
Can Glatiramer Acetate Prevent Cognitive Impairment by Modulating Oxidative Stress in Patients with Multiple Sclerosis?

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Results
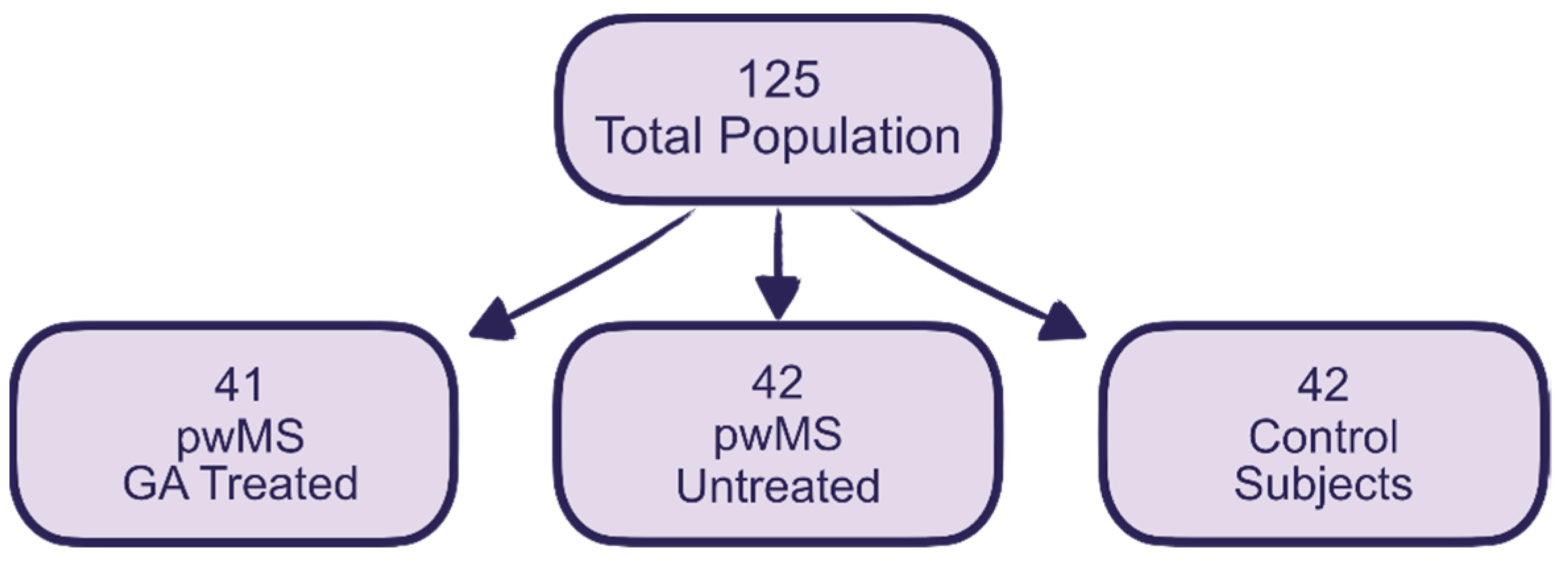
2.1. Sample Description
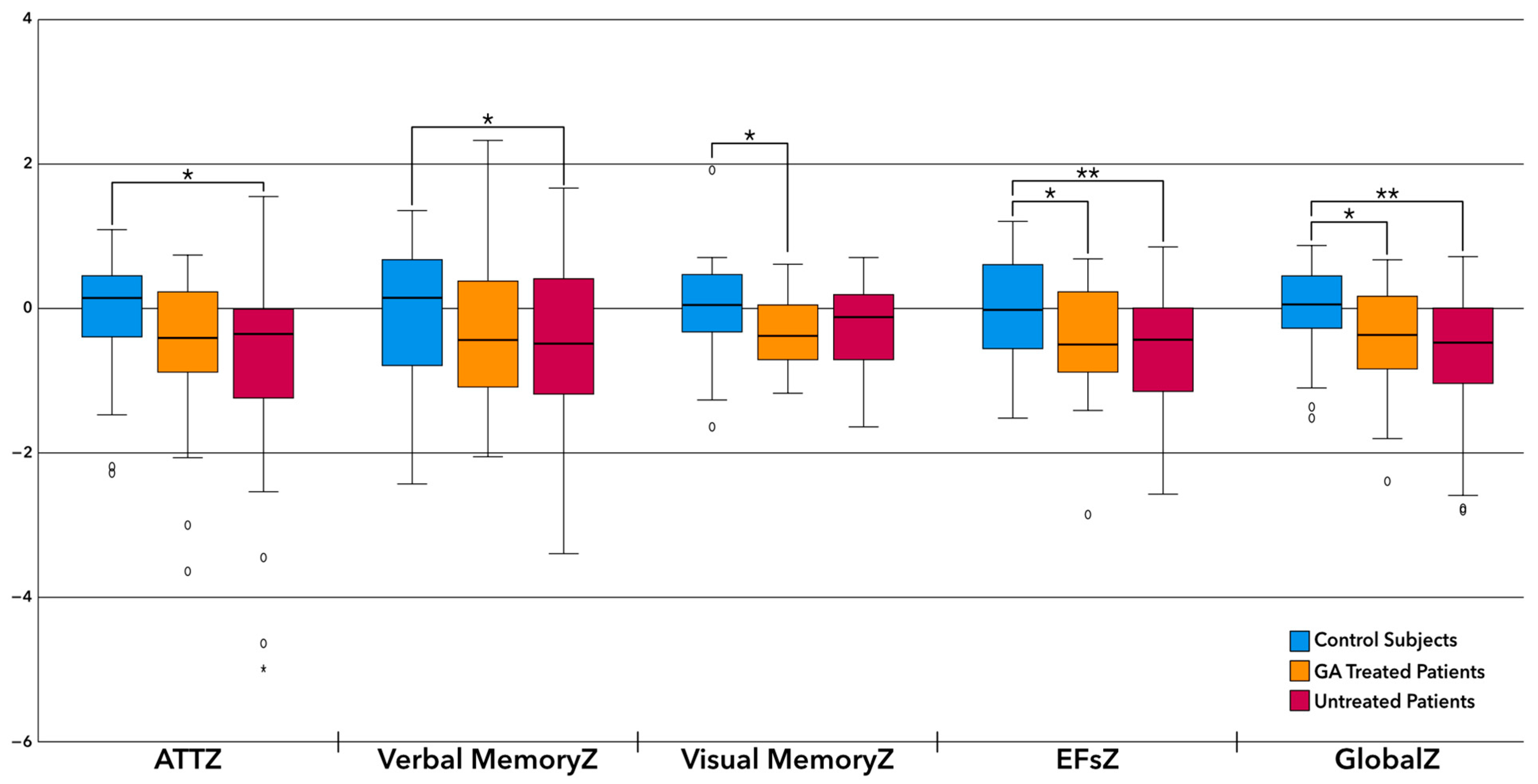
2.2. Differences in Patient’s Cognition
2.3. Antioxidant Capacity
