
Mental Health Screening Approaches for Resettling Refugees and Asylum Seekers: A Scoping Review

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Research Objectives
- ➢
- In what setting(s) has refugee mental health screening been conducted?
- ➢
- At what point in time during the migration pathway is screening conducted and for what purpose?
- ➢
- What tools have been used in the refugee population, and what conditions do they screen for?
- ➢
- In which language(s) and formats are mental health assessments delivered?
- ➢
- Have any of these tools been adapted, validated, or evaluated specifically for use among refugees?
- ➢
- What approaches are used to screen vulnerable subgroups?
- ➢
- What are the professional characteristics and training of individuals who administer mental health assessments?
- ➢
- What are the lessons learned from pilots/approaches that have been tried on the ground?
3. Methods
4. Eligibility Criteria
5. Search Methods
6. Screening and Selection
7. Data Extraction and Management
8. Synthesis of Results
9. Results
10. Characteristics of Included Studies
11. Conditions and Mental Health Screening Tools
12. Pre-Departure Mental Health Screening
13. Mental Health Screening for Survivors of Torture
14. Mental Health Screening Approaches for Refugee Women
15. Mental Health Screening Approaches for Refugee Children and Adolescents
16. Mental Health Screening Tool Validation Studies
17. Discussion
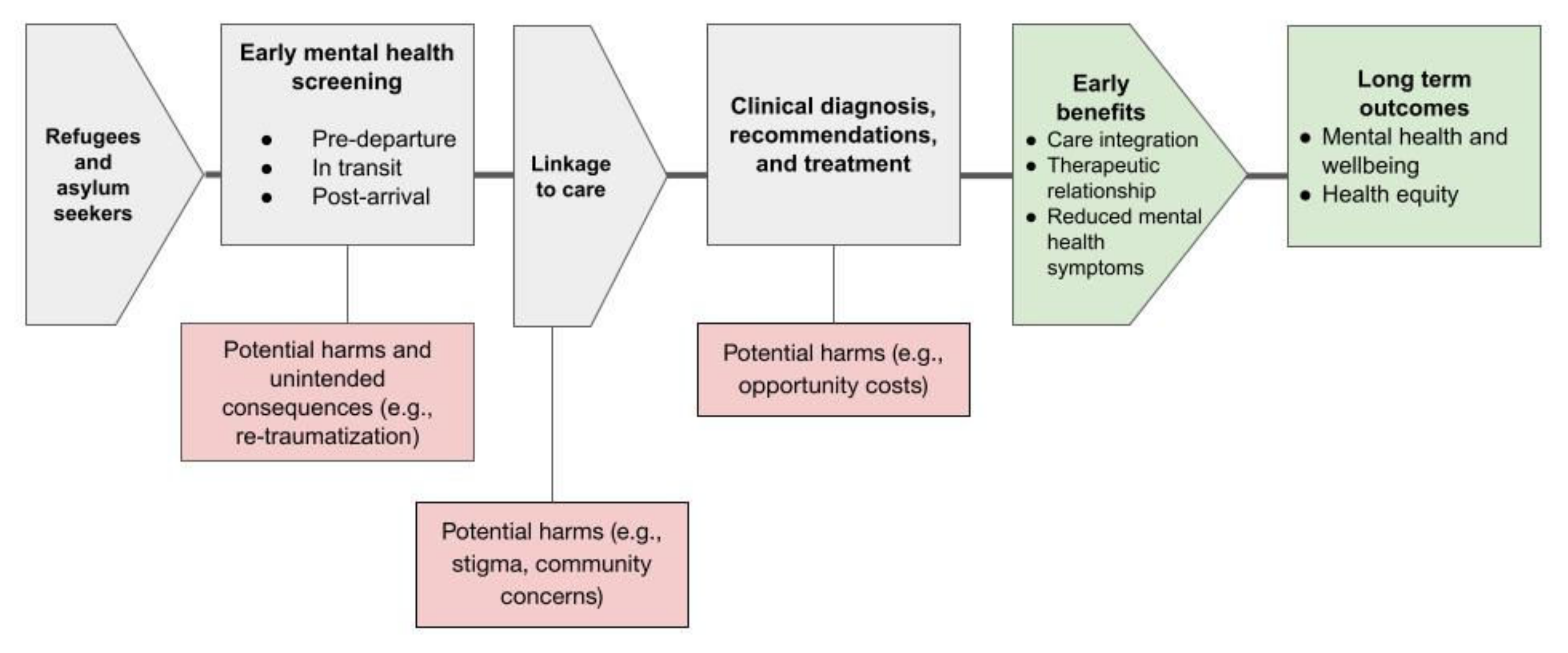
- Who administers mental health screening?Most mental health assessments are administered by a trained health professional with various levels of mental health expertise. This includes general practitioners, nurses, psychiatrists, psychologists, and community health workers. However, some tools can be self-administered (for example, the Refugee Health Screener) and completed on paper or using digital technology such as a tablet or computer. We identified a few mental health screening tools (PROTECT Questionnaire; STAR-MH; Refugee Health Screener) administered by staff without medical or psychological health training. Regardless of who administers the mental health assessment, numerous studies highlighted the importance of a trained interpreter or translator to assist in the assessment and prevent misinterpretations and miscommunications. Authors suggest the presence of trained interpreters improved the quality of communication and also served as cultural mediators [56].Which mental health screening tool should be administered?There is no international consensus regarding the most effective mental health screening tool to be applied in the context of resettlement. While several tools are gaining popularity (for example, the Harvard Trauma Questionnaire or the Refugee Health Screener), there is currently insufficient effective research to guide the selection of mental health screening tools for national level programs. Currently, tools are chosen to reflect the cultural sensitivity and geographical diversity of refugee groups, but as migration patterns change rapidly, it is difficult to specify a singular set of tools that can be applicable