1. Introduction
The imaging of the cerebrospinal system (cisternography) is a diagnostic procedure intended to determine abnormalities and pathologies of the cerebrospinal fluid (CSF)-filled cavities, which include the subarachnoid space and the ventricular system around and inside the brain and spinal cord [
1]. Pathologies are often caused by ruptures in the membrane surrounding the CSF cavities, e.g., due to trauma or surgery, and they are often accompanied by intracranial hypotension, headaches, nausea, or CSF leakage to the surrounding tissues, in some cases even from the nose or ear [
2]. Unless surgical repair of the rupture can be performed, there is an increased risk of meningitis caused by unresolved CSF leakage [
2]. Successful repair requires the preoperative identification and localization of the leakage site by means of suitable imaging methods.
Cisternography can be performed with various diagnostic imaging techniques, including high-resolution and/or contrast-enhanced computed tomography (CT) [
3], contrast-enhanced or non-contrast-enhanced magnetic resonance imaging (MRI) [
1,
4], or radionuclide cisternography (RNC) by means of nuclear medical imaging methods [
3,
5,
6,
7,
8]. Non-contrast-enhanced MRI is feasible as it is a non-invasive imaging technique, enabling a high-contrast-to-noise ratio, the multiplanar evaluation of volumetric data, and thin-section image acquisition. However, non-contrast-enhanced MRI only provides morphological information without a depiction of the actual CSF flow and thus has a considerable rate of false-negative results [
1,
2,
4]. Furthermore, an MRI examination may be contraindicated, for example in patients with metal implants, like pacemakers. Similarly to MRIs, a non-contrast-enhanced high-resolution CT provides only anatomical information and thus only indirect evidence of CSF leakages or fistulas [
2]. In these cases, the administration of either a CT or an MRI contrast agent (CA) into the CSF cavity by means of a lumbar puncture can help to identify the leak [
2]. Similarly, radionuclide cisternography (RNC) requires the administration of a radiopharmaceutical into the CSF cavity, since the nuclear medical imaging modalities exclusively monitor the distribution of the radiopharmaceutical, although they are commonly combined with CT for anatomical reference and attenuation correction. Both CT and RNC examinations involve radiation exposure.
While every administration into the CSF cavity is invasive, contrast agents for CT and MRI are different from radiopharmaceuticals in terms of their chemical and pharmaceutical composition and the administered amounts. For example, for contrast-enhanced CT cisternography, an iodine containing agent is administered in high amounts of several hundred milligrams of iodine per milliliter [
2,
9]. Only one CT contrast agent, Iohexol (Omnipaque
TM, GE Healthcare, Princeton, NJ, USA), is currently approved for intrathecal administration by the US Food and Drug administration (FDA) and the European Medicines Agency (EMA) and is generally considered to have a good safety profile, although reported adverse events include headaches, pain and aches, neck stiffness and nausea, and, albeit very rarely, seizures [
9,
10,
11]. The overall adverse event incidence has been reported to be 7.4% to 40% [
12]. According to the product information, an application of 4–10 mL of the Iohexol injection solution is recommended for cisternography, with a maximum total dose (10 mL) containing 3500 mg iodine or 7550 mg iohexol in Omnipaque 350
TM [
11]. Similarly to CT contrast agents, MRI contrast agents contain high concentrations of the imaging agent and are based on gadolinium chelates. Gadolinium is a heavy metal, and intraventricular injections of high doses of gadolinium-based contrast agents may cause behavioral and neurological disturbances and histopathological changes [
1]. A review into the safety of the intrathecal administration of gadolinium-based contrast agents, including more than 1000 patients, reported an overall rate of adverse events of 13%, while the incidence of serious adverse events, including serious neurotoxic complications (seizures, coma, and death) was 1% [
12]. Serious adverse events were observed if the contrast agents were applied in doses greater than 1.0 mmol [
12]. While, so far, no MRI contrast agent is approved for cisternography [
4], the contrast agent most commonly used off-label for this purpose is gadopentetate dimeglumine (Magnevist
®), which contains 0.5 mmol/mL of Gd-DTPA and is commonly administered in volumes of 0.5–1.0 mL [
12,
13].
In contrast to CT or MRI contrast agents, the concentration of excipients in radiopharmaceutical formulations is very low, thus ensuring the high-quality safety profiles of radiopharmaceuticals in general [
14]. Cases of adverse events reported for the intrathecal administration of radiopharmaceuticals could be explained by calcium(II) and magnesium(II) ion sequestration caused by the presence of excess chelating agent in some formulations, which by now have been identified as being unsuitable for intrathecal administration [
15]. Therefore, an equimolar amount of calcium(II) ions must always be contained in the radiopharmaceutical formulation intended for intrathecal administration [
15].
Conventional RNC is performed with planar scintigraphy and single-photon emission computed tomography (SPECT). Two different radiopharmaceuticals are commonly used for RNC: [
111In]In-DTPA and [
99mTc]Tc-DTPA. To date, [
111In]In-DTPA is the only radiopharmaceutical approved by the EMA for intrathecal use (In DTPA Injection, Curium (Mallinckrodt), Petten, The Netherlands; and Indium DTPA In111, GE Healthcare Inc., Mississauga, ON, USA) [
16,
17,
18]. RNC with [
111In]In-DTPA has been reported to be reliable for detecting CSF leaks [
6,
19]. Since the imaging modality exclusively detects signals stemming from the radiopharmaceutical that is distributed within the intracranial cavity, while at the same time being combined with a CT to provide an anatomical reference and attenuation correction, RNC is a highly selective imaging method. However, the main limitations of RNC when employing the SPECT technique and using [
111In]In-DTPA are the limited image quality and low spatial resolution, which ultimately lead to RNC often not being favored as the modality of choice in comparison to CT and MRI [
1,
2,
5]. The low image resolution is caused by the high photon energy of the indium-111 radionuclide [
20]. For this reason, [
99mTc]Tc-DTPA has emerged as a feasible alternative to [
111In]In-DTPA, providing superior image quality due to the lower photon energy of technetium-99m [
20]. For intrathecal administration, [
99mTc]Tc-DTPA is prepared from preservative-free calcium trisodium DTPA kits [
21,
22].
