
Unveiling the Role of PAR 1: A Crucial Link with Inflammation in Diabetic Subjects with COVID-19

 , , , and
, , , and
Abstract
1. Introduction
2. Results
2.1. Clinical Characteristics
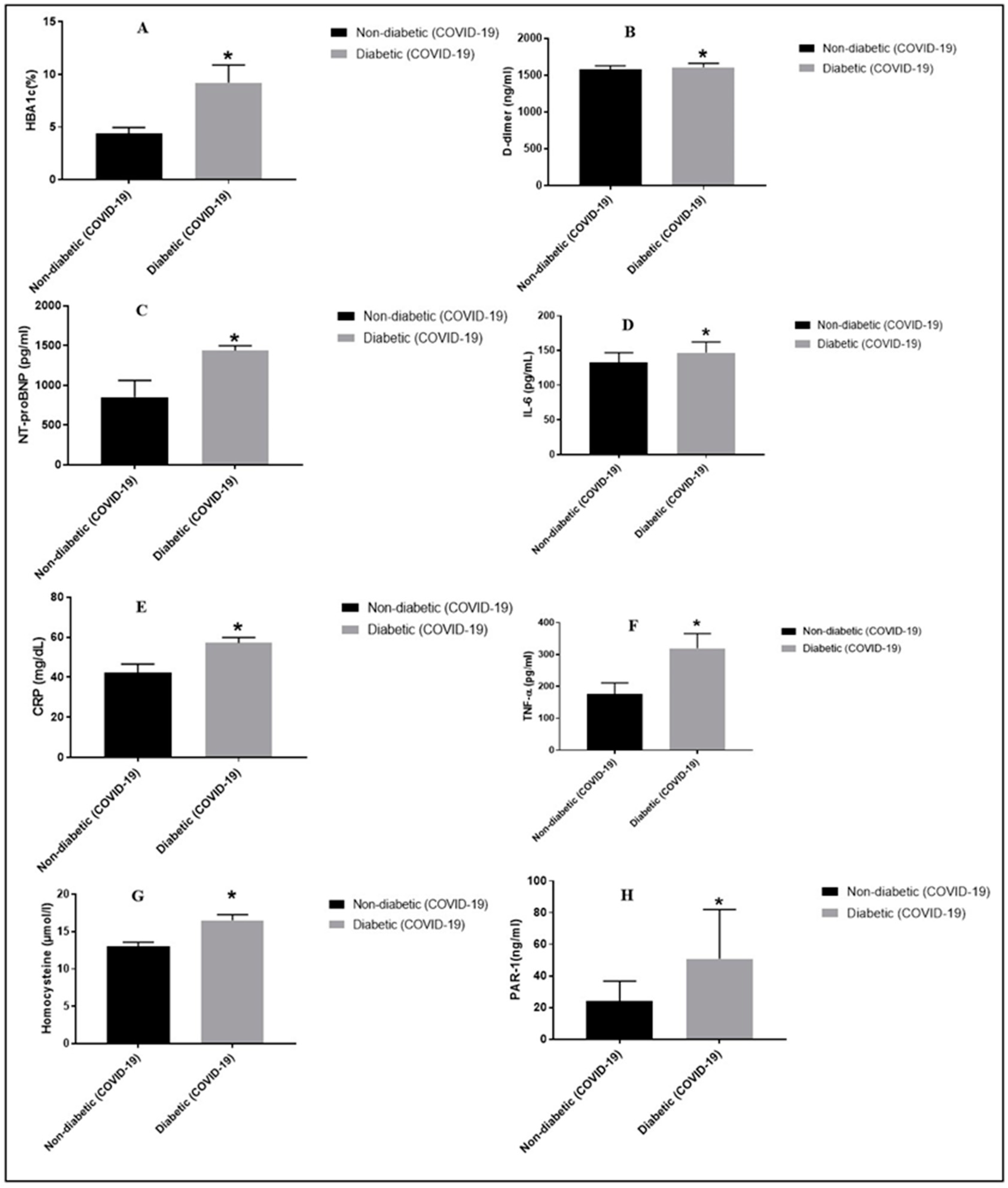
2.2. Comparison of DM Patients and Healthy Controls Subjects
2.3. Spearman Correlation of PAR-1 with Inflammatory Markers and Clinical Variables in COVID-19 DM Patients
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Biochemical Assessment
4.3. Statistical Analysis
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Waisy, A.S.; Al-Fahdawi, S.; Mohammed, M.A.; Abdulkareem, K.H.; Mostafa, S.A.; Maashi, M.S.; Arif, M.; Garcia-Zapirain, B. COVID-CheXNet: Hybrid deep learning framework for identifying COVID-19 virus in chest X-rays images. Soft Comput. 2023, 27, 2657–2672. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.; Kumar, S.; Guleria, K. Outbreak trends of coronavirus disease–2019 in India: A prediction. Disaster Med. Public Health Prep. 2000, 14, e33–e38. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2023. Available online: https://covid19.who.int/ (accessed on 1 February 2024).
