
Cannabis, Cannabinoids, and Stroke: Increased Risk or Potential for Protection—A Narrative Review



Abstract

1. Introduction
2. Negative Impacts of Cannabis Use on Stroke
2.1. Epidemiology
2.2. Age Groups
2.3. Dose, Frequency and Time Dependency
2.4. Co-Consumption
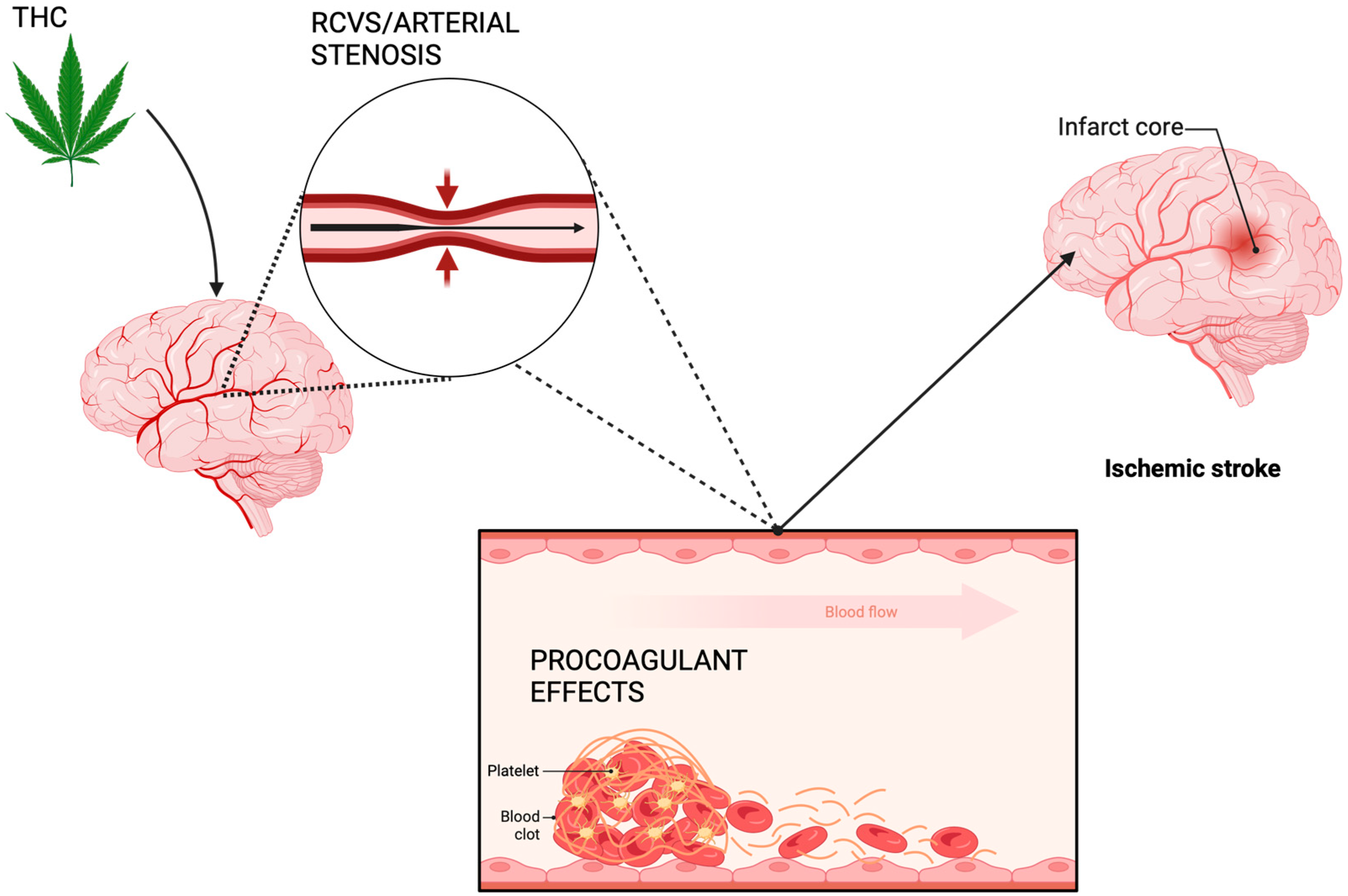
2.5. Mechanisms of Action
3. Potential Positive Effects of Cannabinoids on Stroke Outcome
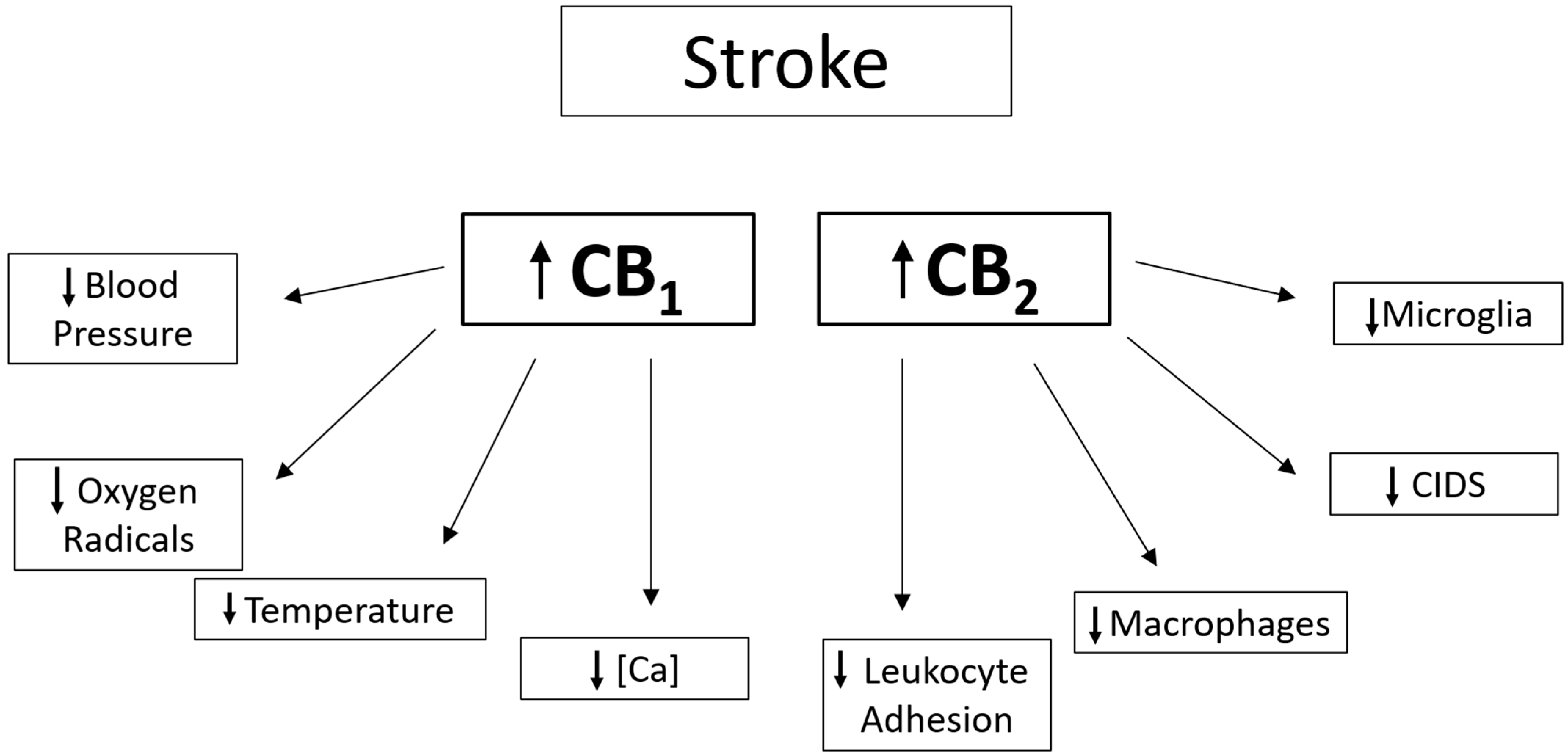
3.1. CB1 Receptor Agonism
3.2. CB1 Receptor Antagonism
3.3. CB2 Receptor Agonism
3.4. CB2 Receptor Antagonism
3.5. Co-Antagonism of CB1 and CB2
3.6. Limitations and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Falkstedt, D.; Wolff, V.; Allebeck, P.; Hemmingsson, T.; Danielsson, A.-K. Cannabis, Tobacco, Alcohol Use, and the Risk of Early Stroke. Stroke 2017, 48, 265–270. [Google Scholar] [CrossRef]
- Singh, A.; Saluja, S.; Kumar, A.; Agrawal, S.; Thind, M.; Nanda, S.; Shirani, J. Cardiovascular Complications of Marijuana and Related Substances: A Review. Cardiol. Ther. 2018, 7, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Maurya, N.; Velmurugan, B.K. Therapeutic applications of cannabinoids. Chem. Interact. 2018, 293, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Latorre, J.G.S.; Schmidt, E.B. Cannabis, Cannabinoids, and Cerebral Metabolism: Potential Applications in Stroke and Disorders of the Central Nervous System. Curr. Cardiol. Rep. 2015, 17, 72. [Google Scholar] [CrossRef] [PubMed]