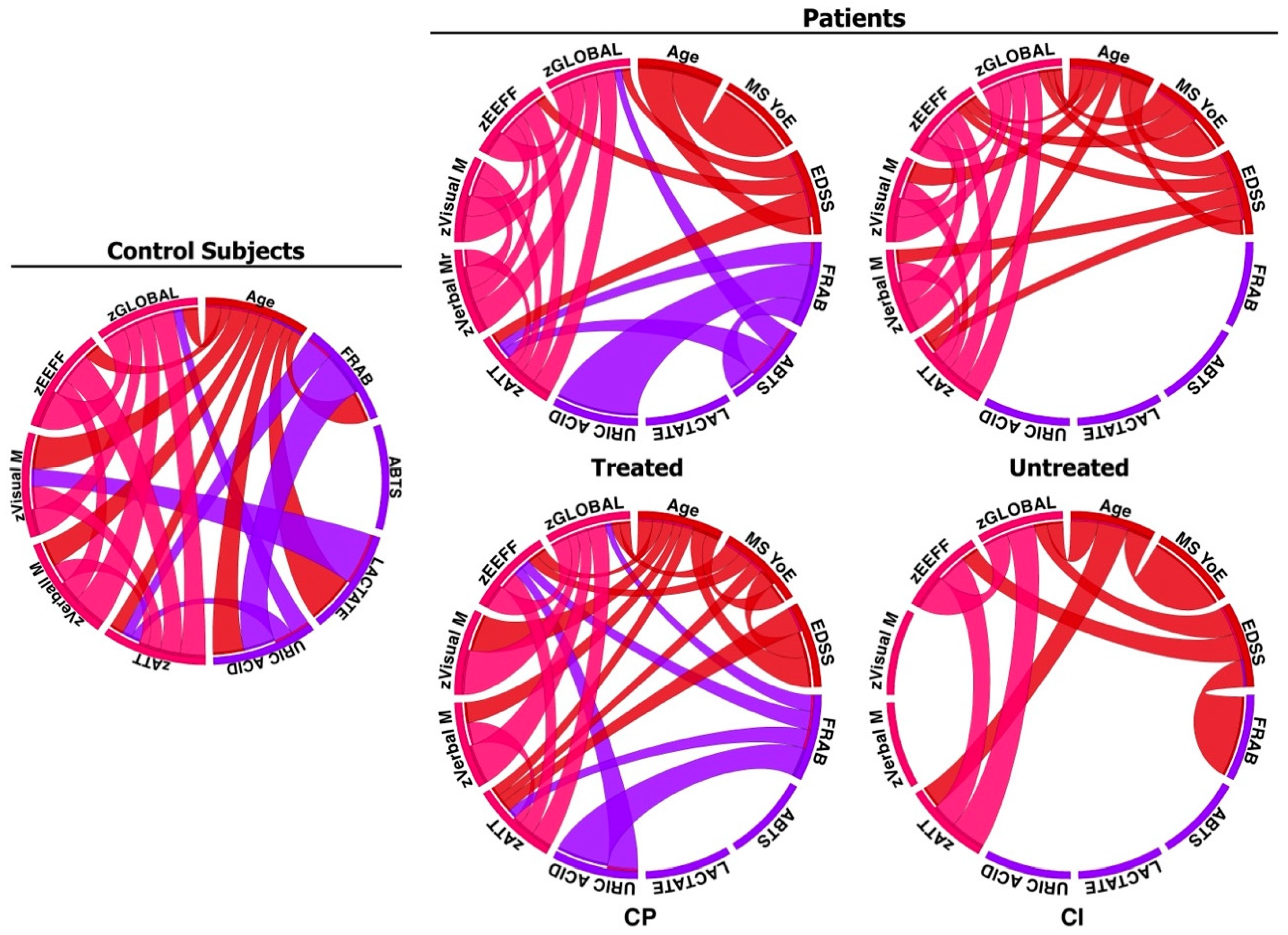
2.4. Relationship between Cognition, Treatment, and Antioxidant Capacity
3. Discussion
4. Materials and Methods
4.1. Design
- (1)
- Control subjects: Subjects not diagnosed with MS or other neurological and/or psychiatric diseases that could compromise their cognitive function. The CS were willing to collaborate in the study without financial benefit.
- (2)
- PwMS treated with GA: patients with a diagnosis of relapsing–remitting MS (RRMS), according to McDonald 2010, whose expanded disability status scale (EDSS) score was ≤3.0 with ≥5 years of MS evolution, and who had been treated with GA for at least the previous year (the two dosages of GA were admitted).
