Abstract
The chemical constituents of the Cannabis plant known as cannabinoids have been extensively researched for their potential therapeutic benefits. The use of cannabinoids applied to the skin as a potential method for both skin-related benefits and systemic administration has attracted increasing interest in recent years. This review aims to present an overview of the most recent scientific research on cannabinoids used topically, including their potential advantages for treating a number of skin conditions like psoriasis, atopic dermatitis, and acne. Additionally, with a focus on the pharmacokinetics and security of this route of administration, we investigate the potential of the transdermal delivery of cannabinoids as a method of systemic administration. The review also discusses the restrictions and difficulties related to the application of cannabinoids on the skin, emphasizing the potential of topical cannabinoids as a promising route for both localized and systemic administration. More studies are required to fully comprehend the efficacy and safety of cannabinoids in various settings.
1. Introduction
For over two millennia, the Cannabis plant has been used for both recreational and therapeutic purposes [1,2], with various archaeological discoveries confirming that it has been cultivated across most of the known world. Ancient Chinese medicine, for example, used the plant for musculoskeletal conditions and to relax and harmonize the mind and body [3], while the Greeks and Romans used it for recreational consumption and medical use [4]. The plant’s psychoactive and analgesic qualities were used by Indians to treat various types of pain [5,6]. In the first Chinese Pharmacopeia, Cannabis seeds were recommended for the treatment of skin diseases and disorders, such as eczema, psoriasis, and other inflammatory conditions [7]. Nowadays, due to the increasing interest in sustainability and ecological issues, the use of plant-based natural products in dermatology has become a valuable method for improving therapies with respect to acute and chronic skin diseases and disorders, with lower costs for patients and healthcare systems [7]. Cannabis, a representative genus of the Cannabaceae family [8], is an annual herbaceous plant, which includes the Cannabis sativa L. (hemp and marijuana), C. ruderalis Janisch, and C. indica Lam. species [9]. Cannabis is a genus characterized by dioecy [10], producing male and female inflorescences on different individuals that are obligatory out-crossers [11]. The plant is naturally occurring and is part of the local flora in the Indian Peninsula and Central Asia; however, in the rest of the world, it is cultivated for a variety of purposes. Cannabis is used in its unprocessed state as dried flower bulbs, known as marijuana, and as pieces of resin, known as hashish [12].
What makes each variety or strain of the Cannabis plant unique in its own way is the presence of three different classes of chemical compounds that exhibit biological activity: phytocannabinoids (pCBs), flavonoids, and terpenes/terpenoids [13]; they may act either individually and/or synergistically [14]. Depending on the plant content in each of these molecules, various modulatory or potentiation pharmacological effects have been observed [15,16]. A recent classification of Cannabis plant constituents identified 545 entities divided into chemical classes based on their structural similarities [17]. Thus, more than 100 Cannabis constituents belong to the pCB class, which is mostly extracted from female plants, with the most well-known being tetrahydrocannabinol (THC) with its two derivatives Δ8-tetrahydrocannabinol (Δ8-THC) and Δ9-tetrahydrocannabinol (Δ9-THC); cannabidiol (CBD); and cannabigerol (CBG) [18,19]. The rest of the natural compounds are classified into seven other main classes: cannabinol (CBN), cannabielsoin (CBE), cannabichromene (CBC), cannabicyclol (CBL), cannabinodiol (CBND), cannabitriol (CBT), and other types of cannabinoids [20].
The pharmacokinetics and metabolism of natural cannabinoids depend on the route of administration [13]. pCBs are known to have high lipophilicity, low aqueous solubility, rapid metabolism, poor bioavailability, and erratic pharmacokinetics [21], being temperature-, light-, and auto-oxidation-sensitive [22]. For example, the oral bioavailability of CBD ranges between 13% and 19% [23] due to its incomplete oral absorption and high hepatic clearance [2], while its bioavailability increases at 34–46% when it is absorbed intranasally [24]. Also, after topical in vivo gel applications, CBD provided significant plasma levels [24]. Consequently, pCB formulations emphasize a low oral bioavailability that led to the necessity of other administration routes to improve pCBs’ bioavailability and efficacy, such as the local (topical), transcutaneous (transdermal), pulmonary, and transmucosal routes [25] that include intranasal and rectal routes, with the last one demonstrating double the rate of bioavailability compared to the oral route [22]. Topical and transdermal administration demonstrated several advantages, such as a higher bioavailability rate, prolonged steady-state plasma concentration, and a reduction in psychoactive impacts of the drug due to its passive diffusion in the main barrier of the skin, stratum corneum [22]. To evaluate the efficacy of pCB topical applications, a plethora of studies emphasizing the mechanisms of action at the molecular level, redox transformation, electronic structure, and stability; and the cytotoxic, phototoxic, and UVA or UVB photoprotective effects of pCBs have been performed [26]. To emphasize the mechanisms of action of pCBs at the molecular level, it has been demonstrated that CBD inhibits nuclear factor kappa B (NF-κB) and the genes involved in the expression of molecules with pro-inflammatory roles, such as cytokines and metalloproteinases [27]. Clinical studies emphasized that topical treatment with CBD-enriched ointment significantly improved skin parameters and disease symptomatology, proving that the topical application is a safe and non-invasive alternative for improving the quality of life in patients with various skin disorders [28].
Outside of clinical studies, to investigate the potential roles of pCBs for the treatment and alleviation of skin diseases and disorders, many types of cell lines have been used in various in vitro studies: inflamed human keratinocytes (HaCaT cells) [29], human SZ95 sebocytes [30], human eccrine-sweat-gland-derived immortalized NCL-SG3 model cells [31], human healthy and stress-induced premature senescent (SIPS) CCD-1064Sk dermal fibroblasts [32], or My-La and HuT-78 cutaneous T-cell lymphoma lines [33].
Skin conditions affect between 30% and 70% of people worldwide and more than 3000 acute and chronic skin diseases that significantly reduce the patients’ quality of life have been described [34]. Traditional systemic treatments used in dermatology are based on topical agents (corticosteroids, vitamin D analogues, moisturizers, retinoids, and calcineurin inhibitors), phototherapy, systemic immunotherapy, systemic antibiotics and hormones, antifungals, biological agents, or small molecule inhibitors. These classic treatments may emphasize several limitations, including poor responses to treatment, potential drug interactions, hepatic and renal toxicity, and even a significant risk of skin malignancy and teratogenicity [28]. The most significant adverse effects of current drug-based therapies applied in the most frequent skin diseases, such as psoriasis, atopic dermatitis, allergic contact dermatitis, asteatotic eczema, acne, and seborrhea, are listed in Table 1: xerosis; erythema; purpura; rosacea or alteration in skin pigmentation; photoaging; skin atrophy; itching; burning sensation; folliculitis; actinic keratosis; allergic reactions; hair loss or hypertrichosis; hyper-lipidaemia; hypertension; metabolic and nutritional disorders; headache; bone marrow suppression; leukopenia; bone growth stimulation; decreased bone density; the inhibition of the hypothalamic–pituitary–adrenal axis in children; herpes simplex reactivation; and delayed wound repair [35,36,37,38,39,40,41,42,43,44]. In dermatology, pCBs have demonstrated anti-inflammatory [27,30], anti-oxidative [45], anti-aging [32], anti-acne [30], and anti-UVA/UVB radiation damage proprieties [46]. Moreover, several pCBs emphasized potent antimicrobial activity against Gram-positive bacteria, including methicillin-resistant Staphylococcus aureus (MRSA) that may cause serious infection on the skin and other organs [47], which is possible due to the inhibition of Staphylococci adhesion to keratinocytes [48]. Interestingly, Luz-Veiga et al. have unveiled that CBD and CBG may be promising topical antimicrobial agents for different skin conditions without a negative impact on skin microbiota [48]. Feldman et al. have shown that CBD can be considered an alternative treatment against fungal infection due to its anti-biofilm activity against Candida albicans [49], which resides on the skin surface and may cause infections [50].
Consequently, Cannabis plant-derived compounds have been recommended for the treatment of many skin disorders and diseases, such as dry/seborrheic skin and acne [30]; atopic dermatitis (or eczema); psoriasis and resulting outcome scars [28,51]; pruritus, including neuropathic itch [52]; pain [53]; and mycosis fungoides, the most common type of cutaneous T-cell lymphoma (CTCL) [33]. An international cross-sectional survey study demonstrated that cannabinoid-based medicine (CBM) may alleviate pain and pruritus and improves wound healing and well-being in patients with epidermolysis bullosa (EB), a group of clinically and genetically heterogeneous genetic skin conditions that express fragile skin and mucosae [54]. In vivo studies demonstrated that, individually or combined, cannabinoids may reduce tumor growth or tumor cell proliferation and promote apoptosis and autophagy in melanoma cells, emerging as potential agents for the treatment of cutaneous melanoma [55]. Lichen simplex chronicus and multiple cutaneous squamous cell carcinoma (SCC) lesions have completely regressed with the topical application of 20% CBD oil [56]. Psoriasis, which emphasizes two clinical manifestations, psoriasis vulgaris and psoriatic arthritis, is the most common autoimmune skin disease that currently affects about 4% of the population [51]. pCBs are known as candidate drugs in the treatment of psoriasis due to their effects of inhibiting the proliferation of keratinocytes and modulating the associated inflammatory response [57]. Acne vulgaris (acne) affects 9.4% of the world’s population and 85% of adolescents [58]. CBD is well known for its anti-inflammatory effects on acne [58]. Both CBG and cannabigerovarin (CBGV) exert potential in the treatment of skin dryness, while CBC, cannabidivarin (CBDV), and Δ(9)-tetrahydrocannabivarin (THCV) have been proposed as novel anti-acne agents due to their efficacy [30]. In regions where cannabis use is legal, there are reported clinical cases where topical formulations including phytocannabinoids (CBD and THC), self-initiated by patients or prescribed by certain dermatologists and prepared by pharmacists, have been shown to be effective in treating a variety of skin conditions [59,60,61].
Cannabinoids work on the endocannabinoid system (ECS) [62]. The endocannabinoid receptors and their endogenous ligands were discovered and identified after the first compounds in the class were isolated and characterized. The endogenous endocannabinoid system (ECS) is represented by a molecular signaling network consisting of endocannabinoids, specific G-protein-coupled receptors (GPCRs), cannabinoid receptor 1 (CB1) and cannabinoid receptor 2 (CB2), and specific enzymes responsible for the synthesis, transport, and degradation of endocannabinoids [59]. Various studies have also identified non-CB1/CB2 receptors modulated by endocannabinoids, such as GPCRs (GPR18, GPR55, and GPR119), transient potential vanilloid receptors (TRPV1 and TRPV3), transient receptor potential ankyrin 1 (TRPA1), nuclear hormone receptors like peroxisome proliferator-activated receptors (PPARs), and others [2,63]. ECS plays a critical role in a number of physiological processes, including immune modulation, vasomotion and vasodilation, motor control, muscle fiber formation, cognitive memory, learning, anxiety, appetite, gastro-intestinal motility, sleep, fertility, lipogenesis, and the formation of insulin and muscle fibers, as well as intestinal and bronchial motility [15,64,65,66,67,68]. It also plays a key role in pathological processes like pain, inflammation, and cancer [69,70,71]. Minor pCBs, such as CBG, CBC, THCV, and cannabigerolic acid (CBGA), exert their anti-inflammatory effect in human keratinocytes via the molecular deregulation of endocannabinoid (ECB) signaling and the mitogen-activated protein kinase (MAPK) pathway [29].
Cannabinoids’ beneficial or harmful effects are determined by how they act on the CB receptors and by their affinity for a particular receptor. The cannabinoids can also interact with a multitude of other receptors, which explains the variety of effects encountered in these compounds [20]. Being fully represented in the skin, the ECS contributes significantly to the body’s homeostasis [59]. By controlling, among other things, cell growth, differentiation, and survival; immune and inflammatory responses; and sensory phenomena, the ECS is also involved in the physiology and pathology of skin functions [72].
The skin is an accessible organ for the non-invasive or minimally invasive administration of medications [73]. However, the variability in skin permeability remains a challenge in optimizing transdermal drug delivery that targets the epidermis, dermis, deeper tissues, and systemic circulation [74]. Hence, the skin can be approached from both points of view as a therapeutic target and as a route of systemic administration.
The skin has the advantage of being an easy and convenient route of administration for a wide range of active ingredients, including natural or synthetic cannabinoids. Various techniques for the enhancement of skin permeabilization are available for the improvement of bioavailability and the efficacy of therapeutic cannabinoids, such as the use of organosilane particles as transdermal delivery vehicles [75], oleic acid and ethanol as good chemical enhancers, ethosomes and nanocryogels as controlled release strategies, and microneedle arrays for both the topical and transdermal delivery of incorporated cannabinoids [76].
Complementary and alternative medicine (CM and CAM) therapies have an increasing presence in dermatology [77], gaining popularity among patients in recent years. Natural remedies are seen as safer than conventional medications, with few if any notable adverse effects. However, dermatologists are wary of prescribing cannabinoid-based remedies due to the lack of studies regarding the formulation and standardization of extracts and safety profiles [78]. There are a few reported clinical cases of allergies related to topical cannabis contact, such as pruritus, urticaria, or angioedema, which were confirmed via specific allergy tests [79]. Similar o many other natural products or extracts, cannabis-based medicines have the potential to cause skin allergies in some individuals. However, thanks to advances in formulation techniques, exposure to some cannabis plant constituents may be significantly reduced.
The current review aims to bridge the gap between cannabinoids as traditional healing herbal extracts and the current science regarding optimal usage, including the formulation, route of administration, dosage, and frequency of use of these compounds in dermatological disorders and diseases.
2. The Topical versus the Transdermal Route of Administration for Natural Cannabinoids
2.1. The Skin as a Potential Therapeutic Target
Skin diseases like atopic dermatitis (AD), allergic contact dermatitis (ACD), asteatotic eczema (AE), psoriasis, pruritus, varicose ulcers, wounds, acne, and seborrhea are challenging to treat, have a significant impact on patients’ quality of life, and assume high costs in the long term throughout the entire life. With annual costs of over EUR 30 billion per year in Europe and USD 5.3 billion in the USA and treatments that are trying to modulate the microbiome or innate immune response, targeting itching or inhibiting Janus kinases, AD affects up to 20% of children and up to 10% of adults worldwide [80]. This pathology significantly reduces the quality of life, and current treatments have limited effectiveness and high costs [80]. Between 44 and 76 million of 217 million EU employees suffer from an allergic disease of the airways or skin in the European Union (EU). Up to 90% of these people are untreated or undertreated [81]. With topical corticosteroids as the primary treatment, ACD is currently a pathology without a permanent cure; the only way to improve the ailment is to eliminate the allergen as much as possible [82]. Psoriasis affects an estimated 60 million people worldwide, with country-specific prevalence being more common in high-income areas and among the elderly [35]. Psoriasis, with annual costs of over USD 11.5 billion in 2008 alone in the United States, might impose a significant economic burden on taxpayers, patients, and society in general due to its high prevalence and significant direct and indirect costs [83]. Psoriasis remains a challenge for medical systems worldwide, with expensive treatments that have short-term effects or a high number of side effects [84], and these are only a few examples of skin conditions that are a challenge for medical systems worldwide. The skin, as a therapeutic target for pCBs, represents a vast research area that has not received enough attention.
2.1.1. The Skin Endocannabinoid System
The skin is the largest organ of the human body, extending over an area of 1.5 to 2 m2 in adults [85]. After the liver, the skin may be considered the largest organ of the human body that metabolizes drugs and xenobiotics [86]. The skin has a plethora of functions, such as body protection via the cutaneous barrier function, vitamin D synthesis, thermoregulation, and immune defense. Skin disorders affect these physiological mechanisms, oftentimes with systemic effects. It was demonstrated that skin models are valuable tools for organ-specific safety assessment concerning xenobiotic metabolism [87]. Hence, many synthetic or/and plants-based natural products may be applied to the skin for either local or systemic effects [85] with the advantage of avoiding first-pass metabolism and improving bioavailability [7]. Thus, topically applied formulations may target different skin compartments, such as the viable epidermis, known as the key target region for the majority of topical products [85]; dermis; hypodermis; or skin appendages, such as pilosebaceous units, sweat glands, and nails, while transdermal drug delivery (TDD) targets systemic circulation [85]. Hence, drug delivery into and across the skin remains challenging [88].
