Theophylline

Abstract
:1. Introduction
2. Chemistry
3. Molecular Mechanisms of Action

{kind=link}
{kind=link}
{kind=link}
|
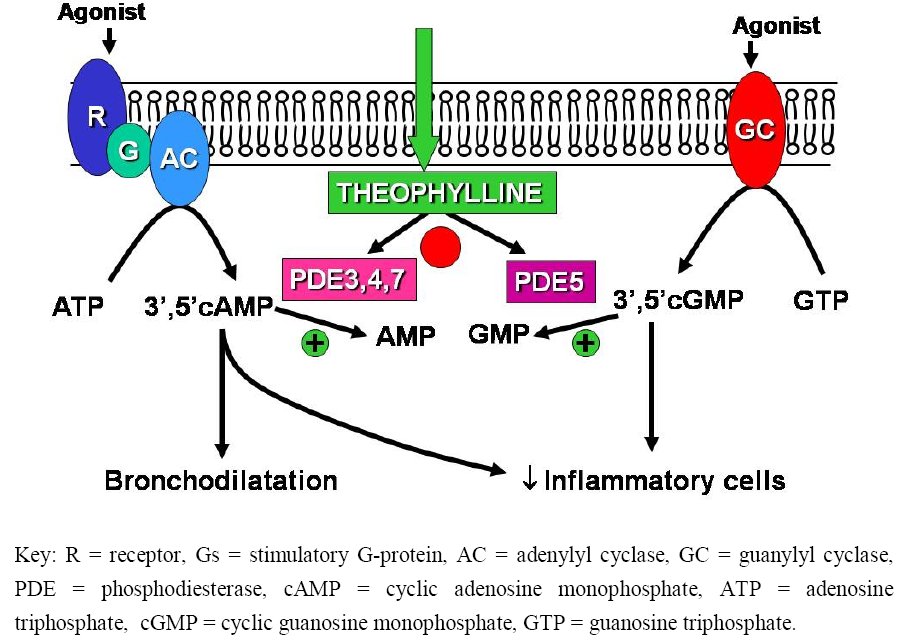
3.1. Phosphodiesterase Inhibition

3.2. Adenosine Receptor Antagonism
3.3. Interleukin-10 Release
3.4. Effects on Gene Transcription
3.5. Effect on Kinases
3.6. Effects on Apoptosis
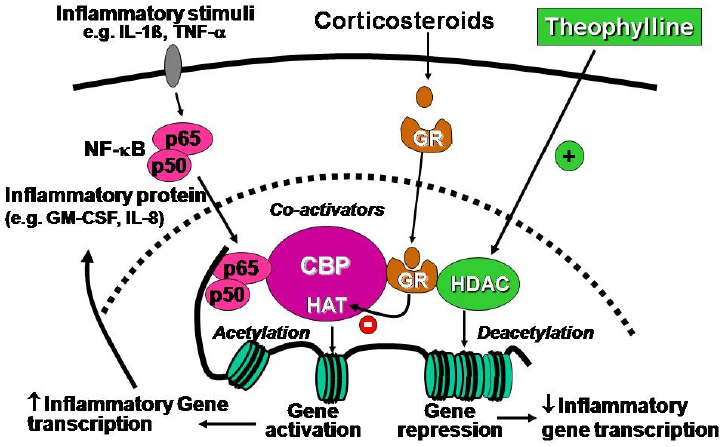
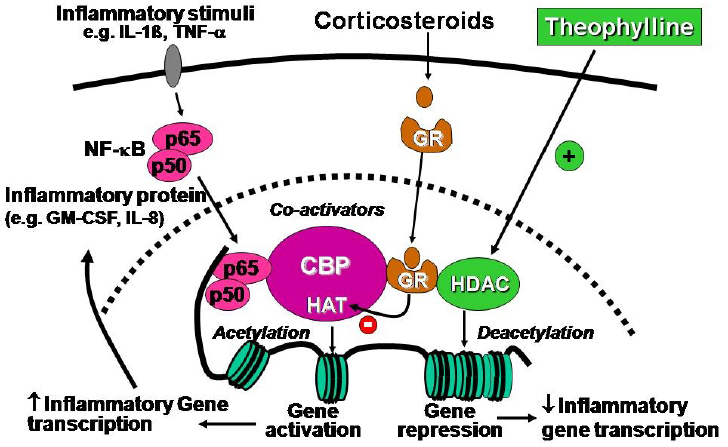
3.7. Histone Deacetylase Activation
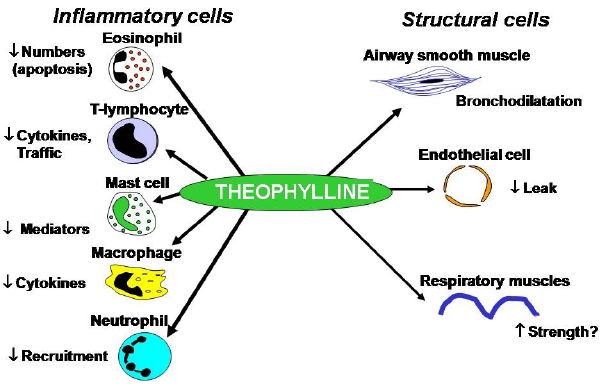
4. Cellular Effects

4.1. Airway Smooth Muscle Effects
4.2. Anti-inflammatory Effects
4.3. Immunomodulatory Effects
4.4. Extrapulmonary Effects
5. Pharmacokinetics
| Increased Clearance | Decreased Clearance |
|---|---|
|
|
5.1. Increased Clearance
5.2. Reduced Clearance
6. Routes of Administration
6.1. Intravenous
6.2. Oral
6.3. Other Routes
7. Clinical Use
7.1. Acute Exacerbations
7.2. Chronic Asthma
7.3. Add-on Therapy
7.4. COPD
7.5. Interaction with ß2-Agonists
8. Side Effects
9. Future Developments
References
- Lam, A.; Newhouse, M.T. Management of asthma and chronic airflow limitation. Are methylxanthines obsolete? Chest 1990, 98, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, M.; Hendeles, L. Theophylline in asthma. New Engl. J. Med. 1996, 334, 1380–1388. [Google Scholar]
- Barnes, P.J. Theophylline: New perspectives on an old drug. Am. J. Respir. Crit. Care Med. 2003, 167, 813–818. [Google Scholar]
- Persson, C.G.A. Development of safer xanthine drugs for the treatment of obstructive airways disease. J. Allergy Clin. Immunol. 1986, 78, 817–824. [Google Scholar]
- Shukla, D.; Chakraborty, S.; Singh, S.; Mishra, B. Doxofylline: A promising methylxanthine derivative for the treatment of asthma and chronic obstructive pulmonary disease. Expert. Opin. Pharmacother. 2009, 10, 2343–2356. [Google Scholar]
- Poolson, J.B.; Kazanowski, J.J.; Goldman, A.L.; Szentivanyi, A. Inhibition of human pulmonary phosphodiesterase activity by therapeutic levels of theophylline. Clin. Exp. Pharmacol. Physiol. 1978, 5, 535–539. [Google Scholar]
- Rabe, K.F.; Magnussen, H.; Dent, G. Theophylline and selective PDE inhibitors as bronchodilators and smooth muscle relaxants. Eur. Respir. J. 1995, 8, 637–642. [Google Scholar]
- Dent, G.; Giembycz, M.A.; Rabe, K.F.; Wolf, B.; Barnes, P.J.; Magnussen, H. Theophylline suppresses human alveolar macrophage respiratory burst through phosphodiesterase inhibition. Am. J. Resp. Cell Mol. Biol. 1994, 10, 565–572. [Google Scholar]
- Kume, H.; Hall, I.P.; Washabau, R.J.; Takagi, K.; Kotlikoff, M.I. Adrenergic agonists regulate KCa channels in airway smooth muscle by cAMP-dependent and -independent mechanisms. J. Clin. Invest. 1994, 93, 371–379. [Google Scholar]
- Beavo, J.A. Cyclic nucleotide phosphodiesterases: Functional implications of multiple isoforms. Physiol. Rev. 1995, 75, 725–748. [Google Scholar]
- Bachelet, M.; Vincent, D.; Havet, N.; Marrash-Chahla, R.; Pradalier, A.; Dry, J.; Vargaftig, B.B. Reduced responsiveness of adenylate cyclase in alveolar macrophages from patients with asthma. J. Allergy Clin. Immunol. 1991, 88, 322–328. [Google Scholar]
- Estenne, M.; Yernault, J.; De Troyer, A. Effects of parenteral aminophylline on lung mechanics in normal humans. Am. Rev. Respir. Dis. 1980, 121, 967–971. [Google Scholar]
- Pauwels, R.A.; Joos, G.F. Characterization of the adenosine receptors in the airways. Arch. Int. Pharmacodyn. Ther. 1995, 329, 151–156. [Google Scholar]