to a large array of refugee populations [53]. It is well recognized that Western diagnostic classifications of mental health conditions have significant limitations with refugee populations because of variations in causality, sociocultural context, and symptom manifestation [6,66]. Authors agree that there is a need for culturally appropriate validated tools to detect mental health problems in refugees [48]. According to Poole et al. screening tools should be (1) self-reported or administered by trained non-medical health workers; (2) responsive to change; with (3) a demonstrated acceptable response rate, reliability, and validity in displaced populations; and (4) a minimal response burden [86].When should mental health screening take place?Despite the existence of country-level guidance for pre-migration mental health screening (for example, from the USA [109], Australia [61], or New Zealand [110]), there are very few published reports evaluating these processes. The published literature shows that most assessments occur post-arrival to the resettlement state. Post-arrival programs can leverage community partnerships (e.g., [69]) and medical home models (e.g., [45]) to ensure efficient and appropriate linkages to care. Some studies noted the difficulty of following up with refugees as they often get transferred from one location to another in the first few months post-arrival [89,94]. Further, one Australian study reported challenges with the information transfer between and within pre-migration and post-arrival health systems, causing duplication of avoidable tests, increased costs, inefficiencies, and possible clinical consequences [61]. Evidence from the UK also identified critical operational issues with the information flow and supports the notion that further evaluation of pre-departure screening is warranted prior to widespread implementation [39]. To date, there is neither consensus nor sufficient program research to identify the optimal time to screen and assess the mental health needs of refugees and asylum seekers.Where does mental health screening take place?The majority of mental health screening takes place in a primary care community setting, including refugee specific clinics or services where professionals were trained and familiar with the caseload. Buchwald et al. proposed that individuals presenting to primary care have come for help and accepted the “patient” role; therefore, psychiatric case finding and offering treatment may be less intrusive than it would be in other settings [49]. Furthermore, because this setting is not defined as “psychiatric,” the stigma associated with mental health treatment may be more easily minimized [6,49]. One study reported a high rate of refusal during a clinic-based post-arrival health assessment and found that mental health screening was more effective when conducted during a home visit [40].Do screening programs facilitate linkages to care?Post-arrival screening programs usually include a linkage to care, either on-site or through referrals to community organizations or further specialized care. Programs which operate a medical home model