The skin functions as an interactive network, consisting of physical/mechanical, chemical, microbiological, and immune barriers [89]. The main components of the mechanical barrier in the skin are the stratum corneum, the tight junctions in the interfollicular epidermis, and pilosebaceous units [88]. Pilosebaceous units are important routes for both localized and systemic drug delivery, especially for topical liposomes [90] that are known to be appropriate as drug delivery systems even for phytocannabinoids [7]. Moreover, endocannabinoids are known to exert an important regulatory role in the biology of skin appendages [31]. CBD, a skin-permeable phytocannabinoid that has become popular in therapeutic skin products, has been discovered to have a permeability that depends on the vehicle solutions and pH of the environment, which affects its skin permeation rate and skin retention. This knowledge was obtained from in vitro research employing assays that are based on artificial membranes. [91]. Thus, CBD may have a suitable skin permeability for the development of dermatological or cosmetic applications [91]. CBD is known as a highly effective sebostatic agent that exerts its anti-inflammatory effect on human skin sebocytes [92] and on human cultured sebocytes [30]. CBD, CBN, and THC were bioaccumulated and detected using liquid chromatography–tandem mass spectrometry (LC-MS/MS) in a keratinized matrix of hair and nail samples obtained by noninvasive collection from Cannabis users, with significantly higher concentrations in fingernails than in toenails and hair [93]. CBD is also known to emphasize antioxidant potential by increasing the expression of the main endogenous antioxidant system, superoxide dismutase (SOD), and glutathione peroxidase (GPx) [27]. Thus, CBD is one of the most effective protectants against UVA radiation [26], protecting keratinocytes against the effects of UVA/UVB radiation by reducing lipid peroxidation products and counteracting oxidative stress [46]. CBD is also involved in wound healing [32]. Two endocannabinoids, anandamide and 2-arachidonoylglycerol, suppressed proliferation, induced apoptosis, deregulated the expression of cytoskeletal proteins (i.e., cytokeratins), upregulated lipid synthesis, and selectively activated the mitogen-activated protein kinase (MAPK) signaling pathway in human eccrine-sweat-gland-derived immortalized NCL-SG3 model cells; the overexpression of endocannabinoids levels helped manage certain sweat-gland-derived disorders, including tumors, and this was characterized by increased proliferative rates [31]. Generalized and focal hyperhidrosis or excessive sweating affects the quality of life for almost 5% of the world’s population [94]. Excessive sweating may be improved immediately after using CBD [94] and by drop administration and the inhalation of THC, which reduced the volume of sweat [95]. At the dermal level, Gerasymchuk et al. demonstrated that several pCBs exert rejuvenation efficacy and prevent cellular senescence in human dermal fibroblasts, with applications in cosmetics [32].
The human endocannabinoid system consists of the two cannabinoid receptors CB1 and CB2; several endogenous ligands such as 2-arachidonoylglycerol (2-AG) and N-arachidonoylethanolamine (anandamide) (AEA); and enzymes involved in the synthesis, transport, and degradation of endocannabinoids [2]. Both CB1 and CB2 skin receptors, which are present in epidermal keratinocytes, cutaneous nerve fibers, dermal cells, melanocytes, eccrine sweat glands, and hair follicles [96,97,98], can be modulated by endocannabinoids, with the most studied being N-arachidonoyl ethanolamide (AEA), 2-arachidonoyl glycerol (2-AG), N-palmitoyl ethanolamide (PEA), N-alpha-linolenoyl ethanolamide (ALEA), N-linoleoyl ethanolamide (LEA), N-oleoyl ethanolamide (OEA), N-stearoyl ethanolamide (SEA), N-eicosapentaenoyl ethanolamide (EPEA), and N-docosahexaenoyl ethanolamide (DHEA) [99,100,101,102,103]. However, endocannabinoids also bind to other receptors found in various skin cells, such as transient receptor potential (TRP) channels, which are involved in a variety of processes, including the development and preservation of the skin barrier, cell growth stimulation, and cell differentiation. They also play a significant role in immunological and inflammatory processes [72]. Endocannabinoids interact with PPARs via direct or indirect signaling pathways. Biological processes like neuroprotection, anti-inflammation, and analgesic action are partially mediated by PPAR activation [59]. ECS’s involvement and role in cutaneous biology is currently an intensely debated research topic both in clinical and preclinical studies [104,105]. Topical applications of cannabinoids provide therapeutic benefits for the patient in multiple pathologies like psoriasis, eczema, and atopic dermatitis, as shown in Figure 1 [59]. These advantages are obtained due to the remarkable role of the ECS in improving dermatological conditions symptoms such as itching, inflammation, and pain.
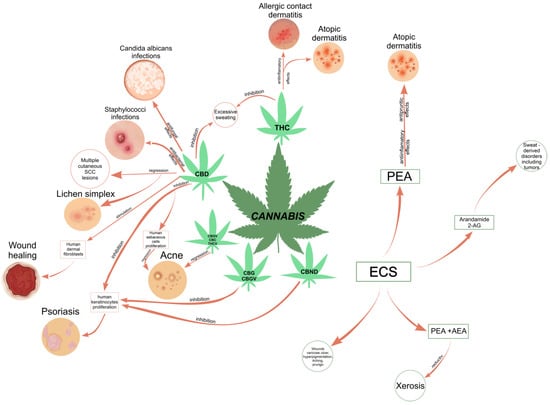
Figure 1.
Correlation diagram between the most common phytocannabinoids and the skin conditions they could treat [30,32,51,59,93,101,106,107,108,109]. Abbreviations: THC, tetrahydrocannabinol; Δ8-tetrahydrocannabinol; Δ9-THC, Δ9-tetrahydrocannabinol; CBD, cannabidiol; CBG, cannabigerol; CBN, cannabinol; CBND, cannabinodiol; ECS, endocannabinoid system; PEA, N-palmitoyl ethanolamide; AEA, N-arachidonoylethanolamine (anandamide); SCC, squamous cell carcinoma.
2.1.2. Skin Disorders Addressed by Cannabis-Based Medicines
The most common skin conditions that currently lack effective treatments that are safe and simple to administer and can significantly improve the patient’s quality of life are psoriasis, atopic dermatitis (AD), allergic contact dermatitis (ACD), asteatotic eczema (AE), acne, and seborrhea. These diseases and current treatments are detailed in Table 1. Psoriasis is a chronic autoimmune inflammatory skin disease characterized by skin lesions that are the result of a rapid turnover of epidermal keratinocyte proliferation, accompanied by the infiltration and increased expression of proinflammatory mediators in the skin [7,110]. Psoriasis incidence has a bimodal pattern, with one peak in childhood and a second peak in adulthood. It tends to persist throughout life, fluctuating in extent and severity [110]. The pathogenesis of psoriasis is complex and involves an association between genetic and environmental factors (trauma, infections, psychological stress, and drugs) [110]. The condition develops due to pathological interactions between skin immune cells and epidermal keratinocytes, leading to increased inflammation (due to the production of cytokines such as IL-17, IL-22, and TNF-α) and the excessive proliferation of keratinocytes, causing the characteristic alteration of skin called psoriatic plaque [7,57,105,110]. Cutaneous ECS inhibits cell growth and angiogenesis, leading to skin cell apoptosis, so CNBs have shown promising results in helping to treat psoriasis [7]. Clinically, psoriasis is characterized by erythematous, well-defined, raised plaques that are covered by pluristratified pearly white scales that are easily removable. The lesions are symmetrical and can affect any region, but they are more common in the extension areas—elbows, knees, lumbosacral, and pretibial regions. Psoriasis can also affect other major folds of the body and the genitals. Symptomatically, itching is mostly mild but can be severe in some patients, leading to excoriations, eczematization, and lichenification. Painful fissures may occur. After the remission of psoriasis plaques, post-inflammatory hypopigmentation or hyperpigmentation can be observed, and it is expected that these will fade in a few months [7,57,110].
In psoriasis, cannabinoids may help reduce keratinocyte proliferation. Wilkinson et al. hypothesized that the primary mechanism of the THC-mediated inhibition of keratinocyte proliferation is proliferative peroxisome-activated receptor gamma (PPARγ) [106]. A secondary inhibitory mechanism occurs via the downregulation of keratin K6 and K16 expression driven by CB1 activation [107]. Cannabinoids can prevent the release of inflammatory cytokines present in the pathogenesis of psoriasis [7]. Moreover, a synthetic cannabinoid, JWH-133, inhibits some inflammatory cytokines and angiogenic factors involved in psoriasis (inducible factor-1α (HIF-1α), vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), and angiopoietin-2) in vivo and in vitro [111]. The complex action of cannabinoids is thus of great potential in psoriasis, which is justified further by their lack of the typical side effects of steroids and calcineurin inhibitors and is the most common current topical approach in this pathology.

Table 1.
The most common skin conditions for which ECS modulation could be an effective therapeutic option.
Table 1.
The most common skin conditions for which ECS modulation could be an effective therapeutic option.
| Affection (Estimative Costs around the Current Course of Therapy) | Current Drug Therapies | Drawbacks/ Most Significant Adverse Effects | Reference | |
|---|---|---|---|---|
| Psoriasis (between USD 23.9 and USD 35.4 billion annually in the US | topical agents | vitamin D analogues corticosteroids | poor therapy responses | [35,112] |
| phototherapy | NB-UVB PUVA | major risks of skin cancer | ||
| standard systemic | acitretin | dry skin, hair loss, hyperlipidemia, hepatotoxicity | ||
| ciclosporin | hypertension, irreversible renal toxicity | |||
| methotrexate | bone marrow suppression, liver fibrosis, teratogenicity, hepatitis | |||
| biologic agents | TNF IL-17 L-23 inhibitors | individualized therapy regimen | ||
| small molecule inhibitors | apremilast dimethyl fumarate | used only in studies | ||
| Atopic dermatitis (USD 3.8 billion annually in the US) | topical moisturizers | glycerin, alpha hydroxy acids, hyaluronic acid, sorbitol, urea, lanolin, mineral oil, olive oil, silicone, collagen, elastin, glyceryl stearate, shea acid, stearic acid | a large number of studies lacking any significant relevance regarding the efficacy | [113,114] |
| topical corticosteroids | clobetasol, fluocinonide, betamethasone, triamcinolone, fluticasone budesonide, hydrocortisone | atrophy, striae, rosacea, perioral dermatitis, acne, purpura, hypertrichosis, alteration of the skin’s pigment, sluggish wound healing, worsening of skin infections | [115] | |
| topical calcineurin inhibitors | tacrolimus pimecrolimus | skin burning, increased bone growth and decreased bone density, inhibition of the hypothalamic-pituitary-adrenal axis in children | [116,117,118] | |
| phototherapy | UVB | xerosis, erythema, actinic keratosis, skin damage tenderness, possible carcinogenic risk | [118,119] | |
| systemic immunotherapy | cyclosporine azathioprine | headache, serum lipid TSH elevation, teratogenicity, liver dysfunction, leukopenia, gastric ulcer, osteoporosis, glaucoma | [120] | |
| Allergic contact dermatitis (USD 5.3 billion in the US in 2015) | systemic corticosteroids | clobetasol, betamethasone, diflorasone, fluocinonide, halcinonide, mometasone furoate, fluocinolone acetonide, desoximetasone, triamcinolone acetonide, alclometasone dipropionate, hydrocortisone, dexamethasone, prednisolone, methylprednisolone | atrophy, infections, hypertrichosis, allergic reactions, problems with systemic absorption | [36,37,121] |
| calcineurin antagonists | cyclosporine | risk of malignity | [36,38] | |
| ultraviolet therapy | PUVA UVB | lentigines (freckling), photoaging, precancerous lesions, actinic keratoses, skin cancer, hyperpigmentation, redness, dryness, pruritus, herpes simplex virus reactivation, polymorphic light eruption | [36,39] | |
| Asteatotic eczema (USD 5.3 billion annually) | topical steroid | hydrocortisone, glucocorticoid, nonfluorinated steroids (hydrocortisone valerate, hydrocortisone probutate, mometasone furoate), fluorinated steroids (dexamethasone, triamcinolone, fluocortolone, flumethasone, betamethasone) | skin atrophy, striae atrophicans, xeroderma, delayed wound repair, capillary telangiectasia, rosacea-like dermatitis, steroid purpura, steroid acne milium, pigmentation disorder, acne uncontrollable, hyper-pilosis | [36,40,41] |
| phototherapy | UVA (UVA-1) UVB PUVA | suppressing immune system | [40] | |
| Acne (acne is thought to cost the economy USD 3 billion annually) | topical retinoids | adapalene, isotretinoin, motretinide, retinoyl-β-glucuronide, tazarotene, tretinoin | used in various combinations, all of these topical treatments disrupt the skin’s natural barrier, requiring frequent treatment changes | [42,43,44] |
| topical antibiotics | clindamycin, erythromycin | disruption of the skin’s natural barrier | ||
| diverse topical agents | azelaic acid, benzoyl peroxide, chemical peels, corticosteroids, dapsone, hydrogen peroxide, niacinamide, salicylic acid, sodium sulfacetamide, sulfur triclosan | specific adverse events | ||
| systemic retinoids | isotretinoin | hematological/lymphatic disorders, immune system disorders, metabolic and nutritional disorders | ||
| systemic antibiotics | azithromycin, clindamycin, co-trimoxazole, doxycycline, erythromycin, levofloxacin, minocycline, roxithromycin | specific adverse events | ||
| other systemic agents | hormones, clofazimine, corticosteroids, ibuprofen, zinc sulfate | specific adverse events | ||
| Seborrhea (in 2021, the value of the global seborrheic dermatitis market was estimated to be USD 2.2 billion) | antifungals | itraconazole, terbinafine, fluconazole, ketoconazole, pramiconazole | itching, burning sensation, dryness | [108,109,122] |
| corticosteroids | prednisone | skin atrophy, telangiectasias, folliculitis, hypertrichosis, hypopigmentation | [109] | |
| calcineurin inhibitors | pimecrolimus | skin malignancy lymphoma | [123] | |
| phototherapy | UVB PUVA red and blue LED light | burning itching sensation genital tumor | [123] | |
Abbreviations: NB-UVB, narrowband ultraviolet B radiation; PUVA, psoralen ultraviolet A radiation; TNF, tumor necrosis factor; IL, interleukin; AD, atopic dermatitis; ACD, allergic contact dermatitis; UVB, ultraviolet B radiation.
Atopic dermatitis (AD) is a chronic, relapsing, pruritic condition that is often associated with allergic rhinitis and/or asthma. Infants and children are most often affected, with 85% of cases appearing in the first year of life and 95% of cases appearing by 5 years [110]. The pathogenesis of AD is not fully understood, but it is believed that genetic and environmental factors influencing epidermal barrier function and adaptive immune function are involved [7,57,110]. Genetic mutations of various genes/proteins are investigated, such as filaggrin mutations, which are present in 50% of cases, causing a defective skin barrier and increased transepidermal water loss–dry skin. Deficiencies in ceramides, antimicrobial peptides, and altered sensation to itch stimuli are also documented. AD involves a type 2 cytokine inflammatory response with the activation of IL-4 and IL-13 [57,110]. Actual treatments for AD are topical moisturizers, corticosteroids, calcineurin inhibitor, phototherapy, and systemic immunotherapy [113,114,115,116,117,118,120]. All of these treatments have limited short-term efficacy, significant or even limiting side effects when administered for long periods of time, or are prohibitively expensive [113,114,115,116,117,118,120].
AD can be divided into three stages: infantile AD, occurring from 2 months to 2 years of age; childhood AD, occurring from 2 to 10 years; and adolescent/adult AD. In all stages, pruritus (itching) is a hallmark of atopic dermatitis, often preceding the appearance of lesions. Clinical features include intense itching, scratching and eczematous lesions that can be acute (erythema, vesicles, bullae, weeping, and crusting), subacute (scaly plaques, papules, round erosions, and crusts) or chronic (lichenification, scaling, and hyper- and hypopigmentation). Acute inflammation with the involvement of the cheeks, scalp, and extensor areas of the extremities predominates in infants, and chronic inflammation with lichenification is preferentially located in flexural areas in children and adults. Follicular patterns of atopic dermatitis (follicular eczema) are more common in persons with darker skin phototypes. The condition has a severe impact on the quality of life due to disturbed sleep, poor performance at school or work, and unsightliness [110].
Despite the complexity of the underlying mechanisms, there are intriguing reports that CB receptor agonists have improved AD symptoms. Cannabinoids have demonstrated anti-inflammatory and antipruritic properties, highlighting a potential therapeutic role [7]. The mechanisms by which cannabinoids decrease inflammation and pruritus are diverse and involve CB1/CB2 receptors, chemokines, and an interaction between the endocannabinoid system and the immune system [7,124]. Nam et al. showed that a CB1 agonist ameliorates AD in mouse models possibly by decreasing mast cell proliferation [121]. Clinical trials have also shown promising results for AD [122]. In a study with pediatric and adult subjects, a cream containing palmitoylethanolamide (PEA) significantly increased the mean time to the next eruption [123]. Similarly, in a pilot study, the use of a topical cannabinoid emulsion resulted in clinical resolution and prevented the relapse of mild atopic dermatitis in 80% of patients [124]. In another study, a cream containing PEA improved itching severity and sleep quality by an average of 60% among subjects [125]. With both anti-pruritic and anti-inflammatory effects, this PEA product is an alternative to traditional steroids, anti-histamines, and calcineurin inhibitors, and it has a superior safety profile in addition to its good efficacy.
Allergic contact dermatitis (ACD) is a pruritic, eczematous reaction and one of the leading causes of occupational diseases [110]. ACD represents a delayed-type (type IV) hypersensitivity reaction that occurs when allergens activate antigen-specific T cells in a sensitized individual. ACD typically requires repeat exposures before an allergic response is noted and can occur 24–48 h after exposure to the offending agent. This exposure induces a specific immune response, predominantly involving T cells and inflammatory cytokines such as interleukin IL-6 and IL-8 and tumor necrosis factor-alpha (TNF-α). There is also an endogenous predisposition that relates to the malfunctioning of epidermal proteins such as filaggrin, ceramides, claudins, antimicrobial factors, and proteases [110]. Clinical patterns will vary based on the actual allergen involved, but the typical appearance is often a well-demarcated pruritic eczematous eruption, which may be acute (blistering, weeping, and/or edema) or chronic (lichenified or scaly plaques). This reaction is typically localized to the area of skin that comes into contact with the allergen. ACD may coexist with irritant contact dermatitis, contact urticaria, and various forms of endogenous eczema, which can complicate establishing an accurate diagnosis [7,110,125]. There are numerous potential contact allergens, but the most common are metals (e.g., nickel, cobalt, and chromates), fragrance, preservatives (e.g., methylisothiazolinone), formaldehyde and formaldehyde releasers (e.g., quaternium-15), paint p-phenylenediamine, topical antibiotics (e.g., neomycin and bacitracin), and rubber accelerators [110].
