Abstract
In this study, we compared the similarities and differences in adverse events (AEs) among CAR T-cell products through signal mining via the FDA Adverse Event Reporting System (FAERS) and identified unknown AEs to provide a reference for safe clinical medication. Data from the FAERS database spanning from the fourth quarter of 2017 to the first quarter of 2024 were extracted. Signals were identified using the reporting odds ratio (ROR) method and the Medicines and Healthcare Products Regulatory Agency (MHRA) method. A total of 11,386 AE reports related to six CAR T-cell products were selected. The top three categories of AEs reported were nervous system disorders, immune system disorders, and general disorders and administration site conditions. However, there were variations in the AE spectra among the different CAR T-cell products. The BCMA-targeting drugs idecabtagene vicleucel (Ide-cel) and ciltacabtagene autoleucel (Cilta-cel) were found to be associated with parkinsonism, which were not observed in CD19-targeting drugs. Tisagenlecleucel (Tisa-cel) and axicabtagene ciloleucel (Axi-cel) exhibited cerebrovascular accident-related AEs, graft versus host disease, and abnormal coagulation indices. Cilta-cel was associated with cerebral hemorrhage, intracranial hemorrhage, cranial nerve disorder, and facial nerve disorder. Cardiopulmonary toxicity, including hypoxia, tachypnoea, cardiorenal syndrome, and hypotension, exhibited strong signal intensities and considerable overlap with CRS. The number of positive signals for cardiopulmonary toxicity associated with drugs targeting CD-19 is greater. Clinicians should assess patients prior to medication and closely monitor their vital signs, mental status, and laboratory parameters during treatment.
1. Introduction
Immunotherapy has become a research hotspot in the field of hematological malignancies in recent years. With advancements in genetic engineering and molecular biology and a deeper understanding of tumor pathogenesis, chimeric antigen receptor T-cell (CAR T-cell) therapy has seen widespread clinical application. Extensive clinical research has demonstrated that CAR T-cell therapies are highly effective in treating relapsed/refractory (RR) B-cell hematological malignancies [1,2,3]. Specifically, the complete response of patients with acute lymphoblastic leukemia (ALL) ranges from 70% to 90% [4,5,6,7,8,9,10,11,12,13], that of patients with lymphoma ranges from 50% to 70% [14,15,16,17], and that of patients with multiple myeloma (MM) ranges from 50% to 98% [18,19,20,21,22,23,24,25]. In 2017, two CD19-targeted CAR T-cell products, tisagenlecleucel (Tisa-cel) and axicabtagene ciloleucel (Axi-cel), were approved by the U.S. Food and Drug Administration (FDA) for the treatment of relapsed/refractory ALL and lymphoma [26,27]. Subsequently, four additional CAR T-cell products were approved by the FDA: lisocabtagene maraleucel (Liso-cel) and brexucabtagene autoleucel (Brexu-cel), which target CD19, and idecabtagene vicleucel (Ide-cel) and ciltacabtagene autoleucel (Cilta-cel), which target B-cell maturation antigen (BCMA) [28,29,30]. With the increasing clinical application of CAR T-cell therapy, treatment-related side effects have garnered significant attention. In addition to cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), a variety of other AEs, such as hematological disorders, infections, and cardiovascular diseases, have been observed in clinical trials. In some instances, these AEs can be fatal [17,31,32,33], posing considerable challenges to routine clinical diagnosis and treatment. At present, the FDA has approved six CAR T-cell products, four of which target CD19 and two of which target BCMA, but no relevant studies have analyzed and compared the adverse reactions of CAR T-cell products with different targets.
Isolated clinical trials and their systematic reviews present the highest quality of evidence and are the basis for guidelines issued by healthcare organizations. However, the evaluation of entire profiles of rare AEs derived from clinical trials is difficult owing to their stringent diagnostic standards and selection criteria, relatively small sample sizes, and limited follow-up time. The FAERS database, one of the largest pharmacovigilance databases, with a large quantity of reported AEs and patient information, could provide data to verify and supplement the findings of clinical trials. In this study, we compared the similarities and differences in AEs among six CAR T-cell products through signal mining via the FAERS database and identified unknown AEs to provide a valuable reference for the selection and long-term management of CAR T-cell therapy.
2. Results
2.1. Characteristics of CAR T-Cell Reports in the FAERS Database
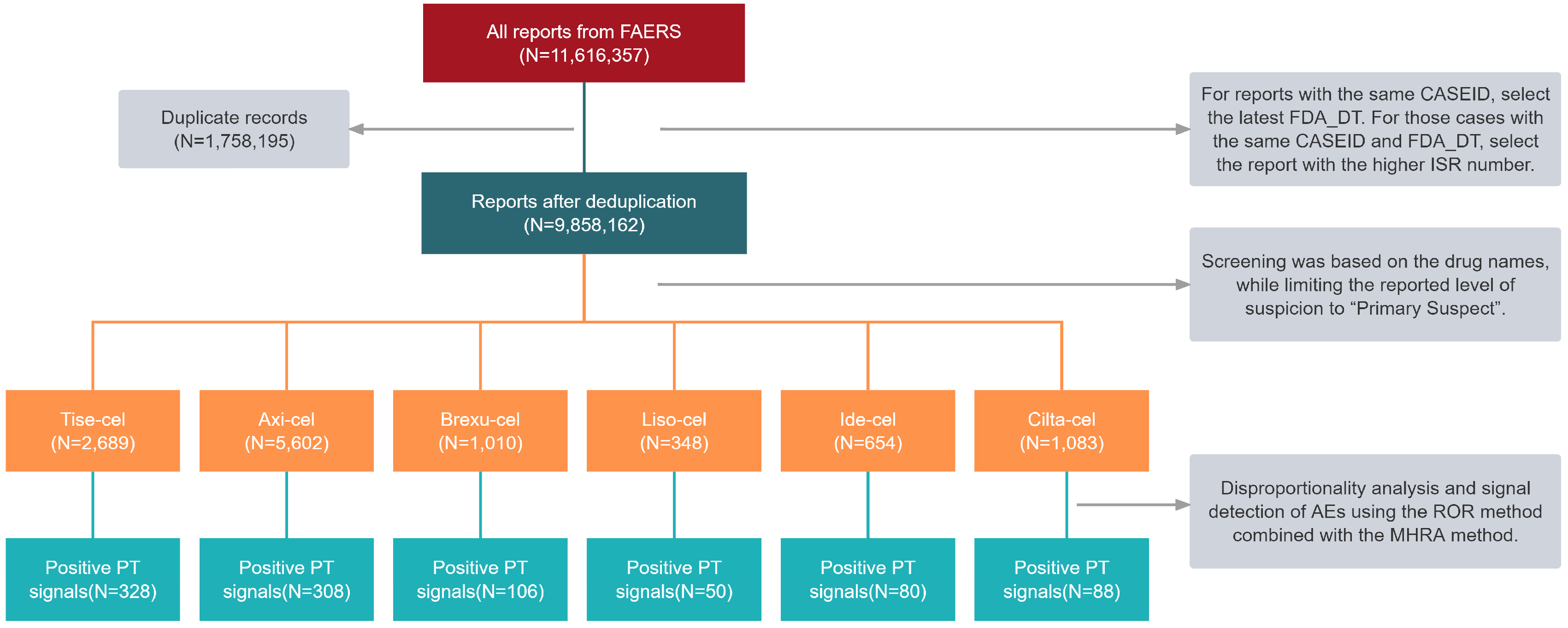
A total of 11,616,357 reports were retrieved in the FAERS database from the inception up to the first quarter (Q1) of 2024, and 11,386 reports were associated with FDA-approved CAR T-cell products after deduplication (2689 involving Tisa-cel, 5602 involving Axi-cel, 1010 involving Brexu-cel, 348 involving Liso-cel, 654 involving Ide-cel, and 1083 involving Cilta-cel) (Figure 1). The specific demographic and clinical details are provided in Table 1. Among these reports, 29.9% were female and 48.7% were male. They were mainly aged 18 to 64 years (33.4%). From the perspective of reporting sources, health professionals reported the most cases (80.8%). Most AE cases were reported in North America, accounting for 63.4% of all cases. This was followed by Europe (20.3%) and Asia (4.3%). Furthermore, a significant proportion of patients (92.1%) experienced serious outcomes, including hospitalization, death, and life threat. The major ADRs overlapped with CRS.
