
Circulating Exosomal miR-1290 for Diagnosis of Epithelial Ovarian Cancer

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Serum and Tissues Specimens from Patients
2.2. RNA Isolation and Assessment
2.3. Serum Exosomal RNA Isolation and Assessment
2.4. Small RNA Library Preparation and Sequencing
2.5. Identification of Known and Novel miRNAs
2.6. Proportions of miRNAs and Other RNAs
2.7. Statistical Analysis of Differential miRNA Expression
2.8. miRNA Preparation and Validation by qRT-PCR
2.9. Cell Transfection & Inhibition of miR-1290
2.10. miRNA Preparation and Validation by qRT-PCR
2.11. Western Blotting
2.12. Immunohistochemistry
2.13. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
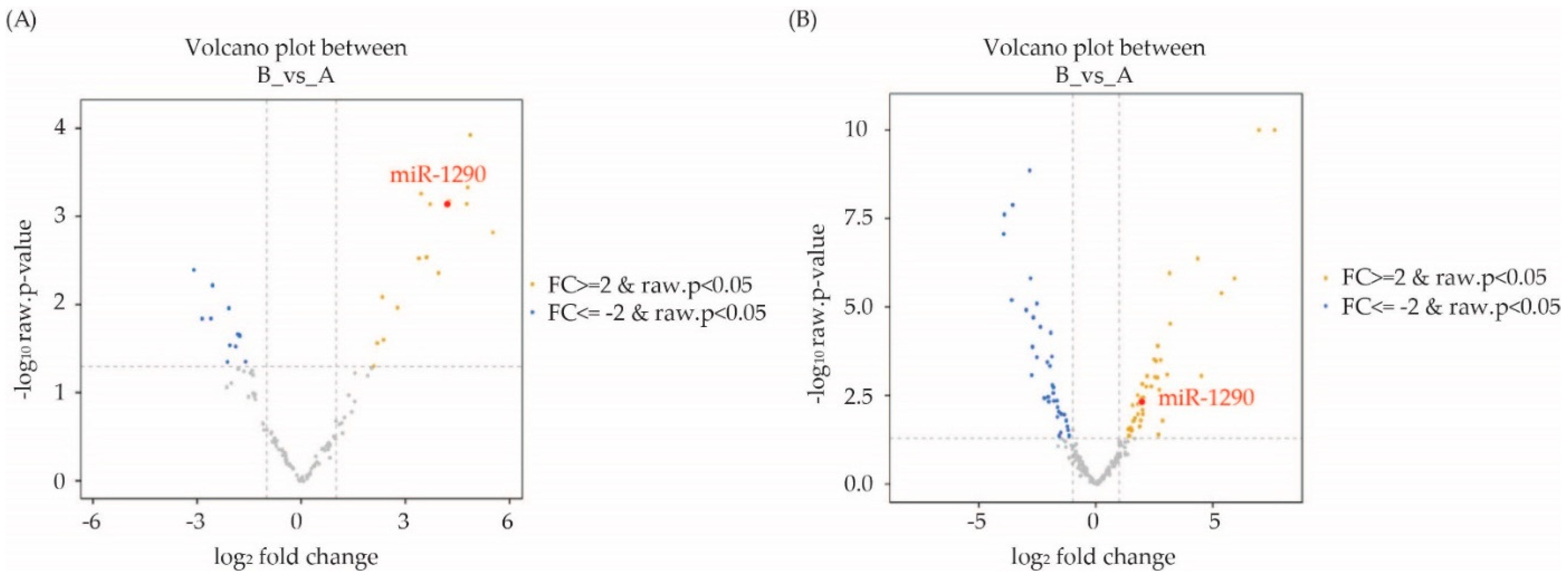
3.2. Differentially Expressed miRNAs in Malignant Ovarian Cancer Patients Based on RNA Sequencing: Identification of Candidate miRNAs
3.3. Validation of Candidate miRNAs by qRT-PCR
3.4. Diagnostic Value of Exosomal miRNA 1290 for Epithelial Ovarian Cancer
3.5. Decreased Expression of SOCS4 in Malignancy Group That Was Negatively Regulated by miRNA 1290
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goff, B.; Mandel, L.; Muntz, H.G.; Melancon, C.H. Ovarian carcinoma diagnosis. Cancer 2000, 89, 2068–2075. [Google Scholar] [CrossRef]
- Bast, R.; Feeney, M.; Lazarus, H.; Nadler, L.M.; Colvin, R.B.; Knapp, R.C. Reactivity of a monoclonal antibody with human ovarian carcinoma. J. Clin. Investig. 1981, 68, 1331–1337. [Google Scholar] [CrossRef] [Green Version]
- Sölétormos, G.; Duffy, M.J.; Abu Hassan, S.O.; Verheijen, R.H.; Tholander, B.; Bast, R.C.; Gaarenstroom, K.N.; Sturgeon, C.M.; Bonfrer, J.M.; Petersen, P.H.; et al. Clinical Use of Cancer Biomarkers in Epithelial Ovarian Cancer: Updated Guidelines from the European Group on Tumor Markers. Int. J. Gynecol. Cancer 2016, 26, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Van Calster, B.; Timmerman, D.; Bourne, T.; Testa, A.C.; Van Holsbeke, C.; Domali, E.; Jurkovic, D.; Neven, P.; Van Huffel, S.; Valentin, L. Discrimination between benign and malignant adnexal masses by specialist ultrasound examination versus serum CA-125. J. Natl. Cancer Inst. 2007, 99, 1706–1714. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C., Jr.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Van Gorp, T.; Cadron, I.; Despierre, E.; Daemen, A.; Leunen, K.; Amant, F.; Timmerman, D.; De Moor, B.; Vergote, I. HE4 and CA125 as a diagnostic test in ovarian cancer: Prospective validation of the Risk of Ovarian Malignancy Algorithm. Br. J. Cancer 2011, 104, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.W.; Smith, A.; DeSimone, C.P.; Seamon, L.; Goodrich, S.; Podzielinski, I.; Sokoll, L.; van Nagell, J.R., Jr.; Zhang, Z.; Ueland, F.R. Performance of the American College of Obstetricians and Gynecologists’ ovarian tumor referral guidelines with a multivariate index assay. Obstet Gynecol. 2011, 117, 1298–1306. [Google Scholar] [CrossRef] [Green Version]
