
Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome



Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DDX3X | DEAD-Box Helicase 3 X-Linked |
| IDD | Intellectual and developmental disabilities |
| DSM-V | Diagnostic and Statistical Manual of Mental Disorders |
| WES | Whole exome sequencing |
| MRI | Magnetic resonance imaging |
| PWS/AS MLPA | Multiplex ligation-dependent probe amplification |
| EEG | Electroencephalogram |
| aCGH | Array-Comparative Genomic Hybridization |
| ASD | Autism Spectrum Disorder |
| SI | Sensory Integration |
| ICF-CY | International Classification of Functioning, Disability and Health for Children and Youth |
| VUS | Variant of Uncertain Significance |
References
- Mo, J.; Liang, H.; Su, C.; Li, P.; Chen, J.; Zhang, B. DDX3X: Structure, Physiologic Functions and Cancer. Mol. Cancer 2021, 20, 38. [Google Scholar] [CrossRef] [PubMed]
- Phung, B.; Cieśla, M.; Sanna, A.; Guzzi, N.; Beneventi, G.; Cao Thi Ngoc, P.; Lauss, M.; Cabrita, R.; Cordero, E.; Bosch, A.; et al. The X-Linked DDX3X RNA Helicase Dictates Translation Reprogramming and Metastasis in Melanoma. Cell Rep. 2019, 27, 3573–3586.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkataramanan, S.; Gadek, M.; Calviello, L.; Wilkins, K.; Floor, S.N. DDX3X and DDX3Y Are Redundant in Protein Synthesis. RNA 2021, 27, 1577–1588. [Google Scholar] [CrossRef] [PubMed]
- Afif, I.Y.; Farkhan, M.; Kurdi, O.; Maula, M.I.; Ammarullah, M.I.; Setiyana, B.; Jamari, J.; Winarni, T.I. Effect of Short-Term Deep-Pressure Portable Seat on Behavioral and Biological Stress in Children with Autism Spectrum Disorders: A Pilot Study. Bioengineering 2022, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Maula, M.I.; Aji, A.L.; Aliyafi, M.B.; Afif, I.Y.; Ammarullah, M.I.; Winarni, T.I.; Jamari, J. The Subjective Comfort Test of Autism Hug Machine Portable Seat. J. Intellect. Disabil.-Diagn. Treat. 2021, 9, 182–188. [Google Scholar] [CrossRef]
- DDX3X Foundation. Available online: http://ddx3x.org/ (accessed on 9 December 2021).
- Blok, L.S.; Madsen, E.; Juusola, J.; Gilissen, C.; Baralle, D.; Reijnders, M.R.F.; Venselaar, H.; Helsmoortel, C.; Cho, M.T.; Hoischen, A.; et al. Mutations in DDX3X are a common cause of unexplained intellectual disability with gender-specific effects on Wnt signaling. Am. J. Hum. Genet. 2015, 97, P343–P352. [Google Scholar] [CrossRef] [Green Version]
- Moresco, G.; Costanza, J.; Santianiello, C.; Rondinone, O.; Grilli, F.; Prada, E.; Prcesi, S.; Coro, I.; Pichiecchio, A.; Marchisio, P.; et al. A novel de novo DDX3X missense variant in a female with brachycephaly and intellectual disability: A case report. Ital. J. Pediatr. 2021, 47, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nicola, P.; Blackburn, P.R.; Rasmussen, K.J.; Bertsch, N.L.; Klee, E.W.; Hasadsri, L.; Pichurin, P.N.; Rankin, J.; Raymond, F.L.; Study, D.D.D.; et al. De novo DDX3X missense variants in males appear viable and contribute to syndromic intellectual disability. Am. J. Med. Genet. Part A 2019, 179, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Garbelli, A.; Beermann, S.; Di Cicco, G.; Dietrich, U.; Maga, G. A motif unique to the human dead-box protein DDX3X is important for nucleic acid binding, ATP hydrolysis, RNA/DNA unwinding and HIV-1 replication. PLoS ONE 2011, 6, e19810. [Google Scholar] [CrossRef] [PubMed]
- Kobylińska, M.; Malak, R.; Majewska, K.; Kędzia, A.; Samborski, W. Assessment of anterior-posterior spinal curvatures in children suffering from hypopituitarism. BMC Endocr. Disord. 2019, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blueprint Genetics. Available online: https://blueprintgenetics.com/variant-classification/ (accessed on 3 March 2022).