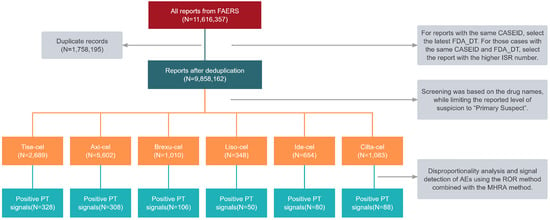
Figure 1.
Flow diagram for data mining from the FAERS database. Positive PT signals: positive signals at the preferred term (PT) level.

Table 1.
Characteristics of reports associated with CAR T-cell therapies.
2.2. CAR T-Cell Therapy-Associated Adverse Events
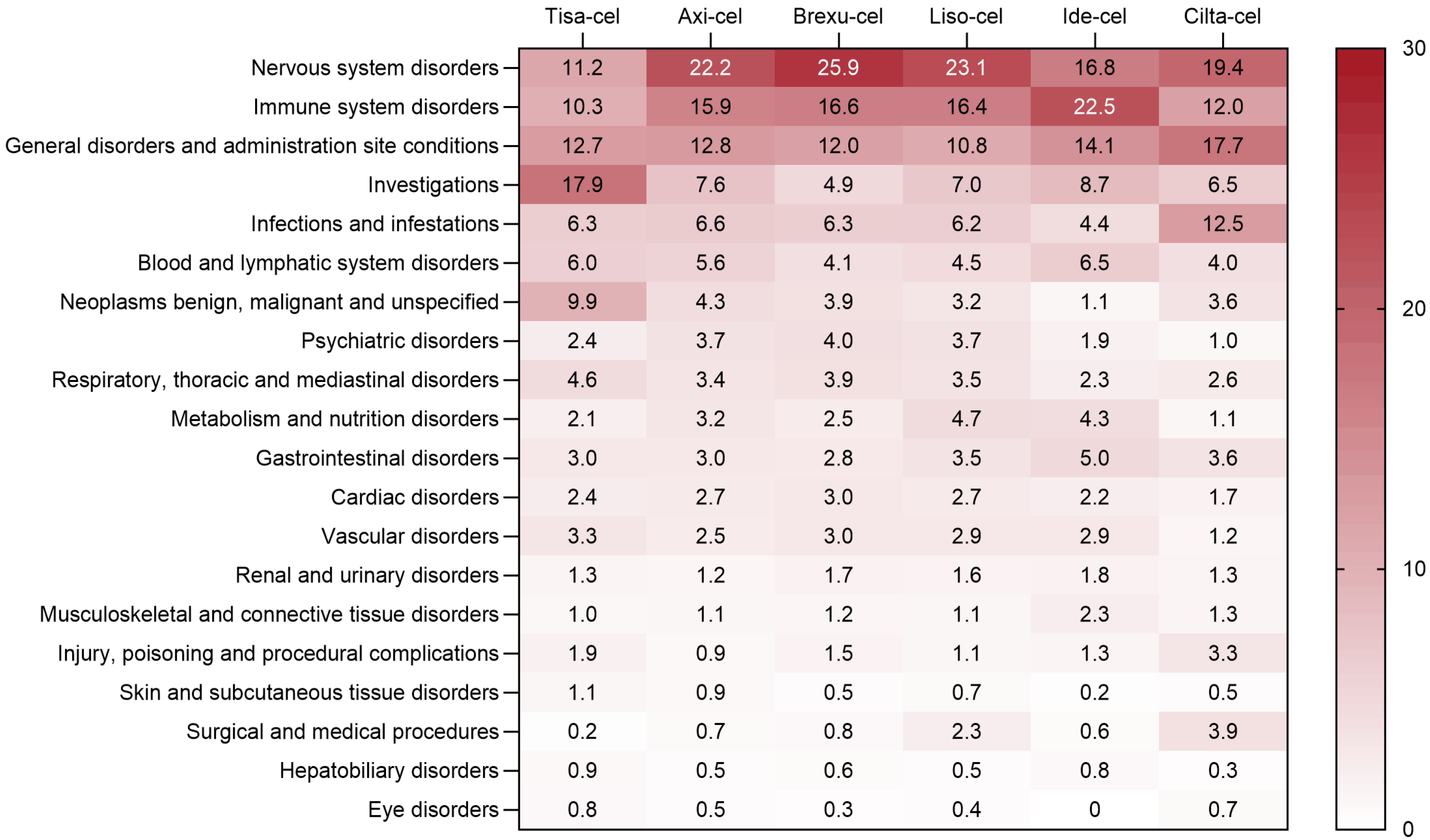
The AE signals were classified according to the system organ class (SOC), and the proportion of AE-positive signals related to CAR T-cell therapy is shown in Figure 2. Overall, nervous system disorders, immune system disorders, and general disorders and administration site conditions are the top three categories of AEs reported for CAR T-cell therapy. Notably, Tisa-cel has a greater incidence of AEs related to various laboratory tests, Ide-cel has a greater incidence of immune system-related AEs, and Brexu-cel has a greater incidence of nervous system-related AEs.
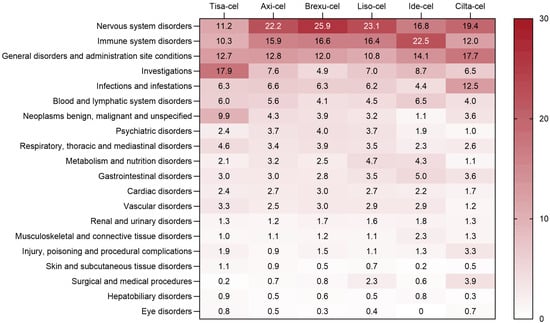
Figure 2.
Distribution of adverse event reporting rates.
2.2.1. Common Adverse Events in Key Organs
The results of the detection of common AE signals associated with CAR T-cell therapy in key organs are shown in Table 2, and differences in the AE profiles were found among the CAR T-cell products. The details are as follows:
Table 2.
Signal detection of common adverse events in key organs associated with CAR T-cell therapies at the preferred terms (PT) level.
Nervous system disorders: ICANS and neurotoxicity are the most common AEs, showing strong signal strength across all drugs. Axi-cel exhibited the strongest signal for ICANS (ROR = 1198.80), while Liso-cel showed the strongest signal for neurotoxicity (ROR = 236.75). Tisa-cel and Axi-cel also exhibited cerebrovascular accident-related AEs. Cilta-cel was associated with cerebral hemorrhage (ROR = 3.81) and intracranial hemorrhage (ROR = 18.47) and exhibited strong signals in cranial nerve disorder (ROR = 991.24), facial nerve disorders (ROR = 727.22), Bell’s palsy (ROR = 253.07), facial paralysis (ROR = 95.69), and Guillain–Barre syndrome (ROR = 19.92). The BCMA-targeting drugs Ide-cel (ROR = 13.00) and Cilta-cel (ROR = 168.90) were found to be associated with parkinsonism, which were not observed in CD19-targeting drugs. There were more AEs in the nervous system, and only AEs with an ROR greater than or equal to 5 are listed in the table.
