Abstract
Gliomas, the most common type of primary malignant brain tumors in adults, pose significant challenges in diagnosis and management due to their heterogeneity and potential aggressiveness. This review evaluates the utility of O-(2-[18F]fluoroethyl)-L-tyrosine ([18F]FET) positron emission tomography (PET), a promising imaging modality, to enhance the clinical management of gliomas. We reviewed 82 studies involving 4657 patients, focusing on the application of [18F]FET in several key areas: diagnosis, grading, identification of IDH status and presence of oligodendroglial component, guided resection or biopsy, detection of residual tumor, guided radiotherapy, detection of malignant transformation in low-grade glioma, differentiation of recurrence versus treatment-related changes and prognostic factors, and treatment response evaluation. Our findings confirm that [18F]FET helps delineate tumor tissue, improves diagnostic accuracy, and aids in therapeutic decision-making by providing crucial insights into tumor metabolism. This review underscores the need for standardized parameters and further multicentric studies to solidify the role of [18F]FET PET in routine clinical practice. By offering a comprehensive overview of current research and practical implications, this paper highlights the added value of [18F]FET PET in improving management of glioma patients from diagnosis to follow-up.
1. Introduction
Gliomas represent the majority of primary malignant brain tumors in adults, with a yearly incidence of approximately 6 per 100,000 in Europe [1]. They are categorized according to the World Health Organization (WHO) classification into grades ranging from 1 to 4 depending on their malignancy [2]. Glioblastoma, the most aggressive and common type of glioma, remains incurable with an almost systematic progression within the year and a median survival of 14.6 months despite optimal treatment [3].
In high-grade tumors, treatment usually consists of maximal resection of the tumor (if feasible) followed by chemotherapy and radiotherapy depending on tumor grade and analysis of molecular markers (i.e., 1p/19q codeletion, IDH mutation, and MGMT promoter methylation) [4]. Treatment of grade 4 gliomas, the same since 2005, is based on the so-called “Stupp protocol”, which includes concomitant radiochemotherapy with Temozolomide [3].
Patients’ monitoring consists of MRI before and after treatment with periodic follow-up. An increase in enhancing areas is considered suspect of recurrence according to the Response Assessment in Neuro-Oncology (RANO) criteria but is not specific [5]. Indeed, frequent post-radiation changes such as pseudoprogression and radionecrosis can cause the same type of suspicious gadolinium-enhancing lesion.
Pseudoprogression typically occurs several weeks up to months (often less than 3 months) after completion of radiotherapy. This phenomenon is responsible for a transitory worsening of MR imaging with an increased contrast enhancement area, resolving without changes in treatment on subsequent MRI scans. There is generally no symptom associated.
Radionecrosis is a severe reaction to radiotherapy, which generally occurs later, months to several years after radiation therapy. MRI findings involve a space-occupying necrotic lesion with a mass effect, which can cause neurological dysfunction.
MRI changes can also be induced by treatments such as corticosteroids, antiangiogenic therapy, or immunotherapy.
For these reasons, there is a need to find other reliable methods to differentiate glioma recurrence from treatment-related changes, given the different managements of these two processes.
Different MRI techniques have been implemented in this indication, such as diffusion weighted imaging (DWI) [6], perfusion-weighted imaging (PWI) [7], and magnetic resonance spectroscopy (MRS) [8].
In nuclear medicine, positron emission tomography using 2-deoxy-2-[18F]fluoro-D-glucose ([18F]FDG) has already proven itself in oncology imaging and has become common practice in numerous pathologies. However, its physiologically high brain metabolism and increased uptake in inflammatory lesions make it difficult to appreciate tumor uptake [9].
Radiolabeled amino acids are preferred in neuro-oncology due to low uptake in normal brain tissue contrasting with increased uptake in neoplastic processes, resulting in a better signal-to-noise ratio [10].
The most widely used amino acid tracers for PET are [11C-methyl]-methionine ([11C]MET), O-(2-[18F]fluoroethyl)-L-tyrosine ([18F]FET), and 3,4dihydroxy-6-[18F]fluoro-L-phenylalanine ([18F]F-DOPA) (Table 1). Their uptake is believed to be driven by an overexpression of the L-type amino-acid transporter (LAT) by brain tumors (Figure 1).

Table 1.
Comparative table of different radiolabeled amino acids.
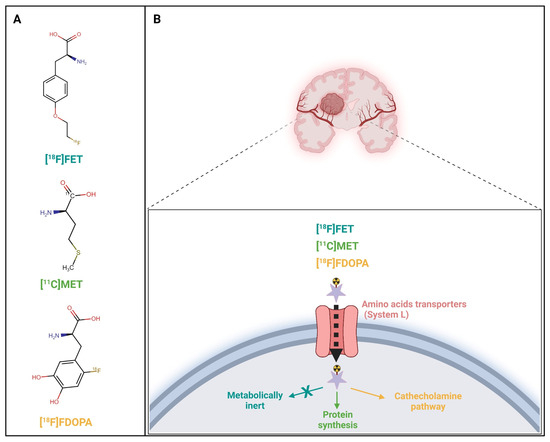
Figure 1.
Radiolabeled amino acids O-(2-[18F]fluoroethyl)-L-tyrosine ([18F]FET), [11C-methyl]-methionine ([11C]MET), and L-3,4-dihydroxy-6-[18F]fluoro-phenyl-alanine ([18F]FDOPA) metabolic pathways. Molecular structures (A) and associated uptake mechanism (B) of each radiolabeled amino acid. Created with BioRender.com.
Detailed Description of different radiolabeled amino acids
11C-Methionine ([11C]MET)
Mechanism: [11C]MET is an amino acid analog taken up by tumor cells via the L-type amino acid transporter (LAT). It reflects increased protein synthesis, which is often elevated in gliomas.
Advantages: High sensitivity in detecting both low- and high-grade gliomas; more effective in high-grade gliomas [11]. Provides rapid uptake and good contrast between tumor and normal brain tissue. It is particularly effective to detect tumor recurrence [12] and in monitoring therapy response [13].
Disadvantages: The short half-life of 11C (about 20 min) necessitates the use of an on-site cyclotron, limiting its use to specialized centers. [11C]MET may also accumulate in inflammatory tissues, leading to potential false positives [14].
[18F]F-DOPA
Mechanism: [18F]F-DOPA is a precursor to dopamine and is taken up by dopaminergic neurons, with uptake also observed in gliomas due to increased amino acid transport and altered tumor metabolism. It is decarboxylated to dopamine and subsequently trapped in cells.
Advantages: The longer half-life of 1⁸F (about 110 min) allows for broader clinical application as it can be transported from off-site production facilities. It has high sensitivity for gliomas [15] and is particularly useful in differentiating between tumor recurrence and radiation necrosis [16].
Disadvantages: Uptake of [18F]F-DOPA in inflamed tissues can lead to false-positive results [17].
1⁸F-Fluoroethyl-L-tyrosine ([18F]FET)
Mechanism: [18F]FET is an artificial amino acid taken up by glioma cells via LAT, reflecting the increased amino acid transport associated with tumor proliferation.
Advantages: [18F]FET has a longer half-life, like 1⁸F-DOPA, allowing it to be produced off-site. It has high sensitivity for gliomas, especially high-grade gliomas [18], with low uptake in inflammatory lesions, making it particularly effective in distinguishing tumor recurrence from treatment-induced changes. Additionally, dynamic acquisition allows information on tracer kinetics, particularly useful for tumor grading [19].
Disadvantages: Though it offers high specificity. There is also potential, though reduced, for uptake in inflammatory tissues [20].
While recent meta-analyses report high sensitivity and specificity of both 1⁸F-DOPA and [18F]FET to differentiate true progression to treatment-related changes, there are still discrepancies in determining the best radiolabeled amino acid [21,22,23].
[18F]FET market authorizations have been delivered in Europe recently, enabling its widespread use in hospitals.