- Page, R.L.; Allen, L.A.; Kloner, R.A.; Carriker, C.R.; Martel, C.; Morris, A.A.; Piano, M.R.; Rana, J.S.; Saucedo, J.F.; On behalf of the American Heart Association Clinical Pharmacology Committee and Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; et al. Medical Marijuana, Recreational Cannabis, and Cardiovascular Health: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e131–e152. [Google Scholar] [CrossRef]
- Cristino, L.; Bisogno, T.; Di Marzo, V. Cannabinoids and the expanded endocannabinoid system in neurological disorders. Nat. Rev. Neurol. 2020, 16, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, B.; Testai, F.D. Cerebrovascular Complications Associated with Marijuana Use. Curr. Neurol. Neurosci. Rep. 2021, 21, 25. [Google Scholar] [CrossRef]
- Amin, M.R.; Ali, D.W. Pharmacology of Medical Cannabis. In Recent Advances in Cannabinoid Physiology and Pathology; Springer: Berlin/Heidelberg, Germany, 2019; pp. 151–165. [Google Scholar] [CrossRef]
- Thanvi, B.R.; Treadwell, S.D. Cannabis and Stroke: Is there a link? Postgrad. Med. J. 2009, 85, 80–83. [Google Scholar] [CrossRef]
- Di Marzo, V.; Piscitelli, F. The Endocannabinoid System and its Modulation by Phytocannabinoids. Neurotherapeutics 2015, 12, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.; Kumar, U. Cannabinoid Receptors and the Endocannabinoid System: Signaling and Function in the Central Nervous System. Int. J. Mol. Sci. 2018, 19, 833. [Google Scholar] [CrossRef] [PubMed]