Treatment for ACD consists of avoiding trigger factors and using topical corticosteroids, calcineurin inhibitors (tacrolimus and pimecrolimus), and systemic immunosuppressive agents for severe cases [110]. Regarding the therapeutic value of using CNBs in the treatment of ACD, human studies are still lacking, but studies in mice have revealed the involvement of CBRs, especially CB2R, in the inflammatory response of ACD, and possible therapies involving it have been proposed targets [57,126].
As with AD, studies have shown that phytocannabinoids are effective in the treatment of ACD. In a rodent study, the topical application of THC reduced inflammation in ACD by inhibiting keratinocyte-derived proinflammatory mediators (CCL8 and CXCL10) independent of CB1/CB2 receptor activation or inhibition [124]. Kim et al. designed a structurally similar compound to anandamides, which improved epidermal barrier function and suppressed TH2 cytokine expression in mice, also activating CB1 receptors [127]. CBD showed anti-inflammatory properties in an ACD experimental model in a different study by Petrosino et al. [128].
Asteatotic eczema (AE), also known as craquelé eczema, winter itch, or xerotic eczema, is a common type of pruritic dermatitis characterized by dry, scaly, cracked, and itchy skin [110]. In terms of pathogenesis, the xerosis of aged skin is not caused by deficient sebum production but by a complex dysfunction of the stratum corneum. A decrease in intercellular lipids is present with a deficiency of all key lipids in the stratum corneum and an altered ratio of esterified fatty acids to ceramide, plus the persistence of corneodesmosomes and the premature expression of involucrin with cornified coat formation, resulting in marked corneocyte retention [110,126]. As a result, the stratum corneum dehydrates, loses its flexibility, and forms small cracks, which make the surface of the skin dull, rough, and scaly. Mild xerosis is asymptomatic, but if it is more pronounced, the skin transmits unpleasant sensations such as itching and stinging. Inflammation is intensified by the release of pro-inflammatory cytokines that are secondary to barrier disruption, mechanical factors (scratching and friction), and the application of irritants or sensitizers in topical preparations or skin care products. Prevention is key in avoiding or controlling itching and irritation, so patients are advised to make several lifestyle changes, such as avoiding harsh cleansers and opting for lukewarm showers, to prevent exacerbation of this uncomfortable disease [57,110,126]. Clinical xerosis usually has a slow and indolent course that progresses over the years. It is characterized by dry, dull, and rough skin with fine bran-like scales that flake off easily. In contrast, eczema craquelé usually has a more acute or subacute onset. It is characterized by redness and tight-appearing polygonal cracked skin with fine, interconnected horizontal and vertical fissures. This forms an irregular network of fissures and cracks, similarly to broken window glass. It is most severe on the distal legs and occasionally the arms and trunk. The face, scalp, groin, and axillae are usually spared from the fine, dry scales of the condition. Crusting, oozing, and bleeding fissures may be observed in advanced cases [57,110,126].
Treatment for AE usually involves the application of emollients containing urea and lactic acid, and severe cases usually require topical corticosteroid treatment [110]. Endocannabinoids such as PEA and AEA exist in high concentrations in the granulosa layer of the skin, and low levels of these compounds have been linked to xerosis. Several studies have provided evidence that the modulation of the cutaneous ECS can lead to increased lipid synthesis in that skin layer, providing relief in eczematous conditions [126,129].
Acne and seborrhea are the most common dermatological conditions, and they are usually self-limiting and characterized by a very high production of sebum (lipids) and chronic inflammation of the pilosebaceous unit. It is especially common in teenagers, but it also occurs in children and adults, and its psychological impact can be profound [110]. The pathogenesis involves multiple factors, including (i) increased sebum production, (ii) follicular hyper-keratinization and corneocyte hyper-cohesiveness, (iii) the proliferation of the bacterium Cutibacterium acnes (formerly known as Propionibacterium acnes), and (iv) inflammation that is neutrophil driven in early lesions and Th1/Th17 driven in established lesions. Acne and seborrhea typically begin at puberty as a result of the androgen stimulation of the pilosebaceous unit and changes during keratinization at the follicular orifice [57,110,126]. Acne is characterized by a wide spectrum of lesions, such as open and closed comedones (blackheads and whiteheads); inflamed papules and pustules; nodules and pseudocysts in severe acne; and post-inflammatory erythematous or pigmented macules. Acne can be classified as mild, moderate, or severe, but this designation may vary between clinicians as there is no single grading system that has been adopted by all. Acne vulgaris is most commonly found on the areas of skin with the greatest density of sebaceous follicles, such as the face, back, and upper chest. While in a benign condition, acne can lead to permanent scarring and significant psychosocial distress. Therefore, the initiation of treatment in the earliest stages is preferable [110]. Acne treatments are aimed at targeting as many pathogenic factors as possible to control the disease. Depending on the stage of acne, the therapeutic management involves the use of the following: (i) mild acne: benzoyl peroxide, topical retinoid (tretinoin, tazarotene, adapalene, and trifarotene), and topical combination therapy (benzoyl peroxide plus a topical antibiotic, a topical retinoid, or both); (ii) moderate acne: topical combination therapy, oral antibiotic (doxycycline, minocycline, and tetracycline) plus topical retinoid and oral antibiotic plus topical retinoid plus benzoyl peroxide; (iii) severe acne: oral antibiotic plus topical combination therapy, oral isotretinoin, and hormonal therapies (female patients)– spironolactone and oral contraceptives. Cannabidiol has been suggested as a promising therapeutic agent for the treatment of acne vulgaris because it normalizes the lipogenesis of sebocyte cells, decreases the proliferation of these cells, and decreases the levels of pro-inflammatory cytokines [105,110,129].
Endocannabinoids have shown promising results for the treatment of acne when CB2 expression was found in human SZ95 sebocytes [130]. The inhibition of CB2 receptors resulted in the suppression of basal lipid production, suggesting that CB2 antagonists may be helpful in the treatment of skin conditions characterized by the dysfunction of the sebaceous gland [100]. In a single-blind study involving 11 patients, Ali et al. investigated the use of a cream containing 3% cannabis seed extracts for acne. Participants used the cream twice daily for 12 weeks, and their sebum production significantly improved [131]. Cannabidiol inhibits sebocyte proliferation by activating TRPV4 according to Olah et al. In cultured human sebocytes, it also inhibits the lipogenic effects of arachidonic acid, linoleic acid, and testosterone [101]. Thus, with future studies to be conducted, cannabinoids could be included in the daily management of this pathology, where the currently available options are far from optimal efficacy and safety.
Wounds, varicose ulcers, hair loss, hyperpigmentation, itching, prurigo, and lichen simplex are a few other skin conditions that have been linked to disruptions of ECS, as per recent studies [97,98,106]. The range of dermatological conditions in which ECS becomes a therapeutic target is widened by the existence of specific cannabinoid receptors at hair follicles and sweat glands level [59]. The mechanisms by which cannabinoids ameliorate inflammation and pruritus are various and involve, in addition to CB1/CB2 receptors, chemokines and interactions between the endocannabinoid system and the immune system [132].
It has been shown in several studies that by inhibiting TRPV1, anandamide had antipruritic effects [133,134]. The cutaneous itch-inducing TRPV1 ion channel is primarily found in the nociceptive neurons of the peripheral nervous system. Twenty-two patients with pruritus, prurigo, and lichen simplex were treated by Stander et al. using PEA incorporated into an emollient lotion. PEA, which inhibits fatty acid amide hydrolase enzyme (FAAH) and activates anandamide at the cannabinoid receptor, reduced itching in these patients by 86.4% [135]. The treatment of uremic pruritus with cannabinoids has also been shown to be successful. In a 3-week study, Szepietowski et al. investigated the efficacy of a cream containing lipids and endogenous cannabinoids in 21 patients with uremic pruritus. According to their findings, 81% of patients had completely reduced xerosis, and 38% of patients had completely resolved itching [136].
Wound healing is a difficult process that involves three overlapping phases: inflammation, proliferation, and tissue remodeling [137,138]. Endocannabinoid system signaling may affect the intricate process of wound healing because it regulates fibroblast function, epithelial differentiation and proliferation, and skin inflammation. The involvement of CB1 and CB2 receptors during the wound-healing process in various immune cells and fibroblasts was demonstrated using murine models [139,140,141]. Different cannabinoid analogs produced a wound-healing response in these models, which may have been mediated by the activation of CB1 and/or CB2 receptors, increasing anti-inflammatory factor synthesis, the indirect activation of TRPV1 and epidermal growth factor receptors, and the inhibition of the FAAH enzyme [140,142]. There is not much research supporting the use of phytocannabinoids, specifically CBD, for the treatment of wounds. Three patients with epidermolysis bullosa, a rare skin condition marked by pain and blisters, had faster wound healing, fewer blisters, and pain relief with respect to self-reported topical cannabidiol use [60,143]. Although there is a lack of clinical evidence, preclinical models indicate a promising future not only due to their efficacy but also based on its excellent safety profile compared to many of the classical options.
The effects of CBD and Cannabis sativa extract (CSE, standardized to 5% CBD) on human keratinocytes (HaCaT cells) and human dermal fibroblast (HDF) cells were examined in a study by Sangiovanni et al. [144]. The TNF-α treatment of human keratinocytes increased the expression of 26 genes involved in inflammatory pathways, including chemokines like CXCL8 and CXCL10; interleukins like IL-17C and IL-1B; and VEGF-A. CSE treatment reduced all 26 genes related to inflammation, while CBD alone reduced only 15 genes. TNF-α treatment increased the expression of 16 genes that are essential for wound healing in HDF cells. CBD had no inhibitory effect on genes that are involved in inflammation and matrix remodeling, such as IL-6 and MMP-9, while CSE was once again able to reduce all genes. These findings suggest that the other cannabinoids, flavonoids, and terpenes present in CSE may have a synergistic anti-inflammatory effect that is greater than CBD alone [144].
Varicose ulcers are extremely common skin wounds on the lower limbs that, despite the use of compression therapies, are still challenging to heal. In a recent study, compression bandages were applied in combination with topical cannabis-based medications to the wound bed and surrounding tissues to treat nonresponsive lower limb ulcers in 14 patients with an average age of 75 years [50]. Complete wound closure, defined as fully epithelialized, was reached in 79% of patients, and 81% of wounds healed in a median time of 34 days. The remaining patients had promising healing trends but were unable to be followed up on. The rapid wound closure of nonhealing venous foreleg ulcers in elderly and highly complex patients suggests that topical cannabis-based medications may be useful therapeutic approaches when combined with compression therapy [61]. The applicability could also be extended to the management of other types of wounds.
2.2. The Skin as a Potential Route for Systemic Administration
The skin, which is the largest organ in the human body and serves as a barrier between the body and the outside world as well as an immunological function, is made up of three layers, the dermis, the epidermis, and the stratum corneum (SC) [145,146,147,148], as shown in Figure 2 and Figure 3.
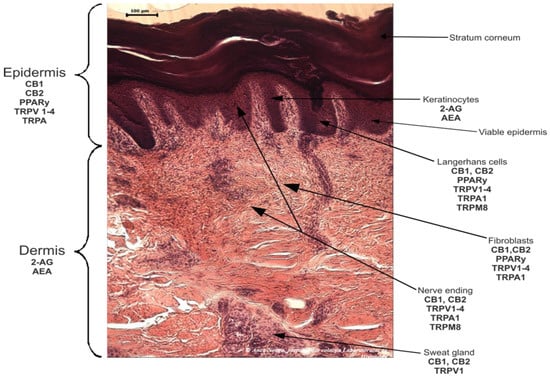
Figure 2.
The molecular members of the skin’s endocannabinoid system (ECS).
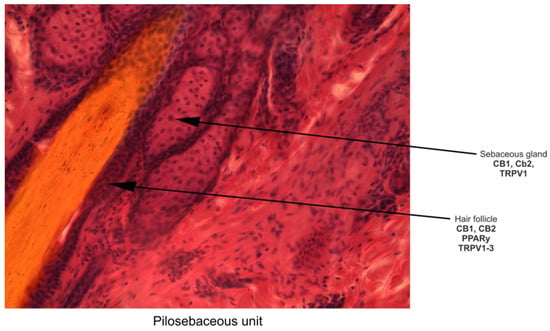
Figure 3.
Particularities of skin ECS at the pilosebaceous unit level.
The skin has unique characteristics: It is permeable relative to the environment and allows the diffusion of air, heat, water, and low molecular weight molecules [145]. Skin permeability can occur in three different ways: the intercellular pathway, which involves the space between corneocytes and keratinocytes; the transcellular pathway, which involves corneocytes and the lipid matrix around them; and the appendicular pathway, which involves sweat glands and hair follicles [149]. Because of this, transdermal application can be used as an alternative method of drug administration. This is because it is simple to use and because it is administered directly into the systemic circulation, avoiding the first hepatic passage and the potential appearance of unwanted metabolites; moreover, the necessary dose and side effects can be significantly reduced [73,150,151].
The transdermal administration of cannabinoids avoids the first-pass metabolism that occurs in the liver, but because they are extremely hydrophobic, they have a limited diffusion across the aqueous layers of the skin [152]. From a physicochemical perspective, molecules with a low weight (below 500 g/mol), a melting point of less than 250 °C, and high potency (less than 10 mg/day) are suitable for transdermal administration. Because transdermal administration necessitates passing through the hydrophobic/lipophilic SC, absorption in the deep aqueous layers, and then passage into the systemic circulation, these substances also need to have a moderate lipophilicity/hydrophilicity balance (logP = 1–5) [73,150,153]. Because the molecular weight of cannabinoids is not what we want, nor is the ratio of lipophilicity/hydrophilicity, they have a log P between 5 and 7 (as seen in Table 2) and low solubility in water; their transdermal administration represents a challenge. These difficulties not only led to the use of permeability enhancers such as oleic acid and ethanol but also techniques that modify the characteristics of the molecule by using microemulsions, physical amplifiers (microneedles and electroporation), iontophoresis, ultrasound, magnetophoresis, encapsulation in micro-/nanogels, nanoparticles, and nanocarriers [25,73,76].
Table 2.
Classification of the most important phytocannabinoids by their lipophilic nature.
2.2.1. Why Transdermal Administration of Cannabinoids Could Be the Solution?
Modern medicine is constantly looking for therapeutic methods that bring definite improvements in the clinical condition of patients. At the same time, researchers are looking for new drugs that have a high degree of safety when administered and, last but not least, can cover a wide range of ailments.
Therefore, cannabinoids are a class of compounds that seem to satisfy these needs via the multiple proven or still researched therapeutic effects, such as the following: analgesic, anti-inflammatory, antioxidant, antibacterial, and antiemetic [45,62,159,160,161]. Cannabinoids have sparked the interest of scientists due to their high therapeutic potential. For this reason, pharmacological studies address subjects that debate and analyze the methods of the administration of cannabinoids to improve their bioavailability, ease of administration, and reduction in adverse reactions. For example, the most intensively analyzed route of administration is the oral one. Additionally, recent studies have highlighted that cannabinoids have low bioavailability following oral administration. Some of the reported causes are as follows: (1) the high lipophilicity of these compounds such that low solubility in water that limits their absorption, (2) hepatic first-pass metabolism, (3) rapid metabolism, (4) irregular pharmacokinetics, (5) their instability in the presence of gastric pH, and (6) the influence of temperature [76,162,163,164]. Considering the above-mentioned reasons, it is expected that researchers will explore other routes of administration in an attempt to minimize these inconveniences. Therefore, transdermal formulations come to the aid of scientists. In other words, theoretically, problems arising from the oral administration of cannabinoids can be solved by using the skin as a way of entering the body when the pathology or symptom being treated allows it. Some disadvantages of cannabinoid oral administration are detailed in the following lines.
The effect of the first hepatic passage is manifested by the biotransformation of the drug before it enters systemic circulation. Both endogenous and exogenous cannabinoids undergo hepatic metabolism after oral administration, a fact that considerably influences the bioavailability of the drug. Specifically, cannabinoids are substrates of the CYP enzyme family [165]. For example, dronabinol (Marinol), a synthetic delta-9-THC for oral use, is primarily metabolized by hydroxylation via multiple CYPs. Both active and inactive metabolites result from this reaction [166]. An in vivo study on patients treated with CBD identified the presence of 33 different metabolites in the patients’ urine using spectrometric methods. Thus, due to the intense metabolism undergone by CBD, the study suggests that this natural compound could provide valuable information about the mechanism of several types of biotransformation [167].
What is interesting is the fact that the metabolism of cannabidiol occurs primarily due to hydroxylation, which is catalyzed by CYP2C19 and CYP3A4 enzymes [168]. In addition, CBD is a potent inhibitor of these enzymes [169]. This information is significant in the context of the simultaneous administration of the Epidiolex product (synthetic cannabidiol: GW Pharmaceuticals) as an adjuvant in patients with refractory epilepsy treated with clobazam, which is another substrate for these enzymes that belong to the CYP family. Consequently, the plasma level of the active metabolite of clobazam (norclobazam) requires frequent monitoring in patients following this treatment simultaneously with CBD [169].
