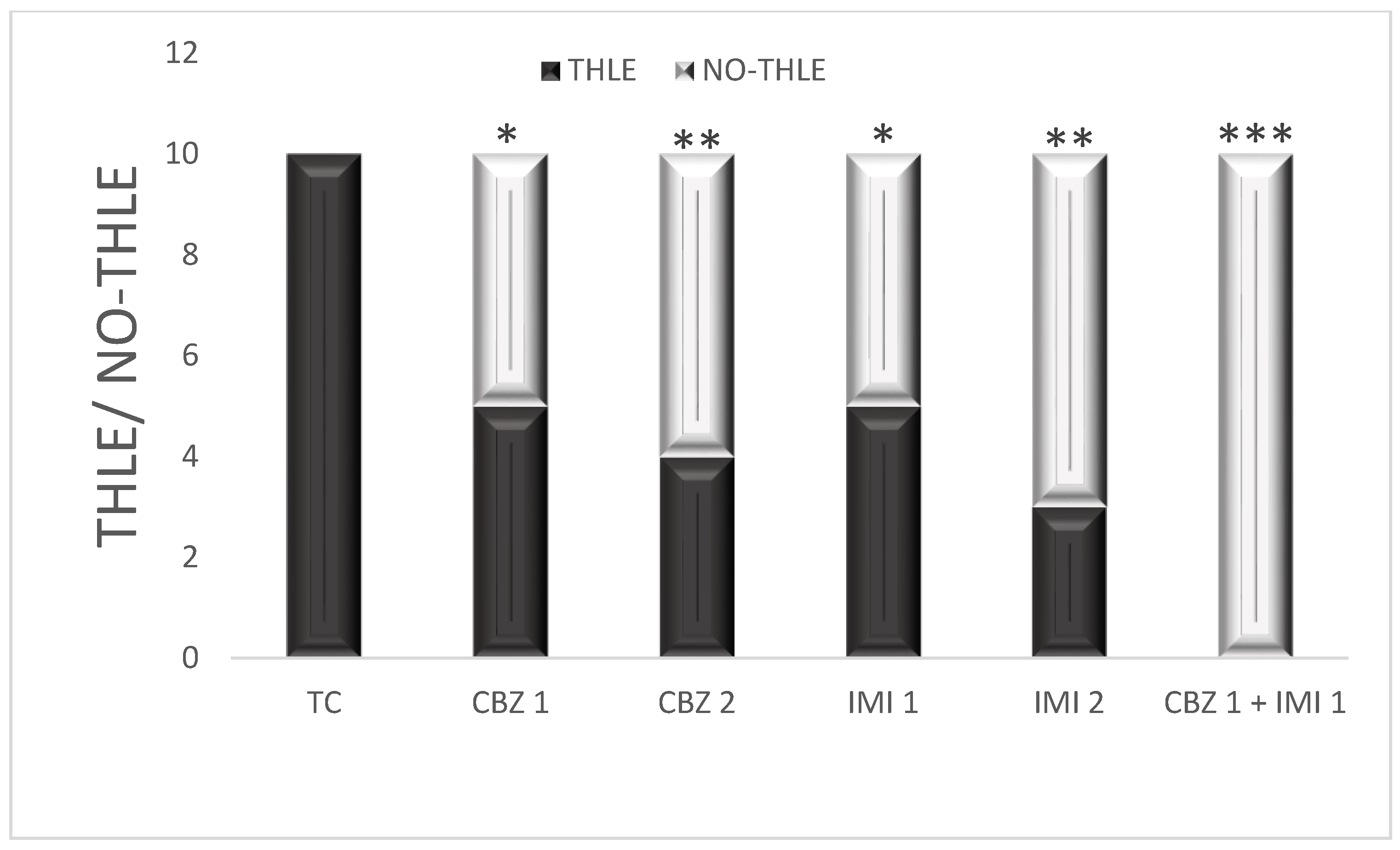
2.1. Effects of Carbamazepine, Imipramine and Their Low Dose Combination on MES Induced Tonic Hind Limb Extension (THLE)
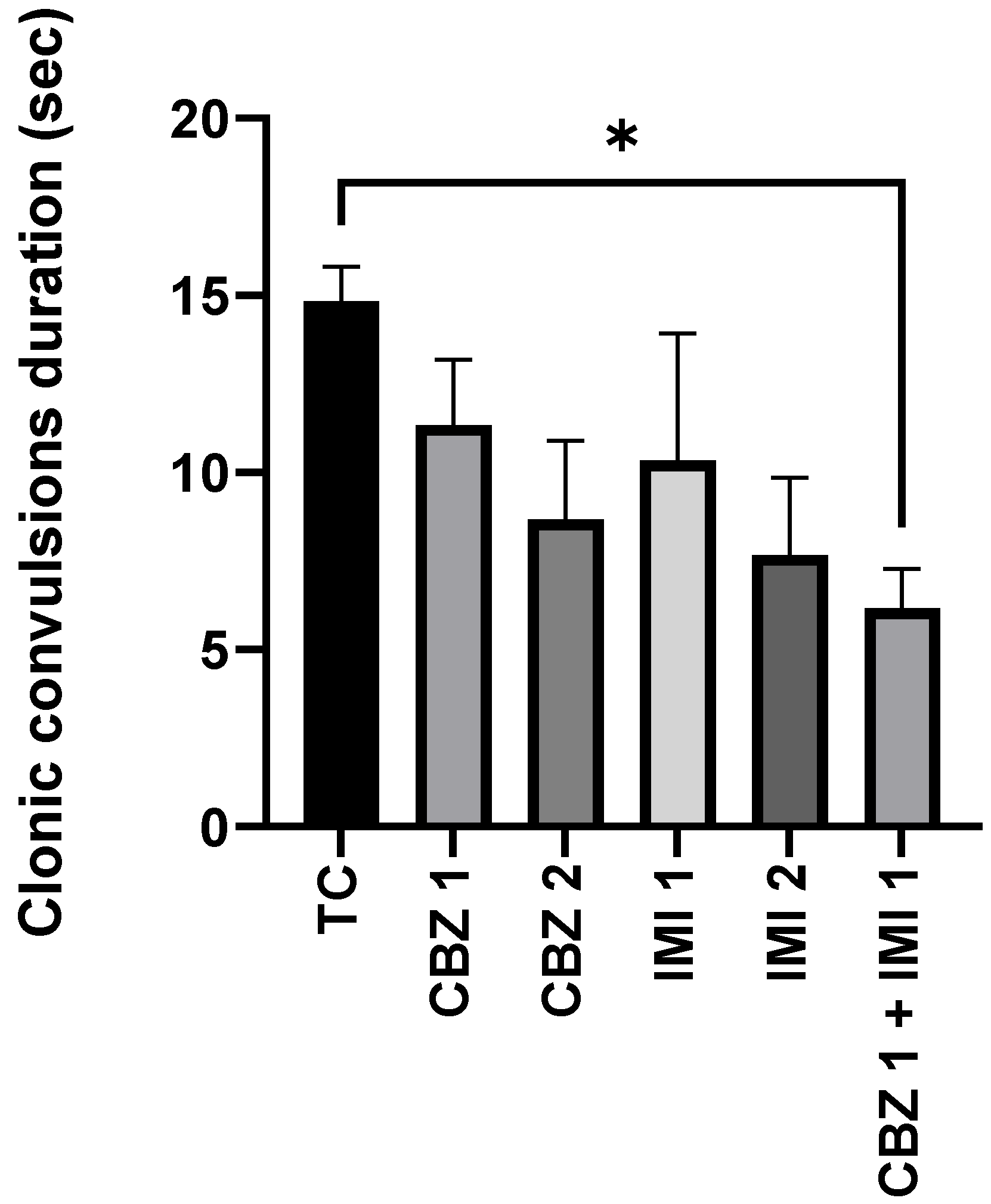
2.2. Effects of Carbamazepine, Imipramine and Their Low Dose Combination on the Duration of Clonic Convulsions
2.3. Effects of Carbamazepine, Imipramine and Their Low Dose Combination on Pro-Inflammatory Makers
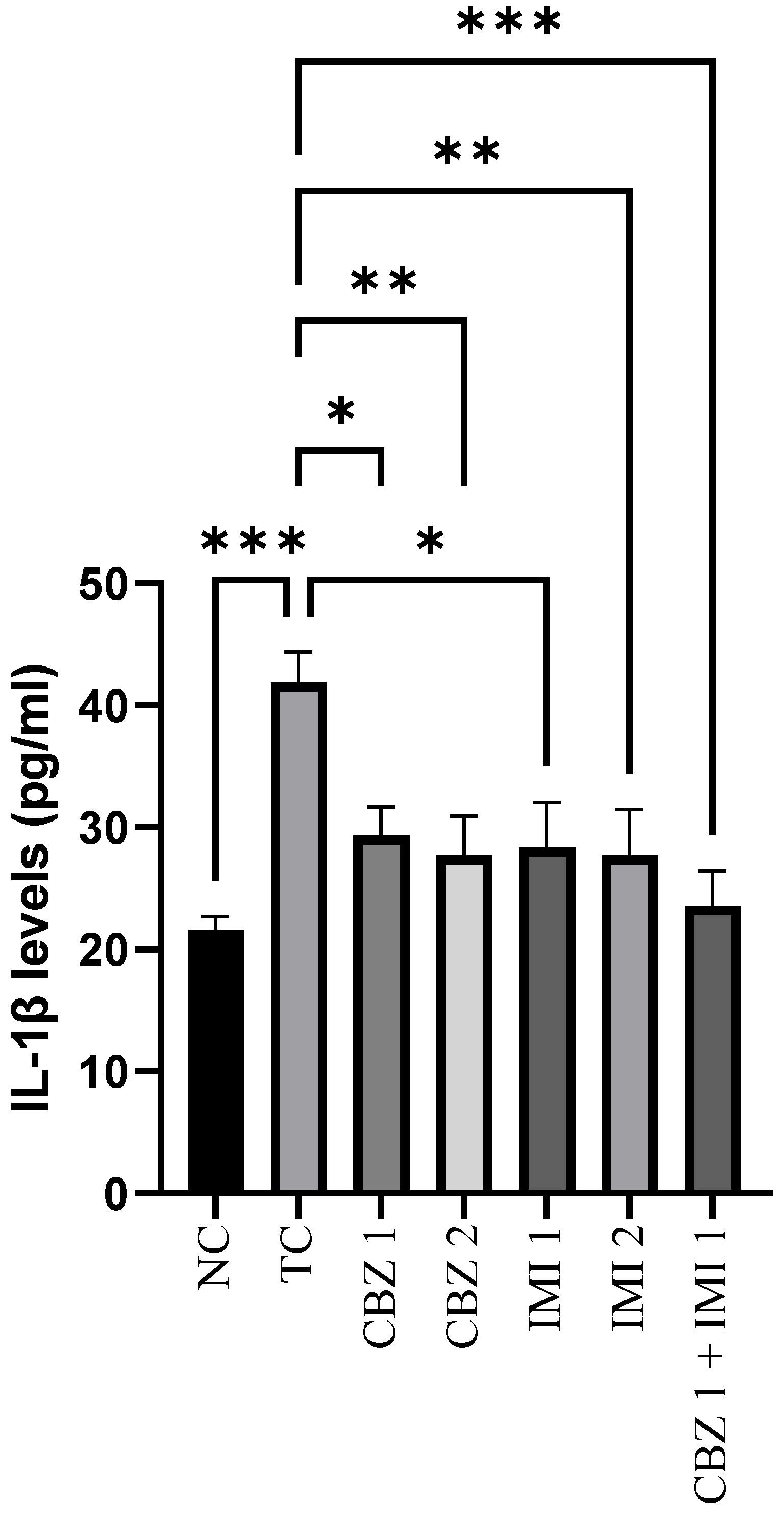
2.3.1. Effect on Hippocampal IL-1β Levels
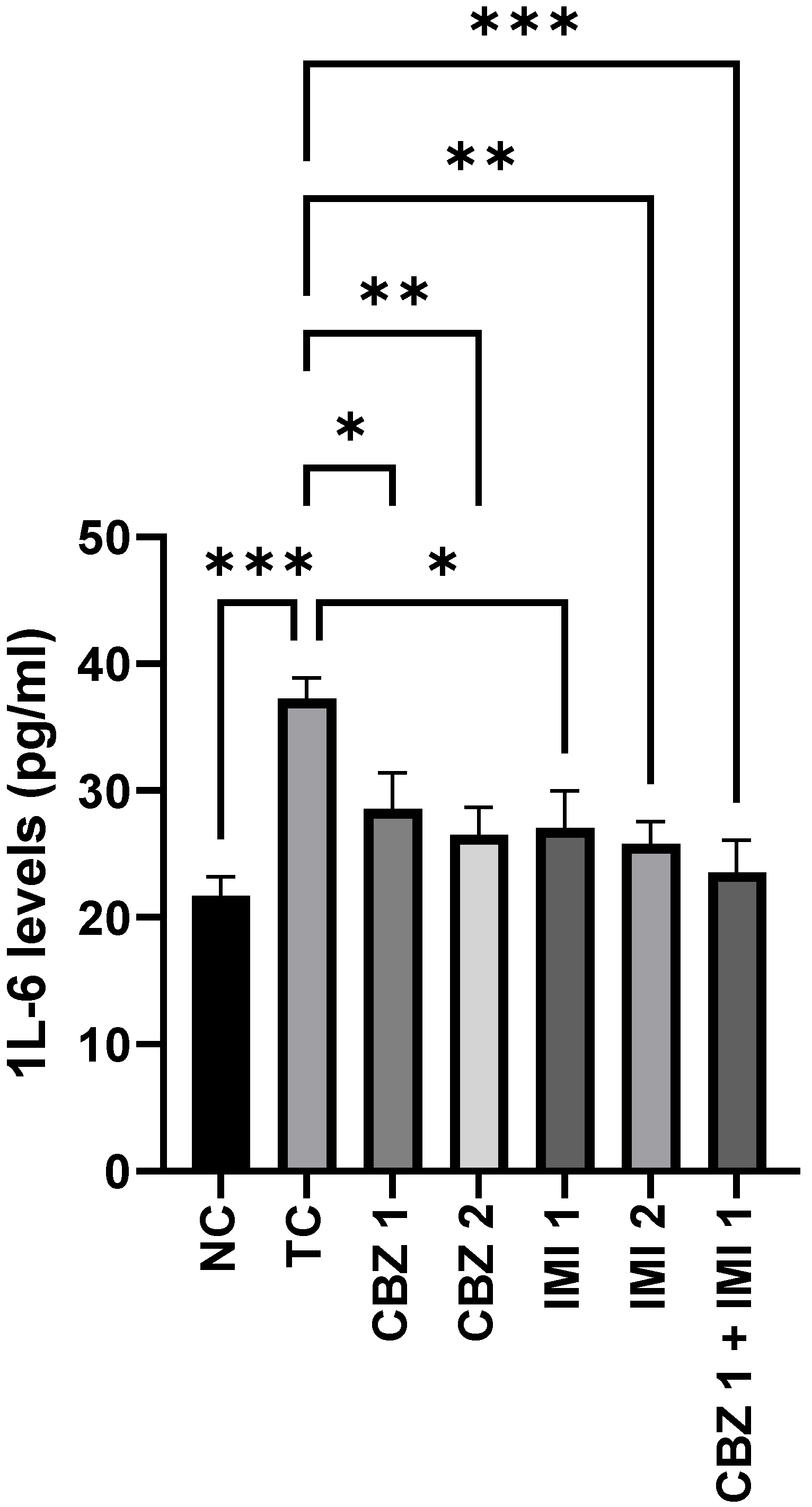
2.3.2. Effect on Hippocampal IL-6 Levels
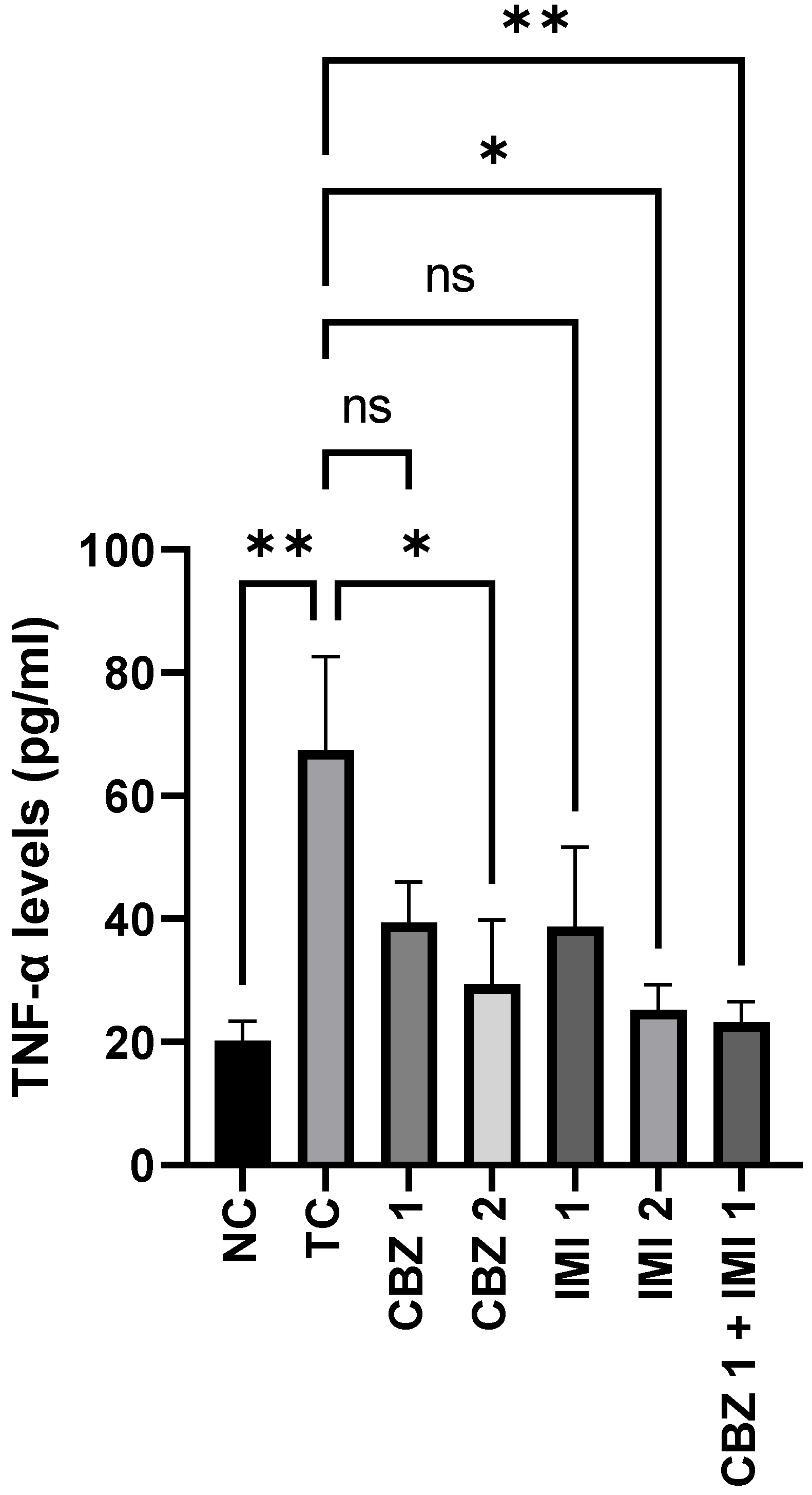
2.3.3. Effect on Hippocampal TNF-α Levels
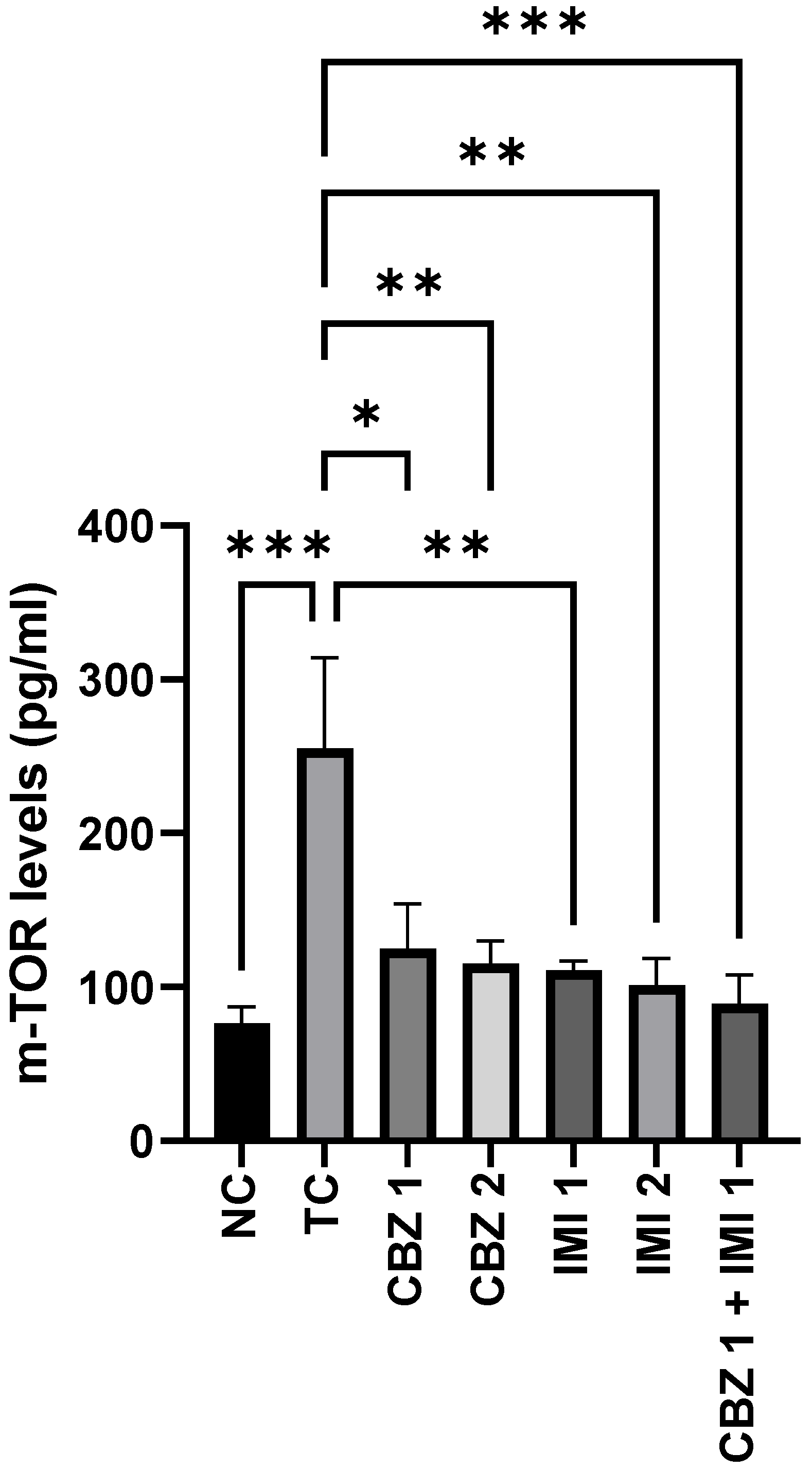
2.4. Effects of Carbamazepine, Imipramine and Their Low Dose Combination on the Hippocampal mTOR Levels
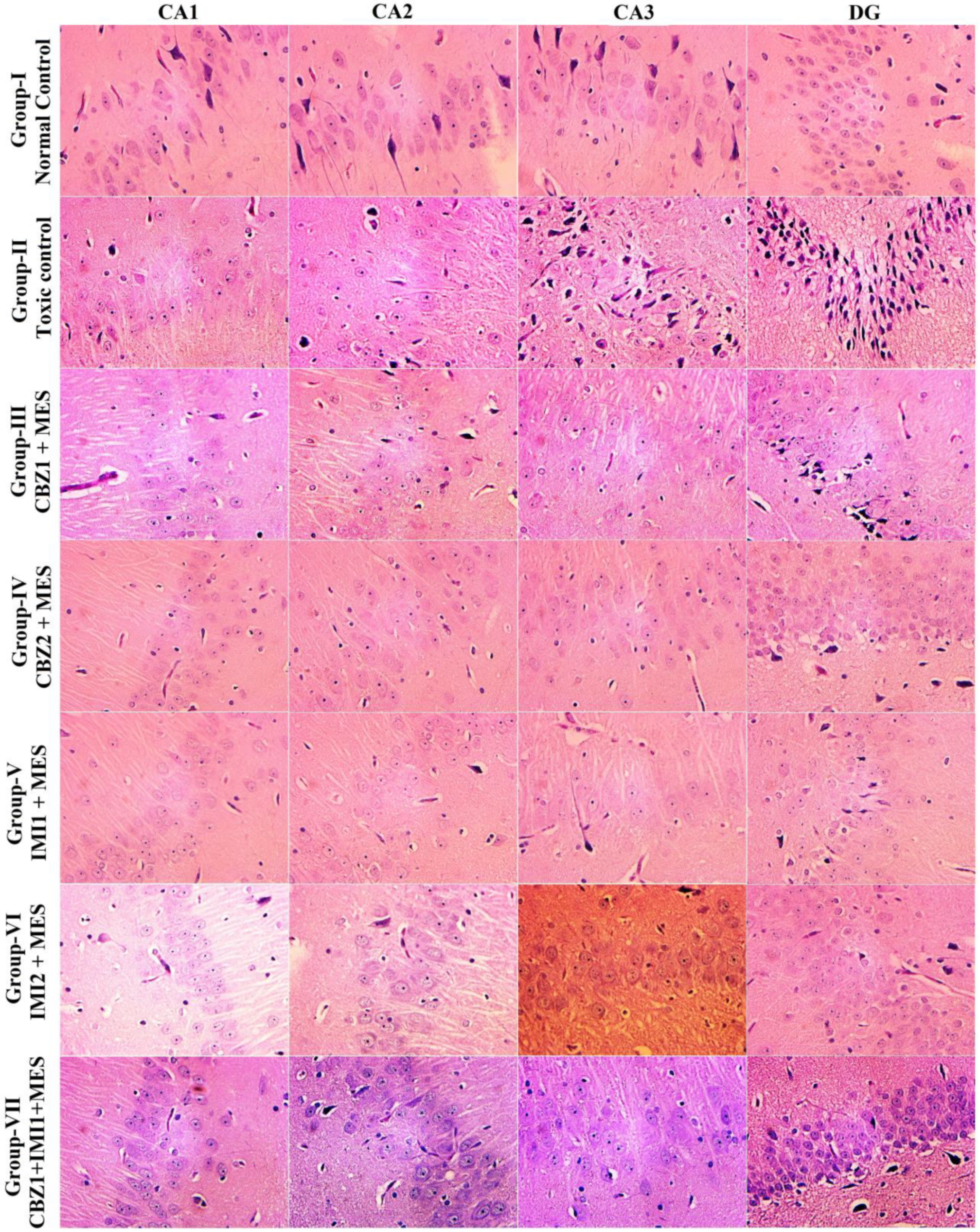
2.5. Effect of Carbamazepine (CBZ), Imipramine (IMI) and Their Low Dose Combination on the Hippocampal Neuronal Damage
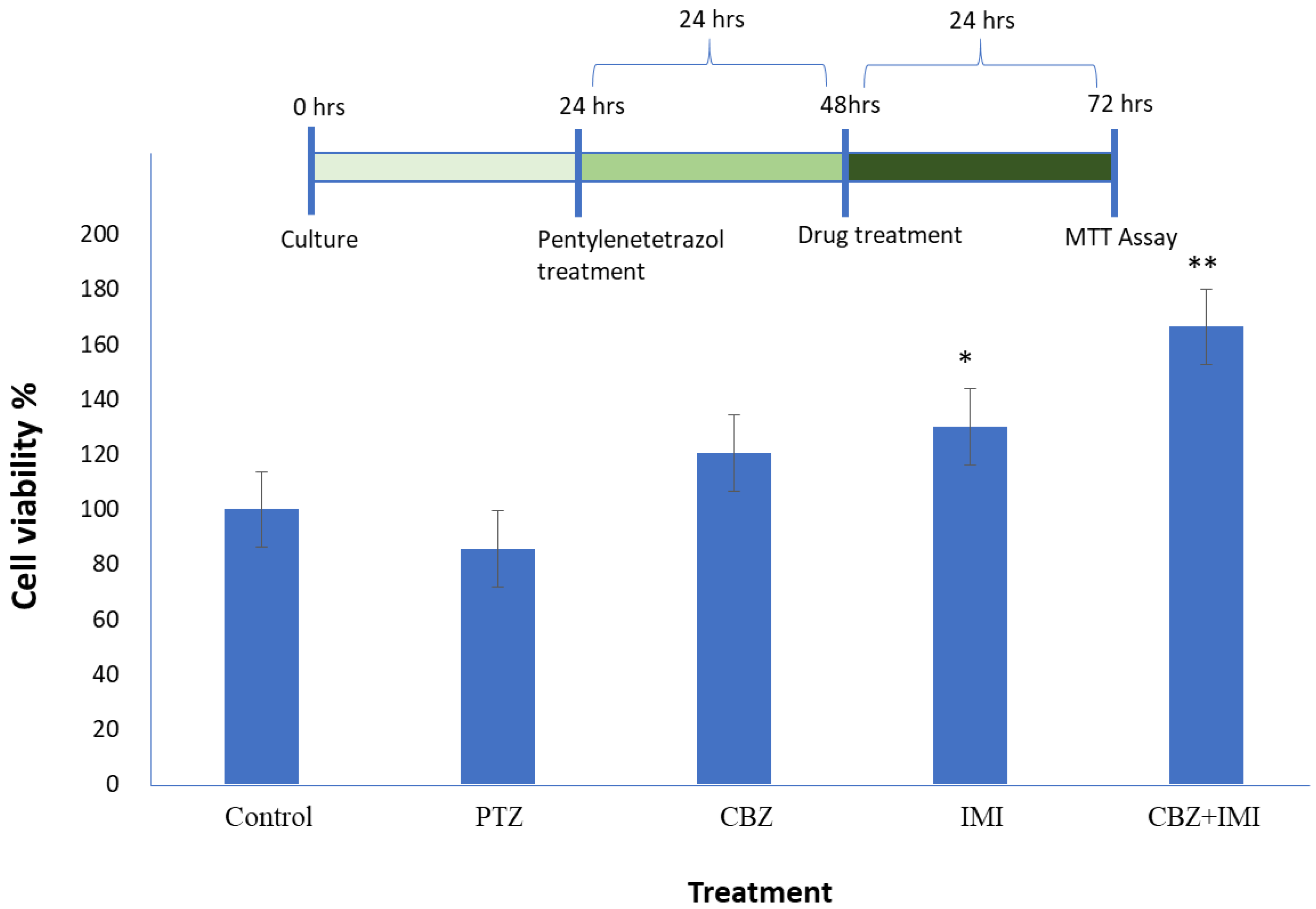
2.6. Cell Viability Assay
2.7. Molecular Docking
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Drugs and Dosing Schedule
4.3. Experimental Groups
4.4. MES induced THLE
4.5. Experimental Design
4.6. MES Induced Neuronal Damage
4.7. Assessment of Hippocampal mTOR Levels
4.8. Assessment of Inflammatory Markers in the Hippocampus
4.9. Invitro Studies
4.9.1. Cell Culture
4.9.2. Invitro Model of Cellular Degeneration
4.9.3. Treatment with Test Drugs
4.9.4. MTT Assay
4.10. Molecular Docking
4.11. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fisher, R.S.; van Emde Boas, W.; Blume, W.; Elger, C.; Genton, P.; Lee, P.; Engel, J. Epileptic Seizures and Epilepsy: Definitions Proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia 2005, 46, 470–472. [Google Scholar] [CrossRef]
- Pottoo, F.H.; Tabassum, N.; Javed, M.N.; Nigar, S.; Rasheed, R.; Khan, A.; Barkat, M.A.; Alam, M.S.; Maqbool, A.; Ansari, M.A.; et al. The Synergistic Effect of Raloxifene, Fluoxetine, and Bromocriptine Protects Against Pilocarpine-Induced Status Epilepticus and Temporal Lobe Epilepsy. Mol. Neurobiol. 2018, 56, 1233–1247. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.A.; Pottoo, F.H.; Akbar, M. Gene Therapy Repairs for the Epileptic Brain: Potential for Treatment and Future Directions. Curr. Gene Ther. 2020, 19, 367–375. [Google Scholar] [CrossRef]