- Coccia, M. Improving preparedness for next pandemics: Max level of COVID-19 vaccinations without social impositions to design effective health policy and avoid flawed democracies. Environ. Res. 2022, 213, 113566. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Delgado, A.; Bontempi, E.; Coccia, M.; Kumar, M.; Farkas, K.; Domingo, J.L. SARS-CoV-2 and other pathogenic microorganisms in the environment. Environ. Res. 2021, 201, 111606. [Google Scholar] [CrossRef] [PubMed]
- Benati, I.; Coccia, M. Global analysis of timely COVID-19 vaccinations: Improving governance to reinforce response policies for pandemic crises. Int. J. Health Gov. 2022, 27, 240–253. [Google Scholar] [CrossRef]
- Bontempi, E.; Coccia, M. International trade as critical parameter of COVID-19 spread that outclasses demographic, economic, environmental, and pollution factors. Environ. Res. 2021, 201, 111514. [Google Scholar] [CrossRef] [PubMed]
- Alimohamadi, Y.; Sepandi, M.; Taghdir, M.; Hosamirudsari, H. Determine the most common clinical symptoms in COVID-19 patients: A systematic review and meta-analysis. J. Prev. Med. Hyg. 2020, 61, E304–E312. [Google Scholar] [CrossRef] [PubMed]
- Rauf, A.; Abu-Izneid, T.; Olatunde, A.; Ahmed Khalil, A.; Alhumaydhi, F.A.; Tufail, T.; Shariati, M.A.; Rebezov, M.; Almarhoon, Z.M.; Mabkhot, Y.N.; et al. COVID-19 pandemic: Epidemiology, etiology, conventional and non-conventional therapies. Int. J. Environ. Res. Public Health 2020, 17, 8155. [Google Scholar] [CrossRef] [PubMed]
- Meftahi, G.H.; Jangravi, Z.; Sahraei, H.; Bahari, Z. The possible pathophysiology mechanism of cytokine storm in elderly adults with COVID-19 infection: The contribution of “inflame-aging”. Inflamm. Res. 2020, 69, 825–839. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; González-Bernal, J.J.; Sánchez-Serrano, N.; Navascués, L.J.; Ascaso-Del-Río, A.; Mielgo-Ayuso, J. Physical exercise as a multimodal tool for COVID-19: Could it be used as a preventive strategy? Int. J. Environ. Res. Public Health 2020, 17, 8496. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Bae, J.H.; Kwon, H.S. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Hyperglycemia and COVID-19: What was known and what is really new? Diabetes Res. Clin. Pract. 2020, 167, 108383. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.G.; Evangelopoulos, A.; Kounatidis, D.; Stratigou, T.; Christodoulatos, G.S.; Karampela, I.; Dalamaga, M. Diabetes mellitus and SARS-CoV-2 infection: Pathophysiologic mechanisms and implications in management. Curr. Diabetes Rev. 2021, 17, e123120189797. [Google Scholar] [CrossRef] [PubMed]