- Basavarajappa, B.S.; Shivakumar, M.; Joshi, V.; Subbanna, S. Endocannabinoid system in neurodegenerative disorders. J. Neurochem. 2017, 142, 624–648. [Google Scholar] [CrossRef] [PubMed]
- Tsatsakis, A.; Docea, A.O.; Calina, D.; Tsarouhas, K.; Zamfira, L.-M.; Mitrut, R.; Sharifi-Rad, J.; Kovatsi, L.; Siokas, V.; Dardiotis, E.; et al. A Mechanistic and Pathophysiological Approach for Stroke Associated with Drugs of Abuse. J. Clin. Med. 2019, 8, 1295. [Google Scholar] [CrossRef] [PubMed]
- Jones, É.; Vlachou, S. A Critical Review of the Role of the Cannabinoid Compounds Δ9-Tetrahydrocannabinol (Δ9-THC) and Cannabidiol (CBD) and their Combination in Multiple Sclerosis Treatment. Molecules 2020, 25, 4930. [Google Scholar] [CrossRef] [PubMed]
- Easton, J.D.; Saver, J.L.; Albers, G.W.; Alberts, M.J.; Chaturvedi, S.; Feldmann, E.; Hatsukami, T.S.; Higashida, R.T.; Johnston, S.C.; Kidwell, C.S.; et al. Definition and Evaluation of Transient Ischemic Attack. Stroke 2009, 40, 2276–2293. [Google Scholar] [CrossRef] [PubMed]
- Montaño, A.; Hanley, D.F.; Hemphill, J.C. Hemorrhagic Stroke. Handb. Clin. Neurol. 2021, 176, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, A.C.; Ferro, J.M. Drug Abuse and Stroke. Curr. Neurol. Neurosci. Rep. 2013, 13, 325. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Stroke, Cerebrovascular Accident. Available online: https://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html (accessed on 23 March 2024).