- Singh, A.; Trevick, S. The Epidemiology of Global Epilepsy. Neurol. Clin. 2016, 34, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Alaqeel, A.; Sabbagh, A.J. Epilepsy; What Do Saudi’s Living in Riyadh Know? Seizure 2013, 22, 205–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beghi, E. The Epidemiology of Epilepsy. Neuroepidemiology 2020, 54, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Pottoo, F.H.; Tabassum, N.; Javed, M.N.; Nigar, S.; Sharma, S.; Barkat, M.A.; Harshita, N.; Alam, M.S.; Ansari, M.A.; Barreto, G.E.; et al. Raloxifene Potentiates the Effect of Fluoxetine against Maximal Electroshock Induced Seizures in Mice. Eur. J. Pharm. Sci. 2020, 146, 105261. [Google Scholar] [CrossRef]
- Thom, M. Review: Hippocampal Sclerosis in Epilepsy: A Neuropathology Review. Neuropathol. Appl. Neurobiol. 2014, 40, 520–543. [Google Scholar] [CrossRef]
- Waldbaum, S.; Patel, M. Mitochondrial Dysfunction and Oxidative Stress: A Contributing Link to Acquired Epilepsy? J. Bioenerg. Biomembr. 2010, 42, 449–455. [Google Scholar] [CrossRef] [Green Version]
- Do Val-da Silva, R.A.; Peixoto-Santos, J.E.; Kandratavicius, L.; De Ross, J.B.; Esteves, I.; De Martinis, B.S.; Alves, M.N.R.; Scandiuzzi, R.C.; Hallak, J.E.C.; Zuardi, A.W.; et al. Protective Effects of Cannabidiol against Seizures and Neuronal Death in a Rat Model of Mesial Temporal Lobe Epilepsy. Front. Pharm. 2017, 8, 131. [Google Scholar] [CrossRef] [Green Version]
- Pottoo, F.H.; Alshayban, D.M.; Joseph, R.; Al-Musa, F.; Al-Jabran, O.; Aljaafari, D. Impact of Adherence to Antiepileptic Medications on Quality of Life of Epileptic Patients in the Eastern Province of Saudi Arabia: A Cross-Sectional Study. Imam J. Appl. Sci. 2020, 5, 1. [Google Scholar] [CrossRef]
- Beydoun, A.; DuPont, S.; Zhou, D.; Matta, M.; Nagire, V.; Lagae, L. Current Role of Carbamazepine and Oxcarbazepine in the Management of Epilepsy. Seizure 2020, 83, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Dalby, M.A. Antiepileptic and Psychotropic Effect of Carbamazepine (Tegretol®) in the Treatment of Psychomotor Epilepsy. Epilepsia 1971, 12, 325–334. [Google Scholar] [CrossRef]