- Björk, T.; Gustafsson, L.E.; Dahlén, S.E. Isolated bronchi from asthmatics are hyperresponsive to adenosine, which apparently acts indirectly by liberation of leukotrienes and histamine. Am. Rev. Respir. Dis. 1992, 145, 1087–1091. [Google Scholar]
- Fozard, J.R.; Pfannkuche, H.J.; Schuurman, H.J. Mast cell degranulation following adenosine A3 receptor activation in rats. Eur. J. Pharmacol. 1996, 298, 293–297. [Google Scholar]
- Hannon, J.P.; Tigani, B.; Williams, I.; Mazzoni, L.; Fozard, J.R. Mechanism of airway hyperresponsiveness to adenosine induced by allergen challenge in actively sensitized Brown Norway rats. Br. J. Pharmacol. 2001, 132, 1509–1523. [Google Scholar]
- Polosa, R.; Blackburn, M.R. Adenosine receptors as targets for therapeutic intervention in asthma and chronic obstructive pulmonary disease. Trends Pharmacol. Sci. 2009, 30, 528–535. [Google Scholar]
- Cushley, M.J.; Tattersfield, A.E.; Holgate, S.T. Adenosine-induced bronchoconstriction in asthma: Antagonism by inhaled theophylline. Am. Rev. Respir. Dis. 1984, 129, 380–384. [Google Scholar]
- Cushley, M.J.; Holgate, S.T. Adenosine induced bronchoconstriction in asthma: Role of mast cell mediator release. J. Allergy Clin. Immunol. 1985, 75, 272–278. [Google Scholar]
- Inbe, H.; Watanabe, S.; Miyawaki, M.; Tanabe, E.; Encinas, J.A. Identification and characterization of a cell-surface receptor, P2Y15, for AMP and adenosine. J. Biol. Chem. 2004, 279, 19790–19799. [Google Scholar] [PubMed]
- Takanashi, S.; Hasegawa, Y.; Kanehira, Y.; Yamamoto, K.; Fujimoto, K.; Satoh, K.; Okamura, K. Interleukin-10 level in sputum is reduced in bronchial asthma, COPD and in smokers. Eur. Respir. J. 1999, 14, 309–314. [Google Scholar]
- Mascali, J.J.; Cvietusa, P.; Negri, J.; Borish, L. Anti-inflammatory effects of theophylline: Modulation of cytokine production. Ann. Allergy Asthma Immunol. 1996, 77, 34–38. [Google Scholar]
- Oliver, B.; Tomita, K.; Keller, A.; Caramori, G.; Adcock, I.; Chung, K.F.; Barnes, P.J.; Lim, S. Low-dose theophylline does not exert its anti-inflammatory effects in mild asthma through upregulation of interleukin-10 in alveolar macrophages. Allergy 2001, 56, 1087–1090. [Google Scholar]
- Tomita, K.; Chikumi, H.; Tokuyasu, H.; Yajima, H.; Hitsuda, Y.; Matsumoto, Y.; Sasaki, T. Functional assay of NF-kappaB translocation into nuclei by laser scanning cytometry: Inhibitory effect by dexamethasone or theophylline. Naunyn Schmiedebergs Arch. Pharmacol. 1999, 359, 249–255. [Google Scholar]
- Ichiyama, T.; Hasegawa, S.; Matsubara, T.; Hayashi, T.; Furukawa, S. Theophylline inhibits NF-kB activation and IkBa degradation in human pulmonary epithelial cells. Naunyn Schmiedebergs Arch. Pharmacol 2001, 364, 558–561. [Google Scholar]
- Foukas, L.C.; Daniele, N.; Ktori, C.; Anderson, K.E.; Jensen, J.; Shepherd, P.R. Direct effects of caffeine and theophylline on p110 delta and other phosphoinositide 3-kinases. Differential effects on lipid kinase and protein kinase activities. J. Biol.Chem. 2002, 277, 37124–37130. [Google Scholar] [PubMed]
- Yamamori, T.; Inanami, O.; Nagahata, H.; Kuwabara, M. Phosphoinositide 3-kinase regulates the phosphorylation of NADPH oxidase component p47(phox) by controlling cPKC/PKCdelta but not Akt. Biochem. Biophys. Res. Commun. 2004, 316, 720–730. [Google Scholar]
- To, M.; Ito, K.; Kizawa, Y.; Failla, M.; Ito, M.; Kusama, T.; Elliot, M.; Hogg, J.C.; Adcock, I.M.; Barnes, P.J. Targeting phosphoinositide-3-kinase-d with theophylline reverses corticosteroid insensitivity in COPD. Am. J. Resp. Crit. Care Med. 2010. ahead of print.. [Google Scholar]