- (3)
- PwMS without treatment: Patients with benign RRMS defined as an EDSS score of ≤3.0 at ≥5 years after the onset of MS. This group did not receive any DMTs, although drug use was accepted to alleviate symptoms of the disease, such as fatigue, pain, or spasms.
- (1)
- Diagnosis of any other neurodegenerative disease that could involve increased CI or OS.
- (2)
- Diagnosis of a psychiatric illness, drug addiction, or mental disability that would have prevented them from understanding the nature of the study.
- (3)
- Refusal to provide informed consent.
4.2. Sample Collection
4.3. Methods to Measure OS or Antioxidant Capacity (FRAP, ABTS, Uric Acid, and Lactate)
4.3.1. FRAP
4.3.2. ABTS
4.3.3. Uric Acid
4.3.4. Lactate
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calabrese, M.; Filippi, M.; Gallo, P. Cortical lesions in multiple sclerosis. Nat. Rev. Neurol. 2010, 6, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Ponziani, G.; Siracusa, G.; Sorbi, S. Cognitive Dysfunction in early-onset Multiple Sclerosis. A Reappraisal after 10 years. Arch. Neurol. 2001, 58, 1602–1606. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.M.; Leo, G.J.; Bernardin, L.; Unverzagt, F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns and predicition. Neurology 1991, 41, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Piacentini, C.; Argento, O.; Nocentini, U. Cognitive impairment in multiple sclerosis: “classic” knowledge and recent acquisitions. Arq. Neuropsiquiatr. 2023, 81, 585–596. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; Goldman, M.D. Epidemiology and Pathophysiology of Multiple Sclerosis. Continuum 2022, 28, 988–1005. [Google Scholar] [CrossRef]
- Geurts, J.J.; Calabrese, M.; Fisher, E.; Rudick, R.A. Measurement and clinical effect of grey matter pathology in multiple sclerosis. Lancet Neurol. 2012, 11, 1082–1092. [Google Scholar] [CrossRef]
- Lisak, M.; Špiljak, B.; Pašić, H.; Trkanjec, Z. Cognitive Aspects in Multiple Sclerosis. Psychiatr. Danub. 2021, 33 (Suppl. 13), 177–182. [Google Scholar] [PubMed]
- Zafrilla, P.; Mulero, J.; Xandri, J.M.; Santo, E.; Caravaca, G.; Morillas, J.M. Oxidative stress in Alzheimer patients in different stages of the disease. Curr. Med. Chem. 2006, 13, 1075–1083. [Google Scholar] [CrossRef]
- Pulido, R.; Jiménez-Escrig, A.; Orensanz, L.; Saura-Calixto, F.; Jiménez-Escrig, A. Study of plasma antioxidant status in Alzheimer’s disease. Eur. J. Neurol. 2005, 12, 531–535. [Google Scholar] [CrossRef]
- Gonsette, R.E. Neurodegeneration in multiple sclerosis: The role of oxidative stress and excitotoxicity. J. Neurol. Sci. 2008, 274, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Flores-Alvarado, L.J.; Gabriel-Ortiz, G.; Pacheco-Mois, F.P.; Bitzer-Quintero, K. Mecanismos patogénicos en el desarrollo de la esclerosis múltiple: Ambiente, genes, sistema inmune y estrés oxidativo [Pathogenic mechanisms of neuronal damage in multiple sclerosis]. Investig. Clin. 2015, 56, 201–214. (In Spanish) [Google Scholar]