Its high efficiency production and its half-life of 110 min allow its transportation to other sites. For these reasons, it is being increasingly used in glioma management in Europe.
In the present review, we aimed to summarize its performance in different indications in low- and high-grade gliomas.
2. Materials and Methods
2.1. Search Strategy
The primary literature was searched up to 31 December 2023, using the PubMed database.
A combination of the search terms «PET», «FET» OR «amino acid» OR «fluoroethyltyrosine» OR «fluoroethylltyrosine», «Glioma» OR «brain tumor», «pediatric», and «neuro-oncology» were used. The screening of abstracts and full-text articles was performed by one reviewer (J.A.R.).
Inclusion criteria were studies in English, using FET, and in humans with a full text available.
Exclusion criteria included studies that included less than 20 patients, did not report on diagnostic test parameters or metrics representing impact on clinical management decisions and/or survival outcomes, did not give information about histology or tumor grades, and studies that included other malignancies. We also excluded studies that did not include histological confirmation or follow-up.
2.2. Data Synthesizing
For each study, the indication, principal author, publication year, study design, number of patients, grade, age, sex, type of imaging modality, test parameter, cut-off used, and their performances were recorded.
3. Results
3.1. Literature Search
We selected 152 studies according to their title and abstract, but upon full-text review, 70 studies were excluded (Figure 2).
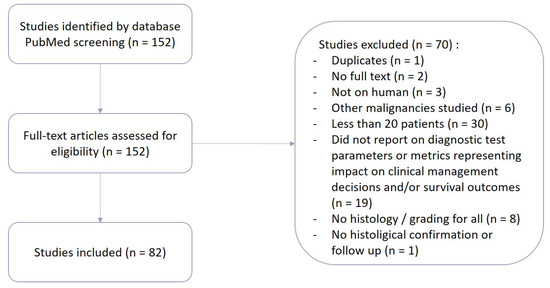
Figure 2.
Flowchart of the literature selection.
The remaining 82 studies [19,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104] were included in this review, with a total of 4657 patients. Details of these study characteristics can be found in Table 2.
Table 2.
Characteristics of the 82 included studies. §: did not reach significance, &: did not reach significance after Bonferroni multiple-test correction, #: significance not available.
Regarding PET parameters, we noticed a high variability in the determination of tumor region of interest (ROI) with an impact on the subsequent calculation of tumor-to-brain ratios (TBRs). We consequently sorted different TBRs according to the methodology used to obtain them (Table 3) in order to be able to compare their performances and then grouped every PET parameter in Table 4. We signified the change of parameters in the legend of Table 4 by writing the name of the parameter used in the table and the name of the original parameter(s) corresponding to this approach.
Table 3.
Different tumor-to-brain ratios and the methodology used to obtain them.
Table 4.
Summary of PET parameters. *: reached significance, X: did not reach significance, &: did not stay significant after Bonferroni multiple-test correction, NA: not available. TBRmax: Lmax/B, SUVmax/BG, LNR, TNR, LBRmax, T/Wm, TBRmax(20–40min), Tmax/B, maximum FET uptake, Tumax/BG; TBR3SD: Lmean/B, mean FET uptake; TBR25mm2: TBR, FET ratio; TBR10mm: TBRmean; TBR16mm: TBRmean, TBRmax; TBR70%: SUV70/BG; TBR80%: SUV80/BG; TBR: UR, FET lesion/brain ratio, FET uptake, tumor/brain tissue ratio, TBRmean, TBRmax; TAC: kinetic pattern, curve pattern; TTP: Tpeak; BTV: volume, MTV, Vol, Tvol 1.6; radiomic features: textural parameters.
3.2. Diagnosis
Four prospective studies [24,25,26,27] evaluated the performance of [18F]FET PET in patients with cerebral lesions suspicious of glioma. Each study chose a different method of TBR determination to detect glioma tissue with a threshold of 1.6 in two of them [26,27], resulting in a sensitivity of 88 to 92% and a specificity of 81 to 88%.
3.3. Grading
Thirteen studies [19,28,29,30,31,32,33,34,35,36,37,38,39] evaluated the performance of [18F]FET PET in glioma grading. Most studies aimed at differentiating low-grade gliomas (LGGs) from high-grade gliomas (HGGs). Multiple TBR methods were used, with a predominance of maximum tumor-to-brain ratio (TBRmax) with sensitivity and specificity ranging from 67 to 92% and 61 to 85%, respectively. Dynamic parameters and notably tumor-activity curves (TAC) had better performance, with a sensitivity of 73 to 96% and a specificity of 63 to 100%.
Notably, one study by Lohmann et al. [31] chose to supplement dynamic imaging from 0 to 50 min post-injection (p.i.) with an additional acquisition from 70 to 90 min p.i. The goal was to compare conventional dynamic imaging to dual-time-point imaging: one acquisition from 20 to 40 min p.i. and a delayed second acquisition from 70 to 90 min p.i. Mean tumor-to-brain ratio (TBRmean) change and TAC achieved similar accuracy of 81% and 83%, respectively.
3.4. IDH Status Determination
Six retrospective studies [34,40,41,42,43,44] evaluated the performance of [18F]FET PET in IDH status determination. Static parameters’ significancy was variable depending on the studies, whereas dynamic ones (Slope, Time-to-peak (TTP), TAC) always showed significant differences between IDH mutated and IDH wild-type groups with an accuracy of around 73%.
3.5. Prediction of Oligodendroglial Components
Two studies [38,44] reported on the performance of [18F]FET PET to determine the presence of oligodendroglial tumor components. Every static parameter tested was significant. Tumor-to-brain ratios showed good sensitivity, but specificity did not exceed 65%.
There were no dynamic parameters studied.
3.6. Guided Resection or Biopsy
Four studies [45,46,47,48] tested the addition of [18F]FET PET to better detect tumor tissue for resection or biopsy. In a study by Ewelt et al. [47], results were separated according to glioma grades (LGG vs. HGG), showing better tissue detection in high-grade glioma with sensitivity and specificity of 88% and 46%. Sensitivity was higher than those of MRI and 5-ALA-fluorescence, with a specificity being the lowest. Combining different modalities did not improve results compared to those of 5-ALA-fluorescence alone (sensitivity of 71% and specificity of 92%).
3.7. Detection of Residual Tumor
Two studies [49,50] aimed at detecting residual tumor tissue after surgery.
Buchmann et al. [49] also aimed to assess whether performing [18F]FET PET after 72 h after neurosurgery had an influence, as it is the case with MRI. Indeed, postoperative MRI after 72 h can lead to falsification of results because of inflammatory reactions. This study found higher sensitivity of PET using a TBR > 1.6 compared to MRI and no influence of timing of [18F]FET PET imaging.
3.8. Guided Radiotherapy
Studies [51,52,53,54,55,56] used the TBR threshold of 1.6 to define the tumor volume to be irradiated. This PET-based volume was increased compared to the MRI-based volume commonly used.
One study (Harat et al. [54]) reported 74% of failures inside primary gross tumor volume (GTV) PET volumes, with no solitary progressions inside the MRI-defined margin +20 mm but outside the GTV PET detected.
3.9. Detection of Malignant Transformation in Low-Grade Gliomas
Three studies [57,58,59] evaluated the use of [18F]FET PET to detect differences between non-transformed LGGs and LGGs that had transformed to high-grade gliomas. Two studies found a good detection value of both static and dynamic parameters in this indication, whether by comparing to baseline or by using parameter thresholds.
The remaining study (Bashir et al. [59]) did not find significant differences when considering all patients. After excluding the oligodendroglial subgroup, however, a significant difference was observed between non-transformed and transformed LGGs when combining [18F]FET parameters. The best result was observed with a combined analysis of TBRmax > 1.6 and TAC with a plateau or decreasing pattern (sensitivity of 75% and specificity of 83%).
3.10. Recurrence vs. Treatment-Related Changes
Twenty studies [60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79] evaluated the performance of [18F]FET PET in the differentiation of recurrence from treatment-related changes.