- Yasui, K.; Hu, B.; Nakazawa, T.; Agematsu, K.; Komiyama, A. Theophylline accelerates human granulocyte apoptosis not via phosphodiesterase inhibition. J. Clin. Invest. 1997, 100, 1677–1684. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.Y.; Nam-Kung, E.K.; Lee, N.M.; Chang, H.S.; Kim, D.J.; Kim, Y.H.; Park, C.S. The downregulation of bcl-2 expression is necessary for theophylline-induced apoptosis of eosinophil. Cell Immunol. 2000, 203, 95–102. [Google Scholar]
- Yasui, K.; Agematsu, K.; Shinozaki, K.; Hokibara, S.; Nagumo, H.; Nakazawa, T.; Komiyama, A. Theophylline induces neutrophil apoptosis through adenosine A2A receptor antagonism. J. Leukoc. Biol. 2000, 67, 529–535. [Google Scholar]
- Ohta, K.; Yamashita, N. Apoptosis of eosinophils and lymphocytes in allergic inflammation. J. Allergy Clin. Immunol. 1999, 104, 14–21. [Google Scholar]
- Moonen, H.J.; Geraets, L.; Vaarhorst, A.; Bast, A.; Wouters, E.F.; Hageman, G.J. Theophylline prevents NAD+ depletion via PARP-1 inhibition in human pulmonary epithelial cells. Biochem. Biophys. Res Commun. 2005, 338, 1805–1810. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Adcock, I.M.; Ito, K. Histone acetylation and deacetylation: Importance in inflammatory lung diseases. Eur. Respir. J. 2005, 25, 552–563. [Google Scholar]
- Barnes, P.J. How corticosteroids control inflammation. Br. J Pharmacol. 2006, 148, 245–254. [Google Scholar]
- Ito, K.; Ito, M.; Elliott, W.M.; Cosio, B.; Caramori, G.; Kon, O.M.; Barczyk, A.; Hayashi, M.; Adcock, I.M.; Hogg, J.C.; Barnes, P.J. Decreased histone deacetylase activity in chronic obstructive pulmonary disease. New Engl. J. Med. 2005, 352, 1967–1976. [Google Scholar]
- Hew, M.; Bhavsar, P.; Torrego, A.; Meah, S.; Khorasani, N.; Barnes, P.J.; Adcock, I.; Chung, K.F. Relative corticosteroid insensitivity of peripheral blood mononuclear cells in severe asthma. Am. J. Respir. Crit. Care Med. 2006, 174, 134–141. [Google Scholar]
- Murahidy, A.; Ito, M.; Adcock, I.M.; Barnes, P.J.; Ito, K. Reduction is histone deacetylase expression and activity in smoking asthmatics: A mechanism of steroid resistance. Proc. Amer. Thorac. Soc. 2005, 2, A889. [Google Scholar]
- Ito, K.; Lim, S.; Caramori, G.; Cosio, B.; Chung, K.F.; Adcock, I.M.; Barnes, P.J. A molecular mechanism of action of theophylline: Induction of histone deacetylase activity to decrease inflammatory gene expression. Proc. Natl. Acad. Sci.USA 2002, 99, 8921–8926. [Google Scholar]
- Cosio, B.G.; Tsaprouni, L.; Ito, K.; Jazrawi, E.; Adcock, I.M.; Barnes, P.J. Theophylline restores histone deacetylase activity and steroid responses in COPD macrophages. J. Exp. Med. 2004, 200, 689–695. [Google Scholar]
- Ito, K.; Yamamura, S.; Essilfie-Quaye, S.; Cosio, B.; Ito, M.; Barnes, P.J.; Adcock, I.M. Histone deacetylase 2-mediated deacetylation of the glucocorticoid receptor enables NF-kB suppression. J. Exp. Med. 2006, 203, 7–13. [Google Scholar]
- Ricciardolo, F.L.; Caramori, G.; Ito, K.; Capelli, A.; Brun, P.; Abatangelo, G.; Papi, A.; Chung, K.F.; Adcock, I.; Barnes, P.J.; Donner, C.F.; Rossi, A.; Di Stefano, A. Nitrosative stress in the bronchial mucosa of severe chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2005, 116, 1028–1035. [Google Scholar]
- Osoata, G.O.; Hanazawa, T.; Brindicci, C.; Ito, M.; Barnes, P.J.; Kharitonov, S.; Ito, K. Peroxynitrite elevation in exhaled breath condensate of COPD and its inhibition by fudosteine. Chest. 2009, 135, 1513–1520. [Google Scholar]