- Piano, M.R. Cannabis Smoking and Cardiovascular Health: It’s Complicated. Clin. Pharmacol. Ther. 2017, 102, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Archie, S.R.; Cucullo, L. Harmful Effects of Smoking Cannabis: A Cerebrovascular and Neurological Perspective. Front. Pharmacol. 2019, 10, 1481. [Google Scholar] [CrossRef] [PubMed]
- Fernández-López, D.; Faustino, J.; Derugin, N.; Wendland, M.; Lizasoain, I.; Moro, M.; Vexler, Z. Reduced infarct size and accumulation of microglia in rats treated with WIN 55,212-2 after neonatal stroke. Neuroscience 2012, 207, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Hackram, D. Cannabis and Stroke: Systemic appraisal of case reports. Stroke 2015, 46, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Jouanjus, E.; Raymond, V.; Lapeyre-Mestre, M.; Wolff, V. What is the Current Knowledge About the Cardiovascular Risk for Users of Cannabis-Based Products? A Systematic Review. Curr. Atheroscler. Rep. 2017, 19, 26. [Google Scholar] [CrossRef] [PubMed]
- Westover, A.N.; McBride, S.; Haley, R.W. Stroke in Young Adults Who Abuse Amphetamines or Cocaine. Arch. Gen. Psychiatry 2007, 64, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Wolff, V.; Jouanjus, E. Strokes are possible complications of cannabinoids use. Epilepsy Behav. 2017, 70, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Middlekauff, H.R.; Cooper, Z.D.; Strauss, S.B. Drugs of Misuse: Focus on Vascular Dysfunction. Can. J. Cardiol. 2022, 38, 1364–1377. [Google Scholar] [CrossRef] [PubMed]
- Wolff, V.; Lauer, V.; Rouyer, O.; Sellal, F.; Meyer, N.; Raul, J.S.; Sabourdy, C.; Boujan, F.; Jahn, C.; Beaujeux, R.; et al. Cannabis Use, Ischemic Stroke, and Multifocal Intracranial Vasoconstriction. Stroke 2011, 42, 1778–1780. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Singh, S.; Patel, K.; Goyal, H.; Shah, M.; Mansuri, Z.; Patel, S.; Mahuwala, Z.K.; Goldstein, L.B.; Qureshi, A.I. Stroke in young cannabis users (18–49 years): National trends in hospitalizations and outcomes. Int. J. Stroke 2020, 15, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Johnston, L.; Miech, R.; O’Malley, P.; Bachman, J.; Schulenberg, J.; Patrick, M. Monitoring the Future National Survey Results on Drug Use, 1975–2018: Overview, Key Findings on Adolescent Drug Use; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2019. [Google Scholar]
- O’keefe, E.L.; Peterson, T.M.; Lavie, C.J. Reevaluating America’s Latest Pharmaceutical Trend: The Cardiovascular Risk of Cannabis. Curr. Opin. Psychol. 2021, 38, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Wolff, V.; Armspach, J.-P.; Lauer, V.; Rouyer, O.; Bataillard, M.; Marescaux, C.; Geny, B. Cannabis-related Stroke. Stroke 2013, 44, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Dabhi, N.; Mastorakos, P.; Sokolowski, J.D.; Kellogg, R.T.; Park, M.S. Effect of drug use in the treatment of acute ischemic stroke: A scoping review. Surg. Neurol. Int. 2022, 13, 367. [Google Scholar] [CrossRef] [PubMed]
- Kalla, A.; Krishnamoorthy, P.M.; Gopalakrishnan, A.; Figueredo, V.M. Cannabis use predicts risks of heart failure and cerebrovascular accidents. J. Cardiovasc. Med. 2018, 19, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Cooles, P.; Michaud, R. Stroke after heavy cannabis smoking. Postgrad. Med. J. 1987, 63, 511. [Google Scholar] [CrossRef]