The majority of studies included patients treated with multiple modalities (such as operation, chemotherapy, and radiotherapy) who had a suspected tumor recurrence or progression as revealed by follow-up MRI. High-grade gliomas represented 87% (992/1141) of tumors.
Most studies used static parameters TBRmax and TBRmean along with dynamic parameters TTP and Slope.
TBRmax was significant in 13 studies with thresholds between 1.64 and 3.69. TBRmean significantly differentiated recurrence from pseudoprogression in 11 studies. The thresholds used varied from 1.8 to 2.31. Accuracy of TBRmax and TBRmean was comparable.
Dynamic parameters, when combined with static ones, allowed to increase diagnostic accuracy in some studies such as Werner et al. [68] and Galldiks et al. [78]. In Werner et al., TBRs alone had a diagnostic accuracy of 83%, which increased to 90% and 93% when combined with TTP and Slope, respectively. This finding was not supported by other studies, such as Werner et al. [66] and Galldiks et al. [67].
3.11. Prognosis and Treatment Response Evaluation
Twenty-eight studies [39,43,61,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104] evaluated the performance of [18F]FET PET in prognosis and treatment response evaluation.
Prognostic parameters can be extracted before, during, and after treatment. For example, Pyka et al. [93] studied patients with untreated, first-diagnosed gliomas and were able to predict tumor recurrence, with dynamic parameters showing better results than static ones, especially in the low-grade subgroup.
Overall, static parameters tended to not reach significance, whereas dynamic ones such as TTP and TAC demonstrated better results. TTP was the best parameter in two studies (Pyka et al. [93] and Bauer et al. [95]) with AUCs of 0.848 and 0.90, respectively.
Many studies also decided to use biological tumor volume (BTV), often determined by an autocontouring process using a TBR threshold of 1.6. Every study used a different cut-off when considering absolute values, and half of them did not reach significance. Three studies [82,87,94] opted for a BTV change after the initiation of chemotherapy to separate responders (relative change 0%) from non-responders (relative change > 0%). Two of them examined patients at first diagnosis and the third one at recurrence. These studies found a decreasing BTV to predict a significantly longer progression-free survival and to be associated with prolonged overall survival.
3.12. Radiomics
Radiomic parameters were used by 1 study, for grading [39] (grade 3 vs. 4), 2 studies in IDH status determination [40,41], 2 studies in the differentiation of recurrence vs. pseudoprogression [69,76], and 2 studies for prognosis [39,89].
Different textural features showed good performance in each study, and the combination of standard PET parameters with textural features could improve results, for example in IDH genotype determination, as shown by Lohmann et al. [41]. Combination of the dynamic parameter Slope with the radiomic feature SZHGE slightly increased diagnostic accuracy to 81% vs. 80% with Slope alone.
4. Discussion/Conclusions
This review proposes an up-to-date summary of PET performance in glioma management using O-(2-[18F]fluoroethyl)-L-tyrosine. The homogenization of PET tumor-to-brain ratios according to the determination of the different regions of interest allowed to truly compare their sensibility, specificity, AUC, and accuracy.
[18F]FET can be useful in every step of glioma management, from diagnosis to suspicion of recurrence.
The ability to discriminate tumor tissue from healthy brain tissue is helpful in diagnosis, to guide a surgical procedure or radiotherapy, and to detect the presence of a residue after surgery. Most studies agree on a TBR threshold > 1.6 to delineate tumor extent.
Different thresholds of tumor-to-brain ratio are also useful to predict histological characteristics (low vs. high grade, malignant transformation of a low-grade glioma, and oligodendroglial components), to differentiate post-treatment changes from a true recurrence, and to extract prognostic parameters and assess treatment response.
It is important to note that while many studies used static parameters TBRmax and TBRmean, the definition of these ratios differs depending on the article. For example, the ratio between the mean standard uptake value (SUVmean) of a 16 mm ROI centered on the maximal tumor uptake and the SUVmean of a contralateral background ROI, named TBR16mm in this review, can be called TBRmean in a study (Verger et al. [64]) and TBRmax in another (Galldiks et al. [78]).
Kertels et al. [63] expressed the need to use comparable approaches to be able to obtain relevant and reliable results. Despite the absence of a significant difference between methods chosen, approaches focusing on voxels with the highest uptake tended to perform superior.
Dynamic acquisition also adds valuable information with parameters such as TTP, TAC, or Slope and should be preferred. An interesting alternative proposed by Lohmann et al. [31] is dual-time point imaging, allowing to reduce costs due to higher patient throughput and imaging time.
Relatively new tools are also available, such as radiomics and hybrid PET/MR imaging, and could be of great interest in the future. The use of hybrid PET/MR is set to increase in neuro-oncology and could improve performance, as suggested by Lohmann et al. [41] concerning radiomics.
Joint EANM/EANO/RANO practice guidelines [9] published in 2018 summarized methods and cut-off values in different clinical situations concerning radiolabeled amino acids and [18F]FDG. It is of importance to note that the studies used to extract these guidelines are often retrospective and/or based on small effectives.
At the beginning of the year, Albert et al. [105] published the first version of PET RANO criteria in an effort to facilitate the structured implementation of PET imaging into clinical research and, ultimately, clinical routine.
The principal limitation of this review is the methodology used and the fact that many of the included studies are also retrospective and do not reflect clinical practice. Additionally, none of the studies included focused on pediatric gliomas, probably because of the limited number of patients in the available research.
While [18F]FET is becoming an important tracer in neuro-oncology, [18F]F-DOPA also showed good results and should not be overlooked. A recent meta-analysis and systematic review compared [18F]F-DOPA and [18F]FET for differentiating treatment-related change from true progression (Yu et al. [21]) and found that [18F]F-DOPA seems to demonstrate superior sensitivity and similar specificity to [18F]FET. Nevertheless, [18F]F-DOPA PET results were obtained from studies with limited sample sizes.
There is a need to pursue research with prospective, multicentric studies to be able to standardize imaging analysis and define the use of technological advancements such as hybrid PET/MRI imaging and radiomics and to compare [18F]FET with existing radiopharmaceuticals such as [18F]F-DOPA head-to-head comparisons.