can offer direct multidisciplinary care with allied health professionals and interpreters [45]. The evidence on pre-departure screening is less conclusive: while this information could function as an “early warning” to help local authorities prepare for individuals needing additional support, the impact of the screening is likely to be limited by resource availability and access to specialist mental health services [39]. Existing community resources may not be appropriate for the specific mental health needs of refugees who have fled conflict or experienced violence, torture, or trauma. However, as these pre-departure reports provide valuable information which is usually not available on arrival or takes time and trust to elicit from a patient, pre-departure mental health screening may help primary care providers save time and take appropriate action more proactively, thereby expediting the referral and provision of care [39].How can mental health screening be implemented?Several studies highlighted that funding for mental health screening and care programs is essential [41,45,102]. Although many factors affect program success, the loss of program funds has been identified as the primary factor contributing to staff reductions and implementation failure [49]. Further, basic training about the context and important health issues of resettled refugees and administration procedures is necessary for all clinical and non-clinical staff [43]. Processes should be streamlined to reduce the time required to complete the assessment [39,43]. National training programs can provide technical assistance and support culturally relevant behaviours, attitudes, and policies in clinical practice [41,106], and help address mental health stigma [66]. Finally, the results from two studies suggest that sequential screening (i.e., categorizing refugees by level of risk to inform linkage to care) is a pragmatic strategy that can reduce the response burden and facilitate the detection of mental health conditions in settings with a scarcity of mental health specialists [80,86].
18. Implications for Policy
19. Implications for Practice
20. Implications for Research
21. Strengths and Limitations
22. Deviations from Protocol
23. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations High Commissioner for Refugees (UNHCR). Projected Global Resettlement Needs 2020; UNHCR: Geneva, Switzerland, 2019. [Google Scholar]
- Brickhill-Atkinson, M.; Hauck, F.R. Impact of COVID-19 on Resettled Refugees. Prim. Care 2021, 48, 57–66. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Projected Global Resettlement Needs 2022; 27th Annual Tripartite Consultations on Resettlement; UNHCR: Geneva, Switzerland, 2021. [Google Scholar]
- International Organization for Migration (IOM). Migration Health Assessments and Travel Health Assistance: 2019 Overview of Pre-Migration Health Activities; IOM: Geneva, Switzerland, 2020. [Google Scholar]
- United Nations High Commissioner for Refugees The Global Report 2005. Available online: https://www.unhcr.org/publications/fundraising/4a0c04f96/global-report-2005.html (accessed on 27 February 2022).