- Bigdelou, B.; Sepand, M.R.; Najafikhoshnoo, S.; Negrete, J.A.T.; Sharaf, M.; Ho, J.Q.; Sullivan, I.; Chauhan, P.; Etter, M.; Shekarian, T.; et al. COVID-19 and preexisting comorbidities: Risks, synergies, and clinical outcomes. Front. Immunol. 2022, 13, 890517. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, R.B.; Botelho, B.G.; Hollanda, J.V.G.; Ferreira, L.V.L.; Junqueira de Andrade, L.Z.; Oei, S.S.M.L.; Mello, T.S.; Muxfeldt, E.S. COVID-19 and the cardiovascular system: A comprehensive review. J. Hum. Hypertens. 2021, 35, 4–11. [Google Scholar] [CrossRef]
- Heuberger, D.M.; Schuepbach, R.A. Protease-activated receptors (PARs): Mechanisms of action and potential therapeutic modulators in PAR-driven inflammatory diseases. Thromb. J. 2019, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Austin, K.M.; Covic, L.; Kuliopulos, A. Matrix metalloproteases and PAR1 activation. Blood J. Am. Soc. Hematol. 2013, 121, 431–439. [Google Scholar] [CrossRef]
- Hou, H.H.; Wang, H.C.; Cheng, S.L.; Chen, Y.F.; Lu, K.Z.; Yu, C.J. MMP-12 activates protease-activated receptor-1, upregulates placenta growth factor, and leads to pulmonary emphysema. Am. J. Physiol. Lung Cell. Mol. Physiol. 2018, 315, L432–L442. [Google Scholar] [CrossRef]
- Fang, X.; Liao, R.; Yu, Y.; Li, J.; Guo, Z.; Zhu, T. Thrombin induces secretion of multiple cytokines and expression of protease-acti-vated receptors in mouse mast cell line. Mediat. Inflamm. 2019. [Google Scholar] [CrossRef] [PubMed]
- Motta, J.P.; Denadai-Souza, A.; Sagnat, D.; Guiraud, L.; Edir, A.; Bonnart, C.; Sebbag, M.; Rousset, P.; Lapeyre, A.; Seguy, C.; et al. Active thrombin produced by the intestinal epithelium controls mucosal biofilms. Nat. Commun. 2019, 10, 3224. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.S.; Probst, C.K.; Brazee, P.L.; Rotile, N.J.; Blasi, F.; Weinreb, P.H.; Black, K.E.; Sosnovik, D.E.; Van Cott, E.M.; Violette, S.M.; et al. Uncoupling of the profibrotic and hemostatic effects of thrombin in lung fibrosis. JCI Insight 2017, 2, e86608. [Google Scholar] [CrossRef] [PubMed]
- Antoniak, S.; Owens, A.P.; Baunacke, M.; Williams, J.C.; Lee, R.D.; Weithäuser, A.; Sheridan, P.A.; Malz, R.; Luyendyk, J.P.; Esserman, D.A.; et al. PAR-1 contributes to the innate immune response during viral infection. J. Clin. Investig. 2013, 123, 1310–1322. [Google Scholar] [CrossRef] [PubMed]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.; Petrey, A.C.; Tolley, N.D.; Guo, L.; Cody, M.; et al. Platelet gene expression and function in patients with COVID-19. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and multiorgan response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, P.; Kaushal, J. Epidemic trend of COVID-19 transmission in India during lockdown1 phase. J. Community Health 2020, 45, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.C.; Derian, C.K.; Andrade-Gordon, P.; Hoekstra, W.J.; McComsey, D.F.; White, K.B.; Poulter, B.L.; Addo, M.F.; Cheung, W.M.; Damiano, B.P.; et al. Discovery and optimization of a novel series of thrombin