Immune system disorders: CRS was the most common AE, followed by hypogammaglobulinemia and hemophagocytic lymphohistiocytosis (HLH). Axi-cel had the strongest signal for CRS (ROR = 676.42), Tisa-cel had the strongest signal for hypogammaglobulinemia (ROR = 151.64), and Cilta-cel had the strongest signal for HLH (ROR = 75.22). Additionally, Tisa-cel and Axi-cel were found to cause graft versus host disease. Axi-cel, Ide-cel, and Cilta-cel were also associated with immunodeficiency.
Infections and infestations: Bacterial infection was the most common type of infection, with Cilta-cel showing relatively strong signals of bacterial (ROR = 7.16), fungal (ROR = 8.17), and viral (ROR = 2.63) infections.
Investigations: Decreased white blood cell count and decreased platelet count were the most common AEs, with Tisa-cel showing relatively strong signals. Tisa-cel, Axi-cel, Brexu-cel, Liso-cel and Cilta-cel all exhibited strong signals for increased serum ferritin. Additionally, Tisa-cel and Axi-cel also observed abnormal coagulation indices.
2.2.2. Adverse Events of Special Interest
Respiratory, thoracic, and mediastinal disorders: Hypoxia, respiratory failure, tachypnea, and pleural effusion were the most common AEs, and strong signals were observed in several CAR T-cell products. Tisa-cel, Axi-cel, and Brexu-cel also exhibited atelectasis, which was not mentioned on the drug labels. Additionally, Tisa-cel was associated with respiratory distress (ROR = 4.08), pulmonary hemorrhage (ROR = 5.29), organizing pneumonia (ROR = 5.00), lung consolidation (ROR = 5.99), and pharyngeal hemorrhage (ROR = 10.64). Axi-cel was associated with pulmonary hemorrhage (ROR = 3.87), lung consolidation (ROR = 4.07), lung infiltration (ROR = 3.56), and pulmonary alveolar hemorrhage (ROR = 2.98). Ide-cel was linked to laryngeal edema (ROR = 30.63). Cilta-cel also detected respiratory distress (ROR = 6.14). Although these AEs are uncommon, they still necessitate clinical attention (Table 3).
Table 3.
Signal detection of adverse events of special interest associated with CAR T-cell therapies at the preferred terms (PT) level.
Cardiac disorders: Tachycardia and arrhythmia were the most common AEs. Additionally, Tisa-cel (ROR = 44.41) and Axi-cel (ROR = 150.61) were associated with cardiorenal syndrome. Tisa-cel was also linked to pericardial effusion (ROR = 2.41), left ventricular dysfunction (ROR = 5.27), mitral valve disease (ROR = 3.78), and aortic valve incompetence (ROR = 4.71). Axi-cel also showed signals of cardiomyopathy (ROR = 4.43) and cardiopulmonary failure (ROR = 4.41) (Table 3).
Vascular disorders: Hypotension was the most common AE, showing strong signals across several drugs. Shock was also detected for Tisa-cel (ROR = 3.20), Axi-cel (ROR = 2.87), Brexu-cel (ROR = 4.31), and Ide-cel (ROR = 4.41), which was not mentioned on the drug labels. Additionally, Tisa-cel was associated with veno-occlusive disease (ROR = 7.03) and hypoperfusion (ROR = 21.54). Axi-cel was associated with hypertensive emergency (ROR = 7.85) and deep vein thrombosis (ROR = 1.85). Ide-cel was found to be associated with hypertension (ROR = 2.40) (Table 3).
2.3. Clinical Characteristics of the Adverse Events
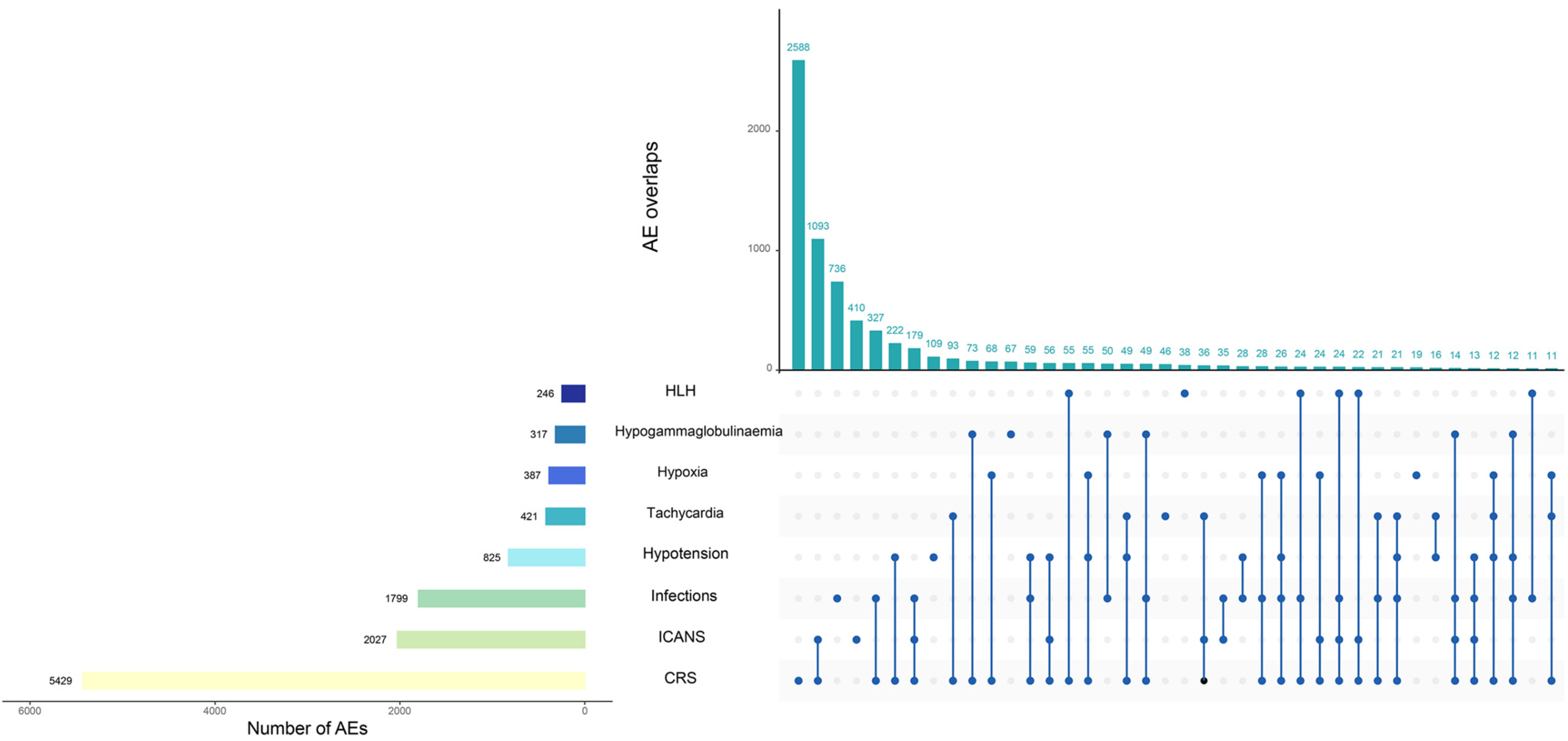
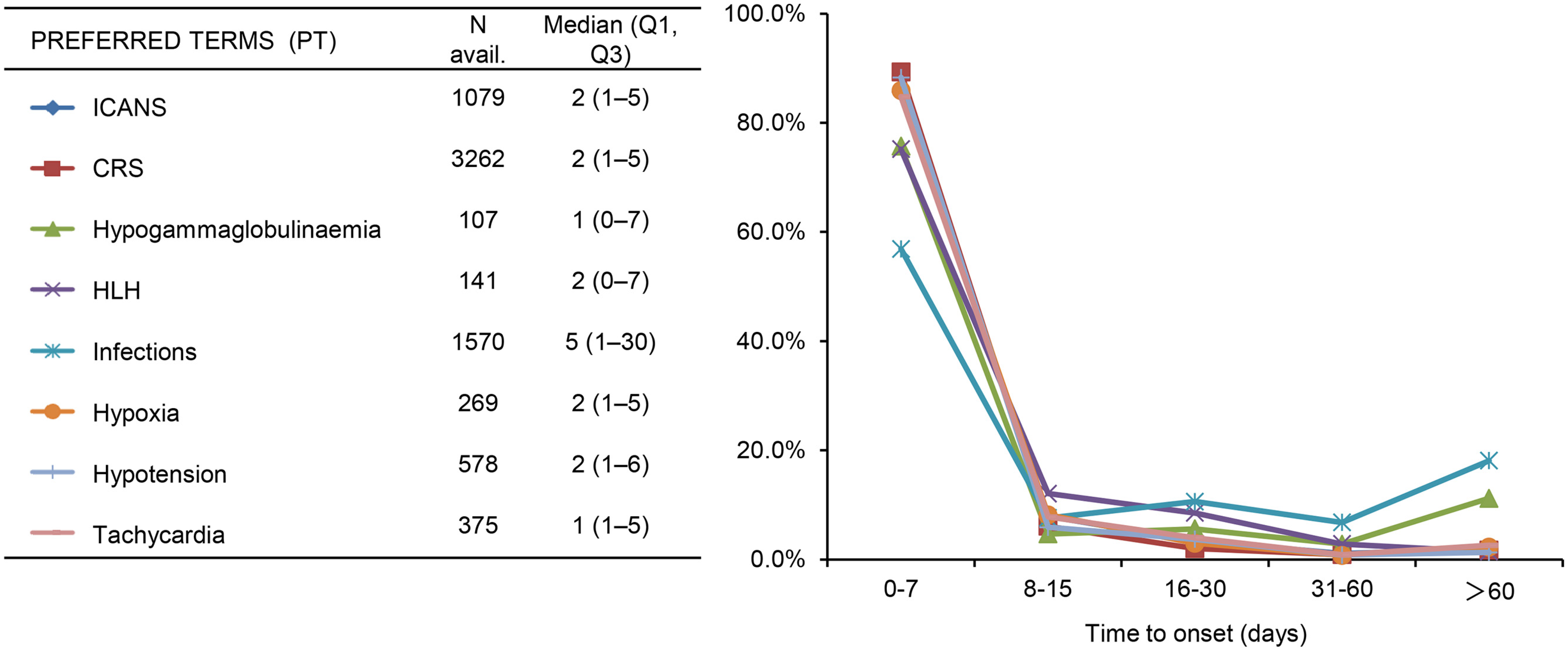
Among the AEs of the target, most AEs overlapped with CRS (overlap rate 49.6%-84.8%). The majority of AEs occurred within 7 days after infusion, with some cases of hypogammaglobulinemia and infections occurring later, more than 60 days after infusion, accounting for 11.2% and 18.1%, respectively, as shown in Figure 3 and Figure 4.
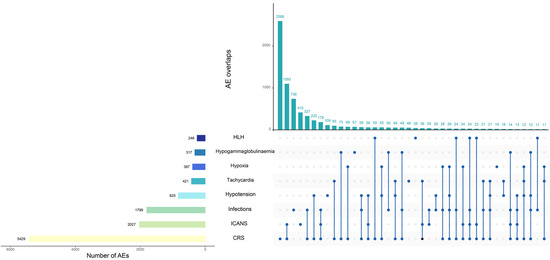
Figure 3.
Overlap within major adverse events.
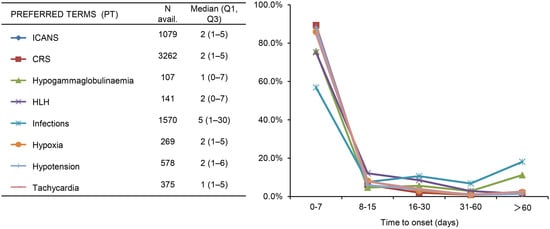
Figure 4.
Days from CAR T-cell infusion to adverse event onset.
3. Discussion