- Ohl, K.; Tenbrock, K.; Kipp, M. Oxidative stress in multiple sclerosis: Central and peripheral mode of action. Exp. Neurol. 2016, 277, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Rathore, K.L.; Kerr, B.J.; Redensek, A.; López-Vales, R.; Jeong, S.Y.; Ponka, P.; David, S. Ceruloplasmin protects injured spinal cord from iron-mediated oxidative damage. J. Neurosci. 2008, 28, 12736–12747. [Google Scholar] [CrossRef] [PubMed]
- Gonzalo, H.; Brieva, L.; Tatzber, F.; Jové, M.; Cacabelos, D.; Cassanyé, A.; Lanau-Angulo, L.; Boada, J.; Serrano, J.C.E.; González, C. Lipidome Analysis in Multiple Sclerosis Reveals Protein Lipoxidative Damage as A Potential Pathogenic Mechanism. J. Neurochem. 2012, 10, 622–634. [Google Scholar] [CrossRef] [PubMed]
- Patti, F.; Leone, C.; D’Amico, E. Treatment options of cognitive impairment in multiple sclerosis. Neurol. Sci. 2010, 31, 265–269. [Google Scholar] [CrossRef]
- Landmeyer, N.C.; Bürkner, P.C.; Wiendl, H.; Ruck, T.; Hartung, H.P.; Holling, H.; Meuth, S.G.; Johnen, A. Disease-modifying treatments and cognition in relapsing-remitting multiple sclerosis: A meta-analysis. Neurology 2020, 94, e2373–e2383. [Google Scholar] [CrossRef] [PubMed]
- Carlomagno, V.; Mirabella, M.; Lucchini, M. Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review. Bioengineering 2023, 10, 848. [Google Scholar] [CrossRef]
- Kasindi, A.; Fuchs, D.T.; Koronyo, Y.; Rentsendorj, A.; Black, K.L.; Koronyo-Hamaoui, M. Glatiramer Acetate Immunomodulation: Evidence of Neuroprotection and Cognitive Preservation. Cells 2022, 11, 1578. [Google Scholar] [CrossRef]
- Weinstein, A.; Schwid, S.R.; Schiffer, R.B.; McDermott, M.P.; Giang, D.W.; Goodman, A.D. Neuropsychologic status in multiple sclerosis after treatment with glatiramer. Arch Neurol. 1999, 56, 319–324, Erratum in Arch. Neurol. 2004, 61, 1284. [Google Scholar] [CrossRef]
- Schwid, S.R.; Goodman, A.D.; Weinstein, A.; McDermott, M.P.; Johnson, K.P.; Copaxone Study Group. Cognitive function in relapsing multiple sclerosis: Vminimal changes in a 10-year clinical trial. J. Neurol. Sci. 2007, 255, 57–63. [Google Scholar] [CrossRef] [PubMed]
- LoPresti, P. Glatiramer acetate guards against rapid memory decline during relapsing-remitting experimental autoimmune encephalomyelitis. Neurochem. Res. 2015, 40, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Aharoni, R.; Schottlender, N.; Bar-Lev, D.D.; Eilam, R.; Sela, M.; Tsoory, M.; Arnon, R. Cognitive impairment in an animal model of multiple sclerosis and its amelioration by glatiramer acetate. Sci. Rep. 2019, 9, 4140. [Google Scholar] [CrossRef] [PubMed]
- Iarlori, C.; Gambi, D.; Lugaresi, A.; Patruno, A.; Felaco, M.; Salvatore, M.; Speranza, L.; Reale, M. Reduction of free radicals in multiple sclerosis: Effect of glatiramer acetate (Copaxone). Mult. Scler. 2008, 14, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Ton, A.M.M.; Vasconcelos, C.C.F.; Alvarenga, R.M.P. Benign multiple sclerosis: Aspects of cognition and neuroimaging. Arq. Neuropsiquiatr. 