
A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units

 ,
,  ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Descriptive Analysis of Reports during the 1 January 2003 and 7 August 2023 Period
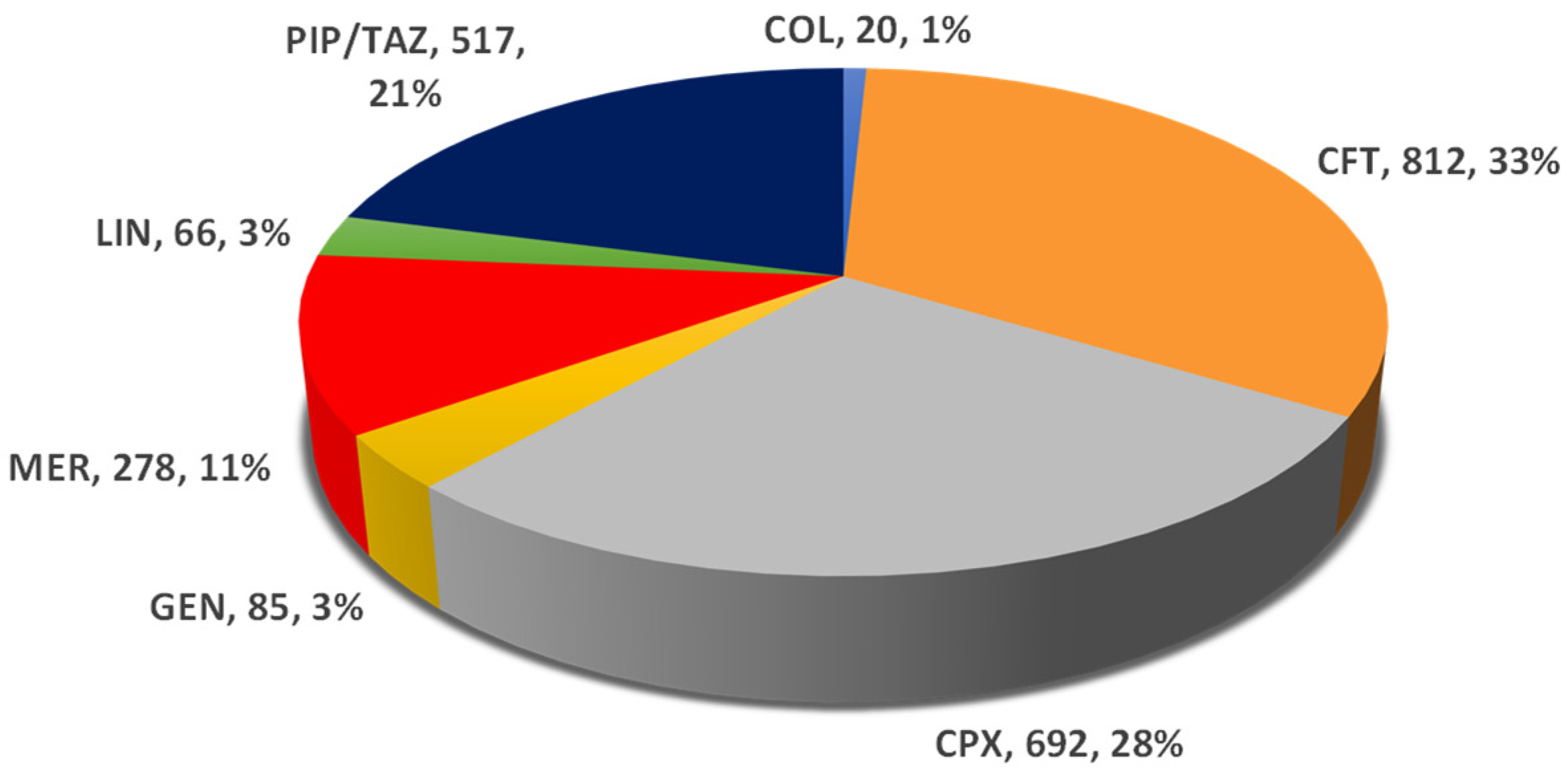
2.1.1. Total Number of Reports Related to Clostridioides difficile Infection
- (a)
- Total ICSRs
- (b)
- Total ADRs related to Clostridioides difficile
- (c)
- Proportion of ADRs related to Clostridioides difficile from total ICSRs
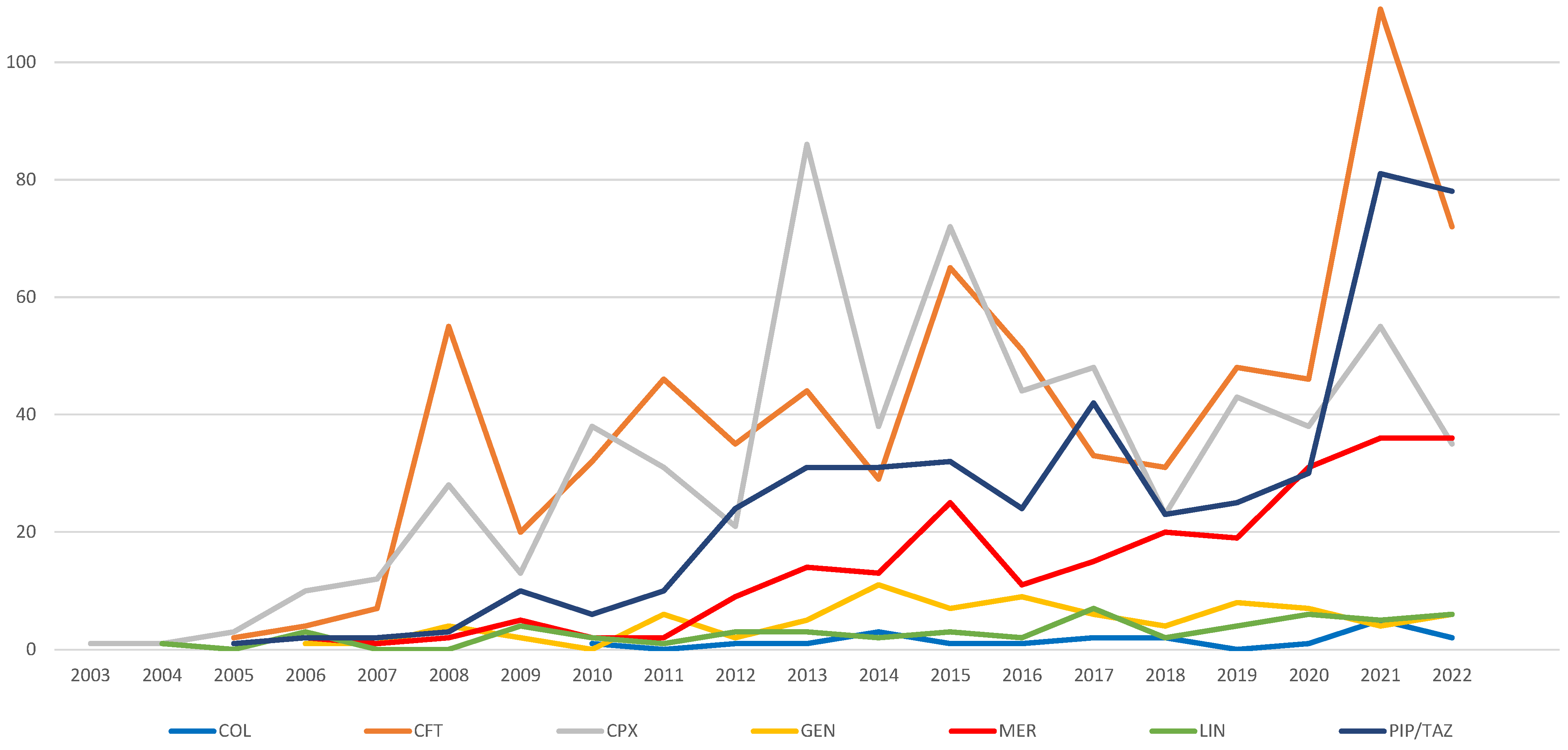
2.1.2. Evolution of ICSR Number Related to Clostridioides difficile Infection
2.1.3. Distribution of CDI-Related Reports by Outcome
2.2. Disproportionality Analysis for Data Reported between 1 January 2003 and 7 August 2023
Forecasting the Number of ICSRs Related to Clostridioides Difficile Infection for 2023–2025 for the Analyzed Antibiotics
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Materials
4.3. Data Analysis
- ROR = reporting odds ratio;
- a = evaluated ADR for targeted drug;
- b = other ADRs for targeted drug;
- c = evaluated ADR for the drug used for comparison;
- d = other ADRs for the drug used for comparison.