Regardless of the applied radionuclide, RNC with SPECT remains inferior to its ‘sister’ imaging technology, which is positron emission tomography (PET). Compared to SPECT, PET exhibits higher sensitivity and better image quality and spatial resolution, and it combines three-dimensional acquisition with high temporal resolution, which makes it feasible for use in the imaging of dynamic processes and the identification of small structures. Therefore, we sought to develop a radiopharmaceutical suitable for PET radionuclide cisternography.
The two most common PET radionuclides, fluorine-18 (half-life 110 min) and gallium-68 (half-life 68 min), are rather short-lived. So far, a study of [
68Ga-]Ga-DOTA has produced promising results for CSF leak detection with PET RNC [
23]. Additionally, an
18F-labeled fluorescein was successfully used for CSF imaging in rats [
24]. Due to the slow CSF circulation dynamics, it takes several hours until the full homogeneous distribution of an agent within the CSF cavity is achieved. Therefore, a longer-lived PET nuclide was deemed favorable for PET RNC. With a half-life of 12.8 h, the PET radionuclide copper-64 is often used for the imaging of slow processes, e.g., via antibody labeling [
25]; thus, it may also be suitable for cisternography intended to localize CSF leaks. Furthermore, compared to short-lived radionuclides like gallium-68, a cisternography agent based on copper-64 would allow for centralized production and long-range distribution.
To prevent preliminary diffusion from the CSF cavity into the blood via the blood–CSF barrier [
26], the [
64Cu]copper(II) ion needs to be chelated by a ligand, similarly to the chelation of the radionuclides in [
111In]In-DTPA and [
99mTc]Tc-DTPA by DTPA. The most suitable and commonly used chelators for copper-64 are macrocycles like DOTA (1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid), TETA (1,4,8,11-tetraazacyclotetradecane-N,N′,N″,N″′-tetraacetic acid), and cyclam (1,4,8,11-tetraazacyclotetradecane) [
25,
27,
28]. Recently, the use of [
64Cu]Cu-albumin for CSF imaging and the evaluation of lymphatic efflux in mice was also reported [
29,
30]. As it is commercially available and due to FDA administration approval [
28], we chose the DOTA ligand as the chelator for the copper-64 radionuclide in the formulation. In 2019, the first successful CSF leak detection with PET radionuclide cisternography using [
64Cu]Cu-DOTA was reported [
31]. Herein, we describe in detail the radiopharmaceutical production of [
64Cu]Cu-DOTA in compliance with standards of good manufacturing practice (GMP) and its use in a clinical case, where PET RNC with [
64Cu]Cu-DOTA proved superior to conventional RNC with [
111In]In-DTPA.
3. Discussion
The evaluation of CSF leaks can be performed with various diagnostic imaging techniques, including CT, MRI, and radionuclide cisternography. The novel PET RNC procedure with [64Cu]Cu-DOTA was proven to be suitable for the identification of CSF leaks and to be superior regarding image resolution compared to conventional SPECT.
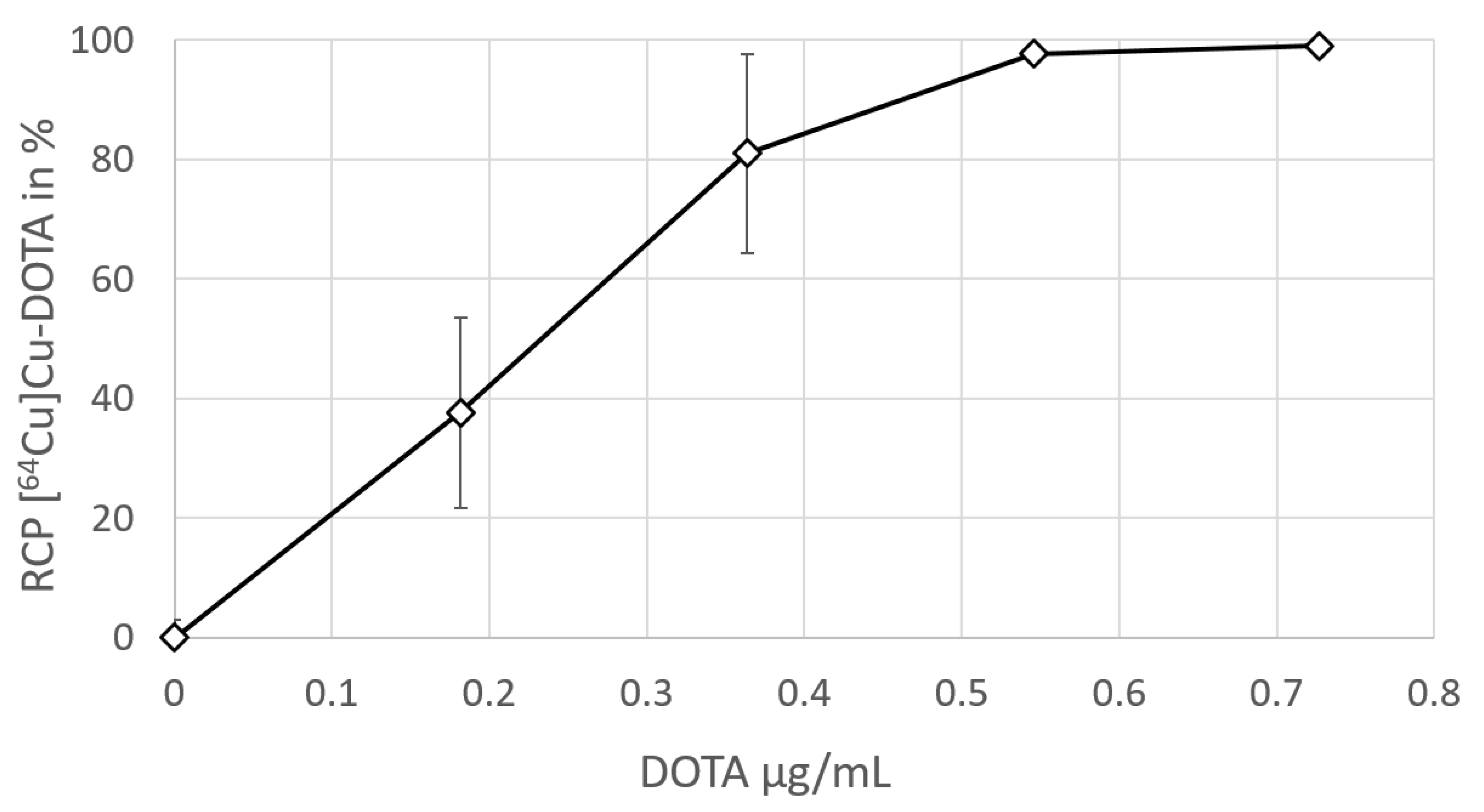
The production and quality control of [64Cu]Cu-DOTA was performed with regard to GMP requirements, using a GMP-certified, commercially available radionuclide precursor [64Cu]Cu-chloride, while further components (DOTA, PBS buffer, and calcium(II) chloride dihydrate) were acquired at chemical or pharmaceutical grade. The radiolabeling of DOTA with [64Cu]Cu-chloride (60 MBq) was performed manually, using 50 µg of DOTA. Although 20 µg of the DOTA precursor was shown to be sufficient for the quantitative radiolabeling of [64Cu]Cu-chloride (60 MBq), 50 µg of DOTA was established as the starting amount for the GMP production batches, in order to ensure quantitative labeling with high certainty.