- Yu, S.-J.; Reiner, D.; Shen, H.; Wu, K.-J.; Liu, Q.-R.; Wang, Y. Time-Dependent Protection of CB2 Receptor Agonist in Stroke. PLoS ONE 2015, 10, e0132487. [Google Scholar] [CrossRef] [PubMed]
- Mittleman, M.A.; Lewis, R.A.; Maclure, M.; Sherwood, J.B.; Muller, J.E. Triggering Myocardial Infarction by Marijuana. Circulation 2001, 103, 2805–2809. [Google Scholar] [CrossRef]
- Parekh, T.; Pemmasani, S.; Desai, R. Marijuana Use Among Young Adults (18–44 Years of Age) and Risk of Stroke. Stroke 2020, 51, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Tirkey, N.K.; Gupta, S. Acute Antero-Inferior Wall Ischaemia with Acute Ischaemic Stroke Caused by Oral Ingestion of Cannabis in a Young Male. J. Assoc. Physicians India 2016, 64, 93–94. [Google Scholar] [PubMed]
- Volpon, L.C.; Sousa, C.L.M.D.M.; Moreira, S.K.K.; Teixeira, S.R.; Carlotti, A.P.D.C.P. Multiple Cerebral Infarcts in a Young Patient Associated with Marijuana Use. J. Addict. Med. 2017, 11, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Šimůnek, L.; Krajina, A.; Herzig, R.; Vališ, M. Cerebral Infarction in Young Marijuana Smokers—Case Reports. Acta Medica 2018, 61, 74–77. [Google Scholar] [CrossRef]
- Hemachandra, D.; McKetin, R.; Cherbuin, N.; Anstey, K.J. Heavy cannabis users at elevated risk of stroke: Evidence from a general population survey. Aust. N. Z. J. Public Health 2016, 40, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Rumalla, K.; Reddy, A.Y.; Mittal, M.K. Recreational marijuana use and acute ischemic stroke: A population-based analysis of hospitalized patients in the United States. J. Neurol. Sci. 2016, 364, 191–196. [Google Scholar] [CrossRef]
- Yau, W.Y.; Chu, E.; Lai, N. Cannabis, serotonergic drug use and stroke in a 50-year-old woman. Intern. Med. J. 2015, 45, 1312–1313. [Google Scholar] [CrossRef] [PubMed]
- Geller, T.; Loftis, L.; Brink, D.S. Cerebellar Infarction in Adolescent Males Associated with Acute Marijuana Use. Pediatrics 2004, 113, e365–e370. [Google Scholar] [CrossRef] [PubMed]
- Russmann, S.; Winkler, A.; Lövblad, K.; Stanga, Z.; Bassetti, C. Lethal Ischemic Stroke after Cisplatin-Based Chemotherapy for Testicular Carcinoma and Cannabis Inhalation. Eur. Neurol. 2002, 48, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Auger, N.; Paradis, G.; Low, N.; Ayoub, A.; He, S.; Potter, B.J. Cannabis use disorder and the future risk of cardiovascular disease in parous women: A longitudinal cohort study. BMC Med. 2020, 18, 328. [Google Scholar] [CrossRef] [PubMed]
- Barber, P.A.; Pridmore, H.M.; Krishnamurthy, V.; Roberts, S.; Spriggs, D.A.; Carter, K.N.; Anderson, N.E. Cannabis, Ischemic Stroke, and Transient Ischemic Attack. Stroke 2013, 44, 2327–2329. [Google Scholar] [CrossRef]