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. Can. Med. Assoc. J. 2011, 183, E959–E967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamen, J.; Girard, V.; Jamani, S.; Magwood, O.; Holland, T.; Sharfuddin, N.; Pottie, K. Access to Refugee and Migrant Mental Health Care Services during the First Six Months of the COVID-19 Pandemic: A Canadian Refugee Clinician Survey. Int. J. Environ. Res. Public Health 2021, 18, 5266. [Google Scholar] [CrossRef] [PubMed]
- Beiser, M. The Health of Immigrants and Refugees in Canada. Can. J. Public Health 2005, 96, S30–S44. [Google Scholar] [CrossRef]
- Sveaass, N.; Lie, B. Early Assessment of Mental Health and Options for Documentation of Torture in Newly Arrived Asylum Seekers; Oxford University Press: Oxford, UK, 2021; pp. 387–394. ISBN 978-0-19-883374-1. [Google Scholar]
- Kronick, R. Mental Health of Refugees and Asylum Seekers: Assessment and Intervention. Can. J. Psychiatry 2018, 63, 290–296. [Google Scholar] [CrossRef]
- Andermann, L.; Kanagaratnam, P.; Wondimagegn, D.; Pain, C. Post-Traumatic Stress Disorder in Refugee and Migrant Mental Health; Oxford University Press: Oxford, UK, 2021; ISBN 978-0-19-187215-0. [Google Scholar]
- World Health Organization. Health of Refugees and Migrants; WHO: Geneva, Switzerland, 2018; p. 37. [Google Scholar]
- Kassam, A.; Magwood, O.; Pottie, K. Fostering Refugee and Other Migrant Resilience through Empowerment, Pluralism, and Collaboration in Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 9557. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Pedersen, D. Toward a new architecture for global mental health. Transcult. Psychiatry 2014, 51, 759–776. [Google Scholar] [CrossRef]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; van Ommeren, M. Association of Torture and other Potentially Traumatic Events with Mental Health Outcomes among Populations Exposed to Mass Conflict and Displacement: A Systematic Review and Meta-analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef]
- Charlson, F.J.; Flaxman, A.; Ferrari, A.J.; Vos, T.; Steel, Z.; Whiteford, H.A. Post-traumatic stress disorder and major depression in conflict-affected populations: An epidemiological model and predictor analysis. Glob. Ment. Health 2016, 3, e4. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Depression and other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Stein, D.J.; McLaughlin, K.A.; Koenen, K.C.; Atwoli, L.; Friedman, M.J.; Hill, E.D.; Maercker, A.; Petukhova, M.; Shahly, V.; van Ommeren, M.; et al. DSM-5 and ICD-11 definitions of posttraumatic stress disorder: Investigating “narrow” and “broad” approaches. Depress. Anxiety 2014, 31, 494–505. [Google Scholar] [CrossRef]
- Wickramage, K.; Mosca, D. Can Migration Health Assessments Become a Mechanism for Global Public Health Good? Int. J. Environ. Res. Public Health 2014, 11, 9954–9963. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, T.; Weinberg, M.; Posey, D.L.; Cetron, M. Immigrant and Refugee Health: A Centers for Disease Control and Prevention Perspective on Protecting the Health and Health Security of Individuals and Communities During Planned Migrations. Pediatr. Clin. North. Am. 2019, 66, 549–560. [Google Scholar] [CrossRef]
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; MacDonald, N.E.; et al. Evidence-based clinical guidelines for immigrants and refugees. Can. Med. Assoc. J. 2011, 183, E824–E925. [Google Scholar] [CrossRef] [Green Version]
- Ali, G.-C.; Ryan, G.; De Silva, M.J. Validated Screening Tools for Common Mental Disorders in Low and Middle Income Countries: A Systematic Review. PLoS ONE 2016, 11, e0156939. [Google Scholar] [CrossRef]