Author Contributions
Conceptualization, J.V.; methodology, J.A.R. and J.V.; validation, A.L. and J.V.; investigation, J.A.R.; resources, J.A.R.; data curation, J.A.R.; writing—original draft preparation, J.A.R. and J.V.; writing—review and editing, J.A.R., A.L., E.E., M.D., D.A. and J.V.; supervision, J.V.; project administration, J.A.R., A.L. and J.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Darlix, A.; Zouaoui, S.; Rigau, V.; Bessaoud, F.; Figarella-Branger, D.; Mathieu-Daudé, H.; Trétarre, B.; Bauchet, F.; Duffau, H.; Taillandier, L.; et al. Epidemiology for primary brain tumors: A nationwide population-based study. J. Neuro Oncol. 2017, 131, 525–546. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Brada, M.; Van Den Bent, M.J.; Tonn, J.-C.; Pentheroudakis, G. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii93–iii101. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; He, Q.; Zhang, B.; Li, N.; Zeng, X.; Li, W. Diagnostic accuracy of diffusion-weighted imaging in differentiating glioma recurrence from posttreatment-related changes: A meta-analysis. Expert. Rev. Anticancer Ther. 2022, 22, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, Y.; Wang, Y.; Xiao, H.; Chen, X.; Lei, Y.; Feng, Z.; Ma, X.; Ma, L. Perfusion magnetic resonance imaging in the differentiation between glioma recurrence and pseudoprogression: A systematic review, meta-analysis and meta-regression. Quant. Imaging Med. Surg. 2022, 12, 4805–4822. [Google Scholar] [CrossRef]
- El-Abtah, M.E.; Talati, P.; Fu, M.; Chun, B.; Clark, P.; Peters, A.; Ranasinghe, A.; He, J.; Rapalino, O.; Batchelor, T.T.; et al. Magnetic resonance spectroscopy outperforms perfusion in distinguishing between pseudoprogression and disease progression in patients with glioblastoma. Neuro Oncol. Adv. 2022, 4, vdac128. [Google Scholar] [CrossRef]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; la Fougère, C.; Langen, K.-J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef]
- Galldiks, N.; Lohmann, P.; Fink, G.R.; Langen, K.-J. Amino Acid PET in Neurooncology. J. Nucl. Med. 2023, 64, 693–700. [Google Scholar] [CrossRef]
- He, Q.; Zhang, L.; Zhang, B.; Shi, X.; Yi, C.; Zhang, X. Diagnostic accuracy of 13N-ammonia PET, 11C-methionine PET and 18F-fluorodeoxyglucose PET: A comparative study in patients with suspected cerebral glioma. BMC Cancer 2019, 19, 332. [Google Scholar] [CrossRef]
- Deuschl, C.; Kirchner, J.; Poeppel, T.D.; Schaarschmidt, B.; Kebir, S.; El Hindy, N.; Hense, J.; Quick, H.H.; Glas, M.; Herrmann, K.; et al. 11C–MET PET/MRI for detection of recurrent glioma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Kracht, L.W.; Burghaus, L.; Thomas, A.; Jacobs, A.H.; Heiss, W.; Herholz, K. Use of 11C-methionine PET to monitor the effects of temozolomide chemotherapy in malignant gliomas. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, R.; Kimura, K.; Abe, K.; Sakai, S. 11C-methionine PET/CT findings in benign brain disease. Jpn. J. Radiol. 2017, 35, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Karunanithi, S.; Sharma, P.; Kumar, A.; Khangembam, B.C.; Bandopadhyaya, G.P.; Kumar, R.; Goenka, A.; Gupta, D.K.; Malhotra, A.; Bal, C. Comparative diagnostic accuracy of contrast-enhanced MRI and 18F-FDOPA PET-CT in recurrent glioma. Eur. Radiol. 2013, 23, 2628–2635. [Google Scholar] [CrossRef] [PubMed]
- Youland, R.S.; Pafundi, D.H.; Brinkmann, D.H.; Lowe, V.J.; Morris, J.M.; Kemp, B.J.; Hunt, C.H.; Giannini, C.; Parney, I.F.; Laack, N.N. Prospective trial evaluating the sensitivity and specificity of 3,4-dihydroxy-6-[18F]-fluoro-L-phenylalanine (18F-DOPA) PET and MRI in patients with recurrent gliomas. J. Neuro Oncol. 2018, 137, 583–591. [Google Scholar] [CrossRef]
- Sala, Q.; Metellus, P.; Taieb, D.; Kaphan, E.; Figarella-Branger, D.; Guedj, E. 18F-DOPA, a Clinically Available PET Tracer to Study Brain Inflammation? Clin. Nucl. Med. 2014, 39, e283–e285. [Google Scholar] [CrossRef]
- Hutterer, M.; Nowosielski, M.; Putzer, D.; Jansen, N.L.; Seiz, M.; Schocke, M.; McCoy, M.; Göbel, G.; la Fougère, C.; Virgolini, I.J.; et al. [18F]-fluoro-ethyl-l-tyrosine PET: A valuable diagnostic tool in neuro-oncology, but not all that glitters is glioma. Neuro Oncol. 2013, 15, 341–351. [Google Scholar] [CrossRef]
- Pöpperl, G.; Kreth, F.W.; Mehrkens, J.H.; Herms, J.; Seelos, K.; Koch, W.; Gildehaus, F.J.; Kretzschmar, H.A.; Tonn, J.C.; Tatsch, K. FET PET for the evaluation of untreated gliomas: Correlation of FET uptake and uptake kinetics with tumour grading. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1933–1942. [Google Scholar] [CrossRef]
- Langen, K.-J.; Stoffels, G.; Filss, C.; Heinzel, A.; Stegmayr, C.; Lohmann, P.; Willuweit, A.; Neumaier, B.; Mottaghy, F.M.; Galldiks, N. Imaging of amino acid transport in brain tumours: Positron emission tomography with O-(2-[18F]fluoroethyl)- L -tyrosine (FET). Methods 2017, 130, 124–134. [Google Scholar] [CrossRef]
- Yu, P.; Wang, Y.; Su, F.; Chen, Y. Comparing [18F]FET PET and [18F]FDOPA PET for glioma recurrence diagnosis: A systematic review and meta-analysis. Front. Oncol. 2024, 13, 1346951. [Google Scholar] [CrossRef]
- Cui, M.; Zorrilla-Veloz, R.I.; Hu, J.; Guan, B.; Ma, X. Diagnostic Accuracy of PET for Differentiating True Glioma Progression From Post Treatment-Related Changes: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 671867. [Google Scholar] [CrossRef]
- Ouyang, Z.-Q.; Zheng, G.-R.; Duan, X.-R.; Zhang, X.-R.; Ke, T.-F.; Bao, S.-S.; Yang, J.; He, B.; Liao, C.-D. Diagnostic accuracy of glioma pseudoprogression identification with positron emission tomography imaging: A systematic review and meta-analysis. Quant. Imaging Med. Surg. 2023, 13, 4943–4959. [Google Scholar] [CrossRef] [PubMed]
- Pauleit, D.; Stoffels, G.; Bachofner, A.; Floeth, F.W.; Sabel, M.; Herzog, H.; Tellmann, L.; Jansen, P.; Reifenberger, G.; Hamacher, K.; et al. Comparison of 18F-FET and 18F-FDG PET in brain tumors. Nucl. Med. Biol. 2009, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Mauler, J.; Lohmann, P.; Maudsley, A.A.; Sheriff, S.; Hoevels, M.; Meissner, A.-K.; Hamisch, C.; Brunn, A.; Deckert, M.; Filss, C.P.; et al. Diagnostic Accuracy of MR Spectroscopic Imaging and 18F-FET PET for Identifying Glioma: A Biopsy-Controlled Hybrid PET/MRI Study. J. Nucl. Med. 2024, 65, 16–21. [Google Scholar] [CrossRef]