- Mathew, R.J.; Wilson, W.H.; Humphreys, D.; Lowe, J.V.; Wiethe, K.E. Middle cerebral artery velocity during upright posture after marijuana smoking. Acta Psychiatr. Scand. 1992, 86, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Swetlik, C.; Migdady, I.; Hasan, L.Z.; Buletko, A.B.; Price, C.M.; Cho, S.-M.D. Cannabis Use and Stroke: Does a Risk Exist? J. Addict. Med. 2022, 16, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Wolff, V.; Schlagowski, A.-I.; Rouyer, O.; Charles, A.-L.; Singh, F.; Auger, C.; Schini-Kerth, V.; Marescaux, C.; Raul, J.-S.; Zoll, J.; et al. Tetrahydrocannabinol Induces Brain Mitochondrial Respiratory Chain Dysfunction and Increases Oxidative Stress: A Potential Mechanism Involved in Cannabis-Related Stroke. BioMed Res. Int. 2015, 2015, 323706. [Google Scholar] [CrossRef] [PubMed]
- Mikami, T.; Obata, R.; Steinberg, D.I.; Skliut, M.; Boniece, I. Marijuana-related Reversible Cerebral Vasoconstriction Syndrome. Intern. Med. 2021, 60, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Kloner, R.A.; Rezkalla, S. Adverse Cardiovascular, Cerebrovascular, and Peripheral Vascular Effects of Marijuana Inhalation: What Cardiologists Need to Know. Am. J. Cardiol. 2014, 113, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-H.; Mou, Y.; Silva, A.C. Cannabis and Cannabinoid Biology in Stroke. Stroke 2019, 50, 2640–2645. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.S.; Quenardelle, V.; Rouyer, O.; Raul, J.S.; Beaujeux, R.; Gény, B.; Wolff, V. A Systematic Review of the Complex Effects of Cannabinoids on Cerebral and Peripheral Circulation in Animal Models. Front. Physiol. 2018, 9, 622. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, S.B. Stroke after heavy marijuana smoking. Stroke 1991, 22, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Testai, F.D.; Gorelick, P.B.; Aparicio, H.J.; Filbey, F.M.; Gonzalez, R.; Gottesman, R.F.; Melis, M.; Piano, M.R.; Rubino, T.; Song, S.Y.; et al. Use of Marijuana: Effect on Brain Health: A Scientific Statement from the American Heart Association. Stroke 2022, 53, E176–E187. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, C.; Chouinard, F.; Lefebvre, J.S.; Flamand, N. Regulation of inflammation by cannabinoids, the endocannabinoids 2-arachidonoyl-glycerol and arachidonoyl-ethanolamide, and their metabolites. J. Leukoc. Biol. 2015, 97, 1049–1070. [Google Scholar] [CrossRef] [PubMed]
- Dahdouh, Z.; Roule, V.; Lognoné, T.; Sabatier, R.; Grollier, G. Cannabis and coronary thrombosis: What is the role of platelets? Platelets 2012, 23, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Steffens, S.; Haskó, G.; Schindler, T.H.; Kunos, G. Cardiovascular effects of marijuana and synthetic cannabinoids: The good, the bad, and the ugly. Nat. Rev. Cardiol. 2018, 15, 151–166. [Google Scholar] [CrossRef]
- O’keefe, E.L.; Dhore-Patil, A.; Lavie, C.J. Early-Onset Cardiovascular Disease from Cocaine, Amphetamines, Alcohol, and Marijuana. Can. J. Cardiol. 2022, 38, 1342–1351. [Google Scholar] [CrossRef]
- Wolff, V.; Armspach, J.-P.; Beaujeux, R.; Manisor, M.; Rouyer, O.; Lauer, V.; Meyer, N.; Marescaux, C.; Geny, B. High Frequency of Intracranial Arterial Stenosis and Cannabis Use in Ischaemic Stroke in the Young. Cerebrovasc. Dis. 2014, 37, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Wolff, V.; Zinchenko, I.; Quenardelle, V.; Rouyer, O.; Geny, B. Characteristics and Prognosis of Ischemic Stroke in Young Cannabis Users Compared with Non-Cannabis Users. J. Am. Coll. Cardiol. 2015, 66, 2052–2053. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, T.; Sinor, A.D.; Simon, R.P.; Chen, J.; Graham, S.H.; Jin, K.; Greenberg, D.A. Cannabinoids and Neuroprotection in Global and Focal Cerebral Ischemia and in Neuronal Cultures. J. Neurosci. 1999, 19, 2987–2995. [Google Scholar] [CrossRef]