- CI = confidence interval;
- SE = standard error.
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADRs | Adverse drug reactions |
| AI | Number of infections/year |
| AMI | Amikacin |
| CD | Clostridioides difficile |
| CDI | Clostridioides difficile infection |
| CEF | Ceftazidime |
| CFT | Ceftriaxone |
| CI | Confidence interval |
| CLI | Clindamycin |
| COL | Colistimethate/Colistin |
| CPX | Ciprofloxacin |
| EMA | European Medicines Agency |
| EV | EudraVigilance |
| FAERS | Food and Drug Administration Adverse Event Reporting System |
| GEN | Gentamicin |
| ICSR | Individual Case Safety Report |
| ICU | Intensive Care Unit |
| IM | Average index of modification |
| IMI | Imipenem/Cilastatin |
| LEV | Levofloxacin |
| LIN | Linezolid |
| MER | Meropenem |
| PIP/TAZ | Piperacilin/Tazobactam |
| ROR | Reporting odds ratio |
| SE | Standard error |
| USD | United States Dollars |
References
- Jones, A.M.; Kuijper, E.J.; Wilcox, M.H. Clostridium difficile: A European Perspective. J. Infect. 2013, 66, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Birlutiu, V.; Mircea Birlutiu, R.; Rusu, H.M. The Influence of the Use of Metronidazole Associated with Vancomycin in Reducing the Mortality Rate at 30 Days in Patients with Clostridium difficile Infection. Biomed. Res. 2018, 29, 606–609. [Google Scholar] [CrossRef]
- Birlutiu, V.; Dobritoiu, E.S.; Lupu, C.D.; Herteliu, C.; Birlutiu, R.M.; Dragomirescu, D.; Vorovenci, A. Our Experience with 80 Cases of SARS-CoV-2-Clostridioides Difficile Co-Infection: An Observational Study. Medicine 2022, 101, E29823. [Google Scholar] [CrossRef]
- Aguilar, R.C.; Salmanton-García, J.; Carney, J.; Böll, B.; Kochanek, M.; Jazmati, N.; Cornely, O.A.; Vehreschild, M.J.G.T. Clostridioides difficile Infections in the Intensive Care Unit: A Monocentric Cohort Study. Infection 2020, 48, 421–427. [Google Scholar] [CrossRef]
- Chiș, A.A.; Rus, L.L.; Morgovan, C.; Arseniu, A.M.; Frum, A.; Vonica-țincu, A.L.; Gligor, F.G.; Mureșan, M.L.; Dobrea, C.M. Microbial Resistance to Antibiotics and Effective Antibiotherapy. Biomedicines 2022, 10, 1121. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.J.; Dubberke, E.R. Clostridium difficile Infection in the Intensive Care Unit. Infect. Dis. Clin. N. Am. 2009, 23, 727–743. [Google Scholar] [CrossRef]
- Codru, I.R.; Sava, M.; Vintilă, B.I.; Bereanu, A.S.; Bîrluțiu, V. A Study on the Contributions of Sonication to the Identification of Bacteria Associated with Intubation Cannula Biofilm and the Risk of Ventilator-Associated Pneumonia. Medicina 2023, 59, 1058. [Google Scholar] [CrossRef]
- da Fonseca Pestana Ribeiro, J.M.; Park, M. Less Empiric Broad-Spectrum Antibiotics Is More in the ICU. Intensive Care Med. 2020, 46, 783–786. [Google Scholar] [CrossRef]
- Vincent, J.L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; MacHado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef]
- Cisneros, J.M.; Rosso-Fernández, C.M.; Roca-Oporto, C.; De Pascale, G.; Jiménez-Jorge, S.; Fernández-Hinojosa, E.; Matthaiou, D.K.; Ramírez, P.; Díaz-Miguel, R.O.; Estella, A.; et al. Colistin versus Meropenem in the Empirical Treatment of Ventilator-Associated Pneumonia (Magic Bullet Study): An Investigator-Driven, Open-Label, Randomized, Noninferiority Controlled Trial. Crit. Care 2019, 23, 383. [Google Scholar] [CrossRef]