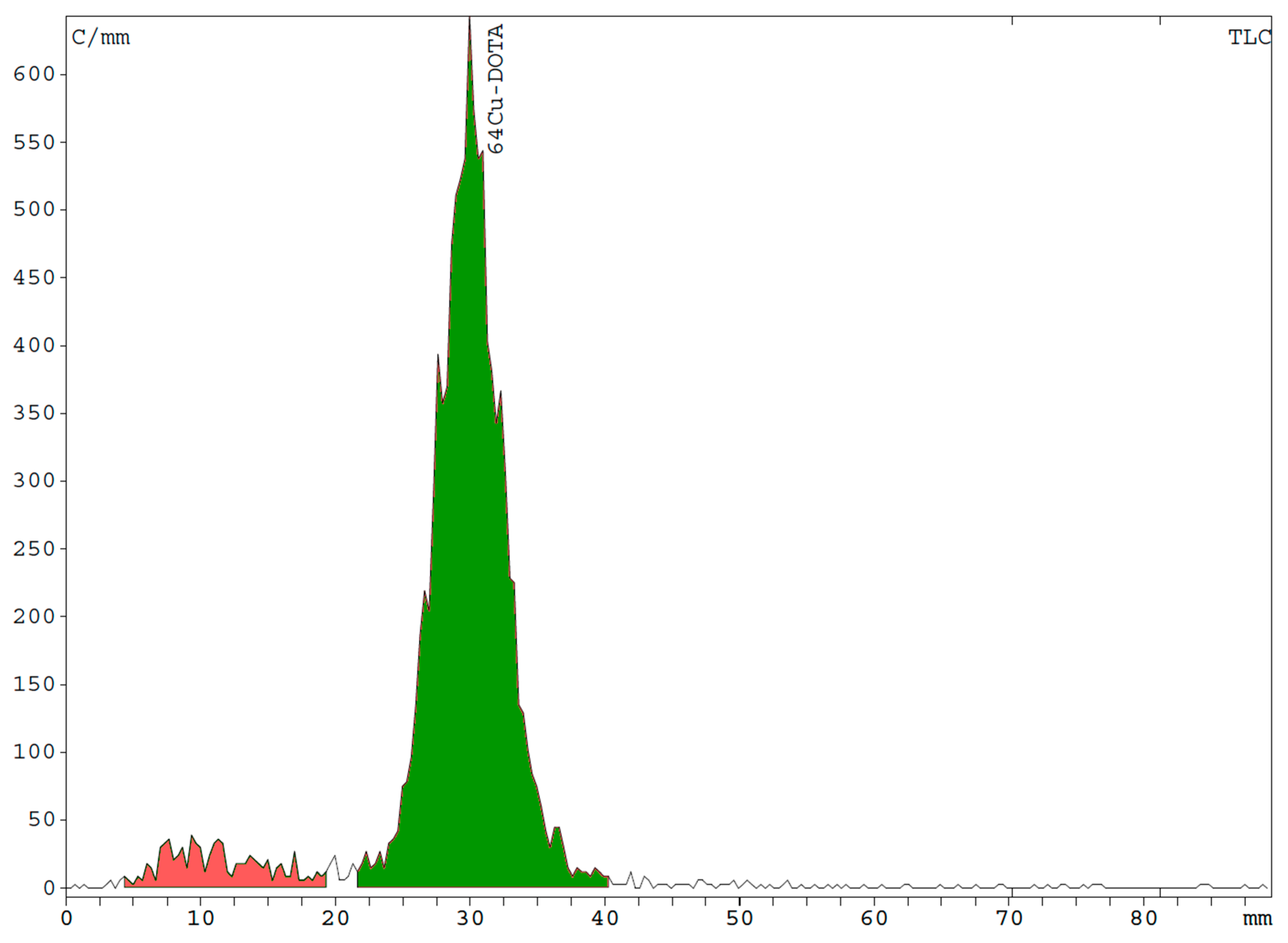
[64Cu]Cu-DOTA was produced in high RCY (≥90%) and RCP (≥90.0%). The PBS buffer exhibited sufficient capacity to buffer up to 400 µL of a [64Cu]Cu-chloride precursor solution (pH 0.7–1.4), providing a final [64Cu]Cu-DOTA product pH of 7.0–7.6. This is relevant because, if a [64Cu]Cu-chloride solution with a lower pH or distinctly higher volume is used, the resulting pH of the final formulation may fall below the specified lower pH limit of 7.0. Thus, we recommend calculating the proton concentration of the [64Cu]Cu-chloride solution prior to production to ensure that the pH will be within the specifications.