receptor (par-1) antagonists: Potent, selective peptide mimetics based on indole and indazole templates. J. Med. Chem. 2001, 44, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Zhang, W.; Mulholland, M. Thrombin and PAR-1-AP increase proinfammatory cytokine expression in C6 cells1. J. Surg. Res. 2005, 129, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tang, Z.Z.; Zhang, Y.M.; Kong, L.; Xiao, W.F.; Ma, T.F.; Liu, Y.W. Thrombin/PAR-1 activation induces endothelial damages via NLRP1 inflammasome in gestational diabetes. Biochem. Pharmacol. 2020, 175, 113849. [Google Scholar] [CrossRef]
- Fortmann, S.D.; Patton, M.J.; Frey, B.F.; Tipper, J.L.; Reddy, S.B.; Vieira, C.P.; Hanumanthu, V.S.; Sterrett, S.; Floyd, J.L.; Prasad, R.; et al. Circulating SARS-CoV-2+ megakaryocytes are associated with severe viral infection in COVID-19. Blood Adv. 2023, 7, 4200–4214. [Google Scholar] [CrossRef] [PubMed]
- Waasdorp, M.; Duitman, J.; Florquin, S.; Spek, C.A. Protease-activated receptor-1 deficiency protects against streptozotocin-induced diabetic nephropathy in mice. Sci. Rep. 2016, 6, 33030. [Google Scholar] [CrossRef] [PubMed]
- Knapp, E.A.; Dong, Y.; Dunlop, A.L.; Aschner, J.L.; Stanford, J.B.; Hartert, T.; Teitelbaum, S.L.; Hudak, M.L.; Carroll, K.; O’Connor, T.G.; et al. Environmental Influences on Child Health Outcomes. Changes in BMI during the COVID-19 pandemic. Pediatrics 2022, 150, e2022056552. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx. New York. Metab. Clin. Exp. 2020, 108, 154262. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. Mild versus severe COVID-19: Laboratory markers. Int. J. Infect. Dis. 2020, 95, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, K.I.; Liu, S.; Yan, Z.; Xu, C.; Qiao, Z. Plasma CRP level is positively associated with the severity of COVID-19. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Kesmez Can, F.; Özkurt, Z.; Öztürk, N.; Sezen, S. Effect of IL-6, IL-8/CXCL8, IP-10/CXCL 10 levels on the severity in COVID 19 infection. Int. J. Clin. Pract. 2021, 75, e14970. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wang, P.; Jia, M.; Li, Q.; Zhang, A.; Zhou, Q. Baicalin alleviates thrombin-induced inflammation in vascular smooth muscle cells. BioMed Res. Int. 2022, 2022, 5799308. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Hu, K.; Li, Y.; Lu, C.; Ling, K.; Cai, C.; Wang, W.; Ye, D. Targeting TNF-α for COVID-19: Recent advanced and controversies. Front. Public Health 2022, 10, 833967. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Jiang, D.; Wen, X.S.; Cheng, X.C.; Sun, M.; He, B.; You, L.N.; Lei, P.; Tan, X.W.; Qin, S.; et al. Prognostic value of NT-proBNP in patients with severe COVID-19. Respir. Res. 2020, 21, 83. [Google Scholar] [CrossRef] [PubMed]