Regarding the metabolism of endocannabinoids, studies have shown the existence of some inactive metabolites. In addition, research has focused on inhibiting the degradation of endocannabinoids with pharmacologically valuable results. Therefore, it is interesting to mention FAAH inhibition strategies, with this molecular target becoming extremely attractive for the anxiolytic effects observed in neuropsychiatric diseases and the antinociceptive effect in pain conditions [170]. Thus, FAAH inhibition has been intensively explored in clinical and preclinical studies [171]. For example, modulating the concentration of anandamide by inhibiting FAAH can reduce anxious behavior in rodents with chronic stress [172]. In addition, in a multicenter, double-blind, placebo-controlled study, JNJ-42165279, an FAAH inhibitor, reduced the Liebowitz Social Anxiety Scale (LSAS) by 30% and achieved an improvement in the Clinical Global Impression-Improvement (CGI-I) by the end of 12 weeks of treatment [173]. Therefore, it is easy to understand that the hepatic metabolism of orally administered cannabinoids produces qualitative and quantitative changes in the active substances. Also, the substrate–enzyme interaction increases the risk of drug interactions, to which the risk of toxicity or failed treatment is added.
Also, cannabinoids are molecules with a high degree of lipophilicity and are susceptible to degradation if they are formulated as solutions. They can undergo autoxidation reactions; thus, control over the pharmacokinetics of the administered compound is lost. In addition, exposure to light, herbal cannabis or cannabis resin, or extracts leads to significant losses in phytochemical component levels [174,175].
Their high lipophilic nature poses serious problems in cannabinoid oral administration. It is well documented that the oral bioavailability of CBD and THC is as low as 6% [175]. Also, THC under various oral formulations shows variable absorption. Moreover, THC absorption is slow, irregular, and unpredictable. Pharmacokinetic studies have noted similar oral absorption for both THC and CBD, a fact that requires the formulation of these compounds in oil to counteract the harmful effects on oral bioavailability given the low solubility of cannabinoids in water [25].
On the other hand, the variable pharmacokinetics of cannabinoids is demonstrated by a significantly different metabolic pattern depending on the oral formulation [176]. For example, in a double-blind, randomized, single-center study, nine healthy male volunteers were treated with unheated Cannabis sp. extracts, heated Cannabis sp. extracts, and dronabinol. The results of the study demonstrated the different plasma concentration levels of certain metabolites depending on the form of administration, in addition to the higher bioavailability of the heated extract compared to the unheated extract and synthetic CBD. Specifically, the authors found the highest scores of the average plasma value of the area under the plasma concentration/time curve (AUC) during the first 24 h after drug administration for THC-COOH, which is the inactive metabolite of dronabinol [177].
Consequently, the results of the oral administration of cannabinoids impose pharmacokinetic problems that are difficult to anticipate and require rigorous comparative studies on the medicinal form approached. Also, the variable bioavailability of cannabinoids requires the development of quality-controlled extracts, with a pharmacological profile that allows the administration of correct doses for optimal therapeutic effects.
That is why the transdermal administration of cannabinoids would have some advantages: the possibility to increase the therapeutic dose by avoiding the hepatic first-pass effect; direct application to the affected area, especially in dermatological conditions or the possibility to obtain an analgesic effect; and adverse effect minimization, as seen in Table 3. On the other hand, transdermal preparations allow the use of larger amounts of active substance, with controlled release for a longer period of time [178]. However, there are several difficulties and restrictions with respect to transdermal cannabinoid preparations. The physico-chemical stability of the preparation is a subject that deserves attention in this context.
Table 3.
Advanced formulations designed in order to penetrate the skin or membranes and to produce systemic effects.
2.2.2. The Use of Nanotechnologies for Cannabinoid Transdermal Administration
The field of cannabinoid research is expanding its boundaries more and more. The understanding of the pharmacology of these compounds and the knowledge of their beneficial effects in the treatment of pain, post-chemotherapy emesis, neuropsychiatric conditions, and dermatological conditions, in particular, stimulated researchers to address topics related to optimal formulations. Theoretically, the most promising formulations, which exceed the limitations imposed by the physico-chemical characteristics of cannabinoids, mentioned above are those that allow their administration on the skin [154]. Among these skin administration methods, we focus on those based on nanotechnology, that have, as observed in Figure 4, better penetration through skin layers than conventional formulations.
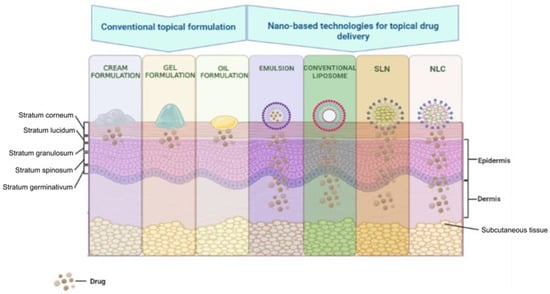
Figure 4.
The passage of substances through the layers of the skin depending on the way they are formulated. SLN, solid lipid nanoparticles; NLC, nanostructured lipid carriers.
These formulations include but are not limited to lipid-based nanocarriers (liposomes, nanostructured lipid carriers, and solid lipid nanoparticles) and vesicular nanocarriers (niosomes, liposomes, transferosomes, ethosomes, and transethosomes) [210].
Due to the high lipophilic nature of cannabinoids, creams are one of their topical administration systems with multiple advantages. The topical application of cream containing CBD and CBD:THC in various proportions allowed a reduction in the symptoms of epidermolysis bullosa simplex and psoriasis [211,212].
However, creams incorporating cannabinoids have their limitations. To increase the stability of active substances, it is necessary to ensure a slightly acidic pH. CBD, for example, degrades at pH = 6 and pH = 7. In addition, increasing the stability of the cannabinoid using alcoholic formulations, as required by the physico-chemical characteristics of these compounds, is not recommended for applications to the skin, especially in dermatological conditions [174,213]. In addition, light and temperature must be controlled so that the product can keep the properties for which it was created [91].
Another delivery system for cannabinoids through the skin, with a series of improved characteristics compared to oils and creams, is to use gels. From a mechanistic point of view, gels allow the deep penetration of cannabinoids through the skin for a systemic effect. It is interesting that researchers have tried to apply different techniques to obtain constant and controllable concentrations of cannabinoids in the plasma. In this sense, in a study on a rat model of arthritis, the gel containing CBD reduced the associated inflammation, limb posture score, and thickening of the synovial membrane in a dose-dependent manner [214].
Advanced research has allowed the improvement of these forms of administration so that both gels and creams have been proposed to improve their characteristics using nanotechnology. Thus, improving the contact time with the skin, producing a uniform dispersion of the active substance, increasing the stability and bioavailability of the active substance, and high penetration through the skin are some of the qualities of the formulations improved by nanotechnology [215].
Nanoemulsion is “a system of water, oil, and amphiphile, which is a single optically isotropic and thermodynamically stable liquid solution” [216]. This type of emulsion is a formulation option that is suitable for both lipophilic and hydrophilic substances [217]. The advantages of nanoemulsions include reduced toxicity, the ability to be administered by various routes (topical, transdermal, parenteral, and others), and an increase in the stability of incorporated active substances [215,217]. Using this release system, numerous pharmaceuticals, including analgesics, anti-inflammatories, antidepressants, anti-anginal, anti-psychotics, and anti-cancer agents, have been researched and developed [217]. Recently, nanoemulsions significantly improved the skin penetration capacity of THCA and CBDA cannabinoids. This transdermal release system potentiated the stability, permeation rates, and solubility of cannabinoids. Thus, these promising results propose nanoemulsions as a strategy to improve the stability of cannabinoids in dermal formulations [189]. On the other hand, although promising, this drug delivery system also presents a series of disadvantages. The realization of nanoemulsions requires a series of special formulation techniques, which involve considerable financial efforts. In addition, there is scientific evidence that confirms a potential disruption of the integrity of the lipids of the corneous layer of the skin, a disadvantage generated by substances that further enhance the permeation of the active substance through the skin [215]. Despite these drawbacks, the research field of nanocarriers continues to develop. Thus, other nanoparticles are created, such as liposomes, to improve drug delivery skin systems.
One or more lipid layers that incorporate an aqueous phase structurally form nanoparticles called liposomes. These vesicular nanocarriers have the advantage of allowing both the topical and transdermal administration of drugs. In addition, liposomes allow the controlled release of the active substance [215]. According to some researchers, by having a higher skin deposition than other delivery systems, liposomes have superior properties relative to oil-/water-type emulsions and solutions [218].
From a mechanistic point of view, liposomes improve the topical administration of drugs by acting as a rate-limiting barrier, which prevents systemic absorption where this is not desired. Additionally, by improving the flexibility of liposomes with the help of surfactants and adding elastic lipid bilayers, these nanocarriers can serve for the transdermal administration of drugs with promising results [219]. At the same time, this delivery system allows the incorporation of highly lipophilic substances, such as cannabinoids. A recent study on an experimental canine model of chronic pain tests the subcutaneous administration of CBD in the form of liposomes. This study demonstrates that liposomal CBD produces qualifying CBD plasma concentrations that are maintained over the tested period (28 days) [220]. Accordingly, liposomes can become a successful method of administration for cannabinoids in the future due to their proven analgesic effect. However, there are also disadvantages with respect to the use of these nanocarriers. These formulations can determine the systemic absorption of active substances through the shunt or follicular pathway. Thus, there is a risk of systemic adverse reactions. In addition, the high costs of the preparation technology used and certain stability problems can create difficulties in the clinical expansion of these types of formulations [219,221].
Solid lipid nanoparticles (SLNs) are lipid nanoparticles that are known for their low toxicity, ensuring biodegradability and biocompatibility for drug delivery. In addition, via topical administration, these systems potentiate the penetration of active substances through the SC of the skin, ensuring a uniform, homogeneous administration and increased adhesiveness. On the other hand, these systems have the disadvantage that they can lead to drug deposits in certain areas of the body where they were administered. The desired drug deposits, which have therapeutic importance, are at the level of hair follicles and sebaceous and sweat glands [215]. These nanocarriers are superior to nanoemulsions and are suitable candidates for the incorporation and topical administration of highly lipophilic drugs [222].
On the other hand, nanostructured lipid carriers (NLCs) are a form of nanoparticles with improved properties compared to SLN. These nanocarriers are made up of a mixture of solid and liquid lipids. These nanoparticles show promising results for topical administration. They form small-sized particles, have superior adhesion power at the level of the SC, increase the bioavailability of drugs, and improve the hydrophilic properties of the active substances. Compared to SLNs, NLCs have improved occlusive properties [223,224]. Unfortunately, the evidence for the effective transdermal administration of NLC is insufficient and inconclusive [225]. Cannabinoids have been studied in the form of NLC. For example, the intranasal administration of CBD in the form of NLC improved antinociceptive effects in chronic neuropathic pain induced by chemotherapy in a murine model. This effect was more potent for NLC compared to the CBD solution [207]. Additionally, in a recent in vitro study, it was shown that the photostability of cannabidiol extracts can be improved by their encapsulation in nanostructured lipid carriers (NLCs). In addition, in the same study, the authors managed, using this type of nanoformulation, to potentiate the anti-inflammatory activity of cannabidiol at this level [162].
In summary, drug delivery systems that use nanotechnologies present both pros and cons. Even so, lipid-based nanotechnologies are intelligent drug delivery systems and are promising for the administration of cannabinoids on the skin for topical and transdermal action.
3. Future Perspectives on the Transdermal Delivery of Cannabinoids
The undeniable development with respect to increasing cannabinoid bioavailability, whether natural or synthetic, has increased their potential of being introduced into therapy, with the ultimate objective of increasing bioavailability and efficacy and lowering toxicity and/or adverse effects. However, as the research study’s findings indicate, highlighted in Section 2 of the current work, such studies need to continue to provide feasible solutions to the issues that scientists in the field are still facing, and these issues are as follows: (i) most cannabinoids have harmful and/or psychoactive effects when administered systemically; (ii) the need for extending the pain-relieving effect; (iii) the poor ability of cannabinoids within topical formulations to cross all skin layers; (iv) overcoming the legal issues associated with the use of these substances for therapeutic purposes.
Cannabinoid study has become a mainstream discipline as a result of the growing interest in the use of cannabinoids in pharmaceutical formulations, which show promise in the treatment of a number of diseases. These studies revealed a couple of key concepts that need to be considered when designing or optimizing novel pharmaceutical formulations with the purpose of enhancing cannabinoid transport. These concepts will be further discussed in more detail. Using cannabinoid compounds with no affinity for CB1 receptors from CNS (central nervous system), which drastically limits the selection of effective solutions, or formulating them so that they cannot cross the BBB are two practical ways to avoid the psychotropic action of cannabinoid compounds. Another interesting perspective in order to avoid the psychotropic effects of common cannabinoids is represented by the design and synthesis of dualsteric/bitopic ligands that are able to selectively target CB2 receptors versus CB1, as Gado et al. reported [226].
When released into the bloodstream, cannabinoids have the ability to cross the BBB, where they will exert their undesirable effects on the CNS. The topical formulations of such substances may thus offer a unique alternative to avoid their binding to CB1 receptors at the central level by employing the structures of the epidermis as a reservoir for cannabinoids. This paradigm is obviously particularly important, as it prevents the rapid release of a large amount of substance into the bloodstream with the detrimental consequences already mentioned, but it is equally important to develop formulations that enable the controlled release of the active ingredient from these deposits as a way to extend the duration of the expected effect.
Pharmaceutical formulations for external application need to ensure effective transdermal delivery of the therapeutically relevant substance. In this regard, the oil–water partition coefficient, logP, which describes the degree of lipophilicity of a molecule or molecular assembly [227,228], is of particular interest, along with other physicochemical properties, including the melting point, aqueous solubility, pKa, and molecular weight (Mw). In order to be able to penetrate through the skin’s layers, particularly the SC, the optimal log P value of a chemical entity should be within the range of 1–3 [229,230]. Consequently, transdermal formulations of cannabinoids should reduce their log P from values of 6–7 to those within the optimum range.
As revealed in Section 2.1, the ongoing research with respect to obtaining appropriate solutions for the use of cannabinoids for therapeutic purposes has resulted in the development of a wide range of formulations, with each one having its advantages and disadvantages. The most promising outcomes from the perspective of therapeutic efficacy which don’t cause significant discomfort for the patient and at a competitive production price, should serve as a basis for the further development of technologies envisioned for introduction the of new cannabinoid therapeutic agents into the clinic. Nanotechnology allowed the encapsulation of cannabinoids in nanocarriers, improving their physical–chemical stability and bioavailability while also preventing degradation. In this regard, several nanotechnology-based formulation strategies have been developed, of which lipid-based nanoparticles have proven to be the most attractive for transdermal delivery. As shown in Figure 4, such formulations can be tailored in various approaches, and these range from simple micro- or nanoemulsions to complex architectures, such as liposomes, solid lipid nanoparticles (SLNs), lipid nanocapsules (LNCs), or self-emulsifying drug delivery systems (SEDDS) [22,231]. Despite the fact that they exhibit obvious benefits over conventional topical formulations, typical liposomes are believed to be unsuitable as transdermal delivery systems of drugs. Unmodified liposomes have been retained in the SC because of their rigid structure, which prevents diffusion into the deeper skin layers. In addition, the use of regular liposomes is limited by their poor stability, poor encapsulation efficiency, and decreased loading capacity [232]. To develop an innovative class of liposomal formulations with enhanced properties, several approaches have therefore been evolved, with one of them being focused on deformable liposomal formulations including transfersomes, ethosomes, invasomes, mentosomes, and niosomes. Ogunsola and colab. have depicted a method for the preparation and characterization of flexible liposomes, also named transfersomes, and they are able to pass through the small intercellular spaces between SC cells (20–40 nm) [233]. This study has established the dependence between the degree of skin permeability and the ratio between phosphatidylcholine (PC) and Tween 80 (a non-ionic surfactant), the main constituents in the composition of the liposomes prepared by the research group. To be included in transdermal formulations, future research should focus on optimizing the preparation method of this type of liposomes to counteract their main weaknesses, such as instability against oxidative degradation [234].
Sermsaksasithorn and colab. have approached the transdermal administration of CBD from Cannabis sativa with the help of a transdermal patch, aiming to alleviate the effect on psoriasis, within a randomized double-blind controlled trial [235]. The authors thought out the benefits of employing transdermal patches, which are similar to those of any other transdermal delivery system; however, the patches also provide better dose control. The most suitable substances for such delivery systems are lipophilic molecules with low molecular weight, and they also have lower melting points and higher volatility, characteristics associated with excellent skin penetration and relatively simple formulation [236]. Isaac and Holvey emphasized the impact of using transdermal patches in psychiatric medication, through which the legal concerns of the use of drugs with psychotropic action are overcome, preventing the possibility of drug abuse and facilitating the least restrictive affordable administration of prescribed medication as well. From an economic point of view, the cost of a transdermal formulation, particularly in the form of patches, has always been a subject of debate as the costs are much higher compared to the same treatment administered orally.
Nevertheless, the formulation of cannabinoids with the help of nanotechnology, along with many other drugs, is in continuous progress, allowing unique solutions to numerous challenges that would otherwise have remained unsolved. Future strategies in the field should provide at the same time accessible, reproducible, and cost-reduced solutions.