- Hashemian, S.M.R.; Farhadi, T.; Ganjparvar, M. Linezolid: A Review of Its Properties, Function, and Use in Critical Care. Drug Des. Dev. Ther. 2018, 12, 1759–1767. [Google Scholar] [CrossRef]
- Rosso-Fernández, C.; Montero, J.G.; Antonelli, M.; Dimopoulos, G.; Cisneros, J.M.; Gallmore, P.R.; Bonastre, J.; González, J.C.M.; Díaz-Miguel, R.O.; García, A.E.; et al. Safety and Efficacy of Colistin versus Meropenem in the Empirical Treatment of Ventilator-Associated Pneumonia as Part of a Macro-Project Funded by the Seventh Framework Program of the European Commission Studying off-Patent Antibiotics: Study Protocol for a randomized controlled trial. Trials 2015, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Steffens, N.A.; Zimmermann, E.S.; Nichelle, S.M.; Brucker, N. Meropenem Use and Therapeutic Drug Monitoring in Clinical Practice: A Literature Review. J. Clin. Pharm. Ther. 2021, 46, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Vintila, B.I.; Arseniu, A.M.; Butuca, A.; Sava, M.; Bîrluțiu, V.; Rus, L.L.; Axente, D.D.; Morgovan, C.; Gligor, F.G. Adverse Drug Reactions Relevant to Drug Resistance and Ineffectiveness Associated with Meropenem, Linezolid, and Colistin: An Analysis Based on Spontaneous Reports from the European Pharmacovigilance Database. Antibiotics 2023, 12, 918. [Google Scholar] [CrossRef] [PubMed]
- Aurilio, C.; Sansone, P.; Barbarisi, M.; Pota, V.; Giaccari, L.G.; Coppolino, F.; Barbarisi, A.; Passavanti, M.B.; Pace, M.C. Mechanisms of Action of Carbapenem Resistance. Antibiotics 2022, 11, 421. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.L.; Periyasamy, P.; Saud, M.N.; Robert, S.A.; Gan, L.Y.; Chin, S.Y.; Pau, K.B.; Kong, S.H.; Tajurudin, F.W.; Yin, M.K.; et al. Plethora of Antibiotics Usage and Evaluation of Carbapenem Prescribing Pattern in Intensive Care Units: A Single-Center Experience of Malaysian Academic Hospital. Antibiotics 2022, 11, 1172. [Google Scholar] [CrossRef]
- Rafey, A.; Jahan, S.; Farooq, U.; Akhtar, F.; Irshad, M.; Nizamuddin, S.; Parveen, A. Antibiotics Associated With Clostridium Difficile Infection. Cureus 2023, 15, e39029. [Google Scholar] [CrossRef]
- Chen, H.; Du, Y.; Xia, Q.; Li, Y.; Song, S.; Huang, X. Role of Linezolid Combination Therapy for Serious Infections: Review of the Current Evidence. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1043–1052. [Google Scholar] [CrossRef]
- Zabel, L.T.; Worm, S. Linezolid Contributed to Clostridium Difficile Colitis with Fatal Outcome. Infection 2005, 33, 155–157. [Google Scholar] [CrossRef]
- Moubareck, C.A. Polymyxins and Bacterial Membranes: A Review of Antibacterial Activity and Mechanisms of Resistance. Membranes 2020, 10, 181. [Google Scholar] [CrossRef]
- Tijerina-Rodríguez, L.; Garza-González, E.; Martínez-Meléndez, A.; Morfín-Otero, R.; Camacho-Ortiz, A.; Gonzalez-Diaz, E.; Perez-Gomez, H.R.; Villarreal-Treviño, L.; Maldonado-Garza, H.; Esparza-Ahumada, S.; et al. Clinical Characteristics Associated with the Severity of Clostridium [Clostridioides] Difficile Infection in a Tertiary Teaching Hospital from Mexico. Biomed. J. 2022, 45, 200–205. [Google Scholar] [CrossRef] [PubMed]
- El-Haffaf, I.; Caissy, J.A.; Marsot, A. Piperacillin-Tazobactam in Intensive Care Units: A Review of Population Pharmacokinetic Analyses. Clin. Pharmacokinet. 2021, 60, 855–875. [Google Scholar] [CrossRef]