- Zimmer, M.; Desh, L.; Rosen, L.D.; Bailey, M.L.; Becker, D.; Culbert, T.P.; McClafferty, H.; Sahler, O.J.Z.; Vohra, S.; Liptak, G.S.; et al. Sensory integration therapies for children with developmental and behavioral disorders. Pediatrics 2012, 129, 1186–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smirni, D.; Smirni, P.; Carotenuto, M.; Parisi, L.; Quatrosi, G.; Roccella, M. Noli Me Tangere: Social Touch, Tactile Defensiveness, and Communication in Neurodevelopmental Disorders. Brain Sci. 2019, 9, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgolte, A.; Roy, M.; Sinke, C.; Wiswede, D.; Stephan, M.; Bleich, S.; Münte, T.F.; Szycik, G.R. Enhanced attentional processing during speech perception in adult high-functioning autism spectrum disorder: An ERP-study. Neuropsychologia 2021, 161, 108022. [Google Scholar] [CrossRef] [PubMed]
- Sparrow, S.S.; Saulnier, C.A.; Cicchetti, D.V.; Doll, E.A. Vineland-3: Vineland AdaptiveBbehavior Scales. 2016. Available online: https://www.worldcat.org/title/vineland-3-vineland-adaptive-behavior-scales-manual/oclc/228032603 (accessed on 2 November 2021).
- Johnson-Kerner, B.; Snijders Blok, L.; Suit, L.; Thomas, J.; Kleefstra, T.; Sherr, E.H. DDX3X-Related Neurodevelopmental Disorder. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Mirzaa, G.M., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Signs in the Presented Case | DDX3X Syndrome Clinical Signs |
|---|---|
| Development | |
| yes | Developmental delay |
| no | Intellectual disability |
| yes | Speech delay |
| Growth | |
| no | Failure to thrive |
| no | Short stature |
| no | Microcephaly |
| yes | Brachycephaly |
| Neurologic/behavioral | |
| no | Seizures |
| no | Hypotonia |
| no | Hypertonia/spasticity |
| no | Mixed hypo and hypertonia |
| yes | Sleep disturbance |
| no | Movement disorders/leg spasticity |