2017, 75, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Tallantyre, E.C.; Major, P.C.; Atherton, M.J.; Davies, W.A.; Joseph, F.; Tomassini, V.; Pickersgill, T.P.; Harding, K.E.; Willis, M.D.; Winter, M.; et al. How common is truly benign MS in a UK population? J. NeurolNeurosurg. Psychiatry 2019, 90, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Meca-Lallana, V.; Gascón-Giménez, F.; Ginestal-López, R.C.; Higueras, Y.; Téllez-Lara, N.; Carreres-Polo, J.; Eichau-Madueño, S.; Romero-Imbroda, J.; Vidal-Jordana, Á.; Pérez-Miralles, F. Cognitive impairment in multiple sclerosis: Diagnosis and monitoring. Neurol. Sci. 2021, 42, 5183–5193. [Google Scholar] [CrossRef] [PubMed]
- Esmael, A.; Elsherif, M.; Abdelsalam, M.; Sabry, D.; Mamdouh, M.; Belal, T. Retinal thickness as a potential biomarker of neurodegeneration and a predictor of early cognitive impairment in patients with multiple sclerosis. Neurol. Res. 2020, 42, 564–574. [Google Scholar] [CrossRef]
- Pflugshaupt, T.; Geisseler, O.; Nyffeler, T.; Linnebank, M. Cognitive Impairment in Multiple Sclerosis: Clinical Manifestation, Neuroimaging Correlates, and Treatment. Semin. Neurol. 2016, 36, 203–211. [Google Scholar] [CrossRef]
- Jakimovski, D.; Bergsland, N.; Dwyer, M.G.; Hagemeier, J.; Ramasamy, D.P.; Szigeti, K.; Guttuso, T.; Lichter, D.; Hojnacki, D.; Weinstock-Guttman, B.; et al. Long-standing multiple sclerosis neurodegeneration: Volumetric magnetic resonance imaging comparison to Parkinson’s disease, mild cognitive impairment, Alzheimer’s disease, and elderly healthy controls. Neurobiol. Aging 2020, 90, 84–92. [Google Scholar] [CrossRef]
- Prod’homme, T.; Zamvil, S.S. The Evolving Mechanisms of Action of Glatiramer Acetate. Cold Spring Harb. Perspect. Med. 2019, 9, a029249. [Google Scholar] [CrossRef]
- Gonzalo, H.; Nogueras, L.; Gil-Sánchez, A.; Hervás, J.V.; Valcheva, P.; González-Mingot, C.; Martin-Gari, M.; Canudes, M.; Peralta, S.; Solana, M.J.; et al. Impairment of Mitochondrial Redox Status in Peripheral Lymphocytes of Multiple Sclerosis Patients. Front. Neurosci. 2019, 13, 938. [Google Scholar] [CrossRef] [PubMed]
- Keytsman, C.; Hansen, D.; Wens, I.; Eijnde, B.O. Exercise-induced lactate responses in Multiple Sclerosis: A retrospective analysis. NeuroRehabilitation 2019, 45, 99–106. [Google Scholar] [CrossRef]
- Cerexhe, L.; Easton, C.; Macdonald, E.; Renfrew, L.; Sculthorpe, N. Blood lactate concentrations during rest and exercise in people with Multiple Sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2022, 57, 103454. [Google Scholar] [CrossRef] [PubMed]
- Albanese, M.; Zagaglia, S.; Landi, D.; Boffa, L.; Nicoletti, C.G.; Marciani, M.G.; Mandolesi, G.; Marfia, G.A.; Buttari, F.; Mori, F.; et al. Cerebrospinal fluid lactate is associated with multiple sclerosis disease progression. J. Neuroinflamm. 2016, 13, 36. [Google Scholar] [CrossRef]
- Alberini, C.M.; Cruz, E.; Descalzi, G.; Bessières, B.; Gao, V. Astrocyte glycogen and lactate: New insights into learning and memory mechanisms. Glia 2018, 66, 1244–1262. [Google Scholar] [CrossRef]