[
64Cu]Cu-DOTA exhibited high in vitro stability, which is in accordance to a previously reported study, although another group observed comparably fast transchelation [
27,
35]. In any case, for successful RNC diagnosis, it is sufficient that [
64Cu]Cu-DOTA exhibits high stability in the practically protein-free CSF, thus preventing preliminary excretion of ions from the CSF cavity. Potential transchelation, occurring once the tracer has crossed the CSF–blood barrier, is then negligible.
Due to the direct injection into the CSF cavity, administrations intended for intrathecal use must comply with particularly strict specifications regarding the level of possible impurities and microbial contamination. To ensure sterility and sufficiently low endotoxin levels, all requirements for aseptic production, including production under GMP grade A, the use of sterile compounds suitable for pharmaceutical production whenever applicable, and sterile filtration, were considered and executed with the utmost care. The US Pharmacopeia (USP) proscribes a maximum of ≤14.0 IU/V bacterial endotoxins for radiopharmaceuticals that are administered via intrathecal injection [
21,
36]. Given the total volume of a produced batch of [
64Cu]Cu-DOTA is 10 mL, whereof a maximum of 5 mL is administered per patient, this would set the acceptance level at ≤2.8 IU/mL per application. However, for means of risk reduction, we chose ≤1.0 IU/mL as the acceptance level and all batches complied with this specification.
The presence of excipients that may exhibit pharmacological activity must be strictly avoided whenever possible. That includes excess chelator and unnecessary anti-oxidants or reducing agents, which may be present in [
99mTc]Tc-DTPA formulations [
15]. The addition of calcium(II) chloride in equimolar amounts to the chelator is crucial to ensure that the excess chelator in the final formulation does not lead to the sequestration of calcium(II) or magnesium(II), as has been reported previously for some formulations of [
99mTc]Tc-DTPA [
15]. The sequestration of calcium(II) or magnesium(II) may lead to irreversible blocking of nerve conduction and has reportedly resulted in adverse events [
15]. Surprisingly, we found that, in contrast to [
111In]In-DTPA (Curium), the [
111In]In-DTPA manufactured by GE Healthcare does not seem to contain any Ca(II), according to the product leaflet [
16,
17]. However, adverse events listed for [
111In]In-DTPA (GE Healthcare), like aseptic meningitis and pyrogenic reactions, exhibit an incidence of less than 0.4% and may also be related to the lumbar puncture procedure itself, rather than to the radiopharmaceutical [
16]. In healthy humans, the CSF contains about 1.2 mmol/L of Ca(II) ions in a total volume of roughly 150 mL, equaling a total molar amount of 180 µmol of Ca(II) ions in the CSF [
37]. Thus, less than 0.1% of the Ca(II) ions in the CSF will be sequestrated by the excess DTPA (0.13 µmol) present in the [
111In]In-DTPA produced by GE Healthcare, which may explain the low incidence of adverse events.
Compared to [
111In]In-DTPA, the molar amounts of excess DOTA chelator (0.06 µmol per administration) present in the formulation of [
64Cu]Cu-DOTA as described herein are even lower and are accompanied by an equimolar amount of calcium(II) chloride. In contrast, some [
99mTc]Tc-DTPA formulations, which have been identified as unsuitable for intrathecal administration, contain up to 24 mg (61 µmol) of excess DTPA [
15] and may thus sequestrate up to a third of the Ca(II) ions contained in the CSF, resulting in notable adverse events. Therefore, among the three known radiopharmaceutical formulations suitable for RNC, [
64Cu]Cu-DOTA is the one least likely to cause any pharmacological adverse events caused by excess chelator. Furthermore, formulations of [
99mTc]Tc-DTPA by necessity contain stannous(II) chloride or stannous(II)-DTPA, which may also affect nerve function [
15], while [
64Cu]Cu-DOTA and [
111In]In-DTPA formulations are free of stannous(II) reagents, since
64Cu and
111In labeling do not require reducing agents.
Compared to these three RNC radiopharmaceuticals, the contrast agents used for cisternography with CT (Iohexol) or MRI (Gd-DTPA) contain high concentrations of the imaging substance. Omnipaque® contains 0.37 mmol/mL of Iohexol, Magnevist® contains 0.5 mmol/mL of Gd-DTPA. Thus, both contrast agents carry a significant risk of adverse events. In contrast, our formulation of [64Cu]Cu-DOTA contains DOTA and calcium(II) chloride in concentrations of 0.012 µmol/mL (or 0.06 µmol per administration), meaning a dose that is smaller by a factor of about 1000.
The natural buffer system within the CSF is a carbonate buffer, which keeps the CSF pH constant within the range of 7.32–7.36 [
34,
38]. The PBS buffer system used for [
64Cu]Cu-DOTA is similar to the one used for [
111In]In-DTPA (Curium). Although a PBS buffer of a higher concentration would exhibit a higher capacity for buffering [
64Cu]Cu-chloride solutions of excessive acidity and volume, we chose not to exceed a PBS concentration of 0.02 mmol/mL (meaning a total molar amount of phosphate 0.09 mmol per administration) in order to avoid negative influences on the CSF osmolarity and ion concentration.