- Floeth, F.W.; Pauleit, D.; Wittsack, H.-J.; Langen, K.J.; Reifenberger, G.; Hamacher, K.; Messing-Jünger, M.; Zilles, K.; Weber, F.; Stummer, W.; et al. Multimodal metabolic imaging of cerebral gliomas: Positron emission tomography with [18F]fluoroethyl-l-tyrosine and magnetic resonance spectroscopy. J. Neurosurg. 2005, 102, 318–327. [Google Scholar] [CrossRef]
- Pauleit, D. O-(2-[18F]fluoroethyl)-L-tyrosine PET combined with MRI improves the diagnostic assessment of cerebral gliomas. Brain 2005, 128, 678–687. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Lim, S.M. Comparison of 3′-deoxy-3′-[18F]fluorothymidine PET and O-(2-[18F]fluoroethyl)-L-tyrosine PET in patients with newly diagnosed glioma. Nucl. Med. Biol. 2012, 39, 977–981. [Google Scholar] [CrossRef]
- Verger, A.; Filss, C.P.; Lohmann, P.; Stoffels, G.; Sabel, M.; Wittsack, H.J.; Kops, E.R.; Galldiks, N.; Fink, G.R.; Shah, N.J.; et al. Comparison of 18F-FET PET and perfusion-weighted MRI for glioma grading: A hybrid PET/MR study. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 2257–2265. [Google Scholar] [CrossRef]
- Lopez, W.O.C.; Cordeiro, J.G.; Albicker, U.; Doostkam, S.; Nikkhah, G.; Kirch, R.D.; Trippel, M.; Reithmeier, T. Correlation of 18F-fluoroethyl tyrosine positron-emission tomography uptake values and histomorphological findings by stereotactic serial biopsy in newly diagnosed brain tumors using a refined software tool. Onco Targets Ther. 2015, 8, 3803–3815. [Google Scholar] [CrossRef]
- Lohmann, P.; Herzog, H.; Rota Kops, E.; Stoffels, G.; Judov, N.; Filss, C.; Galldiks, N.; Tellmann, L.; Weiss, C.; Sabel, M.; et al. Dual-time-point O-(2-[18F]fluoroethyl)-L-tyrosine PET for grading of cerebral gliomas. Eur. Radiol. 2015, 25, 3017–3024. [Google Scholar] [CrossRef] [PubMed]
- Calcagni, M.L.; Galli, G.; Giordano, A.; Taralli, S.; Anile, C.; Niesen, A.; Baum, R.P. Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for Glioma Grading: Assessment of Individual Probability of Malignancy. Clin. Nucl. Med. 2011, 36, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Albert, N.L.; Winkelmann, I.; Suchorska, B.; Wenter, V.; Schmid-Tannwald, C.; Mille, E.; Todica, A.; Brendel, M.; Tonn, J.-C.; Bartenstein, P.; et al. Early static 18F-FET-PET scans have a higher accuracy for glioma grading than the standard 20–40 min scans. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Hua, T.; Zhou, W.; Zhou, Z.; Guan, Y.; Li, M. Heterogeneous parameters based on 18F-FET PET imaging can non-invasively predict tumor grade and isocitrate dehydrogenase gene 1 mutation in untreated gliomas. Quant. Imaging Med. Surg. 2021, 11, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Thon, N.; Eigenbrod, S.; Hartmann, C.; Egensperger, R.; Herms, J.; Geisler, J.; la Fougere, C.; Lutz, J.; Linn, J.; et al. Hot spots in dynamic18FET-PET delineate malignant tumor parts within suspected WHO grade II gliomas. Neuro Oncol. 2011, 13, 307–316. [Google Scholar] [CrossRef]
- Röhrich, M.; Huang, K.; Schrimpf, D.; Albert, N.L.; Hielscher, T.; Von Deimling, A.; Schüller, U.; Dimitrakopoulou-Strauss, A.; Haberkorn, U. Integrated analysis of dynamic FET PET/CT parameters, histology, and methylation profiling of 44 gliomas. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1573–1584. [Google Scholar] [CrossRef]
- Jansen, N.L.; Graute, V.; Armbruster, L.; Suchorska, B.; Lutz, J.; Eigenbrod, S.; Cumming, P.; Bartenstein, P.; Tonn, J.-C.; Kreth, F.W.; et al. MRI-suspected low-grade glioma: Is there a need to perform dynamic FET PET? Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1021–1029. [Google Scholar] [CrossRef]
- Jansen, N.L.; Schwartz, C.; Graute, V.; Eigenbrod, S.; Lutz, J.; Egensperger, R.; Pöpperl, G.; Kretzschmar, H.A.; Cumming, P.; Bartenstein, P.; et al. Prediction of oligodendroglial histology and LOH 1p/19q using dynamic [18F]FET-PET imaging in intracranial WHO grade II and III gliomas. Neuro Oncol. 2012, 14, 1473–1480. [Google Scholar] [CrossRef]
- Pyka, T.; Gempt, J.; Hiob, D.; Ringel, F.; Schlegel, J.; Bette, S.; Wester, H.-J.; Meyer, B.; Förster, S. Textural analysis of pre-therapeutic [18F]-FET-PET and its correlation with tumor grade and patient survival in high-grade gliomas. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 133–141. [Google Scholar] [CrossRef]
- Zhou, W.; Huang, Q.; Wen, J.; Li, M.; Zhu, Y.; Liu, Y.; Dai, Y.; Guan, Y.; Zhou, Z.; Hua, T. Integrated CT Radiomics Features Could Enhance the Efficacy of 18F-FET PET for Non-Invasive Isocitrate Dehydrogenase Genotype Prediction in Adult Untreated Gliomas: A Retrospective Cohort Study. Front Oncol. 2021, 11, 772703. [Google Scholar] [CrossRef]
- Lohmann, P.; Lerche, C.; Bauer, E.K.; Steger, J.; Stoffels, G.; Blau, T.; Dunkl, V.; Kocher, M.; Viswanathan, S.; Filss, C.P.; et al. Predicting IDH genotype in gliomas using FET PET radiomics. Sci. Rep. 2018, 8, 13328. [Google Scholar] [CrossRef]
- Verger, A.; Stoffels, G.; Bauer, E.K.; Lohmann, P.; Blau, T.; Fink, G.R.; Neumaier, B.; Shah, N.J.; Langen, K.-J.; Galldiks, N. Static and dynamic 18F–FET PET for the characterization of gliomas defined by IDH and 1p/19q status. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Durand, P.; Van Der Gucht, A.; Verger, A.; Langen, K.-J.; Dunet, V.; Bloch, J.; Brouland, J.-P.; Nicod-Lalonde, M.; Schaefer, N.; Prior, J.O. Voxel-based 18F-FET PET segmentation and automatic clustering of tumor voxels: A significant association with IDH1 mutation status and survival in patients with gliomas. PLoS ONE 2018, 13, e0199379. [Google Scholar] [CrossRef]
- Bette, S.; Gempt, J.; Delbridge, C.; Kirschke, J.S.; Schlegel, J.; Foerster, S.; Huber, T.; Pyka, T.; Zimmer, C.; Meyer, B.; et al. Prognostic Value of O-(2-[18F]-Fluoroethyl)-L-Tyrosine-Positron Emission Tomography Imaging for Histopathologic Characteristics and Progression-Free Survival in Patients with Low-Grade Glioma. World Neurosurg. 2016, 89, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Ort, J.; Hamou, H.A.; Kernbach, J.M.; Hakvoort, K.; Blume, C.; Lohmann, P.; Galldiks, N.; Heiland, D.H.; Mottaghy, F.M.; Clusmann, H.; et al. 18F-FET-PET-guided gross total resection improves overall survival in patients with WHO grade III/IV glioma: Moving towards a multimodal imaging-guided resection. J. Neurooncol. 2021, 155, 71–80. [Google Scholar] [CrossRef]
- Floeth, F.W.; Sabel, M.; Ewelt, C.; Stummer, W.; Felsberg, J.; Reifenberger, G.; Steiger, H.J.; Stoffels, G.; Coenen, H.H.; Langen, K.-J. Comparison of 18F-FET PET and 5-ALA fluorescence in cerebral gliomas. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 731–741. [Google Scholar] [CrossRef]