The emergence of CAR T-cell therapy has expanded the therapeutic options available for treating hematological tumors. However, safety remains a paramount concern for both medical practitioners and patients when making treatment decisions involving these drugs. This study conducted a comparative analysis of the AE signals of Tisa-cel, Axi-cel, Brexu-cel, Liso-cel, Ide-cel, and Cilta-cel within the FAERS database. By examining both common and rare serious AEs, we obtained comprehensive insights into the safety profiles of these six drugs. These findings indicate that the toxicity profile of CAR T-cell therapy is relatively distinctive and potentially affects nearly every major organ system. Patients may experience toxicities in the respiratory, cardiovascular, hematological, renal, neurological, and gastrointestinal systems, ranging from mild to life-threatening. Furthermore, there are variations in AEs among different CAR T-cell products. While the detected AEs generally align with those reported in the drug labels, this study also identified some novel AE signals, warranting clinical attention.
Neurotoxicity is one of the most prevalent AEs in CAR T-cell therapy, with an incidence ranging from 21% to 66% [33,34,35], and strong signal intensity was detected in this study. In CD19 CAR T-cell therapy, ICANS ranges from altered consciousness to severe brain edema, while in BCMA CAR T-cell therapy, notable toxicity, such as parkinsonism, has occurred in pivotal clinical trials for multiple myeloma [24,25], consistent with the findings of this study. The on-target/off-tumor effect on BCMA+ cells in the basal ganglia is a potential mechanism. However, the reversibility and decline in frontal lobe metabolism suggest additional pathological mechanisms that necessitate further elucidation [36,37]. This parkinsonism, characterized by neurocognitive and dyskinetic features, is sparsely documented in published studies, contrasting with the neurotoxicity observed during CAR T-cell proliferation and cytokine release. Notably, this Parkinson-like neurotoxicity progresses and manifests nearly 3 months after the initiation of CAR T-cell infusion, warranting heightened clinical vigilance. Apart from monitoring CAR T-cell levels, clinicians can employ simple assessments, such as handwriting evaluations, during post-CAR T-cell monitoring. Any observed changes should prompt the consideration of proactive interventions, including steroid administration or alternative therapies, to mitigate effects prior to inducing brain injury. Signals of brain edema were also detected by Tisa-cel, Axi-cel, and Brexu-cel. Patients may rapidly transition from mild lethargy to unconsciousness within hours, culminating in fatality [35,38,39], underscoring the importance of vigilance.
CRS is the most common AE after CAR T-cell infusion, showing strong signal intensity across all six drugs evaluated in this study. The risk, severity, and duration of CRS subsequent to CAR T-cell therapy may be modulated by host-, tumor-, and/or treatment-related factors. Patients with a heightened tumor burden, intensified pretreatment, and elevated baseline levels of C-reactive protein, ferritin, D-dimer, and proinflammatory cytokines may face increased susceptibility to CRS and severe manifestations thereof. Moreover, variations exist in the incidence and severity of CRS across different CAR T-cell products. The incidence of moderate to severe CRS in Tisa-cel, Axi-cel, and Brexu-cel ranges from 8% to 48% [40,41,42], whereas the incidence of CRS in Liso-cel is relatively lower, at 1.1% to 9% [43]. With respect to BCMA, Ide-cel and Cilta-cel exhibit moderate to severe CRS incidence rates ranging from 3% to 9% [44,45]. Characterized by hypotension and hyperthermia, moderate to severe CRS may progress to shock, vascular leak syndrome, disseminated intravascular coagulation (DIC), and multiple organ dysfunction syndrome (MODS), posing life-threatening risks [46]. Continuous electrocardiogram (ECG) monitoring from CAR T-cell reinfusion onset is recommended, enabling early intervention to reverse CRS, including severe cases. Importantly, preventive measures against CRS do not compromise CAR T-cell functionality [47].