- Khilnani, G.C.; Zirpe, K.; Hadda, V.; Mehta, Y.; Madan, K.; Kulkarni, A.; Mohan, A.; Dixit, S.; Guleria, R.; Bhattacharya, P. Guidelines for Antibiotic Prescription in Intensive Care Unit. Indian J. Crit. Care Med. 2019, 23, 1–63. [Google Scholar] [CrossRef]
- Kayambankadzanja, R.K.; Lihaka, M.; Barratt-Due, A.; Kachingwe, M.; Kumwenda, W.; Lester, R.; Bilima, S.; Eriksen, J.; Baker, T. The Use of Antibiotics in the Intensive Care Unit of a Tertiary Hospital in Malawi. BMC Infect. Dis. 2020, 20, 776. [Google Scholar] [CrossRef] [PubMed]
- Gieling, E.M.; Wallenburg, E.; Frenzel, T.; de Lange, D.W.; Schouten, J.A.; ten Oever, J.; Kolwijck, E.; Burger, D.M.; Pickkers, P.; ter Heine, R.; et al. Higher Dosage of Ciprofloxacin Necessary in Critically Ill Patients: A New Dosing Algorithm Based on Renal Function and Pathogen Susceptibility. Clin. Pharmacol. Ther. 2020, 108, 770–774. [Google Scholar] [CrossRef]
- Grigore, N.; Totan, M.; Pirvut, V.; Mitariu, S.I.C.; Chicea, R.; Sava, M.; Hasegan, A. A Risk Assessment of Clostridium difficile Infection after Antibiotherapy for Urinary Tract Infections in the Urology Department for Hospitalized Patients. Rev. Chim. 2017, 68, 1453–1456. [Google Scholar] [CrossRef]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.E.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 Update on the Treatment Guidance Document for Clostridioides difficile Infection in Adults. Clin. Microbiol. Infect. 2021, 27 (Suppl. S2), S1–S21. [Google Scholar] [CrossRef]
- Orenstein, R.; Patron, R.L. Clostridioides difficile Therapeutics: Guidelines and Beyond. Ther. Adv. Infect. Dis. 2019, 6, 2049936119868548. [Google Scholar] [CrossRef]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Anderco, P.; Birsan, S. Fecal Microbiota Transplantation in Inflammatory Bowel Disease. Biomedicines 2023, 11, 1016. [Google Scholar] [CrossRef]
- Popa, D.; Neamtu, B.; Mihalache, M.; Boicean, A.; Banciu, A.; Banciu, D.D.; Moga, D.F.C.; Birlutiu, V. Fecal Microbiota Transplant in Severe and Non-Severe Clostridioides difficile Infection. Is There a Role of FMT in Primary Severe CDI? J. Clin. Med. 2021, 10, 5822. [Google Scholar] [CrossRef]
- Boicean, A.; Neamtu, B.; Birsan, S.; Batar, F.; Tanasescu, C.; Dura, H.; Roman, M.D.; Hașegan, A.; Bratu, D.; Mihetiu, A.; et al. Fecal Microbiota Transplantation in Patients Co-Infected with SARS-CoV2 and Clostridioides difficile. Biomedicines 2022, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Ge, I.Y.; Fevrier, H.B.; Conell, C.; Kheraj, M.N.; Flint, A.C.; Smith, D.S.; Herrinton, L.J. Reducing Risk of Clostridium difficile Infection and Overall Use of Antibiotic in the Outpatient Treatment of Urinary Tract Infection. Ther. Adv. Urol. 2018, 10, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Trigkidis, K.K.; Boukouvala, E.; Falagas, M.E. Clostridium difficile Infection Following Systemic Antibiotic Administration in Randomised Controlled Trials: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2016, 48, 1–10. [Google Scholar] [CrossRef]