4. Conclusions
Cannabis-based products intended for administration on the skin should be developed by keeping the final target of the pharmacological action of compounds in mind. On one hand, those that target local actions in the upper layers of the skin can be formulated as conventional topical formulations (creams, gels, or ointments) by simply incorporating the compounds or natural extracts in the formulation’s base. On the other hand, for systemic actions, advanced transport systems that allow passage through all skin layers into systemic circulation should be developed.
Studies focusing on major dermatologic pathologies assess the potential of cannabinoids as a therapeutic alternative to conventional treatments, not only underlining their efficacy but also their good safety profile. Topical formulations containing natural cannabinoids have shown local analgesic, antipruritic, anti-inflammatory, cicatrizing, or antibacterial actions, demonstrating their benefits in the treatment of conditions such as psoriasis, atopic dermatitis, allergic contact dermatitis, eczema, lichen simplex, varicose ulcer, or epidermolysis bullosa. For millennia, the traditional use of natural cannabinoids has provided empirical evidence that they may have considerably fewer adverse events than current synthetic pharmacological agents. Because they are of natural origin, phytocannabinoids circumvent the drawbacks of synthetic compounds, which require significant resources both for production and for the removal of byproducts or solvents that are typically toxic or have undesirable effects. For these formulations, developing standardized products with an exact content of cannabinoids or standardized Cannabis extracts is required, and they should be clinically tested.
The treatment of conditions that involve the modulation of specific receptors, whether they are endocannabinoid receptors or other types of receptors, requires advanced processing to allow the systemic absorption of cannabinoids. In an attempt to develop such an advanced cannabinoid transport system, it would be ideal to consider the following aspects: (i) Only compounds of known purity can be used to prepare advanced delivery systems, while the active principle content from formulations based on plant extracts is difficult to optimize; (ii) the methods of loading active compounds need to be optimized to obtain precisely dosed products that release a well-defined quantity of the substance; (iii) controlled release systems that can maintain an effective plasma concentration as long as possible should be developed; (iv) cannabinoids exhibiting psychotropic effects should be preferably encapsulated in certain transport systems that prevent their passage through the BBB, and only peripheral CB receptors should be modulated; (v) production technologies have to be improved to circumvent excessively high costs that limit the access to such products.
Author Contributions
Conceptualization, W.B., B.-I.T., A.-N.N., C.M.U. and S.-I.F.; writing—original draft preparation, S.-I.F., W.B., B.-I.T., A.N.N., C.M.U., L.-E.F., I.M.T., A.N.B., M.F.H. and V.P.; supervision, W.B., B.-I.T., C.M.U. and A.-N.N. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by a grant from the Ministry of Research, Innovation, and Digitization, CNCS/CCCDI—UEFISCDI, project number PN-III-P4-ID-PCE-2020-1247, within PNCDI III.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
pCBs: phytocannabinoids; THC, tetrahydrocannabinol; Δ8-THC, Δ8-tetrahydrocannabinol; Δ9-THC, Δ9-tetrahydrocannabinol; CBD, cannabidiol; CBG, cannabigerol; CBN, cannabinol; CBE, cannabielsoin; CBC, cannabichromene; CBL, cannabicyclol; CBND, cannabinodiol; CBT, cannabitriol; ECS, endocannabinoid system; SC, stratum corneum; GPCRs, G-protein-coupled receptors; TRPV1, transient receptor potential vanilloid-1; TRPV3, transient receptor potential vanilloid-3; TRPA1, transient receptor potential ankyrin 1; PPARs, proliferator-activated receptors; AD, atopic dermatitis; ACD, allergic contact dermatitis; NB-UVB, narrowband ultraviolet B radiation; PUVA, psoralen Ultraviolet A radiation; TNF, tumor necrosis factor; IL, interleukin; UVB, ultraviolet B radiations; AEA, N-arachidonoyl ethanolamide; 2-AG, 2-arachidonoyl glycerol; PEA, N-palmitoyl ethanolamide, palmitoylethanolamide; ALEA, N-alpha-linolenoyl ethanolamide; LEA, N-linoleoyl ethanolamide; OEA, N-oleoyl ethanolamide; SEA, N-stearoyl ethanolamide; EPEA, N-eicosapentaenoyl ethanolamide; DHEA, N-docosahexaenoyl ethanolamide; TRP transient receptors; CCL8, C-C Motif Chemokine Ligand 8; CXCL10, C-X-C motif chemokine ligand 10; TH2, T helper 2; PPARγ, proliferative peroxisome-activated receptor gamma; IL, Interleukin; TNF-α, tumor necrosis factor α; HIF-1α, inducible factor-1α; VEGF, vascular endothelial growth factor; bFGF, basic fibro-blast growth factor; FAAH, fatty acid amide hydrolase enzyme; HDF, human dermal fibroblast; VEGF-A, vascular endothelial growth factor A; MMP-9, matrix metallopeptidase 9; CYP, cytochrome P450; AUC, area under the plasma concentration/time curve.
References
- Abel, E.L.; Emboden, W. Marihuana. The First Twelve Thousand Years. Ernest L. Abel. Q. Rev. Biol. 1981, 56, 514. [Google Scholar] [CrossRef]
- Filipiuc, L.E.; Ababei, D.C.; Alexa-Stratulat, T.; Pricope, C.V.; Bild, V.; Stefanescu, R.; Stanciu, G.D.; Tamba, B.-I. Major Phytocannabinoids and Their Related Compounds: Should We Only Search for Drugs That Act on Cannabinoid Receptors? Pharmaceutics 2021, 13, 1823. [Google Scholar] [CrossRef]
- Johal, H.; Vannabouathong, C.; Chang, Y.; Zhu, M.; Bhandari, M. Medical cannabis for orthopaedic patients with chronic musculoskeletal pain: Does evidence support its use? Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X2093796. [Google Scholar] [CrossRef]
- Butrica, J.L. The Medical Use of Cannabis Among the Greeks and Romans. J. Cannabis Ther. 2002, 2, 51–70. [Google Scholar] [CrossRef]
- Turgeman, I.; Bar-Sela, G. Cannabis for cancer–illusion or the tip of an iceberg: A review of the evidence for the use of Cannabis and synthetic cannabinoids in oncology. Expert Opin. Investig. Drugs 2019, 28, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Zuardi, A.W. History of cannabis as a medicine: A review. Rev. Bras. Psiquiatr. 2006, 28, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.; Gomes, A.; Boas, I.; Marto, J.; Ribeiro, H. Cannabis-Based Products for the Treatment of Skin Inflammatory Diseases: A Timely Review. Pharmaceuticals 2022, 15, 210. [Google Scholar] [CrossRef]
- McPartland, J.M. Cannabis Systematics at the Levels of Family, Genus, and Species. Cannabis Cannabinoid Res. 2018, 3, 203–212. [Google Scholar] [CrossRef]
- Gloss, D. An Overview of Products and Bias in Research. Neurotherapeutics 2015, 12, 731–734. [Google Scholar] [CrossRef]
- Pollio, A. The Name of Cannabis: A Short Guide for Nonbotanists. Cannabis Cannabinoid Res. 2016, 1, 234–238. [Google Scholar] [CrossRef]
- Punja, Z.K.; Holmes, J.E. Hermaphroditism in Marijuana (Cannabis sativa L.) Inflorescences—Impact on Floral Morphology, Seed Formation, Progeny Sex Ratios, and Genetic Variation. Front. Plant Sci. 2020, 11, 718. [Google Scholar] [CrossRef]
- Farag, S.; Kayser, O. The Cannabis Plant: Botanical Aspects. In Handbook of Cannabis and Related Pathologies: Biology, Pharmacology, Diagnosis, and Treatment; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 3–12. ISBN 9780128008270. [Google Scholar]
- Chayasirisobhon, S. Mechanisms of Action and Pharmacokinetics of Cannabis. Perm. J. 2021, 25, 1–3. [Google Scholar] [CrossRef]
- Milay, L.; Berman, P.; Shapira, A.; Guberman, O.; Meiri, D. Metabolic Profiling of Cannabis Secondary Metabolites for Evaluation of Optimal Postharvest Storage Conditions. Front. Plant Sci. 2020, 11, 583605. [Google Scholar] [CrossRef] [PubMed]
- Tamba, B.I.; Stanciu, G.D.; Urîtu, C.M.; Rezus, E.; Stefanescu, R.; Mihai, C.T.; Luca, A.; Rusu-zota, G.; Leon-constantin, M.M.; Cojocaru, E.; et al. Challenges and opportunities in preclinical research of synthetic cannabinoids for pain therapy. Medicina 2020, 56, 24. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.B. History of Cannabis and Its Preparations in Saga, Science, and Sobriquet. Chem. Biodivers. 2007, 4, 1614–1648. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, J.; Rosado, T.; Soares, S.; Simão, A.Y.; Caramelo, D.; Luís, Â.; Fernández, N.; Barroso, M.; Gallardo, E.; Duarte, A.P. Cannabis and Its Secondary Metabolites: Their Use as Therapeutic Drugs, Toxicological Aspects, and Analytical Determination. Medicines 2019, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Pertwee, R.G. Cannabinoid pharmacology: The first 66 years. Br. J. Pharmacol. 2006, 147, 163–171. [Google Scholar] [CrossRef]
- Curran, H.V.; Freeman, T.P.; Mokrysz, C.; Lewis, D.A.; Morgan, C.J.A.; Parsons, L.H. Keep off the grass? Cannabis, cognition and addiction. Nat. Rev. Neurosci. 2016, 17, 293–306. [Google Scholar] [CrossRef]
- ElSohly, M.A.; Radwan, M.M.; Gul, W.; Chandra, S.; Galal, A. Phytochemistry of Cannabis sativa L. In Progress in the Chemistry of Organic Natural Products; Kinghorn, A., Falk, H., Gibbons, S., Kobayashi, J., Eds.; Springer: Cham, Switzerland, 2017; Volume 103, pp. 1–36. [Google Scholar]
- Palrasu, M.; Wright, L.; Patel, M.; Leech, L.; Branch, S.; Harrelson, S.; Khan, S. Perspectives on Challenges in Cannabis Drug Delivery Systems: Where Are We? Med. Cannabis Cannabinoids 2022, 5, 102–119. [Google Scholar] [CrossRef]
- Mahmoudinoodezh, H.; Telukutla, S.R.; Bhangu, S.K.; Bachari, A.; Cavalieri, F.; Mantri, N. The Transdermal Delivery of Therapeutic Cannabinoids. Pharmaceutics 2022, 14, 438. [Google Scholar] [CrossRef]
- Mechoulam, R.; Parker, L.A.; Gallily, R. Cannabidiol: An Overview of Some Pharmacological Aspects. J. Clin. Pharmacol. 2002, 42, 11S–19S. [Google Scholar] [CrossRef] [PubMed]
- Paudel, K.S.; Hammell, D.C.; Agu, R.U.; Valiveti, S.; Stinchcomb, A.L. Cannabidiol bioavailability after nasal and transdermal application: Effect of permeation enhancers. Drug Dev. Ind. Pharm. 2010, 36, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Bruni, N.; Della Pepa, C.; Oliaro-Bosso, S.; Pessione, E.; Gastaldi, D.; Dosio, F. Cannabinoid Delivery Systems for Pain and Inflammation Treatment. Molecules 2018, 23, 2478. [Google Scholar] [CrossRef] [PubMed]
- Vacek, J.; Vostalova, J.; Papouskova, B.; Skarupova, D.; Kos, M.; Kabelac, M.; Storch, J. Antioxidant function of phytocannabinoids: Molecular basis of their stability and cytoprotective properties under UV-irradiation. Free Radic. Biol. Med. 2021, 164, 258–270. [Google Scholar] [CrossRef]
- Jîtcă, G.; Ősz, B.E.; Vari, C.E.; Rusz, C.-M.; Tero-Vescan, A.; Pușcaș, A. Cannabidiol: Bridge between Antioxidant Effect, Cellular Protection, and Cognitive and Physical Performance. Antioxidants 2023, 12, 485. [Google Scholar] [CrossRef]
- Palmieri, B.; Laurino, C.; Vadalà, M. A therapeutic effect of cbd-enriched ointment in inflammatory skin diseases and cutaneous scars. Clin. Ther. 2019, 170, e93–e99. [Google Scholar] [CrossRef]
- Tortolani, D.; Di Meo, C.; Standoli, S.; Ciaramellano, F.; Kadhim, S.; Hsu, E.; Rapino, C.; Maccarrone, M. Rare Phytocannabinoids Exert Anti-Inflammatory Effects on Human Keratinocytes via the Endocannabinoid System and MAPK Signaling Pathway. Int. J. Mol. Sci. 2023, 24, 2721. [Google Scholar] [CrossRef]
- Oláh, A.; Markovics, A.; Szabó-Papp, J.; Szabó, P.; Stott, C.; Zouboulis, C.; Bíró, T. Differential effectiveness of selected non-psychotropic phytocannabinoids on human sebocyte functions implicates their introduction in dry/seborrheic skin and acne treatment. Exp. Dermatol. 2016, 25, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Czifra, G.; Szöllősi, A.G.; Tóth, B.I.; Demaude, J.; Bouez, C.; Breton, L.; Bíró, T. Endocannabinoids Regulate Growth and Survival of Human Eccrine Sweat Gland–Derived Epithelial Cells. J. Investig. Dermatol. 2012, 132, 1967–1976. [Google Scholar] [CrossRef]
- Marta, G.; Robinson, G.; Groves, A.; Haselhorst, L.; Nandakumar, S.; Stahl, C.; Kovalchuk, O.; Kovalchuk, I. Phytocannabinoids Stimulate Rejuvenation and Prevent Cellular Senescence in Human Dermal Fibroblasts. Cells 2022, 11, 3939. [Google Scholar] [CrossRef]
- Mazuz, M.; Tiroler, A.; Moyal, L.; Hodak, E.; Nadarajan, S.; Vinayaka, A.C.; Gorovitz-Haris, B.; Lubin, I.; Drori, A.; Drori, G.; et al. Synergistic cytotoxic activity of cannabinoids from cannabis sativa against cutaneous T-cell lymphoma (CTCL) in-vitro and ex-vivo. Oncotarget 2020, 11, 1141–1156. [Google Scholar] [CrossRef]
- Richard, M.A.; Paul, C.; Nijsten, T.; Gisondi, P.; Salavastru, C.; Taieb, C.; Trakatelli, M.; Puig, L.; Stratigos, A.; EADV Burden of Skin Diseases Project Team. Prevalence of most common skin diseases in Europe: A population-based study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Raharja, A.; Mahil, S.K.; Barker, J.N. Psoriasis: A brief overview. Clin. Med. 2021, 21, 170–173. [Google Scholar] [CrossRef]
- Cohen, D.E.; Heidary, N. Treatment of irritant and allergic contact dermatitis. Dermatol. Ther. 2004, 17, 334–340. [Google Scholar] [CrossRef]
- Smith Begolka, W.; Chovatiya, R.; Thibau, I.J.; Silverberg, J.I. Financial Burden of Atopic Dermatitis Out-of-Pocket Health Care Expenses in the United States. Dermatitis 2021, 32, S62–S70. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.B.; Franco, A.I.; Beck, L.A.; Prezzano, J.C. Treatment resistant atopic dermatitis: Challenges and solutions. Clin. Cosmet. Investig. Dermatol. 2019, 12, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Vangipuram, R.; Feldman, S. Ultraviolet phototherapy for cutaneous diseases: A concise review. Oral Dis. 2016, 22, 253–259. [Google Scholar] [CrossRef]
- Plötz, S.G.; Wiesender, M.; Todorova, A.; Ring, J. What is new in atopic dermatitis/eczema? Expert Opin. Emerg. Drugs 2014, 19, 441–458. [Google Scholar] [CrossRef]
- Hino, H. Topical use of steroids in the aged. J. Jpn. Med. Assoc. 1999, 122, 142–147. [Google Scholar]
- Fox, L.; Csongradi, C.; Aucamp, M.; du Plessis, J.; Gerber, M. Treatment Modalities for Acne. Molecules 2016, 21, 1063. [Google Scholar] [CrossRef]
- Tucker, D.; Masood, S. Seborrheic Dermatitis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Brownstone, N. Meeting the Challenges of Acne in Adults. Dermatol. Times 2022, 43, 36–38. [Google Scholar]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2019, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Stasiewicz, A.; Jarocka-Karpowicz, I.; Markowska, A.; Wroński, A.; Gęgotek, A.; Skrzydlewska, E. Antioxidant and Anti-inflammatory Effect of Cannabidiol Contributes to the Decreased Lipid Peroxidation of Keratinocytes of Rat Skin Exposed to UV Radiation. Oxid. Med. Cell. Longev. 2021, 2021, 6647222. [Google Scholar] [CrossRef]
- Klahn, P. Cannabinoids-Promising Antimicrobial Drugs or Intoxicants with Benefits? Antibiotics 2020, 9, 297. [Google Scholar] [CrossRef]
- Luz-Veiga, M.; Amorim, M.; Pinto-Ribeiro, I.; Oliveira, A.L.S.; Silva, S.; Pimentel, L.L.; Rodríguez-Alcalá, L.M.; Madureira, R.; Pintado, M.; Azevedo-Silva, J.; et al. Cannabidiol and Cannabigerol Exert Antimicrobial Activity without Compromising Skin Microbiota. Int. J. Mol. Sci. 2023, 24, 2389. [Google Scholar] [CrossRef]
- Feldman, M.; Sionov, R.; Mechoulam, R.; Steinberg, D. Anti-Biofilm Activity of Cannabidiol against Candida albicans. Microorganisms 2021, 9, 441. [Google Scholar] [CrossRef] [PubMed]
- Kühbacher, A.; Burger-Kentischer, A.; Rupp, S. Interaction of Candida Species with the Skin. Microorganisms 2017, 5, 32. [Google Scholar] [CrossRef]
- Wroński, A.; Jarocka-Karpowicz, I.; Stasiewicz, A.; Skrzydlewska, E. Phytocannabinoids in the Pharmacotherapy of Psoriasis. Molecules 2023, 28, 1192. [Google Scholar] [CrossRef]