Patients receiving CAR T-cell therapy are often in advanced stages of disease, have received multiple lines of treatment, and require pretreatment chemotherapy before CAR T-cell infusion, which often results in severe bone marrow suppression, increasing the risk of infection. There are notable disparities in the pathogens responsible for infections within 30 days post-CAR T-cell infusion compared to those occurring after 30 days. The majority of infections occur within 30 days post-infusion, predominantly bacterial, followed by viral and fungal infections [48]. At 30 days post-infusion, the infection rate declines, but due to decreased immunoglobulin and lymphocytes, viral infections, including respiratory viruses, cytomegalovirus, herpes viruses, and Epstein–Barr virus, become predominant. In this study, a greater incidence of bacterial and viral infections was observed, consistent with previous research findings. The incidence of infection related to CAR T-cell therapy varies significantly across different primary diseases, CAR T-cell therapy products, and medical centers [33]. Signal comparison revealed that compared to other drugs, Cilta-cel poses a relatively greater risk of bacterial, viral, and fungal infections, suggesting that patients receiving Cilta-cel treatment are more susceptible to infections. William et al. reported that infection is a leading cause of non-relapse mortality (NRM) among multiple myeloma patients receiving CAR T-cell therapy [49]. Hence, infection prevention and control are paramount in CAR T-cell therapy and warrant anti-infective treatment according to relevant guidelines. Additionally, attention should be given to patients’ immunoglobulin levels, with intravenous immunoglobulin supplementation administered when necessary [50,51].
Bone marrow suppression associated with CAR T-cell therapy ranks among the common complications in patients with hematological malignancies, characterized by leukopenia, anemia, or thrombocytopenia, often with multiline involvement and a higher incidence of AEs above grade 3. Approximately 30% of patients experience a recovery period exceeding one month [52]. Signal comparison indicated that compared with other drugs, Tisa-cel has the highest risk of hematological toxicity [40,41,42,43,44,45]. High-dose pretreatment can lead to decreased blood cell counts post-CAR T-cell therapy, with severe CRS, infections, high tumor burden, and low baseline blood cell levels contributing to delayed hematopoietic recovery. Although some patients experience prolonged recovery times for blood cells, they do not necessarily develop serious delayed complications and thus do not require specific treatment [17]. However, increased attention should be given to the heightened infection risk during periods of blood cell decline, with hematopoietic growth factors and blood product transfusions administered as necessary [53,54]. Approximately 90% of patients receiving CAR T-cell therapy exhibit at least one abnormal coagulation index, manifested by increased D-dimer levels, decreased blood fibrinogen levels, prolonged activated partial thromboplastin time, and prolonged prothrombin time [55]. In this study, Tisa-cel and Axi-cel exhibited strong signal intensities, while other drugs did not, likely due to their later market introduction and limited data availability. Current understanding suggests that abnormal coagulation function is primarily related to severe CRS and CAR-HLH. It is crucial to note that thrombocytopenia combined with abnormal coagulation can exacerbate bleeding risk, potentially resulting in life-threatening organ bleeding (e.g., cerebral hemorrhage, alveolar hemorrhage, and gastrointestinal bleeding), necessitating close clinical monitoring.
In addition to common AEs, this study analyzed rare but life-threatening AEs. Previous research has demonstrated that CAR T-cell therapy may induce various cardiorespiratory toxicities with high mortality rates [56,57,58,59,60]. Our study revealed a broad spectrum of cardiorespiratory toxicity, with 39 signals disproportionately associated with CAR T-cell therapy, indicating multifaceted cardiorespiratory toxicity related to CAR T-cell therapy. Understanding the diversity in toxicities and the potential risks associated with these drugs is crucial for enhancing toxicity management, representing one of the most important avenues for overall improvement in CAR T-cell therapy. Notably, signals such as hypoxia, tachypnoea, cardiorenal syndrome, and hypotension stand out due to their strong disproportionality. Moreover, some toxicities, such as atelectasis and shock, are underrepresented in published data or remain inadequately recognized. By presenting all potential signals and quantifying their risks, we offer a comprehensive and systematic insight into these rare toxicities, which is a crucial complement to current pharmacovigilance research. Notably, there was a significant overlap between CAR T-cell-related CRS and CAR T-cell-related cardiorespiratory toxicity, consistent with previous findings [56,58,59,61]. However, the underlying pathological mechanisms of heart injury associated with this novel therapy remain unclear. Patients with evident or underlying cardiovascular diseases may be more susceptible to CAR T-cell-related cardiotoxicity [62]. Therefore, a detailed cardiovascular history and physical examination should be conducted before treatment initiation. A retrospective study at Massachusetts General Hospital revealed that cardiovascular events occurred only in patients with grade ≥ 2 CRS, with longer durations between CRS onset and tocilizumab administration associated with higher cardiovascular event risks, increasing by 1.7 times every 12 h. Early tocilizumab use for CRS treatment can mitigate the risk of cardiovascular AEs [56]. Mahmood et al. also reported that combined severe cardiovascular events, such as heart failure, cardiogenic shock, or myocardial infarction, increase the risk of death and correlate with increased peak levels of IL-6, CRP, ferritin, and troponin. Clinicians should remain vigilant regarding these rare but potentially fatal cardiovascular toxicities following CAR T-cell therapy. Monitoring, including continuous echocardiography, baseline biomarkers, and electrocardiograms, should be intensified during treatment.
This study has certain limitations. First, the research data were sourced from a spontaneous reporting system (SRS); underreporting is one of the most important limitations on SRS, as it prevents the precise calculation of the real incidence of the event in the population. In fact, only a small proportion of the AEs that occur in daily practice are reported [63]. However, large-scale data mining still contributes to warning about the safe and rational use of drugs. Second, the reports in the FAERS database predominantly originated from European and American countries, with a relatively low proportion from Asian populations, potentially resulting in geographical bias in the results. Locke et al.’s study [64] indicated that ICANS might vary by race, and we plan to conduct retrospective or prospective studies incorporating more Asian populations to achieve a more comprehensive analysis of AEs. Third, all signal detection results can only indicate potential associations between drugs and adverse events; they cannot establish a definitive causal relationship between drugs and adverse events. In the future, we will conduct prospective observational studies or clinical trials to determine the causal relationship between CAR T-cell therapy and AEs. Future research combining the FAERS database with other data sources is crucial for continuous monitoring of CAR T-cell-related toxicity.
4. Materials and Methods
4.1. Study Design and Data Source
This was a real-world, observational, retrospective pharmacovigilance study, and the data were obtained from the FAERS database. Six CAR T-cell products approved by the FDA (tisagenlecleucel, axicabtagene ciloleucel, brexucabtagene autoleucel, lisocabtagene maraleucel, idecabtagene vicleucel, and ciltacabtagene autoleucel) were selected as the study drugs. All files are available on the FDA website “https://fis.fda.gov/extensions/fpd-qde-faers/fpd-qde-faers.html (accessed on 25 April 2024)”. In this study, all data from 26 quarters of the ASCII packets, spanning from the fourth quarter of 2017 to the first quarter of 2024, were extracted and imported into SAS 9.4 software for data cleaning and analysis. Since the FAERS is a publicly available and anonymized database, neither informed consent nor ethical approval was involved.
4.2. Data Extraction and Mining
The data extraction and mining processes used in this study are shown in Figure 1. The target population was screened based on DRUGNAME and PROD_AI, with the degree of reporting suspicion limited to “primary suspected drug (PS)”. According to the FDA’s recommended method for eliminating duplicate reports, the fields PRIMARYID, CASEID, and FDA_DT from the DEMO table were selected and sorted by CASEID, FDA_DT, and PRIMARYID. For reports with the same CASE number, the latest (most recent) FDA_DT was selected. For those occasions when both the CASE and FDA_DT fields were the same, the report with the higher ISR was selected.