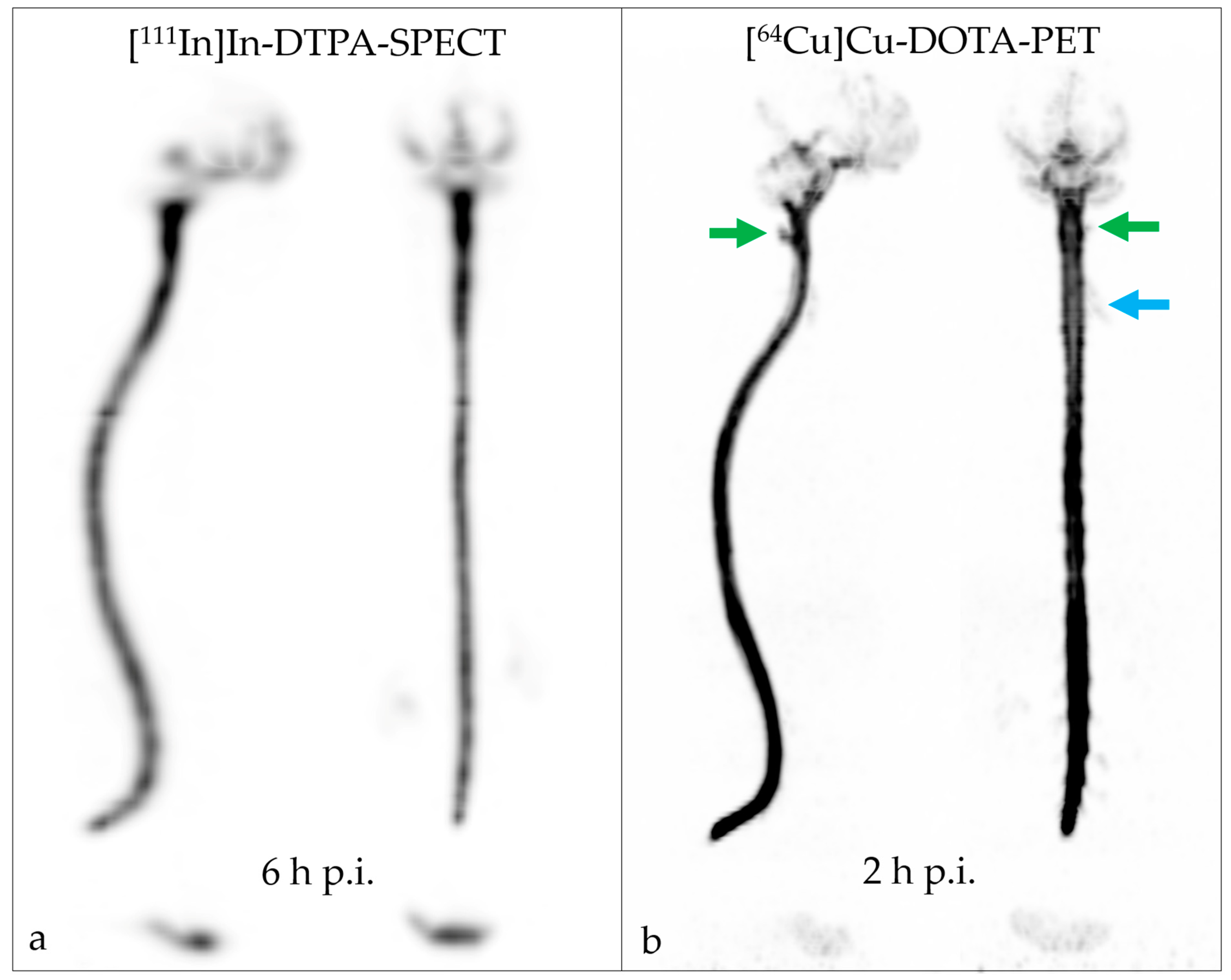
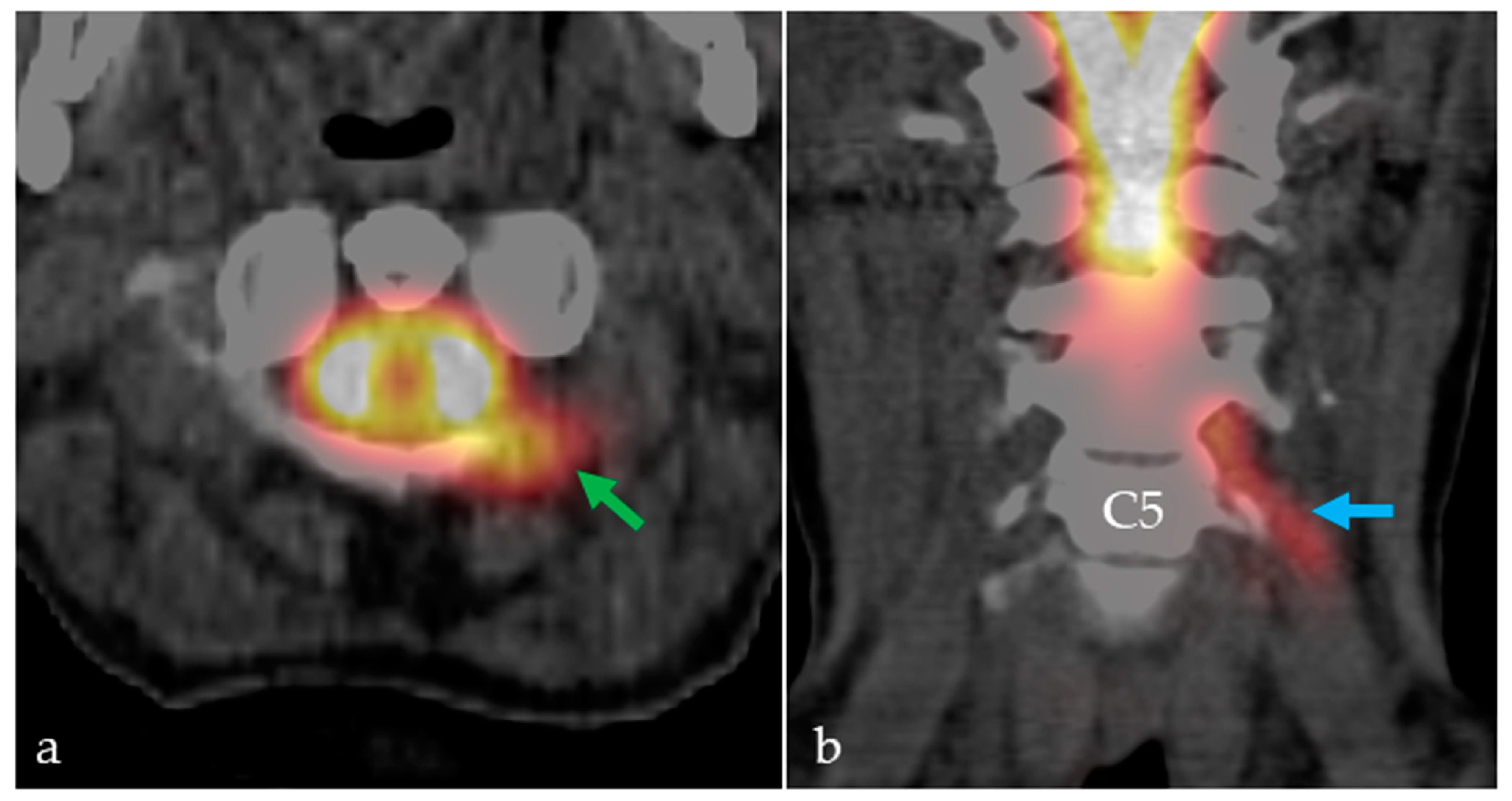
No adverse events were observed following the intrathecal application of [64Cu]Cu-DOTA. We demonstrated that the distinctly improved image resolution of the PET modality led to the identification of a CSF leak, while SPECT RNC with [111In]In-DTPA yielded a false-negative result. The intracranial distribution of [64Cu]Cu-DOTA in the CSF space was faster than that of [111In]In-DTPA; the tracers reached the skull base, cerebellum, and fourth ventricle two hours and six hours after the lumbar injection, respectively. Distribution over the cerebral convexities was seen on [64Cu]Cu-DOTA PET RNC after 6 h and on [111In]In-DTPA SPECT RNC only in the next-day image (22 h). The cervical CSF leak was already apparent on the [64Cu]Cu-DOTA PET RNC images acquired 40 min after injection but was best seen after 2 h and 6 h.