- Green, T.M.; Alpaugh, M.L.; Barsky, S.H.; Rappa, G.; Lorico, A. Breast Cancer-Derived Extracellular Vesicles: Characterization and Contribution to the Metastatic Phenotype. BioMed Res. Int. 2015, 2015, 634865. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Yu, F.; Ding, H.; Wang, Y.; Li, P.; Wang, K. Emerging Function and Clinical Values of Exosomal MicroRNAs in Cancer. Mol. Ther. Nucleic Acids 2019, 16, 791–804. [Google Scholar] [CrossRef] [Green Version]
- Sempere, L.F.; Keto, J.; Fabbri, M. Exosomal MicroRNAs in Breast Cancer towards Diagnostic and Therapeutic Applications. Cancers 2017, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Sun, J.; Wang, X.; Hu, T.; Ma, Y.; Kong, C.; Piao, H.; Yu, T.; Zhang, G. Exosomes: A Promising Avenue for the Diagnosis of Breast Cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033818821421. [Google Scholar] [CrossRef] [Green Version]
- Bahrami, A.; Aledavood, A.; Anvari, K.; Hassanian, S.M.; Maftouh, M.; Yaghobzade, A.; Salarzaee, O.; ShahidSales, S.; Avan, A. The prognostic and therapeutic application of microRNAs in breast cancer: Tissue and circulating microRNAs. J. Cell. Physiol. 2018, 233, 774–786. [Google Scholar] [CrossRef]
- Van der Meel, R.; Fens, M.H.; Vader, P.; van Solinge, W.W.; Eniola-Adefeso, O.; Schiffelers, R.M. Extracellular vesicles as drug delivery systems: Lessons from the liposome field. J. Control. Release 2014, 195, 72–85. [Google Scholar] [CrossRef]
- Liang, Y.; Duan, L.; Lu, J.; Xia, J. Engineering exosomes for targeted drug delivery. Theranostics 2021, 11, 3183–3195. [Google Scholar] [CrossRef]
- Taylor, D.D.; Gercel-Taylor, C. MicroRNA signatures of tumor-derived exosomes as diagnostic biomarkers of ovarian cancer. Gynecol. Oncol. 2008, 110, 13–21. [Google Scholar] [CrossRef]
- Shah, J.S.; Gard, G.B.; Yang, J.; Maidens, J.; Valmadre, S.; Soon, P.S.; Marsh, D.J. Combining serum microRNA and CA-125 as prognostic indicators of preoperative surgical outcome in women with high-grade serous ovarian cancer. Gynecol. Oncol. 2018, 148, 181–188. [Google Scholar] [CrossRef]
- Kobayashi, M.; Sawada, K.; Nakamura, K.; Yoshimura, A.; Miyamoto, M.; Shimizu, A.; Ishida, K.; Nakatsuka, E.; Kodama, M.; Hashimoto, K.; et al. Exosomal miR-1290 is a potential biomarker of high-grade serous ovarian carcinoma and can discriminate patients from those with malignancies of other histological types. J. Ovarian Res. 2018, 11, 81. [Google Scholar] [CrossRef] [Green Version]