- Morin, C.; Raef, H.; Elmariah, S. Neuropathic itch successfully treated with oral cannabinoids: A case series. JAAD Case Rep. 2021, 17, 38–42. [Google Scholar] [CrossRef]
- Martinelli, G.; Magnavacca, A.; Fumagalli, M.; Dell’Agli, M.; Piazza, S.; Sangiovanni, E. Cannabis sativa and Skin Health: Dissecting the Role of Phytocannabinoids. Planta Med. 2021, 88, 492–506. [Google Scholar] [CrossRef]
- Schräder, N.H.B.; Gorell, E.S.; Stewart, R.E.; Duipmans, J.C.; Harris, N.; Perez, V.A.; Tang, J.Y.; Wolff, A.P.; Bolling, M.C. Cannabinoid use and effects in patients with epidermolysis bullosa: An international cross-sectional survey study. Orphanet J. Rare Dis. 2021, 16, 377. [Google Scholar] [CrossRef]
- Bachari, A.; Piva, T.; Salami, S.A.; Jamshidi, N.; Mantri, N. Roles of Cannabinoids in Melanoma: Evidence from In Vivo Studies. Int. J. Mol. Sci. 2020, 21, 6040. [Google Scholar] [CrossRef] [PubMed]
- Laborada, J.; Cohen, P. Cutaneous Squamous Cell Carcinoma and Lichen Simplex Chronicus Successfully Treated with Topical Cannabinoid Oil: A Case Report and Summary of Cannabinoids in Dermatology. Cureus 2022, 14, e23850. [Google Scholar] [CrossRef] [PubMed]
- Sheriff, T.; Lin, M.J.; Dubin, D.; Khorasani, H. The potential role of cannabinoids in dermatology. J. Dermatolog. Treat. 2020, 31, 839–845. [Google Scholar] [CrossRef]
- Peyravian, N.; Deo, S.; Daunert, S.; Jimenez, J. The Anti-Inflammatory Effects of Cannabidiol (CBD) on Acne. J. Inflamm. Res. 2022, 15, 2795–2801. [Google Scholar] [CrossRef] [PubMed]
- Baswan, S.M.; Klosner, A.E.; Glynn, K.; Rajgopal, A.; Malik, K.; Yim, S.; Stern, N. Therapeutic Potential of Cannabidiol (CBD) for Skin Health and Disorders. Clin. Cosmet. Investig. Dermatol. 2020, 13, 927–942. [Google Scholar] [CrossRef]
- Chelliah, M.P.; Zinn, Z.; Khuu, P.; Teng, J.M.C. Self-initiated use of topical cannabidiol oil for epidermolysis bullosa. Pediatr. Dermatol. 2018, 35, e224–e227. [Google Scholar] [CrossRef]
- Maida, V.; Shi, R.B.; Fazzari, F.G.T.; Zomparelli, L. Topical cannabis-based medicines—A novel adjuvant treatment for venous leg ulcers: An open-label trial. Exp. Dermatol. 2021, 30, 1258–1267. [Google Scholar] [CrossRef]
- Makhakhe, L. Topical cannabidiol (CBD) in skin pathology—A comprehensive review and prospects for new therapeutic opportunities. S. Afr. Fam. Pract. 2022, 64, 4. [Google Scholar] [CrossRef]
- Irving, A.; Abdulrazzaq, G.; Chan, S.L.F.; Penman, J.; Harvey, J.; Alexander, S.P.H. Cannabinoid Receptor-Related Orphan G Protein-Coupled Receptors. Adv. Pharmacol. 2017, 80, 223–247. [Google Scholar]
- Premoli, M.; Aria, F.; Bonini, S.A.; Maccarinelli, G.; Gianoncelli, A.; Della Pina, S.; Tambaro, S.; Memo, M.; Mastinu, A. Cannabidiol: Recent advances and new insights for neuropsychiatric disorders treatment. Life Sci. 2019, 224, 120–127. [Google Scholar] [CrossRef]
- Taylor, A.H.; Ang, C.; Bell, S.C.; Konje, J.C. The role of the endocannabinoid system in gametogenesis, implantation and early pregnancy. Hum. Reprod. Update 2007, 13, 501–513. [Google Scholar] [CrossRef]
- Gillies, R.; Lee, K.; Vanin, S.; Laviolette, S.R.; Holloway, A.C.; Arany, E.; Hardy, D.B. Maternal exposure to Δ9-tetrahydrocannabinol impairs female offspring glucose homeostasis and endocrine pancreatic development in the rat. Reprod. Toxicol. 2020, 94, 84–91. [Google Scholar] [CrossRef] [PubMed]
- González-Mariscal, I.; Krzysik-Walker, S.M.; Doyle, M.E.; Liu, Q.R.; Cimbro, R.; Santa-Cruz Calvo, S.; Ghosh, S.; Cieala, A.; Moaddel, R.; Carlson, O.D.; et al. Human CB1 Receptor Isoforms, present in Hepatocytes and β-cells, are Involved in Regulating Metabolism. Sci. Rep. 2016, 6, 33302. [Google Scholar] [CrossRef]
- Joshi, N.; Onaivi, E.S. Endocannabinoid System Components: Overview and Tissue Distribution. Adv. Exp. Med. Biol. 2019, 1162, 1–12. [Google Scholar]
- Deiana, S. Potential Medical Uses of Cannabigerol: A Brief Overview. In Handbook of Cannabis and Related Pathologies: Biology, Pharmacology, Diagnosis, and Treatment; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 958–967. ISBN 9780128008270. [Google Scholar]
- Bodine, M.; Kemp, A.K. Medical Cannabis Use in Oncology; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Donvito, G.; Nass, S.R.; Wilkerson, J.L.; Curry, Z.A.; Schurman, L.D.; Kinsey, S.G.; Lichtman, A.H. The Endogenous Cannabinoid System: A Budding Source of Targets for Treating Inflammatory and Neuropathic Pain. Neuropsychopharmacology 2018, 43, 52–79. [Google Scholar] [CrossRef]
- del Río, C.; Millán, E.; García, V.; Appendino, G.; DeMesa, J.; Muñoz, E. The endocannabinoid system of the skin. A potential approach for the treatment of skin disorders. Biochem. Pharmacol. 2018, 157, 122–133. [Google Scholar] [CrossRef]
- Alkilani, A.; McCrudden, M.T.; Donnelly, R. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the Stratum Corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef]
- Roberts, M.S. Targeted drug delivery to the skin and deeper tissues: Role of physiology, solute structure and disease. Clin. Exp. Pharmacol. Physiol. 1997, 24, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Khabir, Z.; Partalis, C.; Panchal, J.V.; Deva, A.; Khatri, A.; Garcia-Bennett, A. Enhanced Skin Penetration of Cannabidiol Using Organosilane Particles as Transdermal Delivery Vehicles. Pharmaceutics 2023, 15, 798. [Google Scholar] [CrossRef]
- Tijani, A.O.; Thakur, D.; Mishra, D.; Frempong, D.; Chukwunyere, U.I.; Puri, A. Delivering therapeutic cannabinoids via skin: Current state and future perspectives. J. Control. Release 2021, 334, 427–451. [Google Scholar] [CrossRef]
- Landis, E.; Davis, S.; Feldman, S.; Taylor, S. Complementary and Alternative Medicine Use in Dermatology in the United States. J. Altern. Complement. Med. 2014, 20, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Nickles, M.; Lio, P. Cannabinoids in Dermatology: Hope or Hype? Cannabis Cannabinoid Res. 2020, 5, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Shao, K.; Stewart, C.; Grant-Kels, J.M. Cannabis and the skin. Clin. Dermatol. 2021, 39, 784–795. [Google Scholar] [CrossRef]
- House, W. Global Report on Atopic Dermatitis 2022; The Global Atopic Dermatitis Atlas (GADA): Madagascar, Tunisia, 2022. [Google Scholar]
- Zuberbier, T.; Lötvall, J.; Simoens, S.; Subramanian, S.V.; Church, M.K. Economic burden of inadequate management of allergic diseases in the European Union: A GA 2 LEN review. Allergy 2014, 69, 1275–1279. [Google Scholar] [CrossRef]
- Dickel, H. Management of contact dermatitis. Allergo J. Int. 2023, 32, 57–76. [Google Scholar] [CrossRef]
- Michalek, I.M.; Loring, B.; John, S.M. World Health Organization. Global Report on Psoriasis; World Health Organization: Geneva, Switzerland, 2019; ISBN 9789241565189. [Google Scholar]
- Nair, P.A.; Badri, T. Psoriasis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Benson, H.; Grice, J.; Mohammed, Y.; Namjoshi, S.; Roberts, M. Topical and Transdermal Drug Delivery: From Simple Potions to Smart Technologies. Curr. Drug Deliv. 2019, 16, 444–460. [Google Scholar] [CrossRef]
- Korkina, L. Metabolic and redox barriers in the skin exposed to drugs and xenobiotics. Expert Opin. Drug Metab. Toxicol. 2016, 12, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, C.; Hewitt, N.J.; Merk, H.F.; Reisinger, K. Dermal Xenobiotic Metabolism: A Comparison between Native Human Skin, Four in vitro Skin Test Systems and a Liver System. Ski. Pharmacol. Physiol. 2014, 27, 263–275. [Google Scholar] [CrossRef]
- Gorzelanny, C.; Meß, C.; Schneider, S.; Huck, V.; Brandner, J. Skin Barriers in Dermal Drug Delivery: Which Barriers Have to Be Overcome and How Can We Measure Them? Pharmaceutics 2020, 12, 684. [Google Scholar] [CrossRef]
- Eyerich, S.; Eyerich, K.; Traidl-Hoffmann, C.; Biedermann, T. Cutaneous Barriers and Skin Immunity: Differentiating A Connected Network. Trends Immunol. 2018, 39, 315–327. [Google Scholar] [CrossRef]
- Agarwal, R.; Prakash, O.; Vyas, S. The pilosebaceous unit: A pivotal route for topical drug delivery. Methods Find. Exp. Clin. Pharmacol. 2000, 22, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Kirk, R.D.; Akanji, T.; Li, H.; Shen, J.; Allababidi, S.; Seeram, N.P.; Bertin, M.J.; Ma, H. Evaluations of Skin Permeability of Cannabidiol and Its Topical Formulations by Skin Membrane-Based Parallel Artificial Membrane Permeability Assay and Franz Cell Diffusion Assay. Med. Cannabis Cannabinoids 2022, 5, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Oláh, A.; Toth, B.; Borbíró, I.; Sugawara, K.; Szöllõsi, A.; Czifra, G.; Pal, B.; Ambrus, L.; Hundt, J.; Camera, E.; et al. Cannabidiol exerts sebostatic and antiinflammatory effects on human sebocytes. J. Clin. Investig. 2014, 124, 3713–3724. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Golpe, M.; de-Castro-Ríos, A.; Cruz, A.; López-Rivadulla, M.; Lendoiro, E. Determination and Distribution of Cannabinoids in Nail and Hair Samples. J. Anal. Toxicol. 2021, 45, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Pitliuk, R.; Coelho, C.; Fucci, T. Unexpected improvement of hyperhidrosis with cannabidiol. Einstein 2022, 20, eRC5795. [Google Scholar] [CrossRef]
- Kaemmerer, T.; Clanner-Engelshofen, B.M.; Lesmeister, T.; French, L.E.; Reinholz, M. Cannabinoids in hyperhidrosis. J. Dermatolog. Treat. 2023, 34, 2127308. [Google Scholar] [CrossRef] [PubMed]
- Mounessa, J.S.; Siegel, J.A.; Dunnick, C.A.; Dellavalle, R.P. The role of cannabinoids in dermatology. J. Am. Acad. Dermatol. 2017, 77, 188–190. [Google Scholar] [CrossRef]
- Tóth, K.; Ádám, D.; Bíró, T.; Oláh, A. Cannabinoid Signaling in the Skin: Therapeutic Potential of the “C(ut)annabinoid” System. Molecules 2019, 24, 918. [Google Scholar] [CrossRef]
- Tüting, T.; Gaffal, E. Regulatory Role of Cannabinoids for Skin Barrier Functions and Cutaneous Inflammation. In Handbook of Cannabis and Related Pathologies; Elsevier: Amsterdam, The Netherlands, 2017; pp. 543–549. [Google Scholar]
- Kendall, A.C.; Pilkington, S.M.; Massey, K.A.; Sassano, G.; Rhodes, L.E.; Nicolaou, A. Distribution of Bioactive Lipid Mediators in Human Skin. J. Investig. Dermatol. 2015, 135, 1510–1520. [Google Scholar] [CrossRef]
- Gęgotek, A.; Biernacki, M.; Ambrożewicz, E.; Surażyński, A.; Wroński, A.; Skrzydlewska, E. The cross-talk between electrophiles, antioxidant defence and the endocannabinoid system in fibroblasts and keratinocytes after UVA and UVB irradiation. J. Dermatol. Sci. 2016, 81, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Maccarrone, M.; Di Rienzo, M.; Battista, N.; Gasperi, V.; Guerrieri, P.; Rossi, A.; Finazzi-Agrò, A. The Endocannabinoid System in Human Keratinocytes. J. Biol. Chem. 2003, 278, 33896–33903. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, A.; Pasquariello, N.; Barcaroli, D.; Maccarrone, M. Anandamide Regulates Keratinocyte Differentiation by Inducing DNA Methylation in a CB1 Receptor-dependent Manner. J. Biol. Chem. 2008, 283, 6005–6012. [Google Scholar] [CrossRef]
- Ständer, S.; Schmelz, M.; Metze, D.; Luger, T.; Rukwied, R. Distribution of cannabinoid receptor 1 (CB1) and 2 (CB2) on sensory nerve fibers and adnexal structures in human skin. J. Dermatol. Sci. 2005, 38, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Pagano, C.; Navarra, G.; Coppola, L.; Avilia, G.; Bifulco, M.; Laezza, C. Cannabinoids: Therapeutic Use in Clinical Practice. Int. J. Mol. Sci. 2022, 23, 3344. [Google Scholar] [CrossRef] [PubMed]
- Eagleston, L.R.M.; Kalani, N.K.; Patel, R.R.; Flaten, H.K.; Dunnick, C.A.; Dellavalle, R.P. Cannabinoids in dermatology: A scoping review. Dermatol. Online J. 2018, 24, 1–17. [Google Scholar] [CrossRef]
- Wilkinson, J.D.; Williamson, E.M. Cannabinoids inhibit human keratinocyte proliferation through a non-CB1/CB2 mechanism and have a potential therapeutic value in the treatment of psoriasis. J. Dermatol. Sci. 2007, 45, 87–92. [Google Scholar] [CrossRef]
- Ramot, Y.; Sugawara, K.; Zákány, N.; Tóth, B.I.; Bíró, T.; Paus, R. A novel control of human keratin expression: Cannabinoid receptor 1-mediated signaling down-regulates the expression of keratins K6 and K16 in human keratinocytes in vitro and in situ. PeerJ 2013, 1, e40. [Google Scholar] [CrossRef]
- Borda, L.J.; Wikramanayake, T.C. Seborrheic Dermatitis and Dandruff: A Comprehensive Review. J. Clin. Investig. Dermatol. 2015, 3. [Google Scholar] [CrossRef]
- Gupta, A.K.; Richardson, M.; Paquet, M. Systematic Review of Oral Treatments for Seborrheic Dermatitis. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 16–26. [Google Scholar] [CrossRef]
- Bolognia, J.L.; Schaffer, J.V.; Cerroni, L. Dermatology: 2-Volume Set, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 2, pp. 425–478. [Google Scholar]
- Namazi, M. Cannabinoids, loratadine and allopurinol as novel additions to the antipsoriatic ammunition. J. Eur. Acad. Dermatol. Venereol. 2005, 19, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Norooznezhad, A.H.; Norooznezhad, F. Cannabinoids: Possible agents for treatment of psoriasis via suppression of angiogenesis and inflammation. Med. Hypotheses 2017, 99, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Maya-Rico, A.M.; Londoño-García, Á.; Palacios-Barahona, A.U.; Jimenez-Tamayo, S.B.; Muriel-Lopera, E. Out-of-pocket costs for patients with psoriasis in an outpatient dermatology referral service. An. Bras. Dermatol. 2021, 96, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Escobar, L.G.; Mora-Ochoa, H.; Vargas Villanueva, A.; Spineli, L.; Sanclemente, G.; Couban, R.; García, E.; Chapman, E.; Yepes-Nuñez, J.J. Effectiveness and adverse events of topical and allergen immunotherapy for atopic dermatitis: A systematic review and network meta-analysis protocol. Syst. Rev. 2020, 9, 222. [Google Scholar] [CrossRef] [PubMed]
- Giam, Y.C.; Hebert, A.A.; Dizon, M.V.; Van Bever, H.; Tiongco-Recto, M.; Kim, K.-H.; Soebono, H.; Munasir, Z.; Diana, I.A.; Luk, D.C.K. A review on the role of moisturizers for atopic dermatitis. Asia Pac. Allergy 2016, 6, 120–128. [Google Scholar] [CrossRef]
- Coondoo, A.; Phiske, M.; Verma, S.; Lahiri, K. Side-effects of topical steroids: A long overdue revisit. Indian Dermatol. Online J. 2014, 5, 416. [Google Scholar] [CrossRef]
- Varga, E.; Kemény, L. The use of calcineurin inhibitors in atopic dermatitis. Bőrgyógyászati és Venerológiai Szle 2017, 93, 235–239. [Google Scholar] [CrossRef]
- Carr, W.W. Topical Calcineurin Inhibitors for Atopic Dermatitis: Review and Treatment Recommendations. Pediatr. Drugs 2013, 15, 303–310. [Google Scholar] [CrossRef]
- Frazier, W.; Bhardwaj, N. Atopic Dermatitis: Diagnosis and Treatment. Am. Fam. Physician 2020, 101, 590–598. [Google Scholar] [PubMed]
- Patrizi, A.; Raone, B.; Ravaioli, G.M. Management of atopic dermatitis: Safety and efficacy of phototherapy. Clin. Cosmet. Investig. Dermatol. 2015, 8, 511–520. [Google Scholar] [CrossRef]
- Megna, M.; Napolitano, M.; Patruno, C.; Villani, A.; Balato, A.; Monfrecola, G.; Ayala, F.; Balato, N. Systemic Treatment of Adult Atopic Dermatitis: A Review. Dermatol. Ther. 2017, 7, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, A. Contact allergy to topical corticosteroids and sunscreens. Indian J. Dermatol. Venereol. Leprol. 2012, 78, 552. [Google Scholar] [CrossRef] [PubMed]
- FnF Research Global Report on Seborrheic Dermatitis Market Size & Share Worth USD 5 Billion, to Record a 11.1% CAGR by 2030. Available online: https://www.prnewswire.co.uk/news-releases/global-report-on-seborrheic-dermatitis-market-size--share-worth-usd-5-billion-to-record-a-11-1-cagr-by-2030--seborrheic-dermatitis-industry-trends-segmentation-analysis--forecast-by-fnf-301736378.html (accessed on 8 April 2023).