- Ewelt, C.; Floeth, F.W.; Felsberg, J.; Steiger, H.J.; Sabel, M.; Langen, K.-J.; Stoffels, G.; Stummer, W. Finding the anaplastic focus in diffuse gliomas: The value of Gd-DTPA enhanced MRI, FET-PET, and intraoperative, ALA-derived tissue fluorescence. Clin. Neurol. Neurosurg. 2011, 113, 541–547. [Google Scholar] [CrossRef]
- Verburg, N.; Koopman, T.; Yaqub, M.M.; Hoekstra, O.S.; Lammertsma, A.A.; Barkhof, F.; Pouwels, P.J.W.; Reijneveld, J.C.; Heimans, J.J.; Rozemuller, A.J.M.; et al. Improved detection of diffuse glioma infiltration with imaging combinations: A diagnostic accuracy study. Neuro Oncol. 2020, 22, 412–422. [Google Scholar] [CrossRef]
- Buchmann, N.; Kläsner, B.; Gempt, J.; Bauer, J.S.; Pyka, T.; Delbridge, C.; Meyer, B.; Krause, B.J.; Ringel, F. 18F-Fluoroethyl-l-Thyrosine Positron Emission Tomography to Delineate Tumor Residuals After Glioblastoma Resection: A Comparison with Standard Postoperative Magnetic Resonance Imaging. World Neurosurg. 2016, 89, 420–426. [Google Scholar] [CrossRef]
- Kläsner, B.; Buchmann, N.; Gempt, J.; Ringel, F.; Lapa, C.; Krause, B.J. Early [18F]FET-PET in Gliomas after Surgical Resection: Comparison with MRI and Histopathology. PLoS ONE 2015, 10, e0141153. [Google Scholar] [CrossRef]
- Allard, B.; Dissaux, B.; Bourhis, D.; Dissaux, G.; Schick, U.; Salaün, P.-Y.; Abgral, R.; Querellou, S. Hotspot on 18F-FET PET/CT to Predict Aggressive Tumor Areas for Radiotherapy Dose Escalation Guiding in High-Grade Glioma. Cancers 2022, 15, 98. [Google Scholar] [CrossRef] [PubMed]
- Munck af Rosenschold, P.; Costa, J.; Engelholm, S.A.; Lundemann, M.J.; Law, I.; Ohlhues, L.; Engelholm, S. Impact of [18F]-fluoro-ethyl-tyrosine PET imaging on target definition for radiation therapy of high-grade glioma. Neuro Oncol. 2015, 17, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, D.F.; Unterrainer, M.; Schön, R.; Corradini, S.; Maihöfer, C.; Bartenstein, P.; Belka, C.; Albert, N.L.; Niyazi, M. Margin reduction in radiotherapy for glioblastoma through 18F-fluoroethyltyrosine PET?—A recurrence pattern analysis. Radiother. Oncol. 2020, 145, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Harat, M.; Małkowski, B.; Makarewicz, R. Pre-irradiation tumour volumes defined by MRI and dual time-point FET-PET for the prediction of glioblastoma multiforme recurrence: A prospective study. Radiother. Oncol. 2016, 120, 241–247. [Google Scholar] [CrossRef]
- Dissaux, G.; Dissaux, B.; Kabbaj, O.E.; Gujral, D.M.; Pradier, O.; Salaün, P.-Y.; Seizeur, R.; Bourhis, D.; Ben Salem, D.; Querellou, S.; et al. Radiotherapy target volume definition in newly diagnosed high grade glioma using 18F-FET PET imaging and multiparametric perfusion MRI: A prospective study (IMAGG). Radiother. Oncol. 2020, 150, 164–171. [Google Scholar] [CrossRef]
- Hayes, A.R.; Jayamanne, D.; Hsiao, E.; Schembri, G.P.; Bailey, D.L.; Roach, P.J.; Khasraw, M.; Newey, A.; Wheeler, H.R.; Back, M. Utilizing 18F-fluoroethyltyrosine (FET) positron emission tomography (PET) to define suspected nonenhancing tumor for radiation therapy planning of glioblastoma. Pract. Radiat. Oncol. 2018, 8, 230–238. [Google Scholar] [CrossRef]
- Galldiks, N.; Stoffels, G.; Ruge, M.I.; Rapp, M.; Sabel, M.; Reifenberger, G.; Erdem, Z.; Shah, N.J.; Fink, G.R.; Coenen, H.H.; et al. Role of O-(2-18F-Fluoroethyl)-l-Tyrosine PET as a Diagnostic Tool for Detection of Malignant Progression in Patients with Low-Grade Glioma. J. Nucl. Med. 2013, 54, 2046–2054. [Google Scholar] [CrossRef]
- Unterrainer, M.; Schweisthal, F.; Suchorska, B.; Wenter, V.; Schmid-Tannwald, C.; Fendler, W.P.; Schüller, U.; Bartenstein, P.; Tonn, J.-C.; Albert, N.L. Serial 18 F-FET PET Imaging of Primarily 18 F-FET–Negative Glioma: Does It Make Sense? J. Nucl. Med. 2016, 57, 1177–1182. [Google Scholar] [CrossRef]
- Bashir, A.; Brennum, J.; Broholm, H.; Law, I. The diagnostic accuracy of detecting malignant transformation of low-grade glioma using O-(2-[18F]fluoroethyl)-l-tyrosine positron emission tomography: A retrospective study. J. Neurosurg. 2018, 130, 451–464. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Lee, T.H.; Rhee, C.H.; Cho, A.R.; Il Kim, B.; Cheon, G.J.; Choi, C.W.; Lim, S.M. 3′-Deoxy-3′-[18F]fluorothymidine and O-(2-[18F]fluoroethyl)-L-tyrosine PET in Patients with Suspicious Recurrence of Glioma after Multimodal Treatment: Initial Results of a Retrospective Comparative Study. Nucl. Med. Mol. Imaging 2010, 44, 45–54. [Google Scholar] [CrossRef][Green Version]
- Jansen, N.L.; Suchorska, B.; Schwarz, S.B.; Eigenbrod, S.; Lutz, J.; Graute, V.; Bartenstein, P.; Belka, C.; Kreth, F.W.; Fougère, C.L. [18F]Fluoroethyltyrosine–Positron Emission Tomography-Based Therapy Monitoring after Stereotactic Iodine-125 Brachytherapy in Patients with Recurrent High-Grade Glioma. Mol. Imaging 2013, 12, 7290.2012.00027. [Google Scholar] [CrossRef]
- Puranik, A.D.; Rangarajan, V.; Dev, I.D.; Jain, Y.; Purandare, N.C.; Sahu, A.; Choudhary, A.; Gupta, T.; Chatterjee, A.; Moiyadi, A.; et al. Brain FET PET tumor-to-white mater ratio to differentiate recurrence from post-treatment changes in high-grade gliomas. J. Neuroimaging 2021, 31, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Kertels, O.; Mihovilovic, M.I.; Linsenmann, T.; Kessler, A.F.; Tran-Gia, J.; Kircher, M.; Brumberg, J.; Monoranu, C.M.; Samnick, S.; Ernestus, R.-I.; et al. Clinical Utility of Different Approaches for Detection of Late Pseudoprogression in Glioblastoma with O-(2-[18F]Fluoroethyl)-l-Tyrosine PET. Clin. Nucl. Med. 2019, 44, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Verger, A.; Filss, C.P.; Lohmann, P.; Stoffels, G.; Sabel, M.; Wittsack, H.-J.; Kops, E.R.; Galldiks, N.; Fink, G.R.; Shah, N.J.; et al. Comparison of O-(2-18 F-Fluoroethyl)-L-Tyrosine Positron Emission Tomography and Perfusion-Weighted Magnetic Resonance Imaging in the Diagnosis of Patients with Progressive and Recurrent Glioma: A Hybrid Positron Emission Tomography/Magnetic Resonance Study. World Neurosurg. 2018, 113, e727–e737. [Google Scholar] [CrossRef]
- Pyka, T.; Hiob, D.; Preibisch, C.; Gempt, J.; Wiestler, B.; Schlegel, J.; Straube, C.; Zimmer, C. Diagnosis of glioma recurrence using multiparametric dynamic 18F-fluoroethyl-tyrosine PET-MRI. Eur. J. Radiol. 2018, 103, 32–37. [Google Scholar] [CrossRef]
