
Impact of Body Mass Index in the Cardioverter Efficacy of Amiodarone in Persistent Atrial Fibrillation
 ,
,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Results
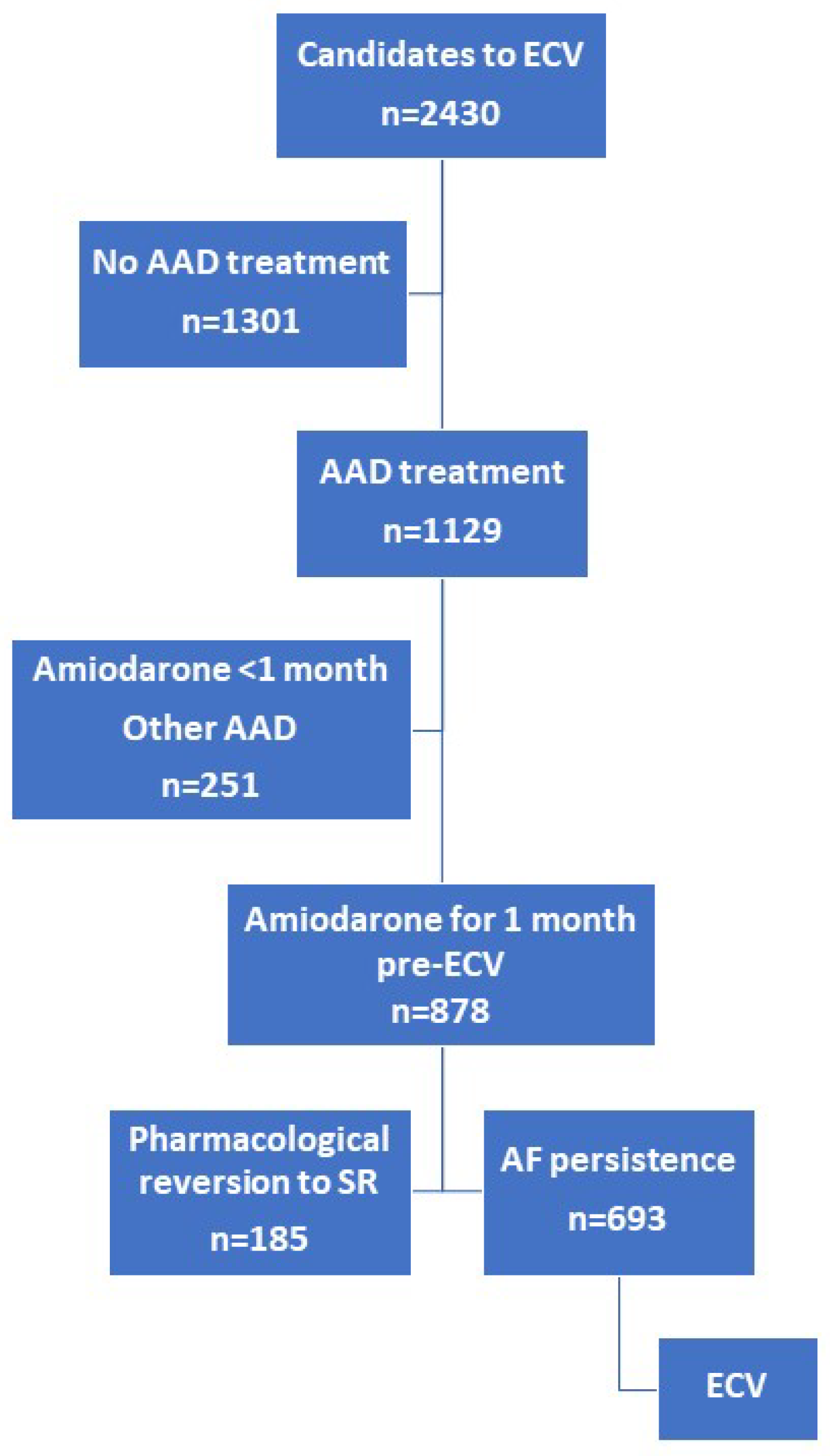
2.1. Patients’ Characteristics
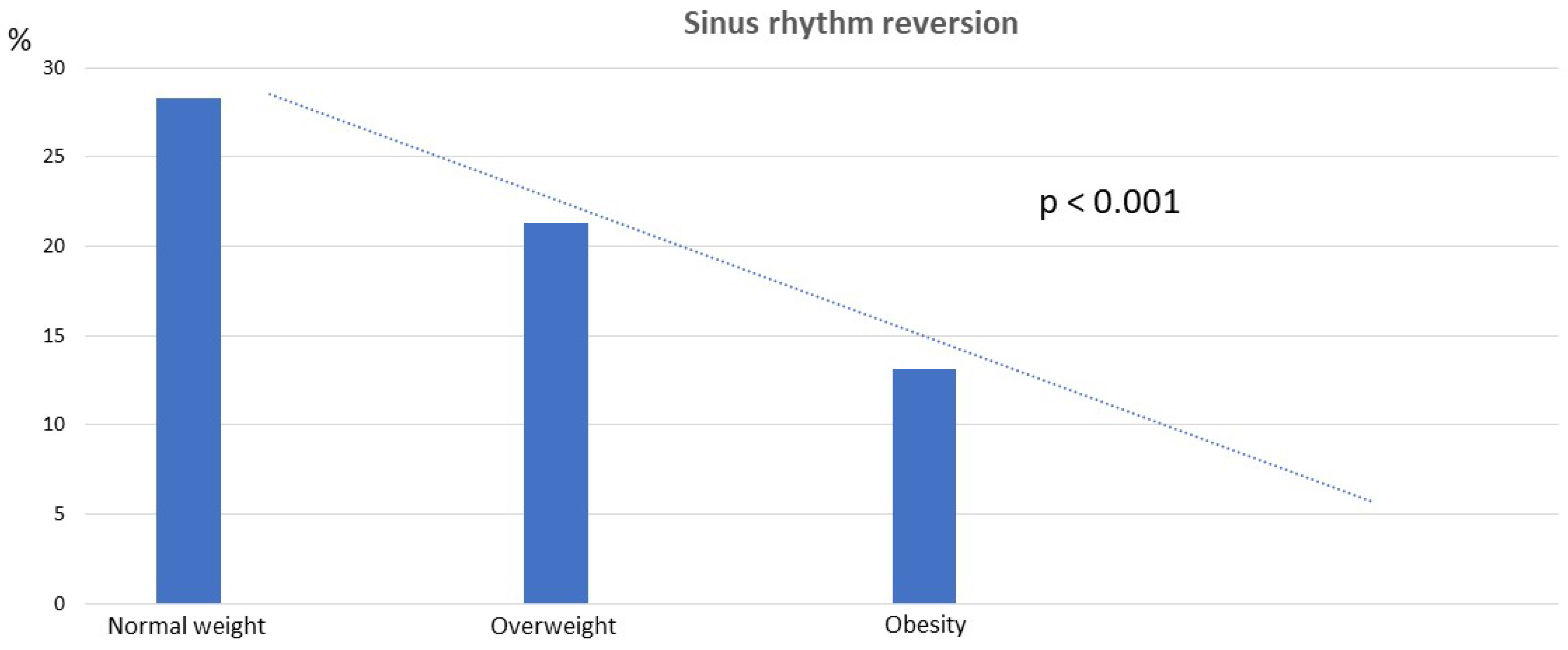
2.2. BMI and SR Reversion
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; Dalquist, J.E.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators*. N. Engl. J. Med. 2002, 23, 1825–1833. [Google Scholar]
- Van Gelder, I.C.; Hagens, V.E.; Bosker, H.A.; Kingma, J.H.; Kamp, O.; Kingma, T.; Said, S.A.; Darmanata, J.I.; Timmermans, A.J.; Tijssen, J.G.; et al. Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation Study Group. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N. Engl. J. Med. 2002, 347, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation|Enhanced Reader. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Vizzardi, E.; Curnis, A.; Latini, M.G.; Salghetti, F.; Rocco, E.; Lupi, L.; Rovetta, R.; Quinzani, F.; Bonadei, I.; Bontempi, L.; et al. Risk factors for atrial fibrillation recurrence: A literature review. J. Cardiovasc. Med. (Hagerstown) 2014, 15, 235–253. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Hernández-Madrid, A.; Svendsen, J.H.; Lip, G.Y.H.; Van Gelder, I.C.; Dobreanu, D.; Blomstrom-Lundqvist, C. Cardioversion for atrial fibrillation in current European practice: Results of the European Heart Rhythm Association survey. Europace 2013, 15, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Freedman, M.D.; Somberg, J.C. Pharmacology and pharmacokinetics of amiodarone. J. Clin. Pharmacol. 1991, 31, 1061–1069. [Google Scholar] [CrossRef]
- Lafuente-Lafuente, C.; Alvarez, J.; Leenhardt, A.; Mouly, S.; Extramiana, F.; Caulin, C.; Funck-Brentano, C.; Bergmann, J. Amiodarone concentrations in plasma and fat tissue during chronic treatment and related toxicity. Br. J. Clin. Pharmacol. 2009, 67, 511–519. [Google Scholar] [CrossRef]
- Brien, J.F.; Jimmo, S.; Brennan, F.J.; Ford, S.E.; Armstrong, P.W. Distribution of amiodarone and its metabolite, desethylamiodarone, in human tissues. Can. J. Physiol. Pharmacol. 1987, 65, 360–364. [Google Scholar] [CrossRef]
- Adams, P.C.; Holt, D.W.; Storey, G.C.A.; Morley, A.R.; Callaghan, J.; Campbell, R.W.F. Amiodarone and its desethyl metabolite: Tissue distribution and morphologic changes during long-term therapy. Circulation 1985, 72, 1064–1075. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española del Medicamento y Productos Sanitarios [Internet]. Available online: https://cima.aemps.es/cima/dochtml/ft/48048/FT_48048.html (accessed on 10 January 2024).