- Dean, L. Carbamazepine Therapy and HLA Genotype. In Medical Genetics Summaries; Pratt, V., McLeod, H., Rubinstein, W., Dean, L., Kattman, B., Malheiro, A., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Colombi, I.; Mahajani, S.; Frega, M.; Gasparini, L.; Chiappalone, M. Effects of Antiepileptic Drugs on Hippocampal Neurons Coupled to Micro-Electrode Arrays. Front. Neuroeng. 2013, 6, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollister, L.E. Tricyclic Antidepressants. N. Engl. J. Med. 1978, 299, 1106–1109. [Google Scholar] [PubMed]
- D’Aquila, P.S.; Galistu, A. Further Characterization of the Effect of the Prototypical Antidepressant Imipramine on the Microstructure of Licking for Sucrose. PLoS ONE 2021, 16, e0245559. [Google Scholar] [CrossRef] [PubMed]
- Heninger, G.R.; Delgado, P.L.; Charney, D.S. The Revised Monoamine Theory of Depression: A Modulatory Role for Monoamines, Based on New Findings from Monoamine Depletion Experiments in Humans. Pharmacopsychiatry 1996, 29, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Shelton, R.C. Cellular Mechanisms in the Vulnerability to Depression and Response to Antidepressants. Psychiatr. Clin. N. Am. 2000, 23, 713–729. [Google Scholar] [CrossRef]
- Fitzgerald, P.J. Is Elevated Norepinephrine an Etiological Factor in Some Cases of Epilepsy? Seizure 2010, 19, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Rudge, D.G.; Koos, J.D.; Vaidialingam, B.; Yang, H.J.; Pavletich, N.P. mTOR Kinase Structure, Mechanism and Regulation. Nature 2013, 497, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Saxton, R.A.; Sabatini, D.M. MTOR Signaling in Growth, Metabolism, and Disease. Cell 2017, 168, 960–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Réus, G.Z.; Quevedo, J.; Rodrigues, A.L.S. MTOR Signaling in the Neuropathophysiology of Depression: Current Evidence. J. Recept. Ligand Channel Res. 2015, 8, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Hodges, S.L.; Lugo, J.N. Therapeutic Role of Targeting MTOR Signaling and Neuroinflammation in Epilepsy. Epilepsy Res. 2020, 161, 106282. [Google Scholar] [CrossRef] [PubMed]