- Werner, J.-M.; Weller, J.; Ceccon, G.; Schaub, C.; Tscherpel, C.; Lohmann, P.; Bauer, E.K.; Schäfer, N.; Stoffels, G.; Baues, C.; et al. Diagnosis of Pseudoprogression Following Lomustine-Temozolomide Chemoradiation in Newly Diagnosed Glioblastoma Patients Using FET-PET. Clin. Cancer Res. 2021, 27, 3704–3713. [Google Scholar] [CrossRef]
- Galldiks, N.; Dunkl, V.; Stoffels, G.; Hutterer, M.; Rapp, M.; Sabel, M.; Reifenberger, G.; Kebir, S.; Dorn, F.; Blau, T.; et al. Diagnosis of pseudoprogression in patients with glioblastoma using O-(2-[18F]fluoroethyl)-l-tyrosine PET. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 685–695. [Google Scholar] [CrossRef]
- Werner, J.-M.; Stoffels, G.; Lichtenstein, T.; Borggrefe, J.; Lohmann, P.; Ceccon, G.; Shah, N.J.; Fink, G.R.; Langen, K.-J.; Kabbasch, C.; et al. Differentiation of treatment-related changes from tumour progression: A direct comparison between dynamic FET PET and ADC values obtained from DWI MRI. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1889–1901. [Google Scholar] [CrossRef]
- Lohmann, P.; Elahmadawy, M.A.; Gutsche, R.; Werner, J.-M.; Bauer, E.K.; Ceccon, G.; Kocher, M.; Lerche, C.W.; Rapp, M.; Fink, G.R.; et al. FET PET Radiomics for Differentiating Pseudoprogression from Early Tumor Progression in Glioma Patients Post-Chemoradiation. Cancers 2020, 12, 3835. [Google Scholar] [CrossRef]
- Kebir, S.; Fimmers, R.; Galldiks, N.; Schäfer, N.; Mack, F.; Schaub, C.; Stuplich, M.; Niessen, M.; Tzaridis, T.; Simon, M.; et al. Late Pseudoprogression in Glioblastoma: Diagnostic Value of Dynamic O-(2-[18F]fluoroethyl)-L-Tyrosine PET. Clin. Cancer Res. 2016, 22, 2190–2196. [Google Scholar] [CrossRef]
- Rachinger, W.; Goetz, C.; Pöpperl, G.; Gildehaus, F.J.; Kreth, F.W.; Holtmannspötter, M.; Herms, J.; Koch, W.; Tatsch, K.; Tonn, J.-C. Positron Emission Tomography with O-(2-[18F]fluoroethyl)-l-tyrosine versus Magnetic Resonance Imaging in the Diagnosis of Recurrent Gliomas. Neurosurgery 2005, 57, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Lohmeier, J.; Bohner, G.; Siebert, E.; Brenner, W.; Hamm, B.; Makowski, M.R. Quantitative biparametric analysis of hybrid 18F-FET PET/MR-neuroimaging for differentiation between treatment response and recurrent glioma. Sci. Rep. 2019, 9, 14603. [Google Scholar] [CrossRef]
- Bashir, A.; Mathilde Jacobsen, S.; Mølby Henriksen, O.; Broholm, H.; Urup, T.; Grunnet, K.; Andrée Larsen, V.; Møller, S.; Skjøth-Rasmussen, J.; Skovgaard Poulsen, H.; et al. Recurrent glioblastoma versus late posttreatment changes: Diagnostic accuracy of O-(2-[18F]fluoroethyl)-L-tyrosine positron emission tomography (18F-FET PET). Neuro Oncol. 2019, 21, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- Steidl, E.; Langen, K.-J.; Hmeidan, S.A.; Polomac, N.; Filss, C.P.; Galldiks, N.; Lohmann, P.; Keil, F.; Filipski, K.; Mottaghy, F.M.; et al. Sequential implementation of DSC-MR perfusion and dynamic [18F]FET PET allows efficient differentiation of glioma progression from treatment-related changes. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1956–1965. [Google Scholar] [CrossRef] [PubMed]
- Pöpperl, G.; Götz, C.; Rachinger, W.; Schnell, O.; Gildehaus, F.J.; Tonn, J.C.; Tatsch, K. Serial O-(2-[18F]fluoroethyl)-L-tyrosine PET for monitoring the effects of intracavitary radioimmunotherapy in patients with malignant glioma. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 792–800. [Google Scholar] [CrossRef]
- Müller, M.; Winz, O.; Gutsche, R.; Leijenaar, R.T.H.; Kocher, M.; Lerche, C.; Filss, C.P.; Stoffels, G.; Steidl, E.; Hattingen, E.; et al. Static FET PET radiomics for the differentiation of treatment-related changes from glioma progression. J. Neurooncol. 2022, 159, 519–529. [Google Scholar] [CrossRef]
- Mehrkens, J.H.; Pöpperl, G.; Rachinger, W.; Herms, J.; Seelos, K.; Tatsch, K.; Tonn, J.C.; Kreth, F.W. The positive predictive value of O-(2-[18F]fluoroethyl)-l-tyrosine (FET) PET in the diagnosis of a glioma recurrence after multimodal treatment. J. Neurooncol. 2008, 88, 27–35. [Google Scholar] [CrossRef]
- Galldiks, N.; Stoffels, G.; Filss, C.; Rapp, M.; Blau, T.; Tscherpel, C.; Ceccon, G.; Dunkl, V.; Weinzierl, M.; Stoffel, M.; et al. The use of dynamic O-(2-18F-fluoroethyl)-l-tyrosine PET in the diagnosis of patients with progressive and recurrent glioma. Neuro Oncol. 2015, 17, 1293–1300. [Google Scholar] [CrossRef]
- Pöpperl, G.; Götz, C.; Rachinger, W.; Gildehaus, F.-J.; Tonn, J.-C.; Tatsch, K. Value of O-(2-[18F]fluoroethyl)-l-tyrosine PET for the diagnosis of recurrent glioma. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1464–1470. [Google Scholar] [CrossRef]
- Müther, M.; Koch, R.; Weckesser, M.; Sporns, P.; Schwindt, W.; Stummer, W. 5-Aminolevulinic Acid Fluorescence-Guided Resection of 18F-FET-PET Positive Tumor Beyond Gadolinium Enhancing Tumor Improves Survival in Glioblastoma. Neurosurgery 2019, 85, E1020–E1029. [Google Scholar] [CrossRef]
- Suchorska, B.; Unterrainer, M.; Biczok, A.; Sosnova, M.; Forbrig, R.; Bartenstein, P.; Tonn, J.-C.; Albert, N.L.; Kreth, F.-W. 18F-FET-PET as a biomarker for therapy response in non-contrast enhancing glioma following chemotherapy. J. Neurooncol. 2018, 139, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Langen, K.-J.; Holy, R.; Pinkawa, M.; Stoffels, G.; Nolte, K.W.; Kaiser, H.J.; Filss, C.P.; Fink, G.R.; Coenen, H.H.; et al. Assessment of Treatment Response in Patients with Glioblastoma Using O-(2-18F-Fluoroethyl)-l-Tyrosine PET in Comparison to MRI. J. Nucl. Med. 2012, 53, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Suchorska, B.; Jansen, N.L.; Linn, J.; Kretzschmar, H.; Janssen, H.; Eigenbrod, S.; Simon, M.; Pöpperl, G.; Kreth, F.W.; La Fougere, C.; et al. Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM. Neurology 2015, 84, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Jansen, N.L.; Suchorska, B.; Wenter, V.; Eigenbrod, S.; Schmid-Tannwald, C.; Zwergal, A.; Niyazi, M.; Drexler, M.; Bartenstein, P.; Schnell, O.; et al. Dynamic 18F-FET PET in Newly Diagnosed Astrocytic Low-Grade Glioma Identifies High-Risk Patients. J. Nucl. Med. 2014, 55, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Thon, N.; Kunz, M.; Lemke, L.; Jansen, N.L.; Eigenbrod, S.; Kreth, S.; Lutz, J.; Egensperger, R.; Giese, A.; Herms, J.; et al. Dynamic 18F-FET PET in suspected WHO grade II gliomas defines distinct biological subgroups with different clinical courses. Int. J. Cancer 2015, 136, 2132–2145. [Google Scholar] [CrossRef]