Since the FAERS database records AE names using the preferred terms (PT) terminology of the Medical Dictionary for Regulatory Activities (MedDRA), and the MedDRA is updated every March and September, involving adjustments to PT levels and changes to system organ classes (SOCs), the latest version of the MedDRA was used to correct the PT names in the FAERS database. The SOC and PT from the latest version of the MedDRA were obtained. Clinical characteristics, including demographic features (age and sex), reporting characteristics (reporting year, region, and reporter’s occupation), and reporting indications, were also collected. Additionally, the time to onset of specific AEs was also assessed, calculated as the interval between the start date of medication (START_DT) and the time of occurrence of AEs (EVENT_DT). Reports with missing or incorrect data (drug usage time later than the time of event occurrence) were excluded.
4.3. Statistical Analysis
The measure of disproportionality is the main method used for research on AE signals and is based on the two-by-two contingency table (Table S1). Its principle is to compare the difference between the frequency of the target drug event and the background frequency. When the frequency of the target drug event is significantly higher than the background frequency and exceeds the set threshold, it is called disproportionality, indicating that some connection may exist between the suspicious drugs and suspected AEs, not due to chance factors or the “noisy background” of the database [65,66,67].
The disproportionality analysis was conducted using the reporting odds ratio (ROR) method and the Medicines and Healthcare Products Regulatory Agency (MHRA) method, which have high reliability and sensitivity in the proportional imbalance method. The study used the ROR and its confidence interval and the proportional reporting ratio (PRR) and its χ2 value to detect the AE signal. To avoid the appearance of false positive signals, the data should meet the number of AE reports ≥ 3, the 95% CI lower limit of ROR > 1, PRR > 2, and χ2 > 4, further excluding reports that did not meet the requirements [68]. The signal intensities were arranged in descending order of the ROR value. The larger the ROR is, the stronger the signal, indicating a stronger correlation between the drug and the AE. All data processing and statistical analysis were performed using SPSS version 26.0 and Prism version 10.1.
5. Conclusions
CRS and ICANS are the most common AEs associated with CAR T-cell therapy. Apart from these, additional AEs may include infection, cytopenia, hypogammaglobulinemia, HLH, coagulation dysfunction, and hypotension. Furthermore, there were variations in the AE spectra among the different CAR T-cell products. Clinicians should assess patients prior to medication and closely monitor their vital signs, mental status, and laboratory parameters during treatment. Prompt intervention should be implemented if AEs occur, thereby effectively reducing the clinical risks associated with medication.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ph17081025/s1, Table S1: Two-by-two contingency table for disproportionality analysis.
Author Contributions
Conceptualization, Q.D. and J.L.; methodology, Y.D.; software, Z.G.; formal analysis, Z.G.; investigation, Z.G.; resources, Y.D.; data curation, M.W. and Q.Z.; writing—original draft preparation, Z.G. and Y.D.; writing—review and editing, Q.D. and J.L.; project administration, Q.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the “Young Eagle” Program of the Shanghai Anti-Cancer Association (grant number: SACA-CY21B04) and the “Soaring” Program of the Shanghai Anti-Cancer Association (grant number: SACA-AX202110).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The FDA Adverse Event Reporting System data are available at https://fis.fda.gov/extensions/fpd-qde-faers/fpd-qde-faers.html (accessed on 26 April 2024).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- June, C.H.; Sadelain, M. Chimeric Antigen Receptor Therapy. N. Engl. J. Med. 2018, 379, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tan, S.Y.E.; Zhao, H.; Ni, F.; Hu, Y.; Huang, H. CAR-T cells: The Chinese experience. Expert Opin. Biol. Ther. 2020, 20, 1293–1308. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Guo, Y.; Wang, Y.; Wu, Z.; Bo, J.; Zhang, B.; Zhu, J.; Han, W. Clinical development of CAR T cell therapy in China: 2020 update. Cell. Mol. Immunol. 2021, 18, 792–804. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Riviere, I.; Gonen, M.; Wang, X.; Senechal, B.; Curran, K.J.; Sauter, C.; Wang, Y.; Santomasso, B.; Mead, E.; et al. Long-Term Follow-up of CD19 CAR Therapy in Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Wu, Z.; Luo, Y.; Shi, J.; Yu, J.; Pu, C.; Liang, Z.; Wei, G.; Cui, Q.; Sun, J.; et al. Potent Anti-leukemia Activities of Chimeric Antigen Receptor-Modified T Cells against CD19 in Chinese Patients with Relapsed/Refractory Acute Lymphocytic Leukemia. Clin. Cancer Res. 2017, 23, 3297–3306. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Wang, G.; Cheng, H.; Wei, C.; Qi, K.; Sang, W.; Zhenyu, L.; Shi, M.; Li, H.; Qiao, J.; et al. Potent anti-leukemia activities of humanized CD19-targeted Chimeric antigen receptor T (CAR-T) cells in patients with relapsed/refractory acute lymphoblastic leukemia. Am. J. Hematol. 2018, 93, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Li, C.; Yin, P.; Guo, T.; Liu, L.; Xia, L.; Wu, Y.; Zhou, F.; Ai, L.; Shi, W.; et al. Anti-CD19 chimeric antigen receptor-modified T-cell therapy bridging to allogeneic hematopoietic stem cell transplantation for relapsed/refractory B-cell acute lymphoblastic leukemia: An open-label pragmatic clinical trial. Am. J. Hematol. 2019, 94, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Zhao, M.; Hu, Y.; Wang, Y.; Li, P.; Cao, J.; Shi, M.; Tan, J.; Zhang, M.; Xiao, X.; et al. Efficacy and safety of CD19-specific CAR T cell-based therapy in B-cell acute lymphoblastic leukemia patients with CNSL. Blood 2022, 139, 3376–3386. [Google Scholar] [CrossRef]
- Shah, B.D.; Ghobadi, A.; Oluwole, O.O.; Logan, A.C.; Boissel, N.; Cassaday, R.D.; Leguay, T.; Bishop, M.R.; Topp, M.S.; Tzachanis, D.; et al. KTE-X19 for relapsed or refractory adult B-cell acute lymphoblastic leukaemia: Phase 2 results of the single-arm, open-label, multicentre ZUMA-3 study. Lancet 2021, 398, 491–502. [Google Scholar] [CrossRef]
- Wang, T.; Tang, Y.; Cai, J.; Wan, X.; Hu, S.; Lu, X.; Xie, Z.; Qiao, X.; Jiang, H.; Shao, J.; et al. Coadministration of CD19- and CD22-Directed Chimeric Antigen Receptor T-Cell Therapy in Childhood B-Cell Acute Lymphoblastic Leukemia: A Single-Arm, Multicenter, Phase II Trial. J. Clin. Oncol. 2023, 41, 1670–1683. [Google Scholar] [CrossRef] [PubMed]
- Leahy, A.B.; Newman, H.; Li, Y.; Liu, H.; Myers, R.; DiNofia, A.; Dolan, J.G.; Callahan, C.; Baniewicz, D.; Devine, K.; et al. CD19-targeted chimeric antigen receptor T-cell therapy for CNS relapsed or refractory acute lymphocytic leukaemia: A post-hoc analysis of pooled data from five clinical trials. Lancet Haematol. 2021, 8, e711–e722. [Google Scholar] [CrossRef] [PubMed]