- Crino, P.B. mTOR Signaling in Epilepsy: Insights from Malformations of Cortical Development. Cold Spring Harb. Perspect. Med. 2015, 5, a022442. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.H.; Bordey, A. Convergent and Divergent Mechanisms of Epileptogenesis in MTORopathies. Front. Neuroanat. 2021, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Baune, B.T.; Konrad, C.; Grotegerd, D.; Suslow, T.; Birosova, E.; Ohrmann, P.; Bauer, J.; Arolt, V.; Heindel, W.; Domschke, K.; et al. Interleukin-6 Gene (IL-6): A Possible Role in Brain Morphology in the Healthy Adult Brain. J. Neuroinflamm. 2012, 9, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobylarek, D.; Iwanowski, P.; Lewandowska, Z.; Limphaibool, N.; Szafranek, S.; Labrzycka, A.; Kozubski, W. Advances in the Potential Biomarkers of Epilepsy. Front. Neurol. 2019, 10, 685. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, N.; Kobayashi, Y.; Fujii, Y.; Kobayashi, M. Increased Interleukin-6 and High-Sensitivity C-Reactive Protein Levels in Pediatric Epilepsy Patients with Frequent, Refractory Generalized Motor Seizures. Seizure Eur. J. Epilepsy 2015, 25, 136–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uludag, I.F.; Duksal, T.; Tiftikcioglu, B.I.; Zorlu, Y.; Ozkaya, F.; Kirkali, G. IL-1β, IL-6 and IL1Ra Levels in Temporal Lobe Epilepsy. Seizure 2015, 26, 22–25. [Google Scholar] [CrossRef] [Green Version]
- Ravizza, T.; Vezzani, A. Pharmacological Targeting of Brain Inflammation in Epilepsy: Therapeutic Perspectives from Experimental and Clinical Studies. Epilepsia Open 2018, 3, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, M. Neuroprotection in Epilepsy. Epilepsia 2007, 48, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Huff, J.S.; Murr, N. Seizure; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Löscher, W.; Potschka, H.; Sisodiya, S.M.; Vezzani, A. Drug Resistance in Epilepsy: Clinical Impact, Potential Mechanisms, and New Innovative Treatment Options. Pharm. Rev. 2020, 72, 606–638. [Google Scholar] [CrossRef] [PubMed]
- Verrotti, A.; Tambucci, R.; Francesco, L.; Pavone, P.; Iapadre, G.; Altobelli, E.; Matricardi, S.; Farello, G.; Belcastro, V. The Role of Polytherapy in the Management of Epilepsy: Suggestions for Rational Antiepileptic Drug Selection. Expert Rev. Neurother. 2019, 20, 167–173. [Google Scholar] [CrossRef]