- Kunz, M.; Albert, N.L.; Unterrainer, M.; la Fougere, C.; Egensperger, R.; Schüller, U.; Lutz, J.; Kreth, S.; Tonn, J.-C.; Kreth, F.-W.; et al. Dynamic 18F-FET PET is a powerful imaging biomarker in gadolinium-negative gliomas. Neuro Oncol. 2019, 21, 274–284. [Google Scholar] [CrossRef]
- Ceccon, G.; Lohmann, P.; Werner, J.-M.; Tscherpel, C.; Dunkl, V.; Stoffels, G.; Rosen, J.; Rapp, M.; Sabel, M.; Herrlinger, U.; et al. Early Treatment Response Assessment Using 18F-FET PET Compared with Contrast-Enhanced MRI in Glioma Patients After Adjuvant Temozolomide Chemotherapy. J. Nucl. Med. 2021, 62, 918–925. [Google Scholar] [CrossRef]
- Galldiks, N.; Dunkl, V.; Ceccon, G.; Tscherpel, C.; Stoffels, G.; Law, I.; Henriksen, O.M.; Muhic, A.; Poulsen, H.S.; Steger, J.; et al. Early treatment response evaluation using FET PET compared to MRI in glioblastoma patients at first progression treated with bevacizumab plus lomustine. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2377–2386. [Google Scholar] [CrossRef]
- Carles, M.; Popp, I.; Starke, M.M.; Mix, M.; Urbach, H.; Schimek-Jasch, T.; Eckert, F.; Niyazi, M.; Baltas, D.; Grosu, A.L. FET-PET radiomics in recurrent glioblastoma: Prognostic value for outcome after re-irradiation? Radiat. Oncol. 2021, 16, 46. [Google Scholar] [CrossRef]
- Suchorska, B.; Giese, A.; Biczok, A.; Unterrainer, M.; Weller, M.; Drexler, M.; Bartenstein, P.; Schüller, U.; Tonn, J.-C.; Albert, N.L. Identification of time-to-peak on dynamic 18F-FET-PET as a prognostic marker specifically in IDH1/2 mutant diffuse astrocytoma. Neuro Oncol. 2018, 20, 279–288. [Google Scholar] [CrossRef]
- Wirsching, H.-G.; Roelcke, U.; Weller, J.; Hundsberger, T.; Hottinger, A.F.; von Moos, R.; Caparrotti, F.; Conen, K.; Remonda, L.; Roth, P.; et al. MRI and 18FET-PET predict survival benefit from bevacizumab plus radiotherapy in patients with IDH wild-type glioblastoma: Results from the randomized ARTE trial. Clin. Cancer Res. 2021, 27, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, R.; Polat, B.; Samnick, S.; Reiners, C.; Flentje, M.; Verburg, F.A. O-(2-[18F]fluoroethyl)-l-tyrosine uptake is an independent prognostic determinant in patients with glioma referred for radiation therapy. Ann. Nucl. Med. 2014, 28, 154–162. [Google Scholar] [CrossRef]
- Pyka, T.; Gempt, J.; Ringel, F.; Hüttinger, S.; van Marwick, S.; Nekolla, S.; Wester, H.-J.; Schwaiger, M.; Förster, S. Prediction of Glioma Recurrence Using Dynamic 18F-Fluoroethyltyrosine PET. AJNR Am. J. Neuroradiol. 2014, 35, 1924–1929. [Google Scholar] [CrossRef] [PubMed]
- Wollring, M.M.; Werner, J.-M.; Bauer, E.K.; Tscherpel, C.; Ceccon, G.S.; Lohmann, P.; Stoffels, G.; Kabbasch, C.; Goldbrunner, R.; Fink, G.R.; et al. Prediction of response to lomustine-based chemotherapy in glioma patients at recurrence using MRI and FET PET. Neuro Oncol. 2022, 25, 984–994. [Google Scholar] [CrossRef]
- Bauer, E.K.; Stoffels, G.; Blau, T.; Reifenberger, G.; Felsberg, J.; Werner, J.M.; Lohmann, P.; Rosen, J.; Ceccon, G.; Tscherpel, C.; et al. Prediction of survival in patients with IDH-wildtype astrocytic gliomas using dynamic O-(2-[18F]-fluoroethyl)-l-tyrosine PET. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1486–1495. [Google Scholar] [CrossRef] [PubMed]
- Piroth, M.D.; Holy, R.; Pinkawa, M.; Stoffels, G.; Kaiser, H.J.; Galldiks, N.; Herzog, H.; Coenen, H.H.; Eble, M.J.; Langen, K.J. Prognostic impact of postoperative, pre-irradiation 18F-fluoroethyl-l-tyrosine uptake in glioblastoma patients treated with radiochemotherapy. Radiother. Oncol. 2011, 99, 218–224. [Google Scholar] [CrossRef]
- Jansen, N.L.; Suchorska, B.; Wenter, V.; Schmid-Tannwald, C.; Todica, A.; Eigenbrod, S.; Niyazi, M.; Tonn, J.-C.; Bartenstein, P.; Kreth, F.-W.; et al. Prognostic Significance of Dynamic 18F-FET PET in Newly Diagnosed Astrocytic High-Grade Glioma. J. Nucl. Med. 2015, 56, 9–15. [Google Scholar] [CrossRef]
- Moller, S.; Law, I.; Munck Af Rosenschold, P.; Costa, J.; Poulsen, H.S.; Engelholm, S.A.; Engelholm, S. Prognostic value of 18F-FET PET imaging in re-irradiation of high-grade glioma: Results of a phase I clinical trial. Radiother. Oncol. 2016, 121, 132–137. [Google Scholar] [CrossRef]
- Dissaux, G.; Basse, V.; Schick, U.; EL Kabbaj, O.; Auberger, B.; Magro, E.; Kassoul, A.; Abgral, R.; Salaun, P.-Y.; Bourhis, D.; et al. Prognostic value of 18F-FET PET/CT in newly diagnosed WHO 2016 high-grade glioma. Medicine 2020, 99, e19017. [Google Scholar] [CrossRef]
- Piroth, M.D.; Pinkawa, M.; Holy, R.; Klotz, J.; Nussen, S.; Stoffels, G.; Coenen, H.H.; Kaiser, H.J.; Langen, K.J.; Eble, M.J. Prognostic Value of Early [18F]Fluoroethyltyrosine Positron Emission Tomography After Radiochemotherapy in Glioblastoma Multiforme. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 176–184. [Google Scholar] [CrossRef]
- Schneider, F.; Wolpert, F.; Stolzmann, P.; Albatly, A.A.; Kenkel, D.; Weller, J.; Weller, M.; Kollias, S.S.; Rushing, E.J.; Veit-Haibach, P.; et al. Prognostic value of O-(2-[18F]-fluoroethyl)-L-tyrosine PET in relapsing oligodendroglioma. Acta Oncol. 2020, 59, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Kertels, O.; Kessler, A.F.; Mihovilovic, M.I.; Stolzenburg, A.; Linsenmann, T.; Samnick, S.; Brändlein, S.; Monoranu, C.M.; Ernestus, R.-I.; Buck, A.K.; et al. Prognostic Value of O-(2-[18F]Fluoroethyl)-L-Tyrosine PET/CT in Newly Diagnosed WHO 2016 Grade II and III Glioma. Mol. Imaging Biol. 2019, 21, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Floeth, F.W.; Pauleit, D.; Sabel, M.; Stoffels, G.; Reifenberger, G.; Riemenschneider, M.J.; Jansen, P.; Coenen, H.H.; Steiger, H.-J.; Langen, K.-J. Prognostic Value of O-(2-18F-Fluoroethyl)-L-Tyrosine PET and MRI in Low-Grade Glioma. J. Nucl. Med. 2007, 48, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Niyazi, M.; Jansen, N.; Ganswindt, U.; Schwarz, S.B.; Geisler, J.; Schnell, O.; Büsing, K.; Eigenbrod, S.; La Fougère, C.; Belka, C. Re-irradiation in recurrent malignant glioma: Prognostic value of [18F]FET–PET. J. Neurooncol. 2012, 110, 389–395. [Google Scholar] [CrossRef]
- Albert, N.L.; Galldiks, N.; Ellingson, B.M.; van den Bent, M.J.; Chang, S.M.; Cicone, F.; de Groot, J.; Koh, E.-S.; Law, I.; Rhun, E.L.; et al. PET-based response assessment criteria for diffuse gliomas (PET RANO 1.0): A report of the RANO group. Lancet Oncol. 2024, 25, e29–e41. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).