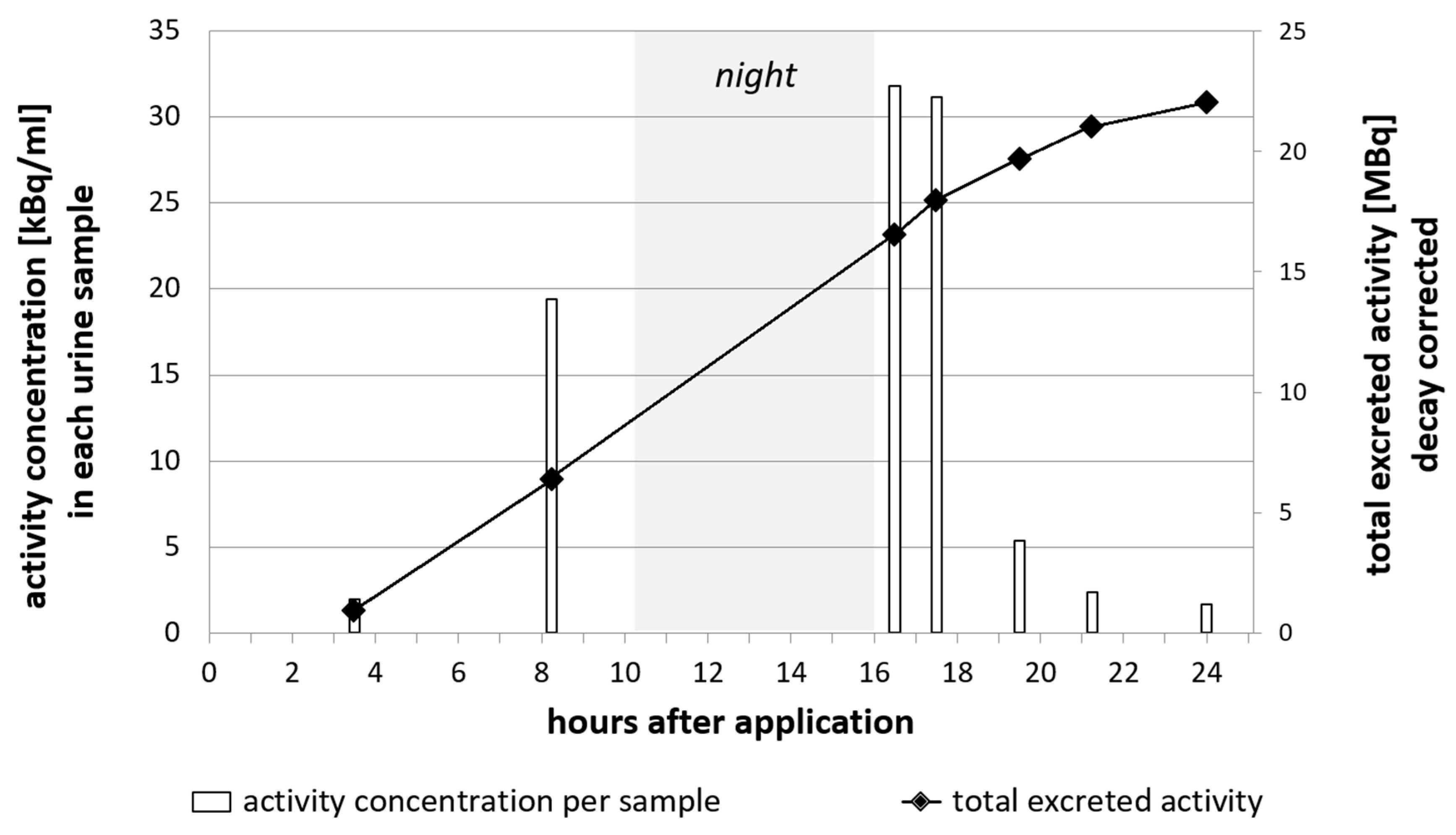
CSF fluid is produced at a rate of about 500 mL/day, meaning that the entire CSF volume (150–170 mL) is renewed every 5–7 h [
38]. The main portion of the CSF volume is reabsorbed by the tissues of the brain, while a smaller part portion into venous sinuses and lymphatic vessels [
39]. Substances that are administered via intrathecal injection can be expected to leave the intracranial cavity over time and be excreted via the blood stream and subsequent renal and/or hepatobiliary pathways. In total, more than 70% of the total injected activity of [
64Cu]Cu-DOTA was found in the urine, indicating renal excretion as the major route. This is comparable to [
111In]In-DTPA, wherein two third of the radiopharmaceutical activity are cleared via the kidneys [
40], while 90% of Iohexol are cleared through the kidneys [
9].