- Osoata, G.; Adcock, I.M.; Barnes, P.J.; Ito, K. Oxidative stress causes HDAC2 reduction by nitration, ubiquitnylation and proteasomall degradation. Proc. Amer. Thorac. Soc. 2005, 2, A755. [Google Scholar]
- Hirano, T.; Yamagata, T.; Gohda, M.; Yamagata, Y.; Ichgikawa, T.; Yanagisawa, S.; Ueshima, K.; Akamatsu, K.; Nakanishi, M.; Matsunaga, K.; Ichimura, M.; Ichinose, M. Inhibition of reactive nitrogen species production in COPD airways: Comparison obetween inhaled corticosteroid and oral theophylline. Thorax 2006, 61, 761–766. [Google Scholar]
- Finney, M.J.B.; Karlson, J.A.; Persson, C.G.A. Effects of bronchoconstriction and bronchodilation on a novel human small airway preparation. Br. J. Pharmacol. 1985, 85, 29–36. [Google Scholar]
- Guillot, C.; Fornaris, M.; Badger, M.; Orehek, J. Spontaneous and provoked resistance to isoproterenol in isolated human bronchi. J. Allergy Clin. Immunol. 1984, 74, 713–718. [Google Scholar]
- Miura, M.; Belvisi, M.G.; Stretton, C.D.; Yacoub, M.H.; Barnes, P.J. Role of potassium channels in bronchodilator responses in human airways. Am. Rev. Respir. Dis. 1992, 146, 132–136. [Google Scholar]
- Goldie, R.G.; Spina, D.; Henry, P.J.; Lulich, K.M.; Paterson, J.W. In vitro responsiveness of human asthmatic bronchus to carbachol, histamine, b-adrenoceptor agonists and theophylline. Br. J. Clin. Pharmacol. 1986, 22, 669–676. [Google Scholar] [PubMed]
- Mitenko, P.A.; Ogilvie, R.I. Rational intravenous doses of theophylline. New Engl. J. Med. 1973, 289, 600–603. [Google Scholar]
- McWilliams, B.C.; Menendez, R.; Kelly, W.H.; Howick, J. Effects of theophylline on inhaled methacholine and histamine in asthmatic children. Am. Rev. Respir. Dis. 1984, 130, 193–197. [Google Scholar]
- Cartier, A.; Lemire, I.; L'Archeveque, J. Theophylline partially inhibits bronchoconstriction caused by inhaled histamine in subjects with asthma. J. Allergy Clin. Immunol. 1986, 77, 570–575. [Google Scholar]
- Magnusson, H.; Reuss, G.; Jorres, R. Theophylline has a dose-related effect on the airway response to inhaled histamine and methacholine in asthmatics. Am. Rev. Respir. Dis. 1987, 136, 1163–1167. [Google Scholar]
- Magnussen, H.; Reuss, G.; Jörres, R. Methylxanthines inhibit exercise-induced bronchoconstriction at low serum theophylline concentrations and in a dose-dependent fashion. J. Allergy Clin. Immunol. 1988, 81, 531–537. [Google Scholar]
- Orange, R.P.; Kaliner, M.A.; Laraia, P.J.; Austen, K.F. Immunological release of histamine and slow reacting substance of anaphylaxis from human lung. II. Influence of cellular levels of cyclic AMP. Fed. Proc. 1971, 30, 1725–1729. [Google Scholar] [PubMed]
- Nielson, C.P.; Crawley, J.J.; Morgan, M.E.; Vestal, R.E. Polymorphonuclear leukocyte inhibition by therapeutic concentrations of theophylline is mediated by cyclic 3',5' adenosine aminophosphate. Am. Rev. Respir. Dis. 1988, 137, 25–30. [Google Scholar]
- Kraft, M.; Pak, J.; Borish, L.; Martin, R.J. Theophylline's effect on neutrophil function and the late asthmatic response. J. Allergy Clin. Immunol. 1996, 98, 251–257. [Google Scholar]
- Schrier, D.J.; Imre, R.M. The effects of adenosine antagonists on human neutrophil function. J. Immunol. 1986, 137, 3284–3289. [Google Scholar]
- Yukawa, T.; Kroegel, C.; Dent, G.; Chanez, P.; Ukena, D.; Barnes, P.J. Effect of theophylline and adenosine on eosinophil function. Am. Rev. Respir. Dis. 1989, 140, 327–333. [Google Scholar]