- Amiri, S. Prevalence of Suicide in Immigrants/Refugees: A Systematic Review and Meta-Analysis. Arch. Suicide Res. 2020, 1–36. [Google Scholar] [CrossRef]
- Morina, N.; Akhtar, A.; Barth, J.; Schnyder, U. Psychiatric Disorders in Refugees and Internally Displaced Persons After Forced Displacement: A Systematic Review. Front. Psychiatry 2018, 9, 433. [Google Scholar] [CrossRef]
- Blackmore, R.; Boyle, J.A.; Fazel, M.; Ranasinha, S.; Gray, K.M.; Fitzgerald, G.; Misso, M.; Gibson-Helm, M. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003337. [Google Scholar] [CrossRef]
- Due, C.; Green, E.; Ziersch, A. Psychological trauma and access to primary healthcare for people from refugee and asylum-seeker backgrounds: A mixed methods systematic review. Int. J. Ment. Health Syst. 2020, 14, 71. [Google Scholar] [CrossRef]
- Satinsky, E.; Fuhr, D.; Woodward, A.; Sondorp, E.; Roberts, B. Mental health care utilisation and access among refugees and asylum seekers in Europe: A systematic review. Health Policy 2019, 123, 851–863. [Google Scholar] [CrossRef]
- Hassan, A.; Sharif, K. Efficacy of Telepsychiatry in Refugee Populations: A Systematic Review of the Evidence. Cureus 2019, 11, e3984. [Google Scholar] [CrossRef] [Green Version]
- Gruner, D.; Magwood, O.; Bair, L.; Duff, L.; Adel, S.; Pottie, K. Understanding Supporting and Hindering Factors in Community-Based Psychotherapy for Refugees: A Realist-Informed Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4618. [Google Scholar] [CrossRef]
- Lu, J.; Jamani, S.; Benjamen, J.; Agbata, E.; Magwood, O.; Pottie, K. Global Mental Health and Services for Migrants in Primary Care Settings in High-Income Countries: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 8627. [Google Scholar] [CrossRef] [PubMed]
- Gadeberg, A.K.; Montgomery, E.; Frederiksen, H.W.; Norredam, M. Assessing trauma and mental health in refugee children and youth: A systematic review of validated screening and measurement tools. Eur. J. Public Health 2017, 27, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Hollifield, M.; Warner, T.D.; Lian, N.; Krakow, B.; Jenkins, J.H.; Kesler, J.; Stevenson, J.; Westermeyer, J. Measuring Trauma and Health Status in RefugeesA Critical Review. JAMA 2002, 288, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Davidson, G.R.; Murray, K.E.; Schweitzer, R.D. Review of Refugee Mental Health Assessment: Best Practices and Recommendations. J. Pac. Rim Psychol. 2010, 4, 72–85. [Google Scholar] [CrossRef]
- Magwood, O.; Muharram, H.; Saad, A.; Mavedatnia, D.; Madana, M.; Agbata, E.; Pottie, K. Mental Health Screening Approaches for Refugees and Asylum Seekers: A Protocol for a Scoping Review; Bruyère Research Institute: Ottawa, ON, Canada, 2021; p. 10. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; Blunt, H.; Brigham, T.; Chang, S.; et al. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- United Nations High Commissioner for Refugees UNHCR Resettlement Handbook and Country Chapters. Available online: https://www.unhcr.org/protection/resettlement/4a2ccf4c6/unhcr-resettlement-handbook-country-chapters.html (accessed on 27 February 2022).
- Veritas Health Innovation. Covidence Systematic Review Software. Available online: https://www.covidence.org/ (accessed on 7 March 2022).
- Hough, C.; O’Neill, E.; Dyer, F.; Beaney, K.; Crawshaw, A. The Global Mental Health Assessment Tool (GMHAT) Pilot Evaluation: Final Report; Public Health England: London, UK, 2019; p. 80. [Google Scholar]
