
Current Status of Baricitinib as a Repurposed Therapy for COVID-19

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Literature Search Strategy
3. Pre-clinical Studies
3.1. In-Silico Studies
3.2. Role of Bioinformatics in Unveiling New Opportunities for Drug Repurposing
3.3. Application of Bioinformatics on Baricitinib-Treated Models and COVID-19 Host-Related Factors
3.3.1. Expression of Cytokines
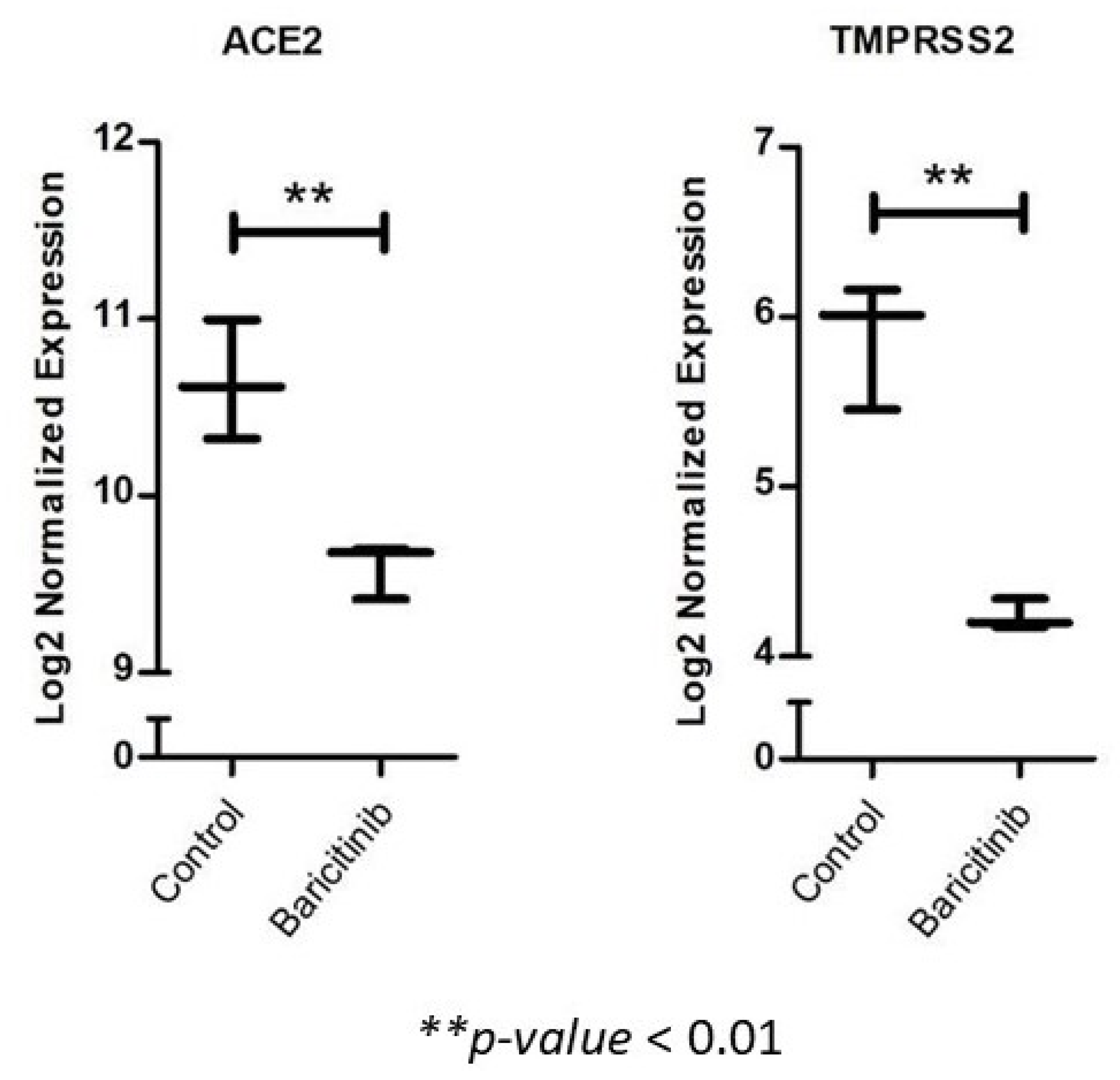
3.3.2. Expression of Viral Entry Receptors
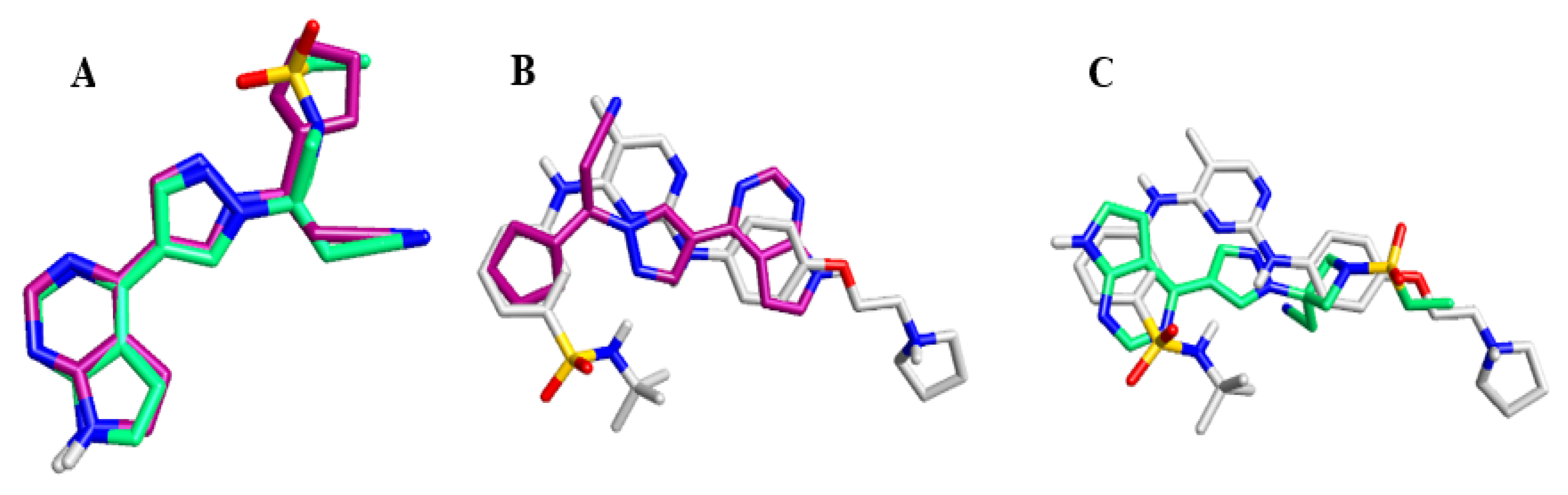
3.3.3. Structural Activity Relationship of JAK Inhibitors
3.4. In-Vitro Studies on Baricitinib in COVID-19 Models
3.5. In-Vivo Studies
4. Repurposed Immunomodulators in Treatment of COVID-19
5. Pharmacology of Baricitinib
6. Baricitinib for COVID-19 Treatment
7. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saber-Ayad, M.; Saleh, M.A.; Abu-Gharbieh, E. The Rationale for Potential Pharmacotherapy of COVID-19. Pharmaceuticals 2020, 13, 96. [Google Scholar] [CrossRef]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef]
- Henstock, P.V. Artificial Intelligence for Pharma: Time for Internal Investment. Trends Pharmacol. Sci. 2019, 40, 543–546. [Google Scholar] [CrossRef]
- Braciale, T.J.; Hahn, Y.S. Immunity to viruses. Immunol. Rev. 2013, 255, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nile, S.H.; Nile, A.; Qiu, J.; Li, L.; Jia, X.; Kai, G. COVID-19: Pathogenesis, cytokine storm and therapeutic potential of interferons. Cytokine Growth Factor Rev. 2020, 53, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef] [Green Version]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2021, 26, 80–93. [Google Scholar] [CrossRef]
- Brown, N.; Fiscato, M.; Segler, M.H.S.; Vaucher, A.C. GuacaMol: Benchmarking Models for de Novo Molecular Design. J. Chem. Inf. Modeling 2019, 59, 1096–1108. [Google Scholar] [CrossRef]