- O'Neill, S.J.; Sitar, D.S.; Kilass, D.J. The pulmonary disposition of theophylline and its influences on human alveolar macrophage bactericidal function. Am. Rev. Respir. Dis. 1988, 134, 1225–1228. [Google Scholar]
- Lim, S.; Tomita, K.; Carramori, G.; Jatakanon, A.; Oliver, B.; Keller, A.; Adcock, I.; Chung, K.F.; Barnes, P.J. Low-dose theophylline reduces eosinophilic inflammation but not exhaled nitric oxide in mild asthma. Am. J. Respir. Crit. Care Med. 2001, 164, 273–276. [Google Scholar]
- Yasui, K.; Agematsu, K.; Shinozaki, K.; Hokibara, S.; Nagumo, H.; Yamada, S.; Kobayashi, N.; Komiyama, A. Effects of theophylline on human eosinophil functions: Comparative study with neutrophil functions. J. Leukoc. Biol. 2000, 68, 194–200. [Google Scholar]
- Erjefalt, I.; Persson, C.G.A. Pharmacologic control of plasma exudation into tracheobronchial airways. Am. Rev. Respir. Dis. 1991, 143, 1008–1014. [Google Scholar]
- Boschetto, P.; Roberts, N.M.; Rogers, D.F.; Barnes, P.J. The effect of antiasthma drugs on microvascular leak in guinea pig airways. Am. Rev. Respir. Dis. 1989, 139, 416–421. [Google Scholar]
- Naclerio, R.M.; Bartenfelder, D.; Proud, D.; Togias, A.G.; Meyers, D.A.; Kagey Sobotka, A.; Norman, P.S.; Lichtenstein, L.M. Theophylline reduces histamine release during pollen-induced rhinitis. J. Allergy Clin. Immunol. 1986, 78, 874–876. [Google Scholar]
- Yao, P.L.; Tsai, M.F.; Lin, Y.C.; Wang, C.H.; Liao, W.Y.; Chen, J.J.; Yang, P.C. Global expression profiling of theophylline response genes in macrophages: Evidence of airway anti-inflammatory regulation. Respir Res. 2005, 6, 89. [Google Scholar]
- Ward, A.J.M.; McKenniff, M.; Evans, J.M.; Page, C.P.; Costello, J.F. Theophylline - an immunomodulatory role in asthma? Am. Rev. Respir. Dis. 1993, 147, 518–523. [Google Scholar] [PubMed]
- Sullivan, P.; Bekir, S.; Jaffar, Z.; Page, C.; Jeffery, P.; Costello, J. Anti-inflammatory effects of low-dose oral theophylline in atopic asthma. Lancet 1994, 343, 1006–1008. [Google Scholar]
- Kraft, M.; Torvik, J.A.; Trudeau, J.B.; Wenzel, S.E.; Martin, R.J. Theophylline: Potential antiinflammatory effects in nocturnal asthma. J. Allergy Clin. Immunol. 1996, 97, 1242–1246. [Google Scholar]
- Culpitt, S.; Maziak, W.; Loukides, S.; Keller, A.; Barnes, P.J. Effect of theophylline on induced sputum inflammatory indices in COPD patients. Am. J. Respir. Crit. Care Med. 1997, 157, A797. [Google Scholar]
- Kobayashi, M.; Nasuhara, Y.; Betsuyaku, T.; Shibuya, E.; Tanino, Y.; Tanino, M.; Takamura, K.; Nagai, K.; Hosokawa, T.; Nishimura, M. Effect of low-dose theophylline on airway inflammation in COPD. Respirology 2004, 9, 249–254. [Google Scholar]
- Kanehara, M.; Yokoyama, A.; Tomoda, Y.; Shiota, N.; Iwamoto, H.; Ishikawa, N.; Taooka, Y.; Haruta, Y.; Hattori, N.; Kohno, N. Anti-inflammatory effects and clinical efficacy of theophylline and tulobuterol in mild-to-moderate chronic obstructive pulmonary disease. Pulm. Pharmacol. Ther. 2008, 21, 874–878. [Google Scholar]
- Wenzel, S.E.; Szefler, S.J.; Leung, D.Y.; Sloan, S.I.; Rex, M.D.; Martin, R.J. Bronchoscopic evaluation of severe asthma. Persistent inflammation associated with high dose glucocorticoids. Am. J. Respir. Crit. Care Med. 1997, 156, 737–743. [Google Scholar] [PubMed]
- Jatakanon, A.; Uasaf, C.; Maziak, W.; Lim, S.; Chung, K.F.; Barnes, P.J. Neutrophilic inflammation in severe persistent asthma. Am. J. Respir. Crit. Care Med. 1999, 160, 1532–1539. [Google Scholar]
- Shohat, B.; Volovitz, B.; Varsano, I. Induction of suppressor T cells in asthmatic children by theophylline treatment. Clin. Allergy 1983, 13, 487–493. [Google Scholar]