- Barnes, D.M. Mental Health Screening in a Refugee Population: A Program Report. J. Immigr. Health 2001, 3, 141–149. [Google Scholar] [CrossRef]
- Al-Obaidi, A.; West, B.; Fox, A.; Savin, D. Incorporating Preliminary Mental Health Assessment in the Initial Healthcare for Refugees in New Jersey. Community Ment. Health J. 2015, 51, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Arnetz, B.B.; Broadbridge, C.L.; Jamil, H.; Lumley, M.A.; Pole, N.; Barkho, E.; Fakhouri, M.; Talia, Y.R.; Arnetz, J.E. Specific Trauma Subtypes Improve the Predictive Validity of the Harvard Trauma Questionnaire in Iraqi Refugees. J. Immigr. Minority Health 2014, 16, 1055–1061. [Google Scholar] [CrossRef] [Green Version]
- Baird, M.B.; Cates, R.; Bott, M.J.; Buller, C. Assessing the Mental Health of Refugees Using the Refugee Health Screener-15. West J. Nurs. Res. 2020, 42, 910–917. [Google Scholar] [CrossRef]
- Barbieri, A.; Visco-Comandini, F.; Alunni Fegatelli, D.; Schepisi, C.; Russo, V.; Calò, F.; Dessì, A.; Cannella, G.; Stellacci, A. Complex trauma, PTSD and complex PTSD in African refugees. Eur. J. Psychotraumatol. 2019, 10, 1700621. [Google Scholar] [CrossRef] [Green Version]
- Bertelsen, N.S.; Selden, E.; Krass, P.; Keatley, E.S.; Keller, A. Primary Care Screening Methods and Outcomes for Asylum Seekers in New York City. J. Immigr. Minority Health 2018, 20, 171–177. [Google Scholar] [CrossRef]
- Bjarta, A.; Leiler, A.; Ekdahl, J.; Wasteson, E. Assessing Severity of Psychological Distress Among Refugees With the Refugee Health Screener, 13-Item Version. J. Nerv. Ment. Dis. 2018, 206, 834–839. [Google Scholar] [CrossRef] [Green Version]
- Boyle, J.A.; Willey, S.; Blackmore, R.; East, C.; McBride, J.; Gray, K.; Melvin, G.; Fradkin, R.; Ball, N.; Highet, N.; et al. Improving Mental Health in Pregnancy for Refugee Women: Protocol for the Implementation and Evaluation of a Screening Program in Melbourne, Australia. JMIR Res Protoc. 2019, 8, e13271. [Google Scholar] [CrossRef] [Green Version]
- Brink, D.R.; Shannon, P.J.; Vinson, G.A. Validation of a brief mental health screener for Karen refugees in primary care. Fam. Pract. 2016, 33, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Buchwald, D.; Manson, S.M.; Brenneman, D.L.; Dinges, N.G.; Keane, E.M.; Beals, J.; Kinzie, J.D. Screening for Depression among Newly Arrived Vietnamese Refugees in Primary Care Settings. West J. Med. 1995, 163, 341–345. [Google Scholar]
- Churbaji, D.; Lindheimer, N.; Schilz, L.; Böge, K.; Abdelmagid, S.; Rayes, D.; Hahn, E.; Bajbouj, M.; Karnouk, C. Development of a Culturally Sensitive Version of the MiniInternational Neuropsychiatric Interview (MINI) in Standard Arabic. Fortschr. Neurol. Psychiatr. 2020, 88, 95–104. [Google Scholar] [CrossRef]
- Cook, T.L.; Shannon, P.J.; Vinson, G.A.; Letts, J.P.; Dwee, E. War trauma and torture experiences reported during public health screening of newly resettled Karen refugees: A qualitative study. BMC Int. Health Hum. Rights 2015, 15, 8. [Google Scholar] [CrossRef] [Green Version]
- Di Pietro, M.L.; Zaçe, D.; Sisti, L.G.; Frisicale, E.M.; Corsaro, A.; Gentili, A.; Giraldi, L.; Bruno, S.; Boccia, S. Development and validation of a questionnaire to assess Unaccompanied Migrant Minors’ needs (AEGIS-Q). Eur. J. Public Health 2021, 31, 313–320. [Google Scholar] [CrossRef]