- Aliper, A.; Plis, S.; Artemov, A.; Ulloa, A.; Mamoshina, P.; Zhavoronkov, A. Deep Learning Applications for Predicting Pharmacological Properties of Drugs and Drug Repurposing Using Transcriptomic Data. Mol. Pharm. 2016, 13, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Li, H.; Li, S.; Leung, K.S. Improving prediction of phenotypic drug response on cancer cell lines using deep convolutional network. BMC Bioinform. 2019. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.G.; Liu, S.; Miller, I.J.; Coon, J.J.; Gitter, A. Learning Drug Functions from Chemical Structures with Convolutional Neural Networks and Random Forests. J. Chem. Inf. Modeling 2019, 59, 4438–4449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, K.Y.; Fokoue, A.; Luo, H.; Iyengar, A.; Dey, S.; Zhang, P. Interpretable drug target prediction using deep neural representation. In Proceedings of the IJCAI International Joint Conference on Artificial Intelligence, Stockholm, Sweden, 13 July 2018. [Google Scholar]
- Beck, B.R.; Shin, B.; Choi, Y.; Park, S.; Kang, K. Predicting commercially available antiviral drugs that may act on the novel coronavirus (SARS-CoV-2) through a drug-target interaction deep learning model. Comput. Struct. Biotechnol. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gysi, D.M.; Do Valle, Í.; Zitnik, M.; Ameli, A.; Gan, X.; Varol, O.; Sanchez, H.; Baron, R.M.; Ghiassian, D.; Loscalzo, J.; et al. Network Medicine Framework for Identifying Drug Repurposing Opportunities for COVID-19. arXiv 2020, arXiv:2004.07229. [Google Scholar]