The single case reported herein serves as a proof-of-concept of the superiority of [64Cu]Cu-DOTA PET RNC over [111In]In-DTPA SPECT RNC. To further evaluate the potential of [64Cu]Cu-DOTA, not just for CSF leak detection but also for studying further abnormalities and fluid characteristics, studies on a larger number of patients are of course required first. The authors plan to undertake these studies in the near future.
4. Materials and Methods
4.1. [64Cu]Cu-Chloride Solution
The [64Cu]Cu-chloride solution was purchased as a radiopharmaceutical precursor of GMP grade from BIONT, a.s., Bratislava, Slovakia. [64Cu]Cu-chloride was delivered as a clear, colorless solution in a conical glass vial, exhibiting a pH range of 0.7–1.4, a radionuclide purity of ≥99.5%, and a radiochemical purity of ≥95.0%.The delivered batches of [64Cu]Cu-chloride solution exhibited varying activity concentrations between 583–901 MBq/mL; therefore, the volume required for [64Cu]Cu-DOTA production was calculated prior to synthesis.
4.2. Preparation of PBS Buffer, Calcium(II) Chloride, and DOTA Stock Solution
All solutions were prepared in a biosafety cabinet (GMP grade A). Weighing of substances was performed using sterile plastic spatulas to avoid metal contamination. The PBS buffer (pH 7.7–7.9) was prepared by dissolving 298 mg disodium hydrogen phosphate (EMSURE® Reag. Ph Eur, Merck KGaA, Darmstadt, Germany), 25 mg potassium dihydrogen phosphate (EMSURE® Reag. Ph Eur, Merck KGaA, Darmstadt, Germany), and 1.0 g of sodium chloride (99.99 Suprapur®, Merck KGaA, Darmstadt, Germany) in 125 mL of sterile water of ultrapure grade (ULTREX™, J. T. BakerTM, Avantor™ Performance Materials, Center Valley, PA, USA).
The DOTA stock solution (5 mg/mL) was prepared by dissolving 50 mg of DOTA (Sigma Aldrich, Merck KGaA, Darmstadt, Germany, purity (CHN) ≥ 97.0%) in 10 mL water of ultrapure grade. Calcium(II) chloride solution (0.75 mg/mL) was prepared by dissolving 12 mg calcium(II) chloride dihydrate (tested according to Ph. Eur., Merck KGaA, Darmstadt, Germany) in 16 mL of sterile ultrapure water.
All stock solutions were freshly prepared on the day of production. For batches produced 24 h after delivery, the solutions were kept overnight in the fridge (4–8 °C).
4.3. Small-Scale Test Batch Production for the Determination of Radiolabeling Efficiency
A stock solution (0.01 mg/mL) of DOTA was prepared using ultrapure water. To an aliquot of buffer (500 µL) in a reaction tube was added a respective volume (0–50 µL) of the DOTA stock solution, containing 0–0.5 µg. Subsequently, the relevant volume of water (50–0 µL) was added to keep the total volume of the reaction mixture at 550 µL. The buffered solution was homogenized by brief shaking. Subsequently, the reaction tube was placed in a lead shield and an aliquot of 8 µL of [64Cu]Cu-chloride solution per tube, containing 3.5–4.5 MBq at time of labeling, was added to the buffered solution. Activities were determined using a dose calibrator (ISOMED 2010, NUVIA Instruments, Dresden, Germany). The reaction tube was placed in a heating block (100 °C, Ministir II, Zinsser Analytics GmbH, Frankfurt, Germany) for 15 min. Subsequently, the reaction was allowed to cool to room temperature and a sample (5 µL) was withdrawn for radio TLC analysis. The experiment was performed in triplicates for each defined amount of DOTA stock solution.
4.4. Full-Scale Test Batch Production for the Determination of the Precursor Amount
Four batches mimicking the conditions of a full-scale labeling reaction were produced, using different starting amounts of DOTA, in order to determine the necessary precursor amount. A sterile evacuated glass vial sealed with a rubber cap (Mallinckrodt) was placed in a lead shield. PBS buffer (2 mL) was placed in a sterile reaction tube with a conical bottom. From a stock solution (1 mg/mL) of DOTA in 2 µL (2 µg) of ultrapure water, 10 µL (10 µg) or 20 µL (20 µg) was removed and mixed with the PBS. Subsequently, the solution was withdrawn with a syringe, equipped with a metal cannula, and transferred into the glass vial. An equal volume of air was withdrawn with the syringe, to keep the air pressure within the glass vial constant.
Then, 3 mL of PBS buffer was placed into a second sterile reaction tube. Using a pipette with sterile pipette tips, an aliquot of the [64Cu]Cu-chloride solution was withdrawn from the delivery vial and transferred into the PBS solution. For test batches nos. 1, 2, and 3, which were produced on the day of delivery, 120 µL (60 ± 5 MBq) of [64Cu]Cu-chloride was removed. For test batch no. 4, produced the day after delivery, 400 µL (60 ± 5 MBq) of [64Cu]Cu-chloride was removed. Using a syringe equipped with a metal cannula, the buffered [64Cu]Cu-chloride solution was transferred into the glass vial. The glass vial was placed in a heating block (100 °C, Ministir II, Zinsser Analytics GmbH Frankfurt, Germany) for 15 min. Samples for RCP analysis were withdrawn after letting the vial cool to room temperature.