- Galperín, J.; Elizari, M.V.; Chiale, P.A.; Molina, R.T.; Ledesma, R.; Scapín, A.O.; Blanco, M.V.; Bonato, R.; Lago, M.; Grupo de Estudio de Fibrilación Auricular Con Amiodarona (GEFACA) Investigators. Pharmacologic Reversion of Persistent Atrial Fibrillation with Amiodarone Predicts Long-Term Sinus Rhythm Maintenance. J. Cardiovasc. Pharmacol. Ther. 2003, 8, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Nalliah, C.J.; Sanders, P.; Kottkamp, H.; Kalman, J.M. The role of obesity in atrial fibrillation. Eur. Heart J. 2015, 37, 1565–1572. [Google Scholar] [CrossRef] [PubMed]
- Cheymol, G. Effects of obesity on pharmacokinetics implications for drug therapy. Clin. Pharmacokinet. 2000, 39, 215–231. [Google Scholar] [CrossRef] [PubMed]
- Abdussalam, A.; Elshenawy, O.H.; bin Jardan, Y.A.; El-Kadi, A.O.S.; Brocks, D.R. The Obesogenic Potency of Various High-Caloric Diet Compositions in Male Rats, and Their Effects on Expression of Liver and Kidney Proteins Involved in Drug Elimination. J. Pharm. Sci. 2017, 106, 1650–1658. [Google Scholar] [CrossRef] [PubMed]
- Fukuchi, H.; Nakashima, M.; Araki, R.; Komiya, N.; Hayano, M.; Yano, K.; Sasaki, H.; Yukawa, E. Effect of obesity on serum amiodarone concentration in Japanese patients: Population pharmacokinetic investigation by multiple trough screen analysis. J. Clin. Pharm. Ther. 2009, 34, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ornelas-Loredo, A.; Kany, S.; Abraham, V.; Alzahrani, Z.; Darbar, F.A.; Sridhar, A.; Ahmed, M.; Alamar, I.; Menon, A.; Zhang, M.; et al. Association between Obesity-Mediated Atrial Fibrillation and Therapy with Sodium Channel Blocker Antiarrhythmic Drugs. JAMA Cardiol. 2020, 5, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Lehnert, A.; Foissac, F.; Bouazza, N.; Urien, S.; Oualha, M.; Renolleau, S.; Barbanti, C.; Di Marzio, A.; Bonnet, D.; Abdalla, S.; et al. Amiodarone/N-desethylamiodarone population pharmacokinetics in paediatric patients. Br. J. Clin. Pharmacol. 2022, 88, 5369–5377. [Google Scholar] [CrossRef] [PubMed]
- Ligero, C.; Bazan, V.; Guerra, J.M.; Rodríguez-Mañero, M.; Viñolas, X.; Alegret, J.M. Influence of body mass index on recurrence of atrial fibrillation after electrical cardioversion. PLoS ONE 2023, 18, e0291938. [Google Scholar] [CrossRef]
- Kanagala, R.; Murali, N.S.; Friedman, P.A.; Ammash, N.M.; Gersh, B.J.; Ballman, K.V.; Shamsuzzaman, A.S.M.; Somers, V.K. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 2003, 107, 2589–2594. [Google Scholar] [CrossRef]
- de Heide, J.; Kock-Cordeiro, D.B.M.; Bhagwandien, R.E.; Hoogendijk, M.G.; van der Meer, K.C.; Wijchers, S.A.; Szili-Torok, T.; Zijlstra, F.; Lenzen, M.J.; Yap, S.-C. Impact of undiagnosed obstructive sleep apnea on atrial fibrillation recurrence following catheter ablation (OSA-AF study). IJC Heart Vasc. 2022, 40, 101014. [Google Scholar] [CrossRef]
- Amrani AEl Viñolas, X.; Arias, M.A.; Bazan, V.; Valdovinos, P.; Alegret, J.M. Pharmacological cardioversion after pre-treatment with antiarrythmic drugs prior to electrical cardioversion in persistent atrial fibrillation: Impact on maintenance of sinus rhythm. J. Clin. Med. 2021, 10, 1029. [Google Scholar] [CrossRef]
- Alpert, M.A.; Omran, J.; Bostick, B.P. Effects of Obesity on Cardiovascular Hemodynamics, Cardiac Morphology, and Ventricular Function. Curr. Obes. Rep. 2016, 5, 424–434. [Google Scholar] [CrossRef]
- Alpert, M.A.; Lavie, C.J.; Agrawal, H.; Aggarwal, K.B.; Kumar, S.A. Obesity and heart failure: Epidemiology, pathophysiology, clinical manifestations, and management. Transl. Res. 2014, 164, 345–356. [Google Scholar] [CrossRef]