- Brodie, M.J.; Sills, G.J. Combining Antiepileptic Drugs—Rational Polytherapy? Seizure 2011, 20, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, F.; Hartz, A.M.S.; Bauer, B. Drug-Resistant Epilepsy: Multiple Hypotheses, Few Answers. Front. Neurol. 2017, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Benardo, L.S. Altered Sodium Channels Underlie Anticonvulsant Drug Insensitivity. Epilepsy Curr. 2003, 3, 227–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grabenstatter, H.L.; Clark, S.; Dudek, F.E. Anticonvulsant Effects of Carbamazepine on Spontaneous Seizures in Rats with Kainate-Induced Epilepsy: Comparison of Intraperitoneal Injections with Drug-in-Food Protocols. Epilepsia 2007, 48, 2287–2295. [Google Scholar] [CrossRef]
- Hawkins, C.A.; Mellanby, J.; Brown, J. Antiepileptic and Antiamnesic Effect of Carbamazepine in Experimental Limbic Epilepsy. J. Neurol. Neurosurg. Psychiatry 1985, 48, 459–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osuntokun, O.S.; Abdulwahab, U.F.; Akanji, N.O.; Adedokun, K.I.; Adekomi, A.D.; Olayiwola, G. Anticonvulsant and Neuroprotective Effects of Carbamazepine-Levetiracetam Adjunctive Treatment in Convulsive Status Epilepticus Rat Model: Inhibition of Cholinergic Transmission. Neurosci. Lett. 2021, 762, 136167. [Google Scholar] [CrossRef]
- Maan, J.S.; Duong, T.v.H.; Saadabadi, A. Carbamazepine; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Turner, A.L.; Perry, M.S. Outside the Box: Medications Worth Considering When Traditional Antiepileptic Drugs Have Failed. Seizure 2017, 50, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Fayez, R.; Gupta, V. Imipramine; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Lange, S.C.; Julien, R.M.; Fowler, G.W. Biphasic Effects of Imipramine in Experimental Models of Epilepsy. Epilepsia 1976, 17, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Guan, K.L. Expanding mTOR Signaling. Cell Res. 2007, 17, 666–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Na, L.; Li, Y.; Chen, L. Roles of the PI3K/AKT/MTOR Signalling Pathways in Neurodegenerative Diseases and Tumours. Cell Biosci. 2020, 10, 54. [Google Scholar] [CrossRef] [Green Version]