- Dembitskaya, Y.; Piette, C.; Perez, S.; Berry, H.; Magistretti, P.J.; Venance, L. Lactate supply overtakes glucose when neural computational and cognitive loads scale up. Proc. Natl. Acad. Sci. USA 2022, 119, e2212004119. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Ticinesi, A.; Prati, B.; Nouvenne, A.; Meschi, T. Uric Acid and Cognitive Function in Older Individuals. Nutrients 2018, 10, 975. [Google Scholar] [CrossRef]
- Raven, J. Manual for Raven’s Progressive Matrices and Vocabulary Scales; Oxford University Press: Oxford, UK; The Psychological Corporation: San Antonio, TX, USA, 1981. [Google Scholar]
- Amato, M.P.; Morra, V.B.; Falautano, M.; Ghezzi, A.; Goretti, B.; Patti, F.; Riccardi, A.; Mattioli, F. Cognitive assessment in multiple sclerosis-an Italian consensus. Neurol. Sci. 2018, 39, 1317–1324, Erratum in Neurol. Sci. 2019, 40, 1097. [Google Scholar] [CrossRef]
- Sepulcre, J.; Vanotti, S.; Hernández, R.; Sandoval, G.; Cáceres, F.; Garcea, O.; Villoslada, P. Cognitive impairment in patients with multiple sclerosis using the Brief Repeatable Battery-Neuropsychology test. Mult. Scler. 2006, 12, 187–195. [Google Scholar] [CrossRef]
- Velázquez-Cardoso, J.; Marosi-Holczberger, E.; Rodríguez-Agudelo, Y.; Yañez-Tellez, G.; Chávez-Oliveros, M. Recall strategies for the verbal fluency test in patients with multiple sclerosis. Neurologia 2014, 29, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Connick, P.; Kolappan, M.; Bak, T.H.; Chandran, S. Verbal fluency as a rapid screening test for cognitive impairment in progressive multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2012, 83, 346–347. [Google Scholar] [CrossRef] [PubMed]
- Reitan, R.M. Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Percept. Mot. Ski. 2016, 8, 271–276. [Google Scholar] [CrossRef]
- Kalb, R.; Beier, M.; Benedict, R.H.; Charvet, L.; Costello, K.; Feinstein, A.; Gingold, J.; Goverover, Y.; Halper, J.; Harris, C.; et al. Recommendations for cognitive screening and management in multiple sclerosis care. Mult. Scler. 2018, 24, 1665–1680. [Google Scholar] [CrossRef] [PubMed]
- De Meo, E.; Portaccio, E.; Giorgio, A.; Ruano, L.; Goretti, B.; Niccolai, C.; Patti, F.; Chisari, C.G.; Gallo, P.; Grossi, P.; et al. Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis. JAMA Neurol. 2021, 78, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F.; Strain, J.J. Ferric reducing/antioxidant power assay: Direct measure of total antioxidant activity of biological fluids and modified version for simultaneous measurement of total antioxidant power and ascorbic acid concentration. Methods Enzymol. 1999, 299, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Gulcin, İ. Antioxidants and antioxidant methods: An updated overview. Arch. Toxicol. 2020, 94, 651–715. [Google Scholar] [CrossRef] [PubMed]
- Re, R.; Pellegrini, N.; Proteggente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Sautin, Y.Y.; Johnson, R.J. Uric acid: The oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef]
- Groussard, C.; Morel, I.; Chevanne, M.; Monnier, M.; Cillard, J.; Delamarche, A. Free radical scavenging and antioxidant effects of lactate ion: An in vitro study. J. Appl. Physiol. 2000, 89, 169–175. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| GA-Treated (n = 41) | Untreated (n = 42) | CS (n = 42) | p-Value | |