- Pisters, R.; Nieuwlaat, R.; Prins, M.H.; Le Heuzey, J.-Y.; Maggioni, A.P.; Camm, A.J.; Crijns, H.J.; for the Euro Heart Survey Investigators. Clinical correlates of immediate success and outcome at 1-year follow-up of real-world cardioversion of atrial fibrillation: The Euro Heart Survey. Europace 2012, 14, 666–674. [Google Scholar] [CrossRef]
- Seko, Y.; Kato, T.; Haruna, T.; Izumi, T.; Miyamoto, S.; Nakane, E.; Inoko, M. Association between atrial fibrillation, atrial enlargement, and left ventricular geometric remodeling. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Rabkin, S.W. The relationship between epicardial fat and indices of obesity and the metabolic syndrome: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2014, 12, 31–42. [Google Scholar] [CrossRef]
- Gaeta, M.; Bandera, F.; Tassinari, F.; Capasso, L.; Cargnelutti, M.; Pelissero, G.; Malavazos, A.E.; Ricci, C. Is epicardial fat depot associated with atrial fibrillation? A systematic review and meta-analysis. Europace 2017, 19, 747–752. [Google Scholar] [CrossRef]
- Conte, M.; Petraglia, L.; Cabaro, S.; Valerio, V.; Poggio, P.; Pilato, E.; Attena, E.; Russo, V.; Ferro, A.; Formisano, P.; et al. Epicardial Adipose Tissue and Cardiac Arrhythmias: Focus on Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 9, 932262. [Google Scholar] [CrossRef]
- Balan, A.I.; Halațiu, V.B.; Scridon, A. Oxidative Stress, Inflammation, and Mitochondrial Dysfunction: A Link between Obesity and Atrial Fibrillation. Antioxidants 2024, 13, 117. [Google Scholar] [CrossRef]
- Zakynthinos, G.E.; Tsolaki, V.; Oikonomou, E.; Vavouranakis, M.; Siasos, G.; Zakynthinos, E. Metabolic Syndrome and Atrial Fibrillation: Different Entities or Combined Disorders. J. Pers. Med. 2023, 13, 1323. [Google Scholar] [CrossRef]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2009, 89, 500–508. [Google Scholar] [CrossRef]
- Rothman, K.J. BMI-related errors in the measurement of obesity. Int. J. Obes. 2008, 32 (Suppl. S3), S56–S59. [Google Scholar] [CrossRef]
- Mehra, R.; Benjamin, E.J.; Shahar, E.; Gottlieb, D.J.; Nawabit, R.; Kirchner, H.L.; Sahadevan, J.; Redline, S.; Sleep Heart Health Study. Association of nocturnal arrhythmias with sleep-disordered breathing: The sleep heart health study. Am. J. Respir. Crit. Care Med. 2006, 173, 910–916. [Google Scholar] [CrossRef]
- Ng, C.Y.; Liu, T.; Shehata, M.; Stevens, S.; Chugh, S.S.; Wang, X. Meta-analysis of obstructive sleep apnea as predictor of atrial fibrillation recurrence after catheter ablation. Am. J. Cardiol. 2011, 108, 47–51. [Google Scholar] [CrossRef]
- Alegret, J.M.; Viñolas, X.; Sagristá, J.; Hernández-Madrid, A.; Berruezo, A.; Moya, A.; Martínez Sande, J.L.; Pastor, A.; nombre de los investigadores del Estudio REVERSE. Clinical characteristics of patients with persistent atrial fibrillation referred for cardioversion: Spanish cardioversion registry (REVERSE). Rev. Esp. Cardiol. 2008, 61, 630–634. [Google Scholar] [CrossRef]
- Alegret, J.M.; Viñolas, X.; Martínez-Rubio, A.; Pedrote, A.; Beiras, X.; García-Sacristán, J.F.; Crespo-Mancebo, F.; Ruiz-Mateas, F. Gender differences in patients with atrial fibrillation undergoing electrical cardioversion. J. Women’s Health 2015, 24, 466–470. [Google Scholar] [CrossRef]
- Obesity and Overweight. World Health Organization, News-Room/Fact-Sheets [Internet]. 1–6 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 6 September 2023).