- Duan, W.; Chen, Y.; Wang, X.R. MicroRNA-155 Contributes to the Occurrence of Epilepsy through the PI3K/Akt/MTOR Signaling Pathway. Int. J. Mol. Med. 2018, 42, 1577–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.H.; Hsiao, C.J.; Lin, Y.N.; Wu, J.W.; Kuo, Y.C.; Lee, C.K.; Hsiao, G. Carbamazepine Attenuates Inducible Nitric Oxide Synthase Expression through Akt Inhibition in Activated Microglial Cells. Pharm. Biol. 2014, 52, 1451–1459. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Lee, J.G.; Seo, M.K.; Lee, C.H.; Cho, H.Y.; Lee, B.J.; Seol, W.; Kim, Y.H. Differential Effects of Antidepressant Drugs on MTOR Signalling in Rat Hippocampal Neurons. Int. J. Neuropsychopharmacol. 2014, 17, 1831–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, S.-H.; Kim, S.H.; Kim, Y.; Kim, Y.S.; Lim, Y.; Lee, Y.H.; Shin, S.Y. The Tricyclic Antidepressant Imipramine Induces Autophagic Cell Death in U-87MG Glioma Cells. Biochem. Biophys. Res. Commun. 2011, 413, 311–317. [Google Scholar] [CrossRef]
- Kim, K.; Kwak, B.O.; Kwon, A.; Ha, J.; Kim, S.-J.; Bae, S.W.; Son, J.S.; Kim, S.-N.; Lee, R. Analysis of Plasma Multiplex Cytokines and Increased Level of IL-10 and IL-1Ra Cytokines in Febrile Seizures. J. Neuroinflamm. 2017, 14, 200. [Google Scholar] [CrossRef]
- Gómez, C.D.; Buijs, R.M.; Sitges, M. The Anti-Seizure Drugs Vinpocetine and Carbamazepine, but Not Valproic Acid, Reduce Inflammatory IL-1β and TNF-α Expression in Rat Hippocampus. J. Neurochem. 2014, 130, 770–779. [Google Scholar] [CrossRef]
- Obuchowicz, E.; Bielecka, A.M.; Paul-Samojedny, M.; Pudełko, A.; Kowalski, J. Imipramine and Fluoxetine Inhibit LPS-Induced Activation and Affect Morphology of Microglial Cells in the Rat Glial Culture. Pharmacol. Rep. 2014, 66, 34–43. [Google Scholar] [CrossRef]
- Ramirez, K.; Sheridan, J.F. Antidepressant Imipramine Diminishes Stress-Induced Inflammation in the Periphery and Central Nervous System and Related Anxiety- and Depressive- like Behaviors. Brain Behav. Immun. 2016, 57, 293–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alboni, S.; Benatti, C.; Montanari, C.; Tascedda, F.; Brunello, N. Chronic Antidepressant Treatments Resulted in Altered Expression of Genes Involved in Inflammation in the Rat Hypothalamus. Eur. J. Pharmacol. 2013, 721, 158–167. [Google Scholar] [CrossRef]