- Slimings, C.; Riley, T.V. Antibiotics and Healthcare Facility-Associated Clostridioides difficile Infection: Systematic Review and Meta-Analysis 2020 Update. J. Antimicrob. Chemother. 2021, 76, 1676–1688. [Google Scholar] [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Rychlíčková, J.; Kubíčková, V.; Suk, P.; Urbánek, K. Challenges of Colistin Use in ICU and Therapeutic Drug Monitoring: A Literature Review. Antibiotics 2023, 12, 437. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.C.; Arakkal, A.T.; Sewell, D.K.; Segre, A.M.; Tholany, J.; Polgreen, P.M. Comparison of Different Antibiotics and the Risk for Community-Associated Clostridioides difficile Infection: A Case–Control Study. Open Forum Infect. Dis. 2023, 10, ofad413. [Google Scholar] [CrossRef]
- Liu, C.; Monaghan, T.; Yadegar, A.; Louie, T.; Kao, D. Insights into the Evolving Epidemiology of Clostridioides difficile Infection and Treatment: A Global Perspective. Antibiotics 2023, 12, 1141. [Google Scholar] [CrossRef]
- Czepiel, J.; Dróżdż, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultańska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile Infection: Review. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1211–1221. [Google Scholar] [CrossRef]
- Eze, P.; Balsells, E.; Kyaw, M.H.; Nair, H. Risk Factors for Clostridium difficile Infections—An Overview of the Evidence Base and Challenges in Data Synthesis. J. Glob. Health 2017, 7, 010417. [Google Scholar] [CrossRef]
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.; Reveles, K.R.; Obodozie-Ofoegbu, O.O.; Frei, C.R. Clostridium difficile Infection Risk with Important Antibiotic Classes: An Analysis of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2019, 16, 630–635. [Google Scholar] [CrossRef]
- Mullish, B.H.; Williams, H.R.T. Clostridium difficile Infection and Antibiotic-Associated Diarrhoea. Clin. Med. 2018, 18, 237–241. [Google Scholar] [CrossRef]
- Pépin, J.; Saheb, N.; Coulombe, M.-A.; Alary, M.-E.; Corriveau, M.-P.; Authier, S.; Leblanc, M.; ve Rivard, G.; Bettez, M.; rie Primeau, V.; et al. Emergence of Fluoroquinolones as the Predominant Risk Factor for Clostridium difficile-Associated Diarrhea: A Cohort Study during an Epidemic in Quebec. Clin. Infect. Dis. 2005, 41, 1254–1260. [Google Scholar] [CrossRef]
- Althaqafi, A.; Munshi, A.; Baghlaf, B.; Munshi, E.; Malakah, M.; Almarhabi, H.; Alharbi, M.; Alsaedi, A. The Prevalence, Risk Factors, and Complications of Clostridium difficile Infection in a Tertiary Care Center, Western Region, Saudi Arabia. J. Infect. Public Health 2022, 15, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Khanafer, N.; Daneman, N.; Fisman, D.N. Meta-Analysis of Antibiotics and the Risk of Community-Associated Clostridium difficile Infection. Antimicrob. Agents Chemother. 2013, 57, 2326–2332. [Google Scholar] [CrossRef]
- Negrut, N.; Nistor-Cseppento, D.C.; Khan, S.A.; Pantis, C.; Maghiar, T.A.; Maghiar, O.; Aleya, S.; Rus, M.; Tit, D.M.; Aleya, L.; et al. Clostridium difficile Infection Epidemiology over a Period of 8 Years—A Single Centre Study. Sustainability 2020, 12, 4439. [Google Scholar] [CrossRef]
- Granata, G.; Monchi, M.; Li, D.; Song, Y.; Bai, Z.; Xi, X.; Liu, F.; Zhang, Y.; Qin, C.; Du, D.; et al. Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure. Antibiotics 2023, 12, 1109. [Google Scholar] [CrossRef]
- European Database of Suspected Adverse Drug Reaction Reports. Available online: https://www.adrreports.eu/ (accessed on 11 October 2023).