- Durieux-Paillard, S.; Whitaker-Clinch, B.; Bovier, P.A.; Eytan, A. Screening for major depression and posttraumatic stress disorder among asylum seekers: Adapting a standardized instrument to the social and cultural context. Can. J. Psychiatry 2006, 51, 587–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ghaziri, N.; Blaser, J.; Darwiche, J.; Suris, J.-C.; Sanchis Zozaya, J.; Marion-Veyron, R.; Spini, D.; Bodenmann, P. Protocol of a longitudinal study on the specific needs of Syrian refugee families in Switzerland. BMC Int. Health Hum. Rights 2019, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Eytan, A.; Durieux-Paillard, S.; Whitaker-Clinch, B.; Loutan, L.; Bovier, P.A. Transcultural Validity of a Structured Diagnostic Interview to Screen for Major Depression and Posttraumatic Stress Disorder among Refugees. J. Nerv. Ment. Dis. 2007, 195, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Eytan, A.; Bischoff, A.; Rrustemi, I.; Durieux, S.; Loutan, L.; Gilbert, M.; Bovier, P.A. Screening of Mental Disorders in Asylum-Seekers from Kosovo. Aust. N. Z. J. Psychiatry 2002, 36, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Geltman, P.L.; Grant-Knight, W.; Mehta, S.D.; Lloyd-Travaglini, C.; Lustig, S.; Landgraf, J.M.; Wise, P.H. The “Lost Boys of Sudan”: Functional and Behavioral Health of Unaccompanied Refugee Minors Resettled in the United States. Arch. Pediatr. Adolesc. Med. 2005, 159, 585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, A.E.; Weinberger, S.J.; Harder, V.S. The Strengths and Difficulties Questionnaire as a Mental Health Screening Tool for Newly Arrived Pediatric Refugees. J. Immigr. Minority Health 2021, 23, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Hanes, G.; Sung, L.; Mutch, R.; Cherian, S. Adversity and resilience amongst resettling Western Australian paediatric refugees: Refugee resilience and adversity. J. Paediatr. Child Health 2017, 53, 882–888. [Google Scholar] [CrossRef]
- Hauff, E.; Vaglum, P. Organised violence and the stress of exile. Predictors of mental health in a community cohort of Vietnamese refugees three years after resettlement. Br. J. Psychiatry 1995, 166, 360–367. [Google Scholar] [CrossRef]
- Heenan, R.C.; Volkman, T.; Stokes, S.; Tosif, S.; Graham, H.; Smith, A.; Tran, D.; Paxton, G. I think we’ve had a health screen: New offshore screening, new refugee health guidelines, new Syrian and Iraqi cohorts: Recommendations, reality, results and review: ‘I think we’ve had a health screen’. J Paediatr. Child Health 2019, 55, 95–103. [Google Scholar] [CrossRef]
- Hirani, K.; Cherian, S.; Mutch, R.; Payne, D.N. Identification of health risk behaviours among adolescent refugees resettling in Western Australia. Arch. Dis. Child 2018, 103, 240–246. [Google Scholar] [CrossRef]
- Hobbs, M.; Moor, C.; Wansbrough, T.; Calder, L. The health status of asylum seekers screened by Auckland Public Health in 1999 and 2000. N. Z. Med. J. 2002, 115, 1160. [Google Scholar]
- Hocking, D.C.; Mancuso, S.G.; Sundram, S. Development and validation of a mental health screening tool for asylum-seekers and refugees: The STAR-MH. BMC Psychiatry 2018, 18, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollifield, M.; Verbillis-Kolp, S.; Farmer, B.; Toolson, E.C.; Woldehaimanot, T.; Yamazaki, J.; Holland, A.; St. Clair, J.; SooHoo, J. The Refugee Health Screener-15 (RHS-15): Development and validation of an instrument for anxiety, depression, and PTSD in refugees. Gen. Hosp. Psychiatry 2013, 35, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Toolson, E.C.; Verbillis-Kolp, S.; Farmer, B.; Yamazaki, J.; Woldehaimanot, T.; Holland, A. Effective Screening for Emotional Distress in Refugees: The Refugee Health Screener. J. Nerv. Ment. Dis. 2016, 204, 247–253. [Google Scholar] [CrossRef]