- Casillas-Espinosa, P.M.; Ali, I.; O’Brien, T.J. Neurodegenerative Pathways as Targets for Acquired Epilepsy Therapy Development. Epilepsia Open 2020, 5, 138–154. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.; Martella, G.; Picconi, B.; Prosperetti, C.; Pisani, A.; di Filippo, M.; Pisani, F.; Bernardi, G.; Calabresi, P. Multiple Mechanisms Underlying the Neuroprotective Effects of Antiepileptic Drugs Against In Vitro Ischemia. Stroke 2006, 37, 1319–1326. [Google Scholar] [CrossRef]
- Ahn, J.H.; Shin, B.N.; Park, J.H.; Lee, T.-K.; Park, Y.E.; Lee, J.-C.; Yang, G.E.; Shin, M.C.; Cho, J.H.; Lee, K.C.; et al. Pre- and Post-Treatment with Novel Antiepileptic Drug Oxcarbazepine Exerts Neuroprotective Effect in the Hippocampus in a Gerbil Model of Transient Global Cerebral Ischemia. Brain Sci. 2019, 9, 279. [Google Scholar] [CrossRef] [Green Version]
- Xiang, C.; Li, Z.-N.; Huang, T.-Z.; Li, J.-H.; Yang, L.; Wei, J.-K. Threshold for Maximal Electroshock Seizures (MEST) at Three Developmental Stages in Young Mice. Zool. Res. 2019, 40, 231–235. [Google Scholar] [CrossRef]
- Pottoo, F.H.; Salahuddin, M.; Khan, F.A.; Alomar, F.; AL Dhamen, M.A.; Alhashim, A.F.; Alqattan, H.H.; Gomaa, M.S.; Alomary, M.N. Thymoquinone Potentiates the Effect of Phenytoin against Electroshock-Induced Convulsions in Rats by Reducing the Hyperactivation of m-TOR Pathway and Neuroinflammation: Evidence from In Vivo, In Vitro and Computational Studies. Pharmaceuticals 2021, 14, 1132. [Google Scholar] [CrossRef]
- Faingold, C.; Blumenfeld, H. (Eds.) Neuronal Networks in Brain Function, CNS Disorders, and Therapeutics; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Zhang, B.; Wong, M. Pentylenetetrazole-Induced Seizures Cause Acute, but Not Chronic, MTOR Pathway Activation in Rat. Epilepsia 2012, 53, 506–511. [Google Scholar] [CrossRef] [Green Version]
- Rehman, S.; Asiri, S.M.; Khan, F.A.; Jermy, R.; Khan, H.; Akhtar, S.; Al Jindan, R.; Khan, K.M.; Qurashi, A. Biocompatible Tin Oxide Nanoparticles: Synthesis, Antibacterial, Anticandidal and Cytotoxic Activities. ChemistrySelect 2019, 4, 4013–4017. [Google Scholar] [CrossRef]