- Postigo, R.; Brosch, S.; Slattery, J.; van Haren, A.; Dogné, J.M.; Kurz, X.; Candore, G.; Domergue, F.; Arlett, P. EudraVigilance Medicines Safety Database: Publicly Accessible Data for Research and Public Health Protection. Drug Saf. 2018, 41, 665–675. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Guidelines on Good Pharmacovigilance Practices (GVP)—Introductory Cover Note, Last Updated with Chapter P.IV on Pharmacovigilance for the Paediatric Population Finalised Post-Public Consultation; European Medicines Agency: London, UK, 2018.
- Screening for Adverse Reactions in EudraVigilance. Available online: https://www.ema.europa.eu/en/documents/other/screening-adverse-reactions-eudravigilance_en.pdf (accessed on 11 October 2023).
- MedCalc’s Odds Ratio Calculator. Available online: https://www.medcalc.org/calc/odds_ratio.php (accessed on 11 October 2023).
- European Database of Suspected Adverse Drug Reaction Reports—Disclaimer. Available online: https://www.adrreports.eu/en/disclaimer.html (accessed on 29 October 2023).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CFT | CPX | COL | GEN | LIN | MER | PIP/TAZ | |
|---|---|---|---|---|---|---|---|
| Minimum | 2 | 1 | 0 | 0 | 0 | 1 | 1 |
| Maximum | 109 | 86 | 5 | 11 | 7 | 36 | 81 |
| Total ICSR | 729 | 640 | 20 | 83 | 54 | 244 | 455 |
| Mean | 40.5 | 32.0 | 1.5 | 4.9 | 2.8 | 13.6 | 25.3 |
| Standard Deviation | 26.0 | 22.8 | 1.3 | 3.1 | 0.5 | 12.0 | 5.5 |
| Confidence Level (95.0%) | 12.91852 | 10.68856 | 0.8037861 | 1.573029 | 1.00671 | 5.989898 | 11.63973 |
| lower bound | 27.6 | 21.3 | 0.7 | 3.3 | 1.8 | 7.6 | 13.6 |
| upper bound | 53.4 | 42.7 | 2.3 | 6.5 | 3.8 | 19.5 | 36.9 |
| Intercept | Slope | 2023 | 2024 | 2025 | |||
|---|---|---|---|---|---|---|---|
| COL | 0.5 | 0.148352 | Predicted values | 2.6 | 2.7 | 2.9 | |
| 95% Prediction Limits | Lower | 0 | 0 | 0 | |||
| Upper | 5.8 | 6.0 | 6.3 | ||||
| 95% Confidence Limits | Lower | 1.0 | 0.9 | 0.9 | |||
| Upper | 4.2 | 4.5 | 4.9 | ||||
| p-value | 0.1381 | ||||||
| CFT | 7.15686 | 3.5098 | Predicted values | 73.8 | 77.4 | 80.9 | |
| 95% Prediction Limits | Lower | 30.0 | 32.8 | 35.5 | |||
| Upper | 117.7 | 121.9 | 126.2 | ||||
| 95% Confidence Limits | Lower | 54.5 | 56.4 | 58.3 | |||
| Upper | 93.2 | 98.3 | 103.4 | ||||
| p-value | <0.001 | ||||||
| CPX | 6.01053 | 2.475193 | Predicted values | 58.0 | 60.5 | 62.9 | |
| 95% Prediction Limits | Lower | 16.3 | 18.2 | 20.1 | |||
| Upper | 99.7 | 102.7 | 105.8 | ||||
| 95% Confidence Limits | Lower | 40.4 | 41.6 | 42.7 | |||
| Upper | 75.6 | 79.3 | 83.1 | ||||