- Braida, D.; Pozzi, M.; Sala, M. CP 55,940 protects against ischemia-induced electroencephalographic flattening and hyperlocomotionin Mongolian gerbils. Neurosci. Lett. 2000, 296, 69–72. [Google Scholar] [CrossRef]
- Parmentier-Batteur, S.; Jin, K.; Mao, X.O.; Xie, L.; Greenberg, D.A. Increased Severity of Stroke in CB1 Cannabinoid Receptor Knock-Out Mice. J. Neurosci. 2002, 22, 9771–9775. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Piser, T.M.; Seybold, V.S.; Thayer, S.A. Cannabinoid Receptor Agonists Inhibit Glutamatergic Synaptic Transmission in Rat Hippocampal Cultures. J. Neurosci. 1996, 16, 4322–4334. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.H.; Azcoitia, I.; Pons, S.; Romero, J.; García-Segura, L.M.; Ramos, J.A.; Hansen, H.S.; Fernández-Ruiz, J. Blockade of cannabinoid CB1 receptor function protects against in vivo disseminating brain damage following NMDA-induced excitotoxicity. J. Neurochem. 2002, 82, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Amantea, D.; Spagnuolo, P.; Bari, M.; Fezza, F.; Mazzei, C.; Tassorelli, C.; Morrone, L.A.; Corasaniti, M.T.; Maccarrone, M.; Bagetta, G. Modulation of the endocannabinoid system by focal brain ischemia in the rat is involved in neuroprotection afforded by 17β-estradiol. FEBS J. 2007, 274, 4464–4775. [Google Scholar] [CrossRef] [PubMed]
- Reichenbach, Z.W.; Li, H.; Ward, S.J.; Tuma, R.F. The CB1 antagonist, SR141716A, is protective in permanent photothrombotic cerebral ischemia. Neurosci. Lett. 2016, 630, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Knowles, M.D.; de la Tremblaye, P.B.; Azogu, I.; Plamondon, H. Endocannabinoid CB1 receptor activation upon global ischemia adversely impact recovery of reward and stress signaling molecules, neuronal survival and behavioral impulsivity. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 66, 8–21. [Google Scholar] [CrossRef] [PubMed]
- James, S.P.; Bondugji, D. Gamma-Aminobutyric Acid (GABA) and the Endocannabinoids: Understanding the Risks and Opportunities. In Natural Drugs from Plants; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Xu, J.; Li, C.; Yin, X.-H.; Zhang, G.-Y. Additive neuroprotection of GABA A and GABA B receptor agonists in cerebral ischemic injury via PI-3K/Akt pathway inhibiting the ASK1-JNK cascade. Neuropharmacology 2008, 54, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Martin, B.R.; Adler, M.W.; Razdan, R.K.; Jallo, J.I.; Tuma, R.F. Cannabinoid CB2 Receptor Activation Decreases Cerebral Infarction in a Mouse Focal Ischemia/Reperfusion Model. J. Cereb. Blood Flow Metab. 2007, 27, 1387–1396. [Google Scholar] [CrossRef] [PubMed]
- Sultana, S.; Burkovskiy, I.; Zhou, J.; Kelly, M.M.; Lehmann, C. Effect of Cannabinoid 2 Receptor Modulation on the Peripheral Immune Response in Central Nervous System Injury-Induced Immunodeficiency Syndrome. Cannabis Cannabinoid Res. 2021, 6, 327–339. [Google Scholar] [CrossRef]