- Morin, R.D.; O’Connor, M.D.; Griffith, M.; Kuchenbauer, F.; Delaney, A.; Prabhu, A.-L.; Zhao, Y.; McDonald, H.; Zeng, T.; Hirst, M.; et al. Application of massively parallel sequencing to microRNA profiling and discovery in human embryonic stem cells. Genome Res. 2008, 18, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Li, A.; Yu, J.; Kim, H.; Wolfgang, C.L.; Canto, M.I.; Hruban, R.H.; Goggins, M. MicroRNA Array Analysis Finds Elevated Serum miR-1290 Accurately Distinguishes Patients with Low-Stage Pancreatic Cancer from Healthy and Disease Controls. Clin. Cancer Res. 2013, 19, 3600–3610. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; He, X.-Y.; Zhang, Z.-M.; Li, S.; Ren, L.-H.; Cao, R.-S.; Feng, Y.-D.; Ji, Y.-L.; Zhao, Y.; Shi, R.-H. MicroRNA-1290 promotes esophageal squamous cell carcinoma cell proliferation and metastasis. World J. Gastroenterol. 2015, 21, 3245–3255. [Google Scholar] [CrossRef]
- Wu, J.; Ji, X.; Zhu, L.; Jiang, Q.; Wen, Z.; Xu, S.; Shao, W.; Cai, J.; Du, Q.; Zhu, Y.; et al. Up-regulation of microRNA-1290 impairs cytokinesis and affects the reprogramming of colon cancer cells. Cancer Lett. 2013, 329, 155–163. [Google Scholar] [CrossRef]
- Zhang, W.C.; Chin, T.M.; Yang, H.; Nga, M.E.; Lunny, D.P.; Lim, E.K.; Sun, L.L.; Pang, Y.H.; Leow, Y.N.; Malusay, S.R.; et al. Tumour-initiating cell-specific miR-1246 and miR-1290 expression converge to promote non-small cell lung cancer progression. Nat. Commun. 2016, 7, 11702. [Google Scholar] [CrossRef]
- Xiao, X.; Yang, D.; Gong, X.; Mo, D.; Pan, S.; Xu, J. miR-1290 promotes lung adenocarcinoma cell proliferation and invasion by targeting SOCS4. Oncotarget 2018, 9, 11977–11988. [Google Scholar] [CrossRef] [Green Version]
- Starr, R.; Willson, T.A.; Viney, E.M.; Murray, L.J.; Rayner, J.R.; Jenkins, B.J.; Gonda, T.J.; Alexander, W.S.; Metcalf, D.; Nicola, N.A.; et al. A family of cytokine-inducible inhibitors of signalling. Nature 1997, 387, 917–921. [Google Scholar] [CrossRef] [PubMed]
- McCormick, S.; Heller, N.M. Regulation of Macrophage, Dendritic Cell, and Microglial Phenotype and Function by the SOCS Proteins. Front. Immunol. 2015, 6, 549. [Google Scholar] [CrossRef] [Green Version]
- Sasi, W.; Jiang, W.G.; Sharma, A.; Mokbel, K. Higher expression levels of SOCS 1,3,4,7 are associated with earlier tumour stage and better clinical outcome in human breast cancer. BMC Cancer 2010, 10, 178. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FFPE | Total (n = 82) | Type | p-Value | |
|---|---|---|---|---|
| Benign (n = 15) | EOC (n = 67) | |||