- Rosenblatt, F. The perceptron: A probabilistic model for information storage and organization in the brain. Psychol. Rev. 1958, 65, 386–408. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Zhou, B.; Pache, L.; Chang, M.; Khodabakhshi, A.H.; Tanaseichuk, O.; Benner, C.; Chanda, S.K. Metascape provides a biologist-oriented resource for the analysis of systems-level datasets. Nat. Commun. 2019, 10, 1523. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Brosius, F.C., 3rd; Adler, S.G.; Kretzler, M.; Mehta, R.L.; Tumlin, J.A.; Tanaka, Y.; Haneda, M.; Liu, J.; Silk, M.E.; et al. JAK1/JAK2 inhibition by baricitinib in diabetic kidney disease: Results from a Phase 2 randomized controlled clinical trial. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. —Eur. Ren. Assoc. 2018, 33, 1950–1959. [Google Scholar] [CrossRef] [Green Version]
- Fetter, T.; Smith, P.; Guel, T.; Braegelmann, C.; Bieber, T.; Wenzel, J. Selective Janus Kinase 1 Inhibition Is a Promising Therapeutic Approach for Lupus Erythematosus Skin Lesions. Front. Immunol. 2020, 11, 344. [Google Scholar] [CrossRef] [Green Version]
- Kubo, S.; Nakayamada, S.; Sakata, K.; Kitanaga, Y.; Ma, X.; Lee, S.; Ishii, A.; Yamagata, K.; Nakano, K.; Tanaka, Y. Janus Kinase Inhibitor Baricitinib Modulates Human Innate and Adaptive Immune System. Front. Immunol. 2018, 9. [Google Scholar] [CrossRef]
- Kremer, J.; Huizinga, T.; Chen, L.; Saifan, C.; Issa, M.; Witt, S.; Walls, C.; de la Torre, I. FRI0090 Analysis of neutrophils, lymphocytes, and platelets in pooled phase 2 and phase 3 studies of baricitinib for rheumatoid arthritis. In Proceedings of the Poster Presentations; BMJ Publishing Group Ltd; European League Against Rheumatism: London, UK; Zürich, Switzerland, 2017; p. 512. [Google Scholar]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1620. [Google Scholar] [CrossRef] [Green Version]
- Owczarek, K.; Szczepanski, A.; Milewska, A.; Baster, Z.; Rajfur, Z.; Sarna, M.; Pyrc, K. Early events during human coronavirus OC43 entry to the cell. Sci. Rep. 2018, 8, 7124. [Google Scholar] [CrossRef] [PubMed]