- Fink, G.; Mittelman, M.; Shohat, B.; Spitzer, S.A. Theophylline-induced alterations in cellular immunity in asthmatic patients. Clin. Allergy 1987, 17, 313–316. [Google Scholar]
- Guillou, P.J.; Ramsden, C.; Kerr, M.; Davison, A.M.; Giles, G.R. A prospective controlled clinical trial of aminophylline as an adjunct immunosuppressive agent. Transpl. Proc. 1984, 16, 1218–1220. [Google Scholar]
- Didier, M.; Aussel, C.; Ferrua, B.; Fehlman, M. Regulation of interleukin 2 synthesis by cAMP in human T cells. J. Immunol. 1987, 139, 1179–1184. [Google Scholar]
- Giembycz, M.A.; Corrigan, C.J.; Seybold, J.; Newton, R.; Barnes, P.J. Identification of cyclic AMP phosphodiesterases 3, 4 and 7 in human CD4+ and CD8+ T-lymphocytes. Br. J. Pharmacol. 1996, 118, 1945–1958. [Google Scholar]
- Hidi, R.; Timmermans, S.; Liu, E.; Schudt, C.; Dent, G.; Holgate, S.T.; Djukanovic, R. Phosphodiesterase and cyclic adenosine monophosphate-dependent inhibition of T-lymphocyte chemotaxis. Eur. Respir. J. 2000, 15, 342–349. [Google Scholar]
- Sanjar, S.; Aoki, S.; Kristersson, A.; Smith, D.; Morley, J. Antigen challenge induces pulmonary eosinophil accumulation and airway hyperreactivity in sensitized guinea pigs: The effect of anti-asthma drugs. Br. J. Pharmacol. 1990, 99, 679–686. [Google Scholar]
- Kosmas, E.N.; Michaelides, S.A.; Polychronaki, A.; Roussou, T.; Toukmatzi, S.; Polychronopoulos, V.; Baxevanis, C.N. Theophylline induces a reduction in circulating interleukin-4 and interleukin-5 in atopic asthmatics. Eur. Respir. J. 1999, 13, 53–58. [Google Scholar]
- Kidney, J.; Dominguez, M.; Taylor, P.M.; Rose, M.; Chung, K.F.; Barnes, P.J. Immunomodulation by theophylline in asthma: Demonstration by withdrawal of therapy. Am. J. Resp. Crit. Care Med. 1995, 151, 1907–1914. [Google Scholar]
- Jaffar, Z.H.; Sullivan, P.; Page, C.; Costello, J. Low-dose theophylline modulates T-lymphocyte activation in allergen-challenged asthmatics. Eur. Respir. J. 1996, 9, 456–462. [Google Scholar]
- Barnes, P.J.; Pauwels, R.A. Theophylline in asthma: Time for reappraisal? Eur. Resp. J. 1994, 7, 579–591. [Google Scholar] [CrossRef]
- Cushley, M.J.; Holgate, S.T. Bronchodilator actions of xanthine derivatives administered by inhalation in asthma. Thorax 1985, 40, 176–179. [Google Scholar]
- Aubier, M.; De Troyer, A.; Sampson, M.; Macklem, P.T.; Roussos, C. Aminophylline improves diaphragmatic contractility. New Engl. J. Med. 1981, 305, 249–252. [Google Scholar]
- Moxham, J. Aminophylline and the respiratory muscles: An alternative view. In: Respiratory Muscles : Function in health and disease. Clin. Chest. Med. 1988, 2, 325–340. [Google Scholar]
- Zhang, Z.Y.; Kaminsky, L.S. Characterization of human cytochromes P450 involved in theophylline 8-hydroxylation. Biochem. Pharmacol. 1995, 50, 205–211. [Google Scholar]
- Taylor, D.R.; Ruffin, D.; Kinney, C.D.; McDevitt, D.G. Investigation of diurnal changes in the disposition of theophylline. Br. J. Clin. Pharmac. 1983, 16, 413–416. [Google Scholar]
- Barnes, P.J.; Greening, A.P.; Neville, L.; Timmers, J.; Poole, G.W. Single dose slow-release aminophylline at night prevents nocturnal asthma. Lancet 1982, i, 299–301. [Google Scholar]
- Heins, M.; Kurtin, L.; Oellerich, M.; Maes, R.; Sybrecht, G.W. Nocturnal asthma: Slow-release terbutaline versus slow-release theophylline therapy. Eur. Respir. J. 1988, 1, 306–310. [Google Scholar]