- Keskin, A.; Ustun, U.; Aci, R.; Duran, U. Homocysteine as a marker for predicting disease severity in patients with COVID-19. Biomark. Med. 2022, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A.A.; Kathuria, A.; Al Mahmeed, W.; Al-Rasadi, K.; Al-Alawi, K.; Banach, M.; Banerjee, Y.; Ceriello, A.; Cesur, M.; Cosentino, F.; et al. Post-COVID syndrome, inflammation, and diabetes. J. Diabetes Its Complicat. 2022, 36, 108336. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | T2DM Patients with COVID-19 | Non-DM Patients with COVID-19 | p Value |
|---|---|---|---|
| n | 50 | 50 | - |
| Age (in years) | 41.38 ± 7.58 | 39.83 ± 7.23 | 0.3655 |
| Gender (Men/Women) | 29/21 | 26/24 | - |
| BMI (kg/m2) | 29.21 ± 3.52 | 21.30 ± 2.11 | <0.0001 |
| HbA1c (%) | 9.23 ± 1.66 | 4.39 ± 0.57 | <0.0001 |
| D-dimer (ng/mL) | 1605.08 ± 56.57 | 1578.66 ± 48.72 | 0.0306 |
| NT-proBNP (pg/mL) | 1438.18 ± 59.48 | 852.82 ± 207.26 | <0.0001 |
| IL-6 (pg/mL) | 146.84 ± 15.43 | 133.03 ± 13.67 | <0.0001 |
| CRP (mg/dL) | 57.13 ± 2.67 | 42.4 ± 4.15 | <0.0001 |
| TNF-α (pg/mL) | 319.09 ± 46.28 | 175.29 ± 35.10 | <0.0001 |
| Homocysteine (µmol/L) | 16.50 ± 0.78 | 13.02 ± 0.57 | <0.0001 |
| PAR-1 (ng/mL) | 50.76 ± 31.21 | 23.99 ± 12.68 | <0.0001 |
| Variables | Univariate Analysis | |
|---|---|---|
| r | p Value | |
| PAR-1 | ||
| Age (years) | 0.4712 | 0.0006 |
| BMI (kg/m2) | 0.9989 | <0.0001 |
| HbA1c (%) | 0.9987 | <0.0001 |
| D-dimer (ng/mL) | 0.9994 | <0.0001 |
| NT-proBNP (pg/mL) | 0.9994 | <0.0001 |
| CRP (mg/dL) | 0.9995 | <0.0001 |
| IL-6 (pg/mL) | 0.9994 | <0.0001 |
| TNF-α (pg/mL) | 0.9997 | <0.0001 |
| Homocysteine (µmol/L) | 0.9993 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, R.; Singh, V.; Ahmad, M.A.; Pasricha, C.; Kumari, P.; Singh, T.G.; Kaur, R.; Mujwar, S.; Wani, T.A.; Zargar, S. Unveiling the Role of PAR 1: A Crucial Link with Inflammation in Diabetic Subjects with COVID-19. Pharmaceuticals 2024, 17, 454. https://doi.org/10.3390/ph17040454
Singh R, Singh V, Ahmad MA, Pasricha C, Kumari P, Singh TG, Kaur R, Mujwar S, Wani TA, Zargar S. Unveiling the Role of PAR 1: A Crucial Link with Inflammation in Diabetic Subjects with COVID-19. Pharmaceuticals. 2024; 17(4):454. https://doi.org/10.3390/ph17040454
Chicago/Turabian StyleSingh, Ravinder, Varinder Singh, Md. Altamash Ahmad, Chirag Pasricha, Pratima Kumari, Thakur Gurjeet Singh, Rupinder Kaur, Somdutt Mujwar, Tanveer A. Wani, and Seema Zargar. 2024. "Unveiling the Role of PAR 1: A Crucial Link with Inflammation in Diabetic Subjects with COVID-19" Pharmaceuticals 17, no. 4: 454. https://doi.org/10.3390/ph17040454
APA StyleSingh, R., Singh, V., Ahmad, M. A., Pasricha, C., Kumari, P., Singh, T. G., Kaur, R., Mujwar, S., Wani, T. A., & Zargar, S. (2024). Unveiling the Role of PAR 1: A Crucial Link with Inflammation in Diabetic Subjects with COVID-19. Pharmaceuticals, 17(4), 454. https://doi.org/10.3390/ph17040454