- Iwata, S.; Tanaka, Y. Progress in understanding the safety and efficacy of Janus kinase inhibitors for treatment of rheumatoid arthritis. Expert Rev. Clin. Immunol. 2016, 12, 1047–1057. [Google Scholar] [CrossRef]
- Wu, P.; Nielsen, T.E.; Clausen, M.H. FDA-approved small-molecule kinase inhibitors. Trends Pharmacol. Sci. 2015, 36, 422–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesa, R.; Vannucchi, A.M.; Yacoub, A.; Zachee, P.; Garg, M.; Lyons, R.; Koschmieder, S.; Rinaldi, C.; Byrne, J.; Hasan, Y.; et al. The efficacy and safety of continued hydroxycarbamide therapy versus switching to ruxolitinib in patients with polycythaemia vera: A randomized, double-blind, double-dummy, symptom study (RELIEF). Br. J. Haematol. 2017, 176, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Leroy, E.; Constantinescu, S.N. Rethinking JAK2 inhibition: Towards novel strategies of more specific and versatile Janus kinase inhibition. Leukemia 2017, 31, 1023–1038. [Google Scholar] [CrossRef] [PubMed]
- Daina, A.; Michielin, O.; Zoete, V. SwissADME: A free web tool to evaluate pharmacokinetics, drug-likeness and medicinal chemistry friendliness of small molecules. Sci. Rep. 2017, 7, 42717. [Google Scholar] [CrossRef] [Green Version]
- Simeon, S.; Jongkon, N. Construction of Quantitative Structure Activity Relationship (QSAR) Models to Predict Potency of Structurally Diversed Janus Kinase 2 Inhibitors. Molecules 2019, 24, 4393. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. FDA Approved Drug Products: Barictinib; Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207924s000lbl.pdf (accessed on 15 May 2021).
- Food and Drug Administration. FDA Approved Drug Products: JAKAFI (Ruxolitinib) Tablets, for Oral Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202192lbl.pdf (accessed on 15 May 2021).