- Hiramatsu, H.; Adachi, S.; Umeda, K.; Kato, I.; Eldjerou, L.; Agostinho, A.C.; Natsume, K.; Tokushige, K.; Watanabe, Y.; Grupp, S.A. Efficacy and safety of tisagenlecleucel in Japanese pediatric and young adult patients with relapsed/refractory B cell acute lymphoblastic leukemia. Int. J. Hematol. 2020, 111, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Y.; Liu, Y.; Tong, C.; Wang, C.; Guo, Y.; Ti, D.; Yang, Q.; Qiao, S.; Wu, Z.; et al. Long-term activity of tandem CD19/CD20 CAR therapy in refractory/relapsed B-cell lymphoma: A single-arm, phase 1-2 trial. Leukemia 2022, 36, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Sang, W.; Shi, M.; Yang, J.; Cao, J.; Xu, L.; Yan, D.; Yao, M.; Liu, H.; Li, W.; Zhang, B.; et al. Phase II trial of co-administration of CD19- and CD20-targeted chimeric antigen receptor T cells for relapsed and refractory diffuse large B cell lymphoma. Cancer Med. 2020, 9, 5827–5838. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.; Zhang, Y.; Liu, Y.; Ji, X.; Zhang, W.; Guo, Y.; Han, X.; Ti, D.; Dai, H.; Wang, C.; et al. Optimized tandem CD19/CD20 CAR-engineered T cells in refractory/relapsed B-cell lymphoma. Blood 2020, 136, 1632–1644. [Google Scholar] [CrossRef] [PubMed]
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.M.; et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): A single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Maric, I.; Hartman, S.D.; Rose, J.J.; Wang, M.; Lam, N.; Stetler-Stevenson, M.; Salem, D.; Yuan, C.; Pavletic, S.; et al. T Cells Genetically Modified to Express an Anti-B-Cell Maturation Antigen Chimeric Antigen Receptor Cause Remissions of Poor-Prognosis Relapsed Multiple Myeloma. J. Clin. Oncol. 2018, 36, 2267–2280. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.H.; Liu, J.; Wang, B.Y.; Chen, Y.X.; Cao, X.M.; Yang, Y.; Zhang, Y.L.; Wang, F.X.; Zhang, P.Y.; Lei, B.; et al. A phase 1, open-label study of LCAR-B38M, a chimeric antigen receptor T cell therapy directed against B cell maturation antigen, in patients with relapsed or refractory multiple myeloma. J. Hematol. Oncol. 2018, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.D.; Garfall, A.L.; Stadtmauer, E.A.; Melenhorst, J.J.; Lacey, S.F.; Lancaster, E.; Vogl, D.T.; Weiss, B.M.; Dengel, K.; Nelson, A.; et al. B cell maturation antigen-specific CAR T cells are clinically active in multiple myeloma. J. Clin. Investig. 2019, 129, 2210–2221. [Google Scholar] [CrossRef]
- Raje, N.; Berdeja, J.; Lin, Y.; Siegel, D.; Jagannath, S.; Madduri, D.; Liedtke, M.; Rosenblatt, J.; Maus, M.V.; Turka, A.; et al. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 380, 1726–1737. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Cao, J.; Cheng, H.; Qiao, J.; Zhang, H.; Wang, Y.; Shi, M.; Lan, J.; Fei, X.; Jin, L.; et al. A combination of humanised anti-CD19 and anti-BCMA CAR T cells in patients with relapsed or refractory multiple myeloma: A single-arm, phase 2 trial. Lancet Haematol. 2019, 6, e521–e529. [Google Scholar] [CrossRef] [PubMed]
- Mei, H.; Li, C.; Jiang, H.; Zhao, X.; Huang, Z.; Jin, D.; Guo, T.; Kou, H.; Liu, L.; Tang, L.; et al. A bispecific CAR-T cell therapy targeting BCMA and CD38 in relapsed or refractory multiple myeloma. J. Hematol. Oncol. 2021, 14, 161. [Google Scholar] [CrossRef] [PubMed]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): A phase 1b/2 open-label study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Anderson, L.J.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Mullard, A. FDA approves first CAR T therapy. Nat. Rev. Drug Discov. 2017, 16, 669. [Google Scholar] [CrossRef]
- FDA. FDA Approves Second CAR T-cell Therapy. Cancer Discov. 2018, 8, 5–6. [Google Scholar] [CrossRef]
- Hou, J.Z.; Ye, J.C.; Pu, J.J.; Liu, H.; Ding, W.; Zheng, H.; Liu, D. Novel agents and regimens for hematological malignancies: Recent updates from 2020 ASH annual meeting. J. Hematol. Oncol. 2021, 14, 66. [Google Scholar] [CrossRef] [PubMed]
- Mullard, A. FDA approves first BCMA-targeted CAR-T cell therapy. Nat. Rev. Drug Discov. 2021, 20, 332. [Google Scholar] [CrossRef]
- Mullard, A. FDA approves fourth CAR-T cell therapy. Nat. Rev. Drug Discov. 2021, 20, 166. [Google Scholar] [CrossRef]
- Cai, C.; Tang, D.; Han, Y.; Shen, E.; Abdihamid, O.; Guo, C.; Shen, H.; Zeng, S. A comprehensive analysis of the fatal toxic effects associated with CD19 CAR-T cell therapy. Aging (Albany Ny) 2020, 12, 18741–18753. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Frey, N.; Shaw, P.A.; Aplenc, R.; Barrett, D.M.; Bunin, N.J.; Chew, A.; Gonzalez, V.E.; Zheng, Z.; Lacey, S.F.; et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 2014, 371, 1507–1517. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jager, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.M.; May, S.; Lei, M.; Qualls, S.; Bushey, K.; Rubin, D.B.; Barra, M.E. CAR T-Cell-Associated Neurotoxicity: Current Management and Emerging Treatment Strategies. Crit. Care Nurs. Q. 2020, 43, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Freyer, C.W.; Porter, D.L. Cytokine release syndrome and neurotoxicity following CAR T-cell therapy for hematologic malignancies. J. Allergy. Clin. Immunol. 2020, 146, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Van Oekelen, O.; Aleman, A.; Upadhyaya, B.; Schnakenberg, S.; Madduri, D.; Gavane, S.; Teruya-Feldstein, J.; Crary, J.F.; Fowkes, M.E.; Stacy, C.B.; et al. Neurocognitive and hypokinetic movement disorder with features of parkinsonism after BCMA-targeting CAR-T cell therapy. Nat. Med. 2021, 27, 2099–2103. [Google Scholar] [CrossRef] [PubMed]
- Karschnia, P.; Miller, K.C.; Yee, A.J.; Rejeski, K.; Johnson, P.C.; Raje, N.; Frigault, M.J.; Dietrich, J. Neurologic toxicities following adoptive immunotherapy with BCMA-directed CAR T cells. Blood 2023, 142, 1243–1248. [Google Scholar] [CrossRef]
- Torre, M.; Solomon, I.H.; Sutherland, C.L.; Nikiforow, S.; DeAngelo, D.J.; Stone, R.M.; Vaitkevicius, H.; Galinsky, I.A.; Padera, R.F.; Trede, N.; et al. Neuropathology of a Case With Fatal CAR T-Cell-Associated Cerebral Edema. J. Neuropathol. Exp. Neurol. 2018, 77, 877–882. [Google Scholar] [CrossRef]
- Schuster, S.J.; Svoboda, J.; Chong, E.A.; Nasta, S.D.; Mato, A.R.; Anak, O.; Brogdon, J.L.; Pruteanu-Malinici, I.; Bhoj, V.; Landsburg, D.; et al. Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas. N. Engl. J. Med. 2017, 377, 2545–2554. [Google Scholar] [CrossRef]
- FDA. KYMRIAH® (Tisagenlecleucel) Suspension for Intravenous Infusion Initial U.S. Approval: 2017. Available online: https://www.fda.gov/media/107296/download?attachment (accessed on 23 April 2024).
- FDA. TECARTUS® (Brexucabtagene autoleucel) Suspension for Intravenous Infusion Initial U.S. Approval: 2020. Available online: https://www.fda.gov/media/140409/download?attachment (accessed on 23 April 2024).
- FDA. YESCARTA® (Axicabtagene ciloleucel) Suspension for Intravenous Infusion Initial U.S. Approval: 2017. Available online: https://www.fda.gov/media/108377/download?attachment (accessed on 23 April 2024).