| p-value | <0.05 | ||||||
| GEN | 1.77206 | 0.345588 | Predicted values | 8.0 | 8.3 | 8.7 | |
| 95% Prediction Limits | Lower | 1.8 | 2.0 | 2.2 | |||
| Upper | 14.2 | 14.7 | 15.1 | ||||
| 95% Confidence Limits | Lower | 5.2 | 5.3 | 5.4 | |||
| Upper | 10.8 | 11.4 | 12.0 | ||||
| p-value | <0.05 | ||||||
| LIN | 0.122807 | 0.27193 | Predicted values | 5.6 | 5.8 | 6.1 | |
| 95% Prediction Limits | Lower | 2.1 | 2.4 | 2.6 | |||
| Upper | 9.0 | 9.3 | 9.6 | ||||
| 95% Confidence Limits | Lower | 4.1 | 4.2 | 4.4 | |||
| Upper | 7.0 | 7.4 | 7.8 | ||||
| p-value | <0.001 | ||||||
| MER | −6.05229 | 2.06398 | Predicted values | 33.2 | 35.2 | 37.3 | |
| 95% Prediction Limits | Lower | 21.3 | 23.2 | 25.0 | |||
| Upper | 45.0 | 47.3 | 49.5 | ||||
| 95% Confidence Limits | Lower | 27.9 | 29.6 | 31.2 | |||
| Upper | 38.4 | 40.9 | 43.4 | ||||
| p-value | <0.0001 | ||||||
| PIP/TAZ | −9.65359 | 3.67699 | Predicted values | 60.2 | 63.9 | 67.6 | |
| 95% Prediction Limits | Lower | 29.2 | 32.3 | 35.5 | |||
| Upper | 91.3 | 95.4 | 99.7 | ||||
| 95% Confidence Limits | Lower | 46.5 | 49.1 | 51.6 | |||
| Upper | 73.9 | 78.7 | 83.5 | ||||
| p-value | <0.0001 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vintila, B.I.; Arseniu, A.M.; Morgovan, C.; Butuca, A.; Sava, M.; Bîrluțiu, V.; Rus, L.L.; Ghibu, S.; Bereanu, A.S.; Roxana Codru, I.; et al. A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units. Pharmaceuticals 2023, 16, 1585. https://doi.org/10.3390/ph16111585
Vintila BI, Arseniu AM, Morgovan C, Butuca A, Sava M, Bîrluțiu V, Rus LL, Ghibu S, Bereanu AS, Roxana Codru I, et al. A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units. Pharmaceuticals. 2023; 16(11):1585. https://doi.org/10.3390/ph16111585
Chicago/Turabian StyleVintila, Bogdan Ioan, Anca Maria Arseniu, Claudiu Morgovan, Anca Butuca, Mihai Sava, Victoria Bîrluțiu, Luca Liviu Rus, Steliana Ghibu, Alina Simona Bereanu, Ioana Roxana Codru, and et al. 2023. "A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units" Pharmaceuticals 16, no. 11: 1585. https://doi.org/10.3390/ph16111585
APA StyleVintila, B. I., Arseniu, A. M., Morgovan, C., Butuca, A., Sava, M., Bîrluțiu, V., Rus, L. L., Ghibu, S., Bereanu, A. S., Roxana Codru, I., & Gligor, F. G. (2023). A Pharmacovigilance Study Regarding the Risk of Antibiotic-Associated Clostridioides difficile Infection Based on Reports from the EudraVigilance Database: Analysis of Some of the Most Used Antibiotics in Intensive Care Units. Pharmaceuticals, 16(11), 1585. https://doi.org/10.3390/ph16111585