- Khan, F.A.; Akhtar, S.; Almohazey, D.; Alomari, M.; Almofty, S.A. Extracts of Clove (Syzygium Aromaticum) Potentiate FMSP-Nanoparticles Induced Cell Death in MCF-7 Cells. Int. J. Biomater. 2018, 2018, 8479439. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, L.G.; Dos Santos, R.N.; Oliva, G.; Andricopulo, A.D. Molecular Docking and Structure-Based Drug Design Strategies. Molecules 2015, 20, 13384–13421. [Google Scholar] [CrossRef] [PubMed]
- Stefan, M.I.; Le Novere, N. Cooperative Binding. PLoS Comput. Biol. 2013, 9, e1003106. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Akt | Docking Score | |||
| Carbamazepine 1st | Carbamazepine/Imipramine | Imipramine 1st | Imipramine/Carbamzepine | |
| −7.8 | −12.5 | −8.4 | −8.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pottoo, F.H.; Salahuddin, M.; Khan, F.A.; AL Dhamen, M.A.; Alsaeed, W.J.; Gomaa, M.S.; Vatte, C.; Alomary, M.N. Combinatorial Regimen of Carbamazepine and Imipramine Exhibits Synergism against Grandmal Epilepsy in Rats: Inhibition of Pro-Inflammatory Cytokines and PI3K/Akt/mTOR Signaling Pathway. Pharmaceuticals 2021, 14, 1204. https://doi.org/10.3390/ph14111204
Pottoo FH, Salahuddin M, Khan FA, AL Dhamen MA, Alsaeed WJ, Gomaa MS, Vatte C, Alomary MN. Combinatorial Regimen of Carbamazepine and Imipramine Exhibits Synergism against Grandmal Epilepsy in Rats: Inhibition of Pro-Inflammatory Cytokines and PI3K/Akt/mTOR Signaling Pathway. Pharmaceuticals. 2021; 14(11):1204. https://doi.org/10.3390/ph14111204
Chicago/Turabian StylePottoo, Faheem Hyder, Mohammed Salahuddin, Firdos Alam Khan, Marwa Abdullah AL Dhamen, Walaa Jafar Alsaeed, Mohamed S. Gomaa, Chittibabu Vatte, and Mohammad N. Alomary. 2021. "Combinatorial Regimen of Carbamazepine and Imipramine Exhibits Synergism against Grandmal Epilepsy in Rats: Inhibition of Pro-Inflammatory Cytokines and PI3K/Akt/mTOR Signaling Pathway" Pharmaceuticals 14, no. 11: 1204. https://doi.org/10.3390/ph14111204
APA StylePottoo, F. H., Salahuddin, M., Khan, F. A., AL Dhamen, M. A., Alsaeed, W. J., Gomaa, M. S., Vatte, C., & Alomary, M. N. (2021). Combinatorial Regimen of Carbamazepine and Imipramine Exhibits Synergism against Grandmal Epilepsy in Rats: Inhibition of Pro-Inflammatory Cytokines and PI3K/Akt/mTOR Signaling Pathway. Pharmaceuticals, 14(11), 1204. https://doi.org/10.3390/ph14111204