- Ronca, R.D.; Myers, A.M.; Ganea, D.; Tuma, R.F.; Walker, E.A.; Ward, S.J. A selective cannabinoid CB2 agonist attenuates damage and improves memory retention following stroke in mice. Life Sci. 2015, 138, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Bietar, B.; Zhou, J.; Lehmann, C. Utility of intestinal intravital microscopy for the study of CNS injury-induced immunodepression syndrome (CIDS). Clin. Hemorheol. Microcirc. 2021, 79, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Burkovskiy, I.; Zhou, J.; Lehmann, C. Experimental Cannabinoid 2 Receptor Inhibition in CNS Injury-Induced Immunodeficiency Syndrome. Microcirculation 2016, 23, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Hillard, C.J. Role of Cannabinoids and Endocannabinoids in Cerebral Ischemia. Curr. Pharm. Des. 2008, 14, 2347–2361. [Google Scholar] [CrossRef]
- Ward, S.J.; Castelli, F.; Reichenbach, Z.W.; Tuma, R.F. Surprising outcomes in cannabinoid CB1/CB2 receptor double knockout mice in two models of ischemia. Life Sci. 2018, 195, 1–5. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Vasculature | Clotting/Thrombosis |
|---|---|
| Reversible cerebral vasoconstriction syndrome | Intracranial arterial stenosis |
| Vasospasm, vasoconstriction | Atherosclerosis |
| Arterial blood flow alterations | Platelet aggregation |
| Mechanism | Compound | Model | Outcome | Reference |
|---|---|---|---|---|
| CB1/2 Agonist | WIN55,212-2 | CCAO & MCAO | Reduced infarct volume | [63] |
| CB1 Agonist | CP5590 | CCAO | Protective effect against motor activity damage | [64] |
| CB1 Antagonist | SR141716A | NDMA | Reduced infarct volume | [67] |
| CB1 Antagonist | SR141716A | MCAO | Reduced infarct volume | [68] |
| CB1 Antagonist | SR141716A | Photothrombotic | Reduced infarct volume | [69] |
| CB1 Antagonist | AM251 | Global Ischemia | [70] | |
| CB2 Agonist | O-1966, O-3853 | MCAO | Reduced infarct volume and improved motor function | [73] |
| CB2 Agonist | O-1966 | Photoinjury | Reduced infarct volume and protection against cognitive deficits | [75] |
| CB2 Agonist | AM1241 | Global Ischemia (4VO) | Reduced infarct volume and a decrease in neurological deficits | [35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carter, C.; Laviolette, L.; Bietar, B.; Zhou, J.; Lehmann, C. Cannabis, Cannabinoids, and Stroke: Increased Risk or Potential for Protection—A Narrative Review. Curr. Issues Mol. Biol. 2024, 46, 3122-3133. https://doi.org/10.3390/cimb46040196
Carter C, Laviolette L, Bietar B, Zhou J, Lehmann C. Cannabis, Cannabinoids, and Stroke: Increased Risk or Potential for Protection—A Narrative Review. Current Issues in Molecular Biology. 2024; 46(4):3122-3133. https://doi.org/10.3390/cimb46040196
Chicago/Turabian StyleCarter, Caroline, Lindsay Laviolette, Bashir Bietar, Juan Zhou, and Christian Lehmann. 2024. "Cannabis, Cannabinoids, and Stroke: Increased Risk or Potential for Protection—A Narrative Review" Current Issues in Molecular Biology 46, no. 4: 3122-3133. https://doi.org/10.3390/cimb46040196
APA StyleCarter, C., Laviolette, L., Bietar, B., Zhou, J., & Lehmann, C. (2024). Cannabis, Cannabinoids, and Stroke: Increased Risk or Potential for Protection—A Narrative Review. Current Issues in Molecular Biology, 46(4), 3122-3133. https://doi.org/10.3390/cimb46040196