{kind=link}
{kind=link}
| n = 878 (%) | No PCV (n = 693) | PCV (n = 185) | p | |
|---|---|---|---|---|
| Age (years) | 64 ± 11 | 63.99 ± 10.92 | 64.99 ± 11.33 | 0.150 |
| Male gender | 593 (67.5) | 482 (69.5) | 111 (60.0) | 0.014 |
| Structural heart disease | 411(46.8) | 337 (48.6) | 74 (40.0) | 0.037 |
| Diabetes mellitus | 130 (14.8) | 108 (15.6) | 22 (11.9) | 0.209 |
| Hypertension | 506 (57.6) | 403 (58.2) | 103 (55.7) | 0.545 |
| COPD | 80 (9.1) | 65 (9.4) | 15 (8.1) | 0.590 |
| LVH | 309 (36.0) | 253 (36.5) | 56 (30.3) | 0.101 |
| LVEF < 40% | 89 (10.9) | 70 (10.0) | 19 (10.7) | 0.910 |
| NYHA ≥ 2 | 429 (48.9) | 338 (48.8) | 91 (49.3) | 0.908 |
| AF duration > 1 year | 102 (11.6) | 90 (12.9) | 12 (6.7) | 0.014 |
| LA size > 50 mm | 162 (19.7) | 136 (19.4) | 26 (14.6) | 0.066 |
| LA size | 44.75 ± 6.40 | 45.18 ± 6.34 | 43.15 ± 6.38 | <0.001 |
| LVEF | 57.83 ± 12.16 | 57.55 ± 12.19 | 58.87 ± 12.03 | 0.205 |
| ACE/ARA II | 513 (58.4) | 406 (58.6) | 107 (57.8) | 0.854 |
| Beta blockers | 564 (64.2) | 445 (64.2) | 119 (64.3) | 0.98 |
| Calcium antagonist | 186 (21.2) | 35 (18.9) | 151 (21.8) | 0.40 |
| BMI | 28.78 ± 4.36 | 29.11 ± 4.09 | 27.45 ± 4.36 | <0.001 |
| OR (95% CI) | p | |
|---|---|---|
| BMI | 0.904 (0.864–0.946) | <0.001 |
| Previous heart disease | 0.590 (0.412–0.846) | 0.004 |
| AF duration > 1 year | 0.417 (0.204–0.855) | 0.017 |
| Gender | 0.083 | |
| LA size (mm) | 0.432 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ligero, C.; Riera, P.; El-Amrani, A.; Bazan, V.; Guerra, J.M.; Herraez, S.; Viñolas, X.; Alegret, J.M. Impact of Body Mass Index in the Cardioverter Efficacy of Amiodarone in Persistent Atrial Fibrillation. Pharmaceuticals 2024, 17, 693. https://doi.org/10.3390/ph17060693
Ligero C, Riera P, El-Amrani A, Bazan V, Guerra JM, Herraez S, Viñolas X, Alegret JM. Impact of Body Mass Index in the Cardioverter Efficacy of Amiodarone in Persistent Atrial Fibrillation. Pharmaceuticals. 2024; 17(6):693. https://doi.org/10.3390/ph17060693
Chicago/Turabian StyleLigero, Carmen, Pau Riera, Amine El-Amrani, Victor Bazan, José M. Guerra, Silvia Herraez, Xavier Viñolas, and Josep M. Alegret. 2024. "Impact of Body Mass Index in the Cardioverter Efficacy of Amiodarone in Persistent Atrial Fibrillation" Pharmaceuticals 17, no. 6: 693. https://doi.org/10.3390/ph17060693
APA StyleLigero, C., Riera, P., El-Amrani, A., Bazan, V., Guerra, J. M., Herraez, S., Viñolas, X., & Alegret, J. M. (2024). Impact of Body Mass Index in the Cardioverter Efficacy of Amiodarone in Persistent Atrial Fibrillation. Pharmaceuticals, 17(6), 693. https://doi.org/10.3390/ph17060693