- Zhang, M.; Xu, C.R.; Shamiyeh, E.; Liu, F.; Yin, J.Y.; von Moltke, L.L.; Smith, W.B. A randomized, placebo-controlled study of the pharmacokinetics, pharmacodynamics, and tolerability of the oral JAK2 inhibitor fedratinib (SAR302503) in healthy volunteers. J. Clin. Pharmacol. 2014, 54, 415–421. [Google Scholar] [CrossRef]
- Ertl, P.; Rohde, B.; Selzer, P. Fast Calculation of Molecular Polar Surface Area as a Sum of Fragment-Based Contributions and Its Application to the Prediction of Drug Transport Properties. J. Med. Chem. 2000, 43, 3714–3717. [Google Scholar] [CrossRef]
- Moriguchi, I.; Hirono, S.; Nakagome, I.; Hirano, H. Comparison of Reliability of log P Values for Drugs Calculated by Several Methods. Chem. Pharm. Bull. 1994, 42, 976–978. [Google Scholar] [CrossRef] [Green Version]
- Cleves, A.E.; Johnson, S.R.; Jain, A.N. Electrostatic-field and surface-shape similarity for virtual screening and pose prediction. J. Comput. Aided Mol. Des. 2019, 33, 865–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stebbing, J.; Krishnan, V.; Bono, S.; Ottaviani, S.; Casalini, G.; Richardson, P.J.; Monteil, V.; Lauschke, V.M.; Mirazimi, A.; Youhanna, S.; et al. Mechanism of baricitinib supports artificial intelligence-predicted testing in COVID -19 patients. EMBO Mol. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Petrone, L.; Petruccioli, E.; Alonzi, T.; Vanini, V.; Cuzzi, G.; Najafi Fard, S.; Castilletti, C.; Palmieri, F.; Gualano, G.; Vittozzi, P.; et al. In-vitro evaluation of the immunomodulatory effects of Baricitinib: Implication for COVID-19 therapy. J. Infect. 2021, 82, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Sánchez Nievas, G.; Falcone, M.; Youhanna, S.; Richardson, P.; Ottaviani, S.; Shen, J.X.; Sommerauer, C.; Tiseo, G.; Ghiadoni, L.; et al. JAK inhibition reduces SARS-CoV-2 liver infectivity and modulates inflammatory responses to reduce morbidity and mortality. Sci. Adv. 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Hoang, T.N.; Pino, M.; Boddapati, A.K.; Viox, E.G.; Starke, C.E.; Upadhyay, A.A.; Gumber, S.; Nekorchuk, M.; Busman-Sahay, K.; Strongin, Z.; et al. Baricitinib treatment resolves lower-airway macrophage inflammation and neutrophil recruitment in SARS-CoV-2-infected rhesus macaques. Cell 2021, 184, 460–475.e21. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Behrens, E.M.; Kreiger, P.A.; Cherian, S.; Cron, R.Q. Interleukin 1 receptor antagonist to treat cytophagic histiocytic panniculitis with secondary hemophagocytic lymphohistiocytosis. J. Rheumatol. 2006, 33, 2081–2084. [Google Scholar] [PubMed]
- Chen, H.; Wang, F.; Zhang, P.; Zhang, Y.; Chen, Y.; Fan, X.; Cao, X.; Liu, J.; Yang, Y.; Wang, B.; et al. Management of cytokine release syndrome related to CAR-T cell therapy. Front. Med. 2019, 13, 610–617. [Google Scholar] [CrossRef]
- Al-Salama, Z.T.; Scott, L.J. Baricitinib: A Review in Rheumatoid Arthritis. Drugs 2018, 78, 761–772. [Google Scholar] [CrossRef]
- Wallace, D.J.; Furie, R.A.; Tanaka, Y.; Kalunian, K.C.; Mosca, M.; Petri, M.A.; Dörner, T.; Cardiel, M.H.; Bruce, I.N.; Gomez, E.; et al. Baricitinib for systemic lupus erythematosus: A double-blind, randomised, placebo-controlled, phase 2 trial. Lancet 2018, 392, 222–231. [Google Scholar] [CrossRef]