| yes | Behavior disorders/autism spectrum disorder/aggression |
| no | Hyperreflexia |
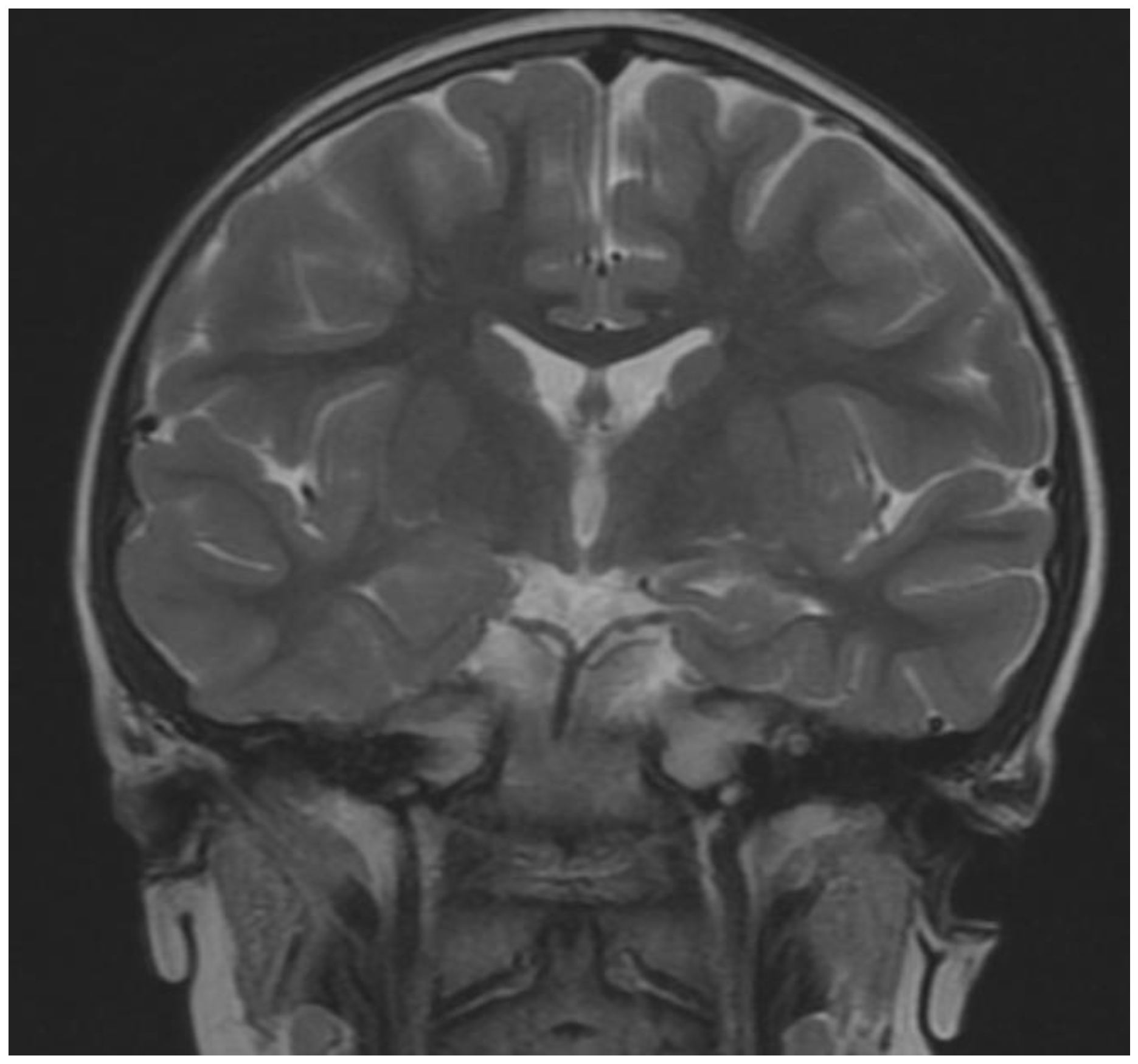
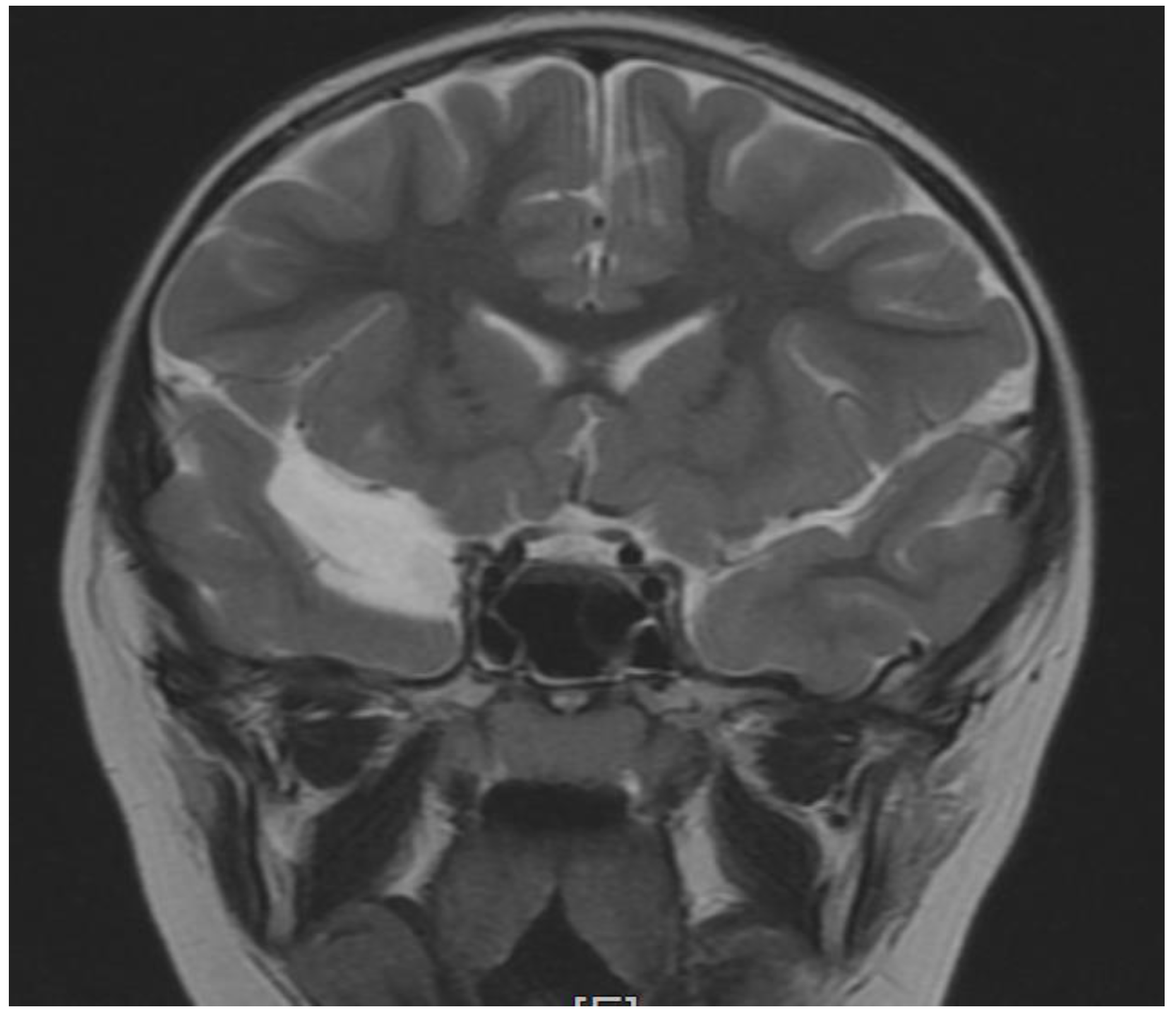
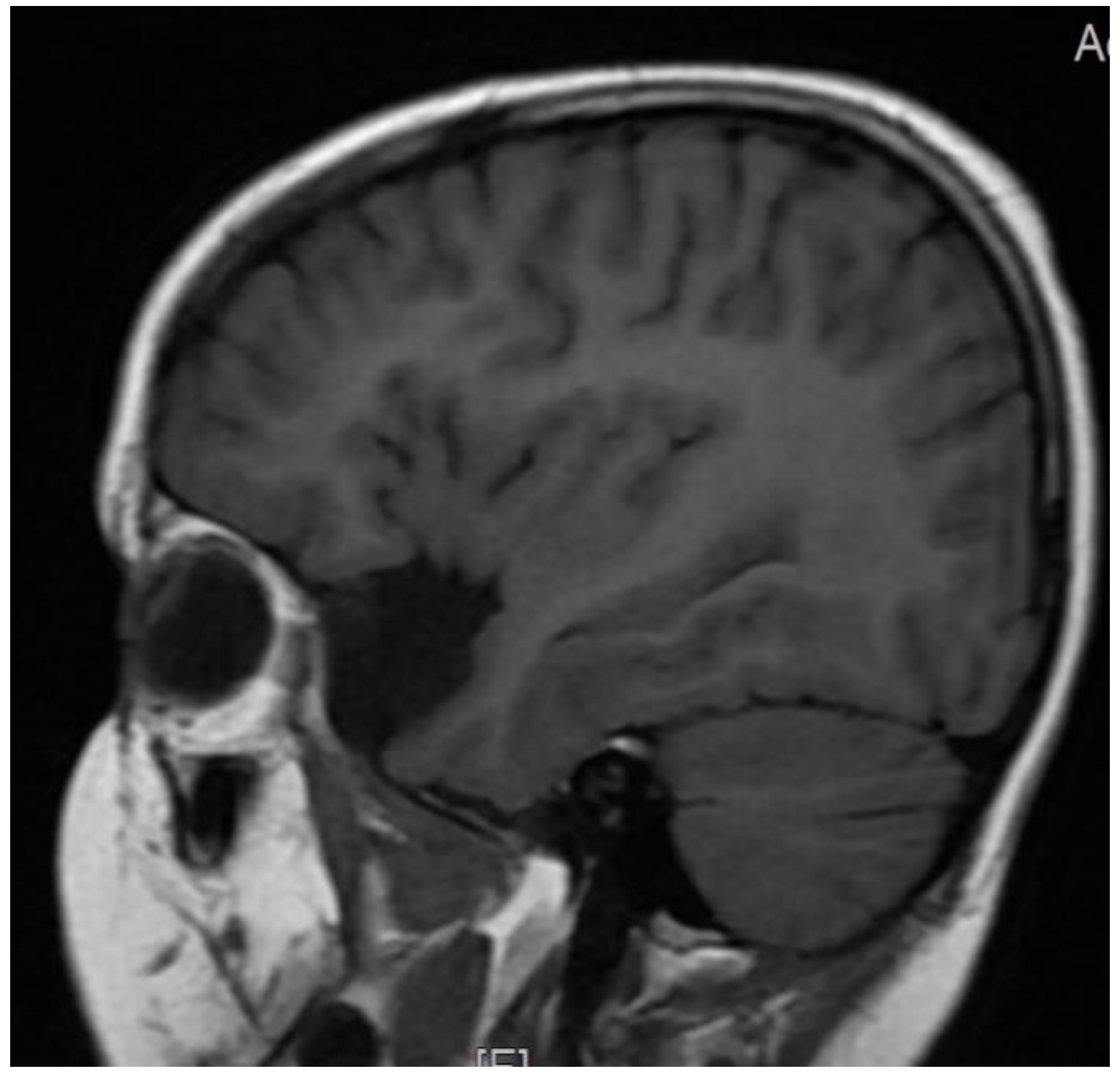
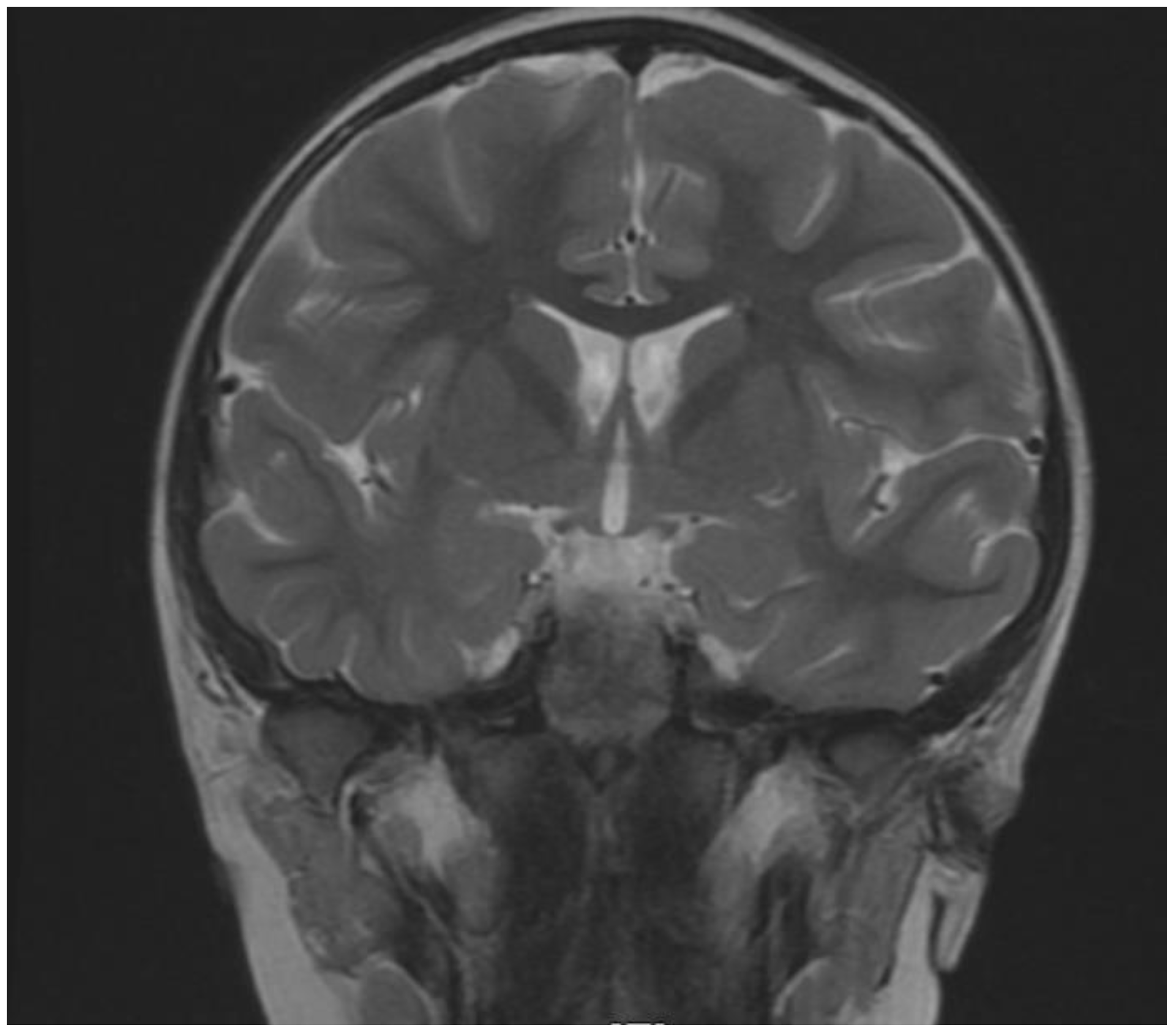
| Brain MRI | |
| no | Polymicrogyria |
| no | Corpus callosum hypoplasia/agenesis |
| no | Ventricular enlargement |
| no | Key-hole shaped temporal horns |
| no | Colpocephaly |
| no | Delayed myelination/decreased cortical white |
| no | Small pons |
| no | Small interior vermis |
| yes | Changes in temporal lobe- cyst |
| Sensory | |
| no | Vision problems (strabismus, coloboma, astigmatism, nystagmus) |
| no | Hearing problems |
| yes | High pain threshold |
| yes | Temperature dysregulation |
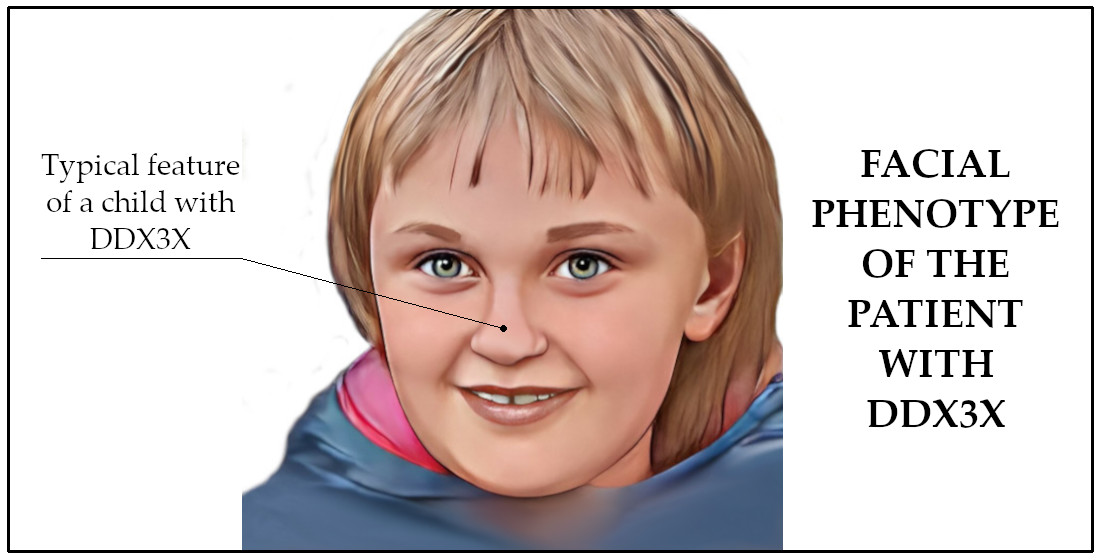
| Facial dysmorphism | |
| no | Short/down-slanting palpebral fissure |
| no | Hypertelorism/telecanthus |
| no | Epicanthal folds |