- Curkova, A.K.; Simaljakova, M. Seborrheic Dermatitis. In European Handbook of Dermatological Treatments; Springer: Berlin/Heidelberg, Germany, 2015; pp. 867–877. [Google Scholar]
- Gaffal, E.; Glodde, N.; Jakobs, M.; Bald, T.; Tüting, T. Cannabinoid 1 receptors in keratinocytes attenuate fluorescein isothiocyanate-induced mouse atopic-like dermatitis. Exp. Dermatol. 2014, 23, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Eicke, C.; Reinhardt, H.-W.; Ring, J. Adjuvant treatment of atopic eczema: Assessment of an emollient containing N-palmitoylethanolamine (ATOPA study). J. Eur. Acad. Dermatol. Venereol. 2007, 22, 73–82. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, B.; Park, B.M.; Jeon, J.E.; Lee, S.H.; Mann, S.; Ahn, S.K.; Hong, S.-P.; Jeong, S.K. Topical cannabinoid receptor 1 agonist attenuates the cutaneous inflammatory responses in oxazolone-induced atopic dermatitis model. Int. J. Dermatol. 2015, 54, e401–e408. [Google Scholar] [CrossRef]
- Petrosino, S.; Verde, R.; Vaia, M.; Allarà, M.; Iuvone, T.; Di Marzo, V. Anti-inflammatory Properties of Cannabidiol, a Nonpsychotropic Cannabinoid, in Experimental Allergic Contact Dermatitis. J. Pharmacol. Exp. Ther. 2018, 365, 652–663. [Google Scholar] [CrossRef]
- Gupta, A.K.; Talukder, M. Cannabinoids for skin diseases and hair regrowth. J. Cosmet. Dermatol. 2021, 20, 2703–2711. [Google Scholar] [CrossRef]
- Dobrosi, N.; Tóth, B.I.; Nagy, G.; Dózsa, A.; Géczy, T.; Nagy, L.; Zouboulis, C.C.; Paus, R.; Kovács, L.; Bíró, T. Endocannabinoids enhance lipid synthesis and apoptosis of human sebocytes via cannabinoid receptor-2-mediated signaling. FASEB J. 2008, 22, 3685–3695. [Google Scholar] [CrossRef]
- Ali, A.; Akhtar, N. The safety and efficacy of 3% Cannabis seeds extract cream for reduction of human cheek skin sebum and erythema content. Pak. J. Pharm. Sci. 2015, 28, 1389–1395. [Google Scholar]
- Gaffal, E.; Cron, M.; Glodde, N.; Tüting, T. Anti-inflammatory activity of topical THC in DNFB-mediated mouse allergic contact dermatitis independent of CB1 and CB2 receptors. Allergy 2013, 68, 994–1000. [Google Scholar] [CrossRef]
- Soliman, E.; Van Dross, R. Anandamide-induced endoplasmic reticulum stress and apoptosis are mediated by oxidative stress in non-melanoma skin cancer: Receptor-independent endocannabinoid signaling. Mol. Carcinog. 2016, 55, 1807–1821. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.; Henderson, K.L.; Danell, A.S.; Van Dross, R. Arachidonoyl-ethanolamide activates endoplasmic reticulum stress-apoptosis in tumorigenic keratinocytes: Role of cyclooxygenase-2 and novel J-series prostamides. Mol. Carcinog. 2016, 55, 117–130. [Google Scholar] [CrossRef]
- Ständer, S.; Reinhardt, H.W.; Luger, T.A. Topical cannabinoid agonists. An effective new possibility for treating chronic pruritus. Der Hautarzt 2006, 57, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Szepietowski, J.C.; Szepietowski, T.; Reich, A. Efficacy and tolerance of the cream containing structured physiological lipids with endocannabinoids in the treatment of uremic pruritus: A preliminary study. Acta Dermatovenerol. Croat. 2005, 13, 97–103. [Google Scholar] [PubMed]
- Broughton, G.; Janis, J.E.; Attinger, C.E. The Basic Science of Wound Healing. Plast. Reconstr. Surg. 2006, 117, 12S–34S. [Google Scholar] [CrossRef]
- Ellis, S.; Lin, E.J.; Tartar, D. Immunology of Wound Healing. Curr. Dermatol. Rep. 2018, 7, 350–358. [Google Scholar] [CrossRef]
- Zhao, Z.; Guan, D.; Liu, W.; Wang, T.; Fan, Y.; Cheng, Z.; Zheng, J.; Hu, G. Expression of cannabinoid receptor I during mice skin incised wound healing course. Fa Yi Xue Za Zhi 2010, 26, 241–245. [Google Scholar]
- Zheng, J.-L.; Yu, T.-S.; Li, X.-N.; Fan, Y.-Y.; Ma, W.-X.; Du, Y.; Zhao, R.; Guan, D.-W. Cannabinoid receptor type 2 is time-dependently expressed during skin wound healing in mice. Int. J. Leg. Med. 2012, 126, 807–814. [Google Scholar] [CrossRef]
- Wang, L.-L.; Zhao, R.; Li, J.-Y.; Li, S.-S.; Liu, M.; Wang, M.; Zhang, M.-Z.; Dong, W.-W.; Jiang, S.-K.; Zhang, M.; et al. Pharmacological activation of cannabinoid 2 receptor attenuates inflammation, fibrogenesis, and promotes re-epithelialization during skin wound healing. Eur. J. Pharmacol. 2016, 786, 128–136. [Google Scholar] [CrossRef]
- Bort, A.; Alvarado-Vazquez, P.A.; Moracho-Vilrriales, C.; Virga, K.G.; Gumina, G.; Romero-Sandoval, A.; Asbill, S. Effects of JWH015 in cytokine secretion in primary human keratinocytes and fibroblasts and its suitability for topical/transdermal delivery. Mol. Pain 2017, 13. [Google Scholar] [CrossRef]
- Ramot, Y.; Oláh, A.; Paus, R. Cover Image: Neuroendocrine treatment of inherited keratin disorders by cannabinoids? Br. J. Dermatol. 2018, 178, 1469. [Google Scholar] [CrossRef] [PubMed]
- Sangiovanni, E.; Fumagalli, M.; Pacchetti, B.; Piazza, S.; Magnavacca, A.; Khalilpour, S.; Melzi, G.; Martinelli, G.; Dell’Agli, M. Cannabis sativa L. extract and cannabidiol inhibit in vitro mediators of skin inflammation and wound injury. Phyther. Res. 2019, 33, 2083–2093. [Google Scholar] [CrossRef] [PubMed]
- Bolzinger, M.-A.; Briançon, S.; Pelletier, J.; Chevalier, Y. Penetration of drugs through skin, a complex rate-controlling membrane. Curr. Opin. Colloid Interface Sci. 2012, 17, 156–165. [Google Scholar] [CrossRef]
- Kong, M.; Chen, X.G.; Kweon, D.K.; Park, H.J. Investigations on skin permeation of hyaluronic acid based nanoemulsion as transdermal carrier. Carbohydr. Polym. 2011, 86, 837–843. [Google Scholar] [CrossRef]
- Larese Filon, F.; Mauro, M.; Adami, G.; Bovenzi, M.; Crosera, M. Nanoparticles skin absorption: New aspects for a safety profile evaluation. Regul. Toxicol. Pharmacol. 2015, 72, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Larrañeta, E.; Lutton, R.E.M.; Woolfson, A.D.; Donnelly, R.F. Microneedle arrays as transdermal and intradermal drug delivery systems: Materials science, manufacture and commercial development. Mater. Sci. Eng. R Rep. 2016, 104, 1–32. [Google Scholar] [CrossRef]
- Moser, K. Passive skin penetration enhancement and its quantification in vitro. Eur. J. Pharm. Biopharm. 2001, 52, 103–112. [Google Scholar] [CrossRef]
- Godin, B.; Touitou, E. Transdermal skin delivery: Predictions for humans from in vivo, ex vivo and animal models. Adv. Drug Deliv. Rev. 2007, 59, 1152–1161. [Google Scholar] [CrossRef]
- Goyal, R.; Macri, L.K.; Kaplan, H.M.; Kohn, J. Nanoparticles and nanofibers for topical drug delivery. J. Control. Release 2016, 240, 77–92. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef]
- Stella, B.; Baratta, F.; Della Pepa, C.; Arpicco, S.; Gastaldi, D.; Dosio, F. Cannabinoid Formulations and Delivery Systems: Current and Future Options to Treat Pain. Drugs 2021, 81, 1513–1557. [Google Scholar] [CrossRef] [PubMed]
- Madej, K.; Chmiołek, A.; Szlachta, K.; Piekoszewski, W. HPLC-DAD Analysis of Hemp Oil Supplements for Determination of Four Cannabinoids: Cannabidiol, Cannabidiolic Acid, Cannabinol and Delta 9-Tetrahydrocannabinol. Separations 2021, 8, 227. [Google Scholar] [CrossRef]
- Toprak, Ş. Theoretical calculation of some chemical properties of the cannabidiol (CBD) molecule. Int. J. Sci. Lett. 2021, 3, 129–142. [Google Scholar] [CrossRef]
- Thomas, B.F.; Compton, D.R.; Martin, B.R. Characterization of the lipophilicity of natural and synthetic analogs of delta 9-tetrahydrocannabinol and its relationship to pharmacological potency. J. Pharmacol. Exp. Ther. 1990, 255, 624–630. [Google Scholar]
- Furqan, T.; Batool, S.; Habib, R.; Shah, M.; Kalasz, H.; Darvas, F.; Kuca, K.; Nepovimova, E.; Batool, S.; Nurulain, S.M. Cannabis Constituents and Acetylcholinesterase Interaction: Molecular Docking, In Vitro Studies and Association with CNR1 rs806368 and ACHE rs17228602. Biomolecules 2020, 10, 758. [Google Scholar] [CrossRef]
- ChemSpider. Cannabigerol. Available online: http://www.chemspider.com/Chemical-Structure.4474921.html (accessed on 12 January 2023).
- Russo, E.B.; Burnett, A.; Hall, B.; Parker, K.K. Agonistic Properties of Cannabidiol at 5-HT1a Receptors. Neurochem. Res. 2005, 30, 1037–1043. [Google Scholar] [CrossRef]
- Costa, B.; Giagnoni, G.; Franke, C.; Trovato, A.E.; Colleoni, M. Vanilloid TRPV1 receptor mediates the antihyperalgesic effect of the nonpsychoactive cannabinoid, cannabidiol, in a rat model of acute inflammation. Br. J. Pharmacol. 2004, 143, 247–250. [Google Scholar] [CrossRef]
- Blaskovich, M.A.T.; Kavanagh, A.M.; Elliott, A.G.; Zhang, B.; Ramu, S.; Amado, M.; Lowe, G.J.; Hinton, A.O.; Pham, D.M.T.; Zuegg, J.; et al. The antimicrobial potential of cannabidiol. Commun. Biol. 2021, 4, 7. [Google Scholar] [CrossRef]
- Morakul, B.; Junyaprasert, V.B.; Sakchaisri, K.; Teeranachaideekul, V. Cannabidiol-Loaded Nanostructured Lipid Carriers (NLCs) for Dermal Delivery: Enhancement of Photostability, Cell Viability, and Anti-Inflammatory Activity. Pharmaceutics 2023, 15, 537. [Google Scholar] [CrossRef]
- Grifoni, L.; Vanti, G.; Donato, R.; Sacco, C.; Bilia, A.R. Promising Nanocarriers to Enhance Solubility and Bioavailability of Cannabidiol for a Plethora of Therapeutic Opportunities. Molecules 2022, 27, 6070. [Google Scholar] [CrossRef]
- Huestis, M.A. Pharmacokinetics and Metabolism of the Plant Cannabinoids, Δ 9-Tetrahydrocannibinol, Cannabidiol and Cannabinol. In Cannabinoids. Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2005; pp. 657–690. [Google Scholar]
- Zendulka, O.; Dovrtělová, G.; Nosková, K.; Turjap, M.; Šulcová, A.; Hanuš, L.; Juřica, J. Cannabinoids and Cytochrome P450 Interactions. Curr. Drug Metab. 2016, 17, 206–226. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration Marinol (Dronabinol) Technical Sheet. Nda 18-651/s-021. 2004, 3. Available online: https://digitalcommons.wcl.american.edu/cgi/viewcontent.cgi?article=2087&context=aulr (accessed on 21 March 2023).