- King, B.; Ko, J.; Forman, S.; Ohyama, M.; Mesinkovska, N.; Yu, G.; McCollam, J.; Gamalo, M.; Janes, J.; Edson-Heredia, E.; et al. Efficacy and safety of the oral Janus kinase inhibitor baricitinib in the treatment of adults with alopecia areata: Phase 2 results from a randomized controlled study. J. Am. Acad. Dermatol. 2021. [Google Scholar] [CrossRef]
- Huizinga, T.W.; Kay, J.; Harigai, M.; Keystone, E.; Smolen, J.; Rosas, J.; Emery, P.; Hall, S.; van den Bosch, F.; Schienberg, M.; et al. e48 Effects of baricitinib on haematological laboratory parameters in patients with rheumatoid arthritis. Rheumatology 2018, 57. [Google Scholar] [CrossRef] [Green Version]
- Anjara, P.; Jiang, M.; Mundae, M. Symptomatic elevation creatine kinase following treatment of rheumatoid arthritis with baricitinib. Clin. Rheumatol. 2020, 39, 613–614. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V.; Ugel, S.; Tinazzi, E.; Vella, A.; De Sanctis, F.; Canè, S.; Batani, V.; Trovato, R.; Fiore, A.; Petrova, V.; et al. Baricitinib restrains the immune dysregulation in COVID-19 patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Cantini, F.; Niccoli, L.; Nannini, C.; Matarrese, D.; di Natale, M.E.; Lotti, P.; Aquilini, D.; Landini, G.; Cimolato, B.; Di Pietro, M.A.; et al. Beneficial impact of Baricitinib in COVID-19 moderate pneumonia; multicentre study. J. Infect. 2020, 81. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, J.L.; Sanchez-Nievas, G.; Arevalo-Serrano, J.; Garcia-Gomez, C.; Jimenez-Vizuete, J.M.; Martinez-Alfaro, E. Baricitinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: An observational cohort study. Rheumatology 2021, 60, 399–407. [Google Scholar] [CrossRef] [PubMed]
- NIH COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 30 May 2021).
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet. Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Xu, Z.S.; Shu, T.; Kang, L.; Wu, D.; Zhou, X.; Liao, B.W.; Sun, X.L.; Zhou, X.; Wang, Y.Y. Temporal profiling of plasma cytokines, chemokines and growth factors from mild, severe and fatal COVID-19 patients. Signal Transduct. Target. Ther. 2020, 5, 100. [Google Scholar] [CrossRef]
- Yang, L.; Liu, S.; Liu, J.; Zhang, Z.; Wan, X.; Huang, B.; Chen, Y.; Zhang, Y. COVID-19: Immunopathogenesis and Immunotherapeutics. Signal Transduct. Target. Ther. 2020, 5, 128. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rojas, M.A.; Vega-Vega, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiology. Ren. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef] [PubMed]
- Verstovsek, S.; Kantarjian, H.; Mesa, R.A.; Pardanani, A.D.; Cortes-Franco, J.; Thomas, D.A.; Estrov, Z.; Fridman, J.S.; Bradley, E.C.; Erickson-Viitanen, S.; et al. Safety and Efficacy of INCB018424, a JAK1 and JAK2 Inhibitor, in Myelofibrosis. N. Engl. J. Med. 2010, 363, 1117–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, H.A. Fedratinib: First Approval. Drugs 2019, 79, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Georgeon, S.; Moser, R.; Moore, D.J.; Caflisch, A.; Hantschel, O. Specificity and mechanism-of-action of the JAK2 tyrosine kinase inhibitors ruxolitinib and SAR302503 (TG101348). Leukemia 2014, 28, 404–407. [Google Scholar] [CrossRef]
- Yeleswaram, S.; Smith, P.; Burn, T.; Covington, M.; Juvekar, A.; Li, Y.; Squier, P.; Langmuir, P. Inhibition of cytokine signaling by ruxolitinib and implications for COVID-19 treatment. Clin. Immunol. 2020, 218, 108517. [Google Scholar] [CrossRef]