- FDA. BREYANZI® (Lisocabtagene maraleucel) Suspension for Intravenous Infusion Initial U.S. Approval: 2021. Available online: https://www.fda.gov/media/145711/download?attachment (accessed on 23 April 2024).
- FDA. ABECMA® (Idecabtagene vicleucel), Suspension for Intravenous Infusion Initial U.S. Approval: 2021. Available online: https://www.fda.gov/media/147055/download?attachment (accessed on 23 April 2024).
- FDA. CARVYKTI® (Ciltacabtagene autoleucel) Suspension for Intravenous Infusion Initial U.S. Approval: 2022. Available online: https://www.fda.gov/media/156560/download?attachment (accessed on 23 April 2024).
- Morris, E.C.; Neelapu, S.S.; Giavridis, T.; Sadelain, M. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nat. Rev. Immunol. 2022, 22, 85–96. [Google Scholar] [CrossRef]
- Zhou, L.; Fu, W.; Wu, S.; Xu, K.; Qiu, L.; Xu, Y.; Yan, X.; Zhang, Q.; Zhang, M.; Wang, L.; et al. Derivation and validation of a novel score for early prediction of severe CRS after CAR-T therapy in haematological malignancy patients: A multi-centre study. Br. J. Haematol. 2023, 202, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Wudhikarn, K.; Palomba, M.L.; Pennisi, M.; Garcia-Recio, M.; Flynn, J.R.; Devlin, S.M.; Afuye, A.; Silverberg, M.L.; Maloy, M.A.; Shah, G.L.; et al. Infection during the first year in patients treated with CD19 CAR T cells for diffuse large B cell lymphoma. Blood Cancer J. 2020, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Wesson, W.; Dima, D.; Suleman, N.; Saif, M.; Tabak, C.; Logan, E.; Davis, J.A.; McGann, M.; Furqan, F.; Mohan, M.; et al. Timing of Toxicities and Non-Relapse Mortality Following CAR T Therapy in Myeloma. Transpl. Cell. Ther. 2024, S2666–S6367. [Google Scholar] [CrossRef] [PubMed]
- Yakoub-Agha, I.; Chabannon, C.; Bader, P.; Basak, G.W.; Bonig, H.; Ciceri, F.; Corbacioglu, S.; Duarte, R.F.; Einsele, H.; Hudecek, M.; et al. Management of adults and children undergoing chimeric antigen receptor T-cell therapy: Best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica 2020, 105, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Doan, A.; Pulsipher, M.A. Hypogammaglobulinemia due to CAR T-cell therapy. Pediatr. Blood Cancer 2018, 65, 1–2. [Google Scholar] [CrossRef]
- Schubert, M.L.; Schmitt, M.; Wang, L.; Ramos, C.A.; Jordan, K.; Muller-Tidow, C.; Dreger, P. Side-effect management of chimeric antigen receptor (CAR) T-cell therapy. Ann. Oncol. 2021, 32, 34–48. [Google Scholar] [CrossRef]
- Brudno, J.N.; Kochenderfer, J.N. Toxicities of chimeric antigen receptor T cells: Recognition and management. Blood 2016, 127, 3321–3330. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.A.; Li, D.; Hay, K.A.; Green, M.L.; Cherian, S.; Chen, X.; Riddell, S.R.; Maloney, D.G.; Boeckh, M.; Turtle, C.J. Infectious complications of CD19-targeted chimeric antigen receptor-modified T-cell immunotherapy. Blood 2018, 131, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qi, K.; Cheng, H.; Cao, J.; Shi, M.; Qiao, J.; Yan, Z.; Jing, G.; Pan, B.; Sang, W.; et al. Coagulation Disorders after Chimeric Antigen Receptor T Cell Therapy: Analysis of 100 Patients with Relapsed and Refractory Hematologic Malignancies. Biol. Blood Marrow Transplant. 2020, 26, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Alvi, R.M.; Frigault, M.J.; Fradley, M.G.; Jain, M.D.; Mahmood, S.S.; Awadalla, M.; Lee, D.H.; Zlotoff, D.A.; Zhang, L.; Drobni, Z.D.; et al. Cardiovascular Events Among Adults Treated With Chimeric Antigen Receptor T-Cells (CAR-T). J. Am. Coll. Cardiol. 2019, 74, 3099–3108. [Google Scholar] [CrossRef]
- Ganatra, S.; Redd, R.; Hayek, S.S.; Parikh, R.; Azam, T.; Yanik, G.A.; Spendley, L.; Nikiforow, S.; Jacobson, C.; Nohria, A. Chimeric Antigen Receptor T-Cell Therapy-Associated Cardiomyopathy in Patients With Refractory or Relapsed Non-Hodgkin Lymphoma. Circulation 2020, 142, 1687–1690. [Google Scholar] [CrossRef]
- Lefebvre, B.; Kang, Y.; Smith, A.M.; Frey, N.V.; Carver, J.R.; Scherrer-Crosbie, M. Cardiovascular Effects of CAR T Cell Therapy: A Retrospective Study. Jacc-Cardiooncol. 2020, 2, 193–203. [Google Scholar] [CrossRef]
- Goldman, A.; Maor, E.; Bomze, D.; Liu, J.E.; Herrmann, J.; Fein, J.; Steingart, R.M.; Mahmood, S.S.; Schaffer, W.L.; Perales, M.A.; et al. Adverse Cardiovascular and Pulmonary Events Associated With Chimeric Antigen Receptor T-Cell Therapy. J. Am. Coll. Cardiol. 2021, 78, 1800–1813. [Google Scholar] [CrossRef]
- Steiner, R.E.; Banchs, J.; Koutroumpakis, E.; Becnel, M.; Gutierrez, C.; Strati, P.; Pinnix, C.C.; Feng, L.; Rondon, G.; Claussen, C.; et al. Cardiovascular events in patients treated with chimeric antigen receptor T-cell therapy for aggressive B-cell lymphoma. Haematologica 2022, 107, 1555–1566. [Google Scholar] [CrossRef]
- Shalabi, H.; Sachdev, V.; Kulshreshtha, A.; Cohen, J.W.; Yates, B.; Rosing, D.R.; Sidenko, S.; Delbrook, C.; Mackall, C.; Wiley, B.; et al. Impact of cytokine release syndrome on cardiac function following CD19 CAR-T cell therapy in children and young adults with hematological malignancies. J. Immunother. Cancer 2020, 8, e001159. [Google Scholar] [CrossRef]
- Totzeck, M.; Michel, L.; Lin, Y.; Herrmann, J.; Rassaf, T. Cardiotoxicity from chimeric antigen receptor-T cell therapy for advanced malignancies. Eur. Heart J. 2022, 43, 1928–1940. [Google Scholar] [CrossRef]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug. Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Locke, F.L.; Siddiqi, T.; Jacobson, C.A.; Ghobadi, A.; Ahmed, S.; Miklos, D.B.; Perales, M.A.; Munoz, J.; Fingrut, W.B.; Pennisi, M.; et al. Real-world and clinical trial outcomes in large B-cell lymphoma with axicabtagene ciloleucel across race and ethnicity. Blood. 2024, 143, 2722–2734. [Google Scholar] [CrossRef]
- Bate, A.; Lindquist, M.; Edwards, I.R.; Olsson, S.; Orre, R.; Lansner, A.; De Freitas, R.M. A Bayesian neural network method for adverse drug reaction signal generation. Eur. J. Clin. Pharmacol. 1998, 54, 315–321. [Google Scholar] [CrossRef]
- van Puijenbroek, E.; Diemont, W.; van Grootheest, K. Application of quantitative signal detection in the Dutch spontaneous reporting system for adverse drug reactions. Drug. Saf. 2003, 26, 293–301. [Google Scholar] [CrossRef]
- Evans, S.J.; Waller, P.C.; Davis, S. Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol. Drug Saf. 2001, 10, 483–486. [Google Scholar] [CrossRef] [PubMed]
- van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).