| flattened face | Elongated/flattened face/triangular face |
| high forehead | High/broad forehead |
| No | Wide nasal bridge/bulbous tip |
| narrow nose | Short/narrow nose, anteverted nares |
| no | Micrognathia |
| no | High arched palate |
| no | Thin upper lip |
| no | Low set/protruding/wide ears |
| no | Smooth/long philtrum |
| no | Cleft lip/palate |
| no | Macroglossia |
| Other | |
| no | Congenital cardiac defects |
| not applicable | Precocious puberty |
| no | Feeding difficulties (gastro-esophageal reflux/swallowing) |
| no | Joint hyperlaxity |
| yes | Scoliosis/asymmetry in the spine |
| no | Malformations of the hands |
| no | Skin pigmentation anomalies |
| no | Loss/reduced subcutaneous fat |
| Yes | Higher Inflammatory cytokine profile |
| yes | IL-1β |
| yes | IL-6 |
| yes | IL-10 |
| Gene | Pos | Transcript | Nomenclature | Consequence | Genotype | Classification |
|---|---|---|---|---|---|---|
| HSD17B4 | 5:118788281 | NM_000414.4 | c.11C>G, p(Pro4Arg) | missense_variant | HET | Variant of uncertain significance |
| ID | GNOMAD | POLYPHEN | SIFT | MUTTASTER | ||
| rs142889209 | 52/282304 | benign | tolerated | polymorphism | ||
| OMIM | PHENOTYPE | INHERITANCE | COMMENT | |||
| D-bifunctional protein deficiency, | AR | |||||
| Perrault Syndrome | ||||||
| GENE | POS | TRANSCRIPT | NOMENCLATURE | CONSEQUENCE | GENOTYPE | CLASSIFICATION |
| HSD17B4 | 5:118813169 | NM_001199291.3 | c.482A>G, (Glu161Gly) | missense_variant | HET | Variant of uncertain significance |
| ID | GNOMAD | POLYPHEN | SIFT | MUTTASTER | ||
| 0/0 | Benign | tolerated | disease causing | |||
| OMIM | PHENOTYPE | INHERITANCE | COMMENT | |||
| D-bifunctional protein deficiency, Perrault Syndrome | AR | |||||
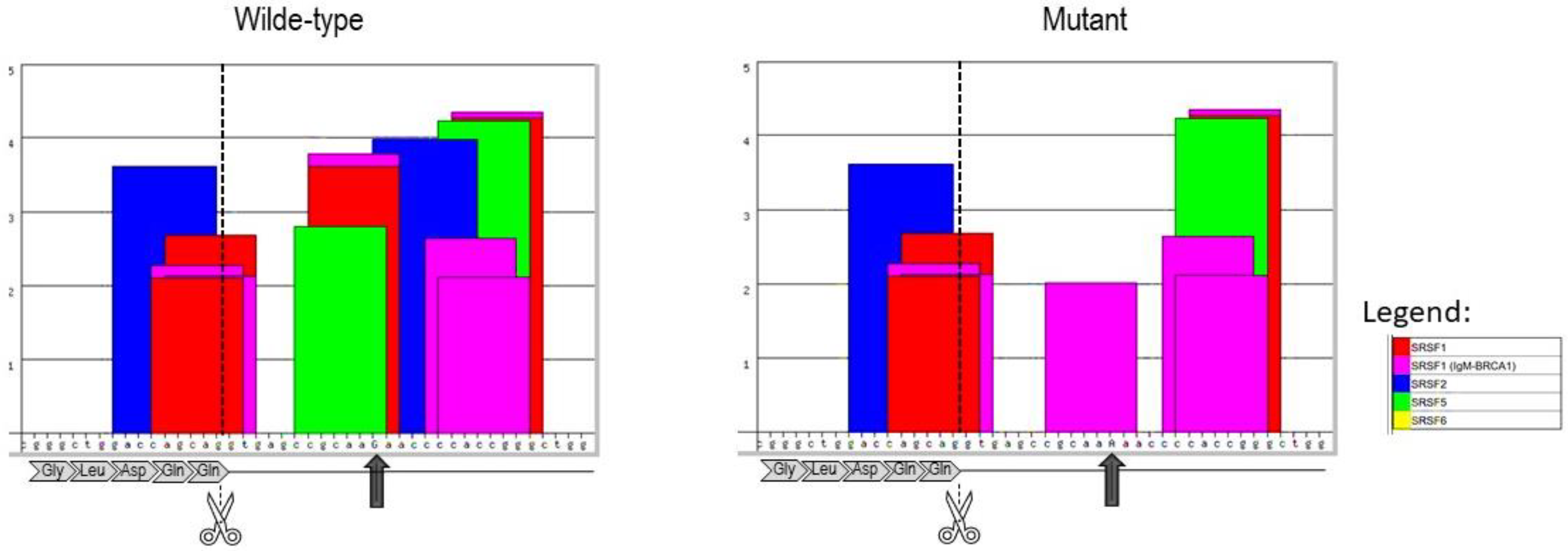
| GENE | POS | TRANSCRIPT | NOMENCLATURE | CONSEQUENCE | GENOTYPE | CLASSIFICATION |