- Harvey, D.J.; Samara, E.; Mechoulam, R. Urinary metabolites of cannabidiol in dog, rat and man and their identification by gas chromatography—Mass spectrometry. J. Chromatogr. B Biomed. Sci. Appl. 1991, 562, 299–322. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Yamaori, S.; Takeda, S.; Yamamoto, I.; Watanabe, K. Identification of cytochrome P450 enzymes responsible for metabolism of cannabidiol by human liver microsomes. Life Sci. 2011, 89, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Geffrey, A.L.; Pollack, S.F.; Bruno, P.L.; Thiele, E.A. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia 2015, 56, 1246–1251. [Google Scholar] [CrossRef] [PubMed]
- Flannery, L.E.; Kerr, D.M.; Finn, D.P.; Roche, M. FAAH inhibition attenuates TLR3-mediated hyperthermia, nociceptive- and anxiety-like behaviour in female rats. Behav. Brain Res. 2018, 353, 11–20. [Google Scholar] [CrossRef]
- Zanfirescu, A.; Nitulescu, G.; Mihai, D.P.; Nitulescu, G.M. Identifying FAAH Inhibitors as New Therapeutic Options for the Treatment of Chronic Pain through Drug Repurposing. Pharmaceuticals 2021, 15, 38. [Google Scholar] [CrossRef]
- Hill, M.N.; Kumar, S.A.; Filipski, S.B.; Iverson, M.; Stuhr, K.L.; Keith, J.M.; Cravatt, B.F.; Hillard, C.J.; Chattarji, S.; McEwen, B.S. Disruption of fatty acid amide hydrolase activity prevents the effects of chronic stress on anxiety and amygdalar microstructure. Mol. Psychiatry 2013, 18, 1125–1135. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Liebowitz, M.R.; Stein, M.B.; Grunfeld, J.; Van Hove, I.; Simmons, W.K.; Van Der Ark, P.; Palmer, J.A.; Saad, Z.S.; Pemberton, D.J.; et al. The effects of inhibition of fatty acid amide hydrolase (FAAH) by JNJ-42165279 in social anxiety disorder: A double-blind, randomized, placebo-controlled proof-of-concept study. Neuropsychopharmacology 2021, 46, 1004–1010. [Google Scholar] [CrossRef]
- Pacifici, R.; Marchei, E.; Salvatore, F.; Guandalini, L.; Busardò, F.P.; Pichini, S. Evaluation of long-term stability of cannabinoids in standardized preparations of cannabis flowering tops and cannabis oil by ultra-high-performance liquid chromatography tandem mass spectrometry. Clin. Chem. Lab. Med. 2018, 56, 94–96. [Google Scholar] [CrossRef]
- Fairbairn, J.W.; Liebmann, J.A.; Rowan, M.G. The stability of cannabis and its preparations on storage. J. Pharm. Pharmacol. 2011, 28, 1–7. [Google Scholar] [CrossRef]
- Agurell, S.; Carlsson, S.; Lindgren, J.E.; Ohlsson, A.; Gillespie, H.; Hollister, L. Interactions ofΔ 11-tetrahydrocannabinol with cannabinol and cannabidiol following oral administration in man. Assay of cannabinol and cannabidiol by mass fragmentographywith cannabinol and cannabidiol following oral administration in man. Assay of cannabinol and cannabidiol by mass fragmentography. Experientia 1981, 37, 1090–1092. [Google Scholar] [CrossRef] [PubMed]
- Eichler, M.; Spinedi, L.; Unfer-Grauwiler, S.; Bodmer, M.; Surber, C.; Luedi, M.; Drewe, J. Heat Exposure of Cannabis sativa Extracts Affects the Pharmacokinetic and Metabolic Profile in Healthy Male Subjects. Planta Med. 2012, 78, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Anselmo, A.C.; Mitragotri, S. An overview of clinical and commercial impact of drug delivery systems. J. Control. Release 2014, 190, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Cuevas, G.; Martin-Fardon, R.; Kerr, T.M.; Stouffer, D.G.; Parsons, L.H.; Hammell, D.C.; Banks, S.L.; Stinchcomb, A.L.; Weiss, F. Unique treatment potential of cannabidiol for the prevention of relapse to drug use: Preclinical proof of principle. Neuropsychopharmacology 2018, 43, 2036–2045. [Google Scholar] [CrossRef]
- Liput, D.J.; Hammell, D.C.; Stinchcomb, A.L.; Nixon, K. Transdermal delivery of cannabidiol attenuates binge alcohol-induced neurodegeneration in a rodent model of an alcohol use disorder. Pharmacol. Biochem. Behav. 2013, 111, 120–127. [Google Scholar] [CrossRef]
- Stinchcomb, A.; Golinski, M.; Hammell, D.; Alltranz, H.J. Products of Tetrahydrocannabinol, Compositions Comprising Prodrugs of Tetrahydrocannabinol and Methods of Using the Same. Patent US20090143462, 26 July 2019. [Google Scholar]
- Doroudian, A.; Frankham, P. Biphasix Cannabinoid Delivery. Patent WO2018213932, 25 May 2018. [Google Scholar]
- Gutterman, D.; Sebree, T.; Smith, T.; Messenheimer, J. Synthetic Transdermal Cannabidiol for the Treatment of Focal Epilepsy in Adults. Patent US20190083388, 19 March 2019. [Google Scholar]
- Bonn-Miller, M.; Tich, N.; Gutterman, D.; Messenheimer, J.; Sebree, T. Treatment of Fragile X Syndrome with Cannabidiol. Patent US10213390, 26 February 2019. [Google Scholar]
- ME, S. Formulations of Argan Oil and Cannabidiol for Treating Inflammatory Disorders Including Arthritis. WO2017160923A121, 21 September 2017. [Google Scholar]
- Cairns, E.A.; Baldridge, W.H.; Kelly, M.E.M. The Endocannabinoid System as a Therapeutic Target in Glaucoma. Neural Plast. 2016, 2016, 9364091. [Google Scholar] [CrossRef]
- Adelli, G.R.; Bhagav, P.; Taskar, P.; Hingorani, T.; Pettaway, S.; Gul, W.; ElSohly, M.A.; Repka, M.A.; Majumdar, S. Development of a Δ9-Tetrahydrocannabinol Amino Acid-Dicarboxylate Prodrug With Improved Ocular Bioavailability. Investig. Opthalmology Vis. Sci. 2017, 58, 2167. [Google Scholar] [CrossRef]
- Radwan-Pragłowska, J.; Janus, Ł.; Piątkowski, M.; Sierakowska, A.; Szajna, E.; Matýsek, D.; Bogdał, D. Development of Stimuli-Responsive Chitosan/ZnO NPs Transdermal Systems for Controlled Cannabidiol Delivery. Polymers 2021, 13, 211. [Google Scholar] [CrossRef]
- Park, C.; Zuo, J.; Somayaji, V.; Lee, B.-J.; Löbenberg, R. Development of a novel cannabinoid-loaded microemulsion towards an improved stability and transdermal delivery. Int. J. Pharm. 2021, 604, 120766. [Google Scholar] [CrossRef]
- Sharkawy, A.; Silva, A.M.; Rodrigues, F.; Barreiro, F.; Rodrigues, A. Pickering emulsions stabilized with chitosan/collagen peptides nanoparticles as green topical delivery vehicles for cannabidiol (CBD). Colloids Surf. A Physicochem. Eng. Asp. 2021, 631, 127677. [Google Scholar] [CrossRef]
- Wright, S.; Wilkhu, J. Oral Cannabinoid Formulations. Patent WO2018150182, 23 August 2018. [Google Scholar]
- Wilkhu, J.; Bender, J. GW Research Limited. Cannabinoid Formulations. Patent WO2018002665, 4 January 2018. [Google Scholar]
- Wilkhu, J.; Johan, B. Oral Pharmaceutical Formulation Comprising Cannabinoids and Poloxamer. Patent WO2019135077A1, 11 July 2019. [Google Scholar]
- Hershberger, P.; Arlen, P. Cannabinoid Conjugate Molecules. Patent WO2020263888A1, 30 December 2020. [Google Scholar]
- Patrician, A.; Versic-Bratincevic, M.; Mijacika, T.; Banic, I.; Marendic, M.; Sutlović, D.; Dujić, Ž.; Ainslie, P.N. Examination of a New Delivery Approach for Oral Cannabidiol in Healthy Subjects: A Randomized, Double-Blinded, Placebo-Controlled Pharmacokinetics Study. Adv. Ther. 2019, 36, 3196–3210. [Google Scholar] [CrossRef]
- Macleman, P.D.; Mavlianov, M. Solid Self-Emulsifying Pharmaceutical Compositions. WO2020024009A1, 06 February 2020. [Google Scholar]
- Mavlianov, M.; Macleman, P.D.R. Free-Flowing Powder Compositions. WO2020024011A1, 06 February 2020. [Google Scholar]
- Anastassov, G.; Changoer, L. Chewing Gum Composition Comprising Cannabinoids and Opioid Agonists and/or Antagonists. Patent WO2018075665A1, 26 April 2018. [Google Scholar]
- Williams, N.N.B.; Ewell, T.R.; Abbotts, K.S.S.; Harms, K.J.; Woelfel, K.A.; Dooley, G.P.; Weir, T.L.; Bell, C. Comparison of Five Oral Cannabidiol Preparations in Adult Humans: Pharmacokinetics, Body Composition, and Heart Rate Variability. Pharmaceuticals 2021, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Knaub, K.; Sartorius, T.; Dharsono, T.; Wacker, R.; Wilhelm, M.; Schön, C. A Novel Self-Emulsifying Drug Delivery System (SEDDS) Based on VESIsorb® Formulation Technology Improving the Oral Bioavailability of Cannabidiol in Healthy Subjects. Molecules 2019, 24, 2967. [Google Scholar] [CrossRef] [PubMed]
- Jagtap, P.; Avidan-Shlomovich, S.; Shoken, D.; Salzman, A.L. Cannabinoid Derivatives and Conjugates and Uses Thereof. Patent WO2019159168A1, 22 August 2019. [Google Scholar]
- NCT03773796; Nabilone for Non-Motor Symptoms in Parkinson’s Disease: An Open-Label Study to Evaluate Longterm Safety and Efficacy. U.S. National Library of Medicine: Bethesda, MD, USA, 2021.
- Viernstein, H.; Toegel, S.; Schueller, R. Fast Disintegrating Compositions Comprising Nabilone and Randomly Methylated β-Cyclodextrin. Patent WO2012069591, 31 May 2012. [Google Scholar]
- Kingsley, K.; Lee, S.; Greenbaum, E. Cannabinoid Formulations with Improved Solubility. Patent US20190030170, 31 January 2019. [Google Scholar]
- Temtsin-Krayz, G.; Glozman, S.; Kazhdan, P. Pharmaceutical Compositions for Transmucosal Delivery. WO2017072774A1, 04 May 2017. [Google Scholar]
- Bryson, N.; Sharma, A.C. Nasal Cannabidiol Compositions. WO2017208072A2, 11 January 2018. [Google Scholar]
- Matarazzo, A.P.; Elisei, L.M.S.; Carvalho, F.C.; Bonfílio, R.; Ruela, A.L.M.; Galdino, G.; Pereira, G.R. Mucoadhesive nanostructured lipid carriers as a cannabidiol nasal delivery system for the treatment of neuropathic pain. Eur. J. Pharm. Sci. 2021, 159, 105698. [Google Scholar] [CrossRef] [PubMed]
- Sosnik, A.; Ben Shabo, R.; Halamish, H.M. Cannabidiol-Loaded Mixed Polymeric Micelles of Chitosan/Poly(Vinyl Alcohol) and Poly(Methyl Methacrylate) for Trans-Corneal Delivery. Pharmaceutics 2021, 13, 2142. [Google Scholar] [CrossRef] [PubMed]
- Moqejwa, T.; Marimuthu, T.; Kondiah, P.P.D.; Choonara, Y.E. Development of Stable Nano-Sized Transfersomes as a Rectal Colloid for Enhanced Delivery of Cannabidiol. Pharmaceutics 2022, 14, 703. [Google Scholar] [CrossRef]
- Tapfumaneyi, P.; Imran, M.; Mohammed, Y.; Roberts, M.S. Recent advances and future prospective of topical and transdermal delivery systems. Front. Drug Deliv. 2022, 2, 957732. [Google Scholar] [CrossRef]
- Sinai, A.; Turner, Z.; Baruch, Y. Cannabis-Based Extracts and Topical Formulations for Use in Skin Disorders. US20180042890A1, 21 June 2017. [Google Scholar]
- Hossain, S. Use of Topical Formulations of Cannabinoids in the Treatment of Epidermolysis Bullosa and Related Connective Tissue Disorders. WO2017190249A1, 4 May 2017. [Google Scholar]
- Lindholst, C. Long term stability of cannabis resin and cannabis extracts. Aust. J. Forensic Sci. 2010, 42, 181–190. [Google Scholar] [CrossRef]
- Hammell, D.C.; Zhang, L.P.; Ma, F.; Abshire, S.M.; McIlwrath, S.L.; Stinchcomb, A.L.; Westlund, K.N. Transdermal cannabidiol reduces inflammation and pain-related behaviours in a rat model of arthritis. Eur. J. Pain 2016, 20, 936–948. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Potential of Nanoparticles as Permeation Enhancers and Targeted Delivery Options for Skin: Advantages and Disadvantages. Drug Des. Devel. Ther. 2020, 14, 3271–3289. [Google Scholar] [CrossRef]
- Danielsson, I.; Lindman, B. The definition of microemulsion. Colloids Surf. 1981, 3, 391–392. [Google Scholar] [CrossRef]
- Shukla, T.; Upmanyu, N.; Agrawal, M.; Saraf, S.; Saraf, S.; Alexander, A. Biomedical applications of microemulsion through dermal and transdermal route. Biomed. Pharmacother. 2018, 108, 1477–1494. [Google Scholar] [CrossRef] [PubMed]
- Egbaria, K.; Ramachandran, C.; Weiner, N. Topical Delivery of Ciclosporin: Evaluation of Various Formulations Using in vitro Diffusion Studies in Hairless Mouse Skin. Skin Pharmacol. Physiol. 1990, 3, 21–28. [Google Scholar] [CrossRef] [PubMed]
- El Maghraby, G.M.M.; Williams, A.C.; Barry, B.W. Can drug-bearing liposomes penetrate intact skin? J. Pharm. Pharmacol. 2010, 58, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Shilo-Benjamini, Y.; Cern, A.; Zilbersheid, D.; Hod, A.; Lavy, E.; Barasch, D.; Barenholz, Y. A Case Report of Subcutaneously Injected Liposomal Cannabidiol Formulation Used as a Compassion Therapy for Pain Management in a Dog. Front. Vet. Sci. 2022, 9, 892306. [Google Scholar] [CrossRef]
- Choi, M.J.; Maibach, H.I. Liposomes and Niosomes as Topical Drug Delivery Systems. Skin Pharmacol. Physiol. 2005, 18, 209–219. [Google Scholar] [CrossRef]
- Pokharkar, V.B.; Mendiratta, C.; Kyadarkunte, A.Y.; Bhosale, S.H.; Barhate, G.A. Skin delivery aspects of benzoyl peroxide-loaded solid lipid nanoparticles for acne treatment. Ther. Deliv. 2014, 5, 635–652. [Google Scholar] [CrossRef]
- Fang, J.-Y.; Fang, C.-L.; Liu, C.-H.; Su, Y.-H. Lipid nanoparticles as vehicles for topical psoralen delivery: Solid lipid nanoparticles (SLN) versus nanostructured lipid carriers (NLC). Eur. J. Pharm. Biopharm. 2008, 70, 633–640. [Google Scholar] [CrossRef]
- Ricci, M.; Puglia, C.; Bonina, F.; Di Giovanni, C.; Giovagnoli, S.; Rossi, C. Evaluation of Indomethacin Percutaneous Absorption from Nanostructured Lipid Carriers (NLC): In Vitro and In Vivo Studies. J. Pharm. Sci. 2005, 94, 1149–1159. [Google Scholar] [CrossRef]
- Garcês, A.; Amaral, M.H.; Sousa Lobo, J.M.; Silva, A.C. Formulations based on solid lipid nanoparticles (SLN) and nanostructured lipid carriers (NLC) for cutaneous use: A review. Eur. J. Pharm. Sci. 2018, 112, 159–167. [Google Scholar] [CrossRef]
- Gado, F.; Ferrisi, R.; Polini, B.; Mohamed, K.A.; Ricardi, C.; Lucarini, E.; Carpi, S.; Domenichini, F.; Stevenson, L.A.; Rapposelli, S.; et al. Design, Synthesis, and Biological Activity of New CB2 Receptor Ligands: From Orthosteric and Allosteric Modulators to Dualsteric/Bitopic Ligands. J. Med. Chem. 2022, 65, 9918–9938. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhu, L.; Li, R.; Pang, L.; Zhu, S.; Ma, J.; Du, L.; Jin, Y. Electroporation-enhanced transdermal drug delivery: Effects of logP, pKa, solubility and penetration time. Eur. J. Pharm. Sci. 2020, 151, 105410. [Google Scholar] [CrossRef] [PubMed]
- Uritu, C.M.; Calin, M.; Maier, S.S.; Cojocaru, C.; Nicolescu, A.; Peptanariu, D.; Constantinescu, C.A.; Stan, D.; Barboiu, M.; Pinteala, M. Flexible cyclic siloxane core enhances the transfection efficiency of polyethylenimine-based non-viral gene vectors. J. Mater. Chem. B 2015, 3, 8250–8267. [Google Scholar] [CrossRef] [PubMed]
- N’Da, D. Prodrug Strategies for Enhancing the Percutaneous Absorption of Drugs. Molecules 2014, 19, 20780–20807. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.B.; Martin, G.P.; Jones, S.A.; Akomeah, F.K. Dermal and Transdermal Drug Delivery Systems: Current and Future Prospects. Drug Deliv. 2006, 13, 175–187. [Google Scholar] [CrossRef]
- Reddy, T.S.; Zomer, R.; Mantri, N. Nanoformulations as a strategy to overcome the delivery limitations of cannabinoids. Phyther. Res. 2023, 37, 1526–1538. [Google Scholar] [CrossRef]
- Kuznetsova, D.A.; Vasilieva, E.A.; Kuznetsov, D.M.; Lenina, O.A.; Filippov, S.K.; Petrov, K.A.; Zakharova, L.Y.; Sinyashin, O.G. Enhancement of the Transdermal Delivery of Nonsteroidal Anti-inflammatory Drugs Using Liposomes Containing Cationic Surfactants. ACS Omega 2022, 7, 25741–25750. [Google Scholar] [CrossRef]
- Ogunsola, O.A.; Kraeling, M.E.; Zhong, S.; Pochan, D.J.; Bronaugh, R.L.; Raghavan, S.R. Structural analysis of “flexible” liposome formulations: New insights into the skin-penetrating ability of soft nanostructures. Soft Matter 2012, 8, 10226. [Google Scholar] [CrossRef]
- Kumar, A. Transferosome: A Recent Approach for Transdermal Drug Delivery. J. Drug Deliv. Ther. 2018, 8, 100–104. [Google Scholar] [CrossRef]
- Sermsaksasithorn, P.; Asawanonda, P.; Phutrakool, P.; Ondee, T.; Payungporn, S.; Pongpirul, K.; Hirankarn, N.; Medicine, S.; Management, C.D.; Botany, P.; et al. Efficacy and Safety of Cannabis Transdermal Patch for Alleviating Psoriasis Symptoms: Protocol for a Randomized Controlled Trial (CanPatch). medRxiv 2023, 1–15. [Google Scholar] [CrossRef]
- Bunge, A.; Vecchia, B. Evaluating the Transdermal Permeability of Chemicals. In Transdermal Drug Delivery Systems; CRC Press: Boca Raton, FL, USA, 2002. [Google Scholar]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).