| Age (years, mean ± SD) | 51.80 ± 11.74 | 46.27 ± 15.72 | 53.04 ± 10.4 | 0.1297 |
| FIGO stage (%) | n(%) | n(%) | n(%) | |
| Stage1 | 26 (38.81) | - | 26 (38.81) | - |
| Stage2 | 7 (10.44) | - | 7 (10.44) | |
| Stage3 | 26 (38.81) | - | 26 (38.81) | |
| Stage4 | 8 (11.94) | - | 8 (11.94) | |
| CA 125 (U/mL) | ||||
| ≥35 | 60 (73.17) | 4 (26.67) | 56 (83.58) | <0.001 |
| <35 | 22 (26.83) | 11 (73.33) | 11 (16.42) | |
| miR-1290 | ||||
| ≥1.71 | 66 (80.49) | 65 (97.01) | 1 (6.67) | <0.001 |
| <1.71 | 16 (19.51) | 2 (2.99) | 14 (93.33) | |
| Serum | Total (n = 84) | Type | p-Value | |
|---|---|---|---|---|
| Benign (n = 13) | EOC (n = 71) | |||
| Age (years, mean ± SD) | 51.81 ± 11.66 | 45.46 ± 14.36 | 52.97 ± 10.82 | 0.0933 |
| FIGO stage (%) | n(%) | n(%) | n(%) | |
| Stage1 | 25 (35.21) | - | 25 (35.21) | >0.99 |
| Stage2 | 5 (7.04) | - | 5 (7.04) | |
| Stage3 | 34 (47.89) | - | 34 (47.89) | |
| Stage4 | 7 (9.86) | - | 7 (9.86) | |
| CA 125 (U/mL) | ||||
| ≥35 | 64 (76.19) | 6 (46.15) | 58 (81.69) | 0.011 |
| <35 | 20 (23.81) | 7 (53.85) | 13 (18.31) | |
| miR-1290 | ||||
| ≥0.73 | 66 (78.57) | 4 (30.77) | 62 (87.32) | <0.001 |
| <0.73 | 18 (21.43) | 9 (69.23) | 9 (12.68) | |
| Mature miRNA | Fold Change in Tissue | Fold Change in Serum |
|---|---|---|
| has-miR-1246 | 6.78 | 27.61 |
| has-miR-1290 | 3.66 | 27.04 |
| has-miR-21-5p | 4.1 | −3.43 |
| has-miR-7-5p | 41.33 | −4.27 |
| has-miR-93-5p | 3.76 | −4.39 |
| has-miR-16-5p | 2.63 | −8.58 |
| has-miR-29c-3p | −2.4 | −3.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, H.; Seo, S.M.; Kim, T.W.; Ryu, J.; Kong, H.; Jang, S.H.; Jang, Y.S.; Kim, K.S.; Kim, J.H.; Ryu, S.; et al. Circulating Exosomal miR-1290 for Diagnosis of Epithelial Ovarian Cancer. Curr. Issues Mol. Biol. 2022, 44, 288-300. https://doi.org/10.3390/cimb44010021
Jeon H, Seo SM, Kim TW, Ryu J, Kong H, Jang SH, Jang YS, Kim KS, Kim JH, Ryu S, et al. Circulating Exosomal miR-1290 for Diagnosis of Epithelial Ovarian Cancer. Current Issues in Molecular Biology. 2022; 44(1):288-300. https://doi.org/10.3390/cimb44010021
Chicago/Turabian StyleJeon, Hyeji, Su Min Seo, Tae Wan Kim, Jaesung Ryu, Hyejeong Kong, Si Hyeong Jang, Yong Soo Jang, Kwang Seock Kim, Jae Hoon Kim, Seongho Ryu, and et al. 2022. "Circulating Exosomal miR-1290 for Diagnosis of Epithelial Ovarian Cancer" Current Issues in Molecular Biology 44, no. 1: 288-300. https://doi.org/10.3390/cimb44010021
APA StyleJeon, H., Seo, S. M., Kim, T. W., Ryu, J., Kong, H., Jang, S. H., Jang, Y. S., Kim, K. S., Kim, J. H., Ryu, S., & Jeon, S. (2022). Circulating Exosomal miR-1290 for Diagnosis of Epithelial Ovarian Cancer. Current Issues in Molecular Biology, 44(1), 288-300. https://doi.org/10.3390/cimb44010021