| DDX3X | X:41193562 | NM_001356.4 | c.45+12G>A | intron_variant | HET | Variant of uncertain significance |
| ID | GNOMAD | POLYPHEN | SIFT | MUTTASTER | ||
| 0/175946 | N/A | N/A | N/A | |||
| OMIM | PHENOTYPE | INHERITANCE | COMMENT | |||
| Mental retardation, X-linked 102 | X-linked |
| Adaptive Level | Age Equivalent | V-Scale Score/Standard Score | Raw Score | Domain |
|---|---|---|---|---|
| Low | N/A | 27 | N/A | Communication |
| Low | 1:01 | 1 | 26 | Receptive |
| Low | 0:11 | 1 | 16 | Expressive |
| Low | <3:0 | 4 | 4 | Written |
| Low | N/A | 57 | N/A | Daily Living Skills |
| Low | 3:00 | 9 | 60 | Personal |
| Low | <3:0 | 6 | 0 | Domestic |
| Low | <3:0 | 6 | 6 | Community |
| Low | N/A | 46 | N/A | Socialization |
| Low | 0:09 | 6 | 25 | Interpersonal Relationships |
| Low | 0:09 | 5 | 12 | Play and Leisure |
| Low | <2:0 | 5 | 6 | Coping Skills |
| Moderately Low | N/A | 74 | N/A | Motor |
| Moderately Low | 5:00 | 13 | 81 | Gross Motor Skills |
| Low | 2:11 | 8 | 37 | Fine Motor Skills |
| Low | N/A | 49 | N/A | Adaptive Behavior Composite |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefaniak, U.; Malak, R.; Mojs, E.; Samborski, W. Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome. Brain Sci. 2022, 12, 390. https://doi.org/10.3390/brainsci12030390
Stefaniak U, Malak R, Mojs E, Samborski W. Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome. Brain Sciences. 2022; 12(3):390. https://doi.org/10.3390/brainsci12030390
Chicago/Turabian StyleStefaniak, Urszula, Roksana Malak, Ewa Mojs, and Włodzimierz Samborski. 2022. "Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome" Brain Sciences 12, no. 3: 390. https://doi.org/10.3390/brainsci12030390
APA StyleStefaniak, U., Malak, R., Mojs, E., & Samborski, W. (2022). Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome. Brain Sciences, 12(3), 390. https://doi.org/10.3390/brainsci12030390