- Bowler, S.D.; Mitchell, C.A.; Armstrong, J.G. Nebulised fenoterol and i.v. aminophylline in acute severe asthma. Eur. Resp. J. 1987, 70, 280–283. [Google Scholar]
- Parameswaran, K.; Belda, J.; Rowe, B.H. Addition of intravenous aminophylline to beta2-agonists in adults with acute asthma. Cochrane. Database. Syst. Rev. 2000. [Google Scholar]
- Mitra, A.; Bassler, D.; Goodman, K.; Lasserson, T.J.; Ducharme, F.M. Intravenous aminophylline for acute severe asthma in children over two years receiving inhaled bronchodilators. Cochrane. Database. Syst. Rev. 2005. [Google Scholar]
- Eason, J.; Makowe, H.L.J. Aminophylline toxicity - how many hospital asthma deaths does it cause? Resp. Med. 1989, 83, 219–226. [Google Scholar] [CrossRef]
- Duffy, N.; Walker, P.; Diamantea, F.; Calverley, P.M.; Davies, L. Intravenous aminophylline in patients admitted to hospital with non-acidotic exacerbations of chronic obstructive pulmonary disease: A prospective randomised controlled trial. Thorax 2005, 60, 713–717. [Google Scholar]
- Barr, R.G.; Rowe, B.H.; Camargo, C.A., Jr. Methylxanthines for exacerbations of chronic obstructive pulmonary disease: Meta-analysis of randomised trials. Br. Med. J. 2003, 327, 643. [Google Scholar]
- Wilson, A.J.; Gibson, P.G.; Coughlan, J. Long acting beta-agonists versus theophylline for maintenance treatment of asthma. Cochrane Database Syst. Rev. 2000, 2, CD001281. [Google Scholar]
- Nassif, E.G.; Weinburger, M.; Thompson, R.; Huntley, W. The value of maintenance theophylline in steroid-dependent asthma. New Engl. J. Med. 1981, 304, 71–75. [Google Scholar]
- Brenner, M.R.; Berkowitz, R.; Marshall, N.; Strunk, R.C. Need for theophylline in severe steroid-requiring asthmatics. Clin. Allergy 1988, 18, 143–150. [Google Scholar]
- Rivington, R.N.; Boulet, L.P.; Cote, J.; Kreisman, H.; Small, D.I.; Alexander, M.; Day, A.; Harsanyi, Z.; Darke, A.C. Efficacy of slow-release theophylline, inhaled salbutamol and their combination in asthmatic patients on high-dose inhaled steroids. Am. J. Respir. Crit. Care Med. 1995, 151, 325–332. [Google Scholar]
- Barnes, P.J. The role of theophylline in severe asthma. Eur. Respir. Rev. 1996, 6, 154S–159S. [Google Scholar]
- Markham, A.; Faulds, D. Theophylline. A review of its potential steroid sparing effects in asthma. Drugs 1998, 56, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- Selby, C.; Engleman, H.M.; Fitzpatrick, M.F.; Sime, P.M.; Mackay, T.W.; Douglas, N.J. Inhaled salmeterol or oral theophylline in nocturnal asthma? Am. J. Respir. Crit. Care Med. 1997, 155, 104–108. [Google Scholar] [PubMed]
- Evans, D.J.; Taylor, D.A.; Zetterstrom, O.; Chung, K.F.; O'Connor, B.J.; Barnes, P.J. A comparison of low-dose inhaled budesonide plus theophylline and high-dose inhaled budesonide for moderate asthma. New Engl. J. Med. 1997, 337, 1412–1418. [Google Scholar]
- Ukena, D.; Harnest, U.; Sakalauskas, R.; Magyar, P.; Vetter, N.; Steffen, H.; Leichtl, S.; Rathgeb, F.; Keller, A.; Steinijans, V.W. Comparison of addition of theophylline to inhaled steroid with doubling of the dose of inhaled steroid in asthma. Eur. Respir. J. 1997, 10, 2754–2760. [Google Scholar]
- Lim, S.; Groneberg, D.; Fischer, A.; Oates, T.; Caramori, G.; Mattos, W.; Adcock, I.; Barnes, P.J.; Chung, K.F. Expression of heme oxygenase isoenzymes 1 and 2 in normal and asthmatic airways. Effect of inhaled corticosteroids. Am. J. Respir. Crit. Care Med. 2000, 162, 1912–1918. [Google Scholar] [PubMed]