|---|---|---|---|---|
| Sex (n, % females) | 25 (61%) | 33 (79%) | 33 (79%) | 0.116 |
| Age (, SD5) | 42.05 (9.16) | 42.9 (8.56) | 38.05 (15.55) | 0.125 |
| Years of education (, SD) | 12.9 (3.1) | 12.64 (3.18) | 13.83 (3.16) | 0.192 |
| MS years of evolution (, SD) | 10.39 (5.56) | 13.02 (7.15) | - | 0.072 |
| EDSS (median) | 1 (0–3) | 1.5 (0–3) | - | 0.307 |
| CP vs. CI (n/n, %CP/%CI) | 28/12 (68.3%/31.7%) | 26/16 (61.9%/38.1%) | 40/2 (95.2%/4.8%) | - |
| CI: Mild (n,%) | 3 (7.3%) | 6 (14.3%) | 2 (4.8%) | - |
| CI: Moderate (n,%) | 6 (14.6%) | 4 (9.5%) | - | - |
| CI: Severe (n,%) | 4 (9.8%) | 6 (14.3%) | - | - |
| CS (n = 42) | pwMS | ||||
|---|---|---|---|---|---|
| Total (n = 83) | Treated (n = 41) | Untreated (n = 42) | p-Value * | ||
| FRAP (, SD) | 275.86 (138.80) | 259.23 (138.15) | 288.77 (139.21) | 230.39 (132.44) | 0.453 |
| ABTS (, SD) | 551.21 (130.79) | 516.77 (155.60) | 486.53 (151.74) | 546.28 (155.40) | 0.500 |
| Lactate (, SD) | 20.17 (10.98) | 17.25 (8.25) | 18.27 (8.61) | 16.24 (7.86) | 0.210 |
| Uric acid (, SD) | 3.72 (1.81) | 3.28 (1.51) | 3.57 (1.74) | 3.01 (1.21) | 0.267 |
| CS (n = 42) | pwMS CP (n = 54) | pwMS CI (n = 29) | p-Value | |
|---|---|---|---|---|
| FRAP (, SD) | 275.86 (138.80) | 236.59 (110.7) | 301.39 (172.83) | 0.136 |
| ABTS (, SD) | 551.21 (130.79) | 528.35 (136.5) | 495.2 (186.79) | 0.724 |
| Lactate (, SD) | 20.17 (10.98) | 18.52 (8.28) | 14.87 (7.78) | 0.038 * |
| Uric Acid (, SD) | 3.72 (1.81) | 3.34 (1.66) | 3.19 (1.22) | 0.879 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Sánchez, A.; Gonzalo, H.; Canudes, M.; Nogueras, L.; González-Mingot, C.; Valcheva, P.; Torres, P.; Serrano, J.C.; Peralta, S.; Solana, M.J.; et al. Can Glatiramer Acetate Prevent Cognitive Impairment by Modulating Oxidative Stress in Patients with Multiple Sclerosis? Pharmaceuticals 2024, 17, 459. https://doi.org/10.3390/ph17040459
Gil-Sánchez A, Gonzalo H, Canudes M, Nogueras L, González-Mingot C, Valcheva P, Torres P, Serrano JC, Peralta S, Solana MJ, et al. Can Glatiramer Acetate Prevent Cognitive Impairment by Modulating Oxidative Stress in Patients with Multiple Sclerosis? Pharmaceuticals. 2024; 17(4):459. https://doi.org/10.3390/ph17040459
Chicago/Turabian StyleGil-Sánchez, Anna, Hugo Gonzalo, Marc Canudes, Lara Nogueras, Cristina González-Mingot, Petya Valcheva, Pascual Torres, Jose Carlos Serrano, Silvia Peralta, Maria José Solana, and et al. 2024. "Can Glatiramer Acetate Prevent Cognitive Impairment by Modulating Oxidative Stress in Patients with Multiple Sclerosis?" Pharmaceuticals 17, no. 4: 459. https://doi.org/10.3390/ph17040459
APA StyleGil-Sánchez, A., Gonzalo, H., Canudes, M., Nogueras, L., González-Mingot, C., Valcheva, P., Torres, P., Serrano, J. C., Peralta, S., Solana, M. J., & Brieva, L. (2024). Can Glatiramer Acetate Prevent Cognitive Impairment by Modulating Oxidative Stress in Patients with Multiple Sclerosis? Pharmaceuticals, 17(4), 459. https://doi.org/10.3390/ph17040459