4.5. Stability Determination
From test batch no. 3, an aliquot of 100 µL was removed and mixed with 400 µL of human serum (from human male AB plasma, USA origin, sterile-filtered, Merck KGaA, Darmstadt, Germany). Another aliquot of 100 µL of test batch no. 3 was mixed with 400 µL of fresh cerebrospinal fluid taken from a patient. The samples were incubated at 37 °C and aliquots for radio TLC and HPLC analyses were removed after 12 h and 24 h. The sample incubated with human serum was centrifuged (3500 rpm, 685 rcf, 5 min) prior to the HPLC analysis, in order to remove insoluble parts.
Another aliquot (1000 µL, equaling a content of 4 µg or 0.01 µmol of DOTA precursor) of test batch no. 3 was mixed with 100 µL (0.51 µmol) of calcium(II) chloride solution (0.75 mg/mL), resulting in an excess of Calcium(II):DOTA of 500:1; then, it was kept at room temperature. Aliquots for the radio TLC and radio HPLC analyses were removed after 12 h and 24 h.
4.6. GMP Production
The radiolabeling was performed manually in a biosafety cabinet (GMP grade A). In preparation, a sterile evacuated glass vial sealed with a rubber cap (Mallinckrodt) and two sterile reaction tubes with conical bottoms (5 mL) were placed in lead shields. Then, 3 mL of PBS buffer was placed into the first sterile reaction tube, and 2 mL of PBS buffer was placed into the second sterile reaction tube. Using an autoclaved pipette with sterile pipette tips, an aliquot of [64Cu]Cu-chloride solution (65–250 µL, 60 ± 5 MBq) was withdrawn from the delivery vial and transferred into the first sterile reaction tube containing 3 mL of PBS solution. In the second sterile reaction tube, an aliquot (10 µL) of DOTA stock solution (5 mg/mL) was mixed with the PBS (2 mL). Then, both the [64Cu]Cu-chloride/PBS solution and, subsequently, the DOTA/PBS solution were withdrawn from the reaction tubes, using a syringe (10 mL) equipped with a metal cannula. The combined solutions were then transferred into the sterile evacuated glass vial, followed by the removal of an aliquot of air (5 mL) to keep the pressure within the vial constant. The glass vial was placed in a heating block (100 °C, Ministir II, Zinsser Analytics GmbH Frankfurt, Germany) for 15 min.
During the heating of the reaction, 5 mL of PBS buffer was placed into a third sterile reaction tube with conical bottom (5 mL). Then, 12 µL of calcium(II) chloride solution (0.75 mg/mL) was transferred into the PBS using an autoclaved pipette with sterile pipette tips.
After letting the reaction cool to room temperature, the entire volume of the vial (5 mL) was withdrawn using a 20 mL syringe and a metal cannula. A second sterile evacuated vial, which had been equipped with a short cannula and a vented sterile filter (0.22 µm) and a long cannula and a vented sterile filter (0.22 µm), was placed in a lead shield. The entire volume of the [64Cu]Cu-DOTA formulation was slowly passed through the sterile filter on the long cannula into the vial. Then, using the same syringe and metal cannula, the calcium(II) chloride/PBS solution was withdrawn from the reaction tube. The syringe was placed in the same sterile filter and the solution was slowly passed through the filter into the vial. Afterwards, the vial was briefly shaken to ensure homogenization.
The vented filter was removed from the long cannula and a sample (2 mL) was withdrawn for quality control.
4.7. Quality Control
Radiochemical purity (RCP) was determined via radio HPLC using a eurosphere 125 × 4 mm column (100–5 C18, Knauer) and the following gradient: 0.0–2.0 min 100% B, 2.0–5.0 min 100% B → 80% B, 5.0–7.0 min 80% B → 65% B, 7.0–9.0 min 65% B → 0% B, 9.0–11.0 min 100% A, 11.0–11.05 min 0.0% B → 100% B, 11.05–13.00 min 100% B, with A being acetonitrile and B being triethylammonium phosphate solution (50 mM, pH 3.6; prepared from mixing 855 µL orthophosphoric acid, 1.26 g trimethylamine in 250 mL of water). This method was established in the same way as a previously published protocol [
35].
Additionally, radio TLC was performed using silica gel plates on aluminum (1 cm × 6 cm Merck, Darmstadt, Germany) and an eluent of methanol/ammonium acetate (77 g/L) (1/1 v/v).
4.8. [111In]In-DTPA and [64Cu]Cu-DOTA Administration and Imaging Protocol
Injection solutions of [111In]In-DTPA (1 mL, 37 MBq) and [64Cu]Cu-DOTA (5 mL, 30 MBq) were administered to the patient on separate days via lumbar puncture between vertebrae L2 and L3. Following the [111In]In-DTPA administration, SPECT acquisitions were performed at 2 h, 6m and 22 h p.i. Following [64Cu]Cu-DOTA administration, PET/CT acquisitions were performed at 40 min, 2 h and 6 h p.i.
4.9. Urine Sampling for Excretion Profiling
Urine samples were collected from two patients at irregular timepoints after the intrathecal administration of [64Cu]Cu-DOTA. Sampling was performed between 1.75 h and 24 h p.i. In total, seven samples were taken from patient 1 and six from patient 2. The total volume of each urine sample was determined. The samples were homogenized by shaking prior to withdrawing an aliquot of 100 µL. The aliquot was transferred into a test tube and the activity in 100 µL was determined using a gamma ray spectrometer (Cryo-Pulse5 plus, Mirion Technologies (Canberra) GmbH, Hamburg, Germany). The total activity in each urine sample was calculated by multiplying the activity concentration by the total sample volume.



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}