- Chen, C.-X.; Wang, J.-J.; Li, H.; Yuan, L.-T.; Gale, R.P.; Liang, Y. JAK-inhibitors for coronavirus disease-2019 (COVID-19): A meta-analysis. Leukemia 2021, 1–5. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties/Drug | Baricitinib [32] | Ruxolitinib [33] | Fedratinib [34] |
|---|---|---|---|
| TPSA a (Å2) | 128.94 | 83.18 | 116.86 |
| Log Po/w (XLOGP3) b | −0.46 | 2.12 | 4.76 |
| Log Po/w (MLOGP) c | −0.58 | 1.36 | 2.47 |
| HBD d | 1 | 1 | 3 |
| HBA e | 7 | 4 | 9 |
| BBB d | 0.009148 (CNS −ve) | 0.148161 (CNS −ve) | 0.781302 (CNS −ve) |
| Caco-2 e (nm/s) | 1.55292 (Low) | 13.7647 (Medium) | 20.9596 (Medium) |
| HIA f | 93.89 % | 92.38% | 93.98% |
| P-gp inhibitor | −ve | +ve | −ve |
| P-gp substrate | +ve | +ve | −ve |
| PPB (%) | 87.49% (50%) | 84.28% (97%) | 83.95% (92%) |
| Log Kp (skin) g | −3.93772 | −3.97931 | −2.17719 |
| F (10%) score h | 0.55 (0.79) | 0.55 (0.95) | 0.55 (0.96) |
| hERG-block activity | Medium-risk | Medium-risk | High-risk |
| Repurposed JAK Inhibitor | Study Title | Study Design | Phase | Status | Clinical Trial ID |
|---|---|---|---|---|---|
| Baricitinib | Treatment of Moderate to Severe Coronavirus Disease (COVID-19) in Hospitalised Patients | Non-randomised Parallel Assignment | Phase 2 | recruiting | NCT04321993 |
| Baricitinib | A Study of Baricitinib (LY3009104) in Participants With COVID-19 (COV-BARRIER) | Randomised Parallel Assignment Double blind | Phase 3 | recruiting | NCT04421027 |
| Baricitinib | Baricitinib Therapy in COVID-19 | Non-randomised Cross-over assignment | Phase 2 and 3 | Completed | NCT04358614 |
| Baricitinib (+Hydroxy chloroquine) | Baricitinib, Placebo and Antiviral Therapy for the Treatment of Patients With Moderate and Severe COVID-19 | Randomised Parallel Assignment Double blind | Phase 2 | recruiting | NCT04373044 |
| Baricitinib And remdesivir ACTT-2 | Adaptive COVID-19 Treatment Trial 2 (ACTT-2) | Interventional (Clinical Trial) Randomized Parallel Assignment | Phase 3 | Completed | NCT04401579 Completed and published [42] |
| ACTT-4 Baricitinib in comparison to Remdesivir, and dexamethasone as monotherapies | Adaptive COVID-19 Treatment Trial 4 (ACTT-4) | Interventional (Clinical Trial) Randomized Parallel Assignment | Phase 3 | This study closed because neither treatment regimen was significantly better than the other. | NCT04640168 |
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saber-Ayad, M.; Hammoudeh, S.; Abu-Gharbieh, E.; Hamoudi, R.; Tarazi, H.; Al-Tel, T.H.; Hamid, Q. Current Status of Baricitinib as a Repurposed Therapy for COVID-19. Pharmaceuticals 2021, 14, 680. https://doi.org/10.3390/ph14070680
Saber-Ayad M, Hammoudeh S, Abu-Gharbieh E, Hamoudi R, Tarazi H, Al-Tel TH, Hamid Q. Current Status of Baricitinib as a Repurposed Therapy for COVID-19. Pharmaceuticals. 2021; 14(7):680. https://doi.org/10.3390/ph14070680
Chicago/Turabian StyleSaber-Ayad, Maha, Sarah Hammoudeh, Eman Abu-Gharbieh, Rifat Hamoudi, Hamadeh Tarazi, Taleb H. Al-Tel, and Qutayba Hamid. 2021. "Current Status of Baricitinib as a Repurposed Therapy for COVID-19" Pharmaceuticals 14, no. 7: 680. https://doi.org/10.3390/ph14070680
APA StyleSaber-Ayad, M., Hammoudeh, S., Abu-Gharbieh, E., Hamoudi, R., Tarazi, H., Al-Tel, T. H., & Hamid, Q. (2021). Current Status of Baricitinib as a Repurposed Therapy for COVID-19. Pharmaceuticals, 14(7), 680. https://doi.org/10.3390/ph14070680