- Spears, M.; Donnelly, I.; Jolly, L.; Brannigan, M.; Ito, K.; McSharry, C.; Lafferty, J.; Chaudhuri, R.; Braganza, G.; Adcock, I.M.; Barnes, P.J.; Wood, S.; Thomson, N.C. Effect of theophylline plus beclometasone on lung function in smokers with asthma-a pilot study. Eur. Respir. J. 2009, 33, 1010–1017. [Google Scholar]
- Taylor, D.R.; Buick, B.; Kinney, C.; Lowry, R.C.; McDevitt, D.G. The efficacy of orally administered theophylline, inhaled salbutamol, and a combination of the two as chronic therapy in the management of chronic bronchitis with reversible airflow obstruction. Am. Rev. Respir. Dis. 1985, 131, 747–751. [Google Scholar] [PubMed]
- Murciano, D.; Avclair, M.H.; Parievte, R.; Aubier, M. A randomized controlled trial of theophylline in patients with severe chronic obstructive pulmonary disease. New Engl. J. Med. 1989, 320, 1521–1525. [Google Scholar]
- Chrystyn, H.; Mulley, B.A.; Peake, M.D. Dose response relation to oral theophylline in severe chronic obstructive airway disease. Br. Med. J. 1988, 297, 1506–1510. [Google Scholar]
- Culpitt, S.V.; de Matos, C.; Russell, R.E.; Donnelly, L.E.; Rogers, D.F.; Barnes, P.J. Effect of theophylline on induced sputum inflammatory indices and neutrophil chemotaxis in COPD. Am. J. Respir. Crit. Care Med. 2002, 165, 1371–1376. [Google Scholar]
- Cosio, B.G.; Iglesias, A.; Rios, A.; Noguera, A.; Sala, E.; Ito, K.; Barnes, P.J.; Agusti, A. Low-dose theophylline enhances the anti-inflammatory effects of steroids during exacerbations of chronic obstructive pulmonary disease. Thorax 2009, 64, 424–429. [Google Scholar]
- Barnes, P.J. Theophylline in chronic obstructive pulmonary disease: New horizons. Proc. Am. Thorac. Soc. 2005, 2, 334–339. [Google Scholar]
- Barnes, P.J. Theophylline for COPD. Thorax 2006, 61, 742–743. [Google Scholar]
- Kume, H.; Graziano, M.P.; Kotlikoff, M.I. Stimulatory and inhibitory regulation of calcium-activated potassium channels by guanine nucleotide binding proteins. Proc. Natl. Acad. Sci. USA 1992, 89, 11051–11055. [Google Scholar]
- Giembycz, M.A. Phosphodiesterase 4 and tolerance to beta 2-adrenoceptor agonists in asthma. Trends. Pharmacol. Sci. 1996, 17, 331–336. [Google Scholar]
- Cheung, D.; Wever, A.M.; de GOEIJ, J.A.; de GRAAFF, C.S.; Steen, H.; Sterk, P.J. Effects of theophylline on tolerance to the bronchoprotective actions of salmeterol in asthmatics in vivo. Am. J. Respir. Crit. Care Med. 1998, 158, 792–796. [Google Scholar] [PubMed]
- Williamson, B.H.; Milligan, C.; Griffiths, K.; Sparta, S.; Tribe, A.C.; Thompson, P.J. An assessment of major and minor side effects of theophylline. Aust. NZ J. Med. 1988, 19, 539. [Google Scholar]
- Nicholson, C.D.; Challiss, R.A.J.; Shahid, M. Differential modulation of tissue function and therapeutic potential of selective inhibitors of cyclic nucleotide phosphodiesterase isoenzymes. Trends Pharmacol. Sci. 1991, 12, 19–27. [Google Scholar]
- Kelloway, J.S.; Wyatt, R.A.; Adlis, S.A. Comparison of patients' compliance with prescribed oral and inhaled asthma medications. Arch. Int. Med. 1994, 154, 1349–1352. [Google Scholar]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Barnes, P.J. Theophylline. Pharmaceuticals 2010, 3, 725-747. https://doi.org/10.3390/ph3030725
Barnes PJ. Theophylline. Pharmaceuticals. 2010; 3(3):725-747. https://doi.org/10.3390/ph3030725
Chicago/Turabian StyleBarnes, Peter J. 2010. "Theophylline" Pharmaceuticals 3, no. 3: 725-747. https://doi.org/10.3390/ph3030725
APA StyleBarnes, P. J. (2010). Theophylline. Pharmaceuticals, 3(3), 725-747. https://doi.org/10.3390/ph3030725