- Jakobsen, M.; Meyer DeMott, M.A.; Heir, T. Validity of screening for psychiatric disorders in unaccompanied minor asylum seekers: Use of computer-based assessment. Transcult. Psychiatry 2017, 54, 611–625. [Google Scholar] [CrossRef]
- Javanbakht, A.; Amirsadri, A.; Abu Suhaiban, H.; Alsaud, M.I.; Alobaidi, Z.; Rawi, Z.; Arfken, C.L. Prevalence of Possible Mental Disorders in Syrian Refugees Resettling in the United States Screened at Primary Care. J. Immigr. Minority Health 2019, 21, 664–667. [Google Scholar] [CrossRef]
- Johnson-Agbakwu, C.E.; Allen, J.; Nizigiyimana, J.F.; Ramirez, G.; Hollifield, M. Mental health screening among newly arrived refugees seeking routine obstetric and gynecologic care. Psychol. Serv. 2014, 11, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Kaltenbach, E.; Härdtner, E.; Hermenau, K.; Schauer, M.; Elbert, T. Efficient identification of mental health problems in refugees in Germany: The Refugee Health Screener. Eur. J. Psychotraumatol. 2017, 8, 1389205. [Google Scholar] [CrossRef]
- Kennedy, J.; Seymour, D.J.; Hummel, B.J. A comprehensive refugee health screening program. Public Health Rep. 1999, 114, 469–477. [Google Scholar] [CrossRef]
- Kleijn, W.C.; Hovens, J.E.; Rodenburg, J.J. Posttraumatic Stress Symptoms in Refugees: Assessments with the Harvard Trauma Questionnaire and the Hopkins Symptom Checklist–25 in Different Languages. Psychol. Rep. 2001, 88, 527–532. [Google Scholar] [CrossRef]
- Kleinert, E.; Müller, F.; Furaijat, G.; Hillermann, N.; Jablonka, A.; Happle, C.; Simmenroth, A. Does refugee status matter? Medical needs of newly arrived asylum seekers and resettlement refugees—A retrospective observational study of diagnoses in a primary care setting. Confl. Health 2019, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Kröger, C.; Frantz, I.; Friel, P.; Heinrichs, N. Posttraumatische und depressive Symptomatik bei Asylsuchenden. Psychother Psychosom. Med. Psychol. 2016, 66, 377–384. [Google Scholar] [CrossRef]
- LeMaster, J.W.; Broadbridge, C.L.; Lumley, M.A.; Arnetz, J.E.; Arfken, C.; Fetters, M.D.; Jamil, H.; Pole, N.; Arnetz, B.B. Acculturation and post-migration psychological symptoms among Iraqi refugees: A path analysis. Am. J. Orthopsychiatry 2018, 88, 38–47. [Google Scholar] [CrossRef]
- Lillee, A.; Thambiran, A.; Laugharne, J. Evaluating the mental health of recently arrived refugee adults in Western Australia. J. Public Ment. Health 2015, 14, 56–68. [Google Scholar] [CrossRef]
- Loutan, L.; Bollini, P.; Pampallona, S.; Haan, D.B.D.; Gar, F. Impact of trauma and torture on asylum-seekers. Eur. J. Public Health 1999, 9, 93–96. [Google Scholar] [CrossRef]
- Masmas, T.N.; Student, E.M.; Bunch, V.; Jensen, J.H.; Hansen, T.N.; Jørgensen, L.M.; Kj, C.; Oxholm, A.; Worm, L.; Ekstrøm, M. Asylum seekers in Denmark—A study of health status and grade of traumatization of newly arrived asylum seekers. Torture Q. J. Rehabil. Torture Vict. Prev. Torture 2008, 18, 10. [Google Scholar]
- McLeod, A.; Reeve, M. The health status of quota refugees screened by New Zealand’s Auckland Public Health Service between 1995 and 2000. N. Z. Med. J. 2005, 118, 1224. [Google Scholar]
- Mewes, R.; Friele, B.; Bloemen, E. Validation of the Protect Questionnaire: A tool to detect mental health problems in asylum seekers by non-health professionals. Torture J. 2018, 28, 2. [Google Scholar] [CrossRef]
- Morina, N.; Ewers, S.M.; Passardi, S.; Schnyder, U.; Knaevelsrud, C.; Müller, J.; Bryant, R.A.; Nickerson, A.; Schick, M. Mental health assessments in refugees and asylum seekers: Evaluation of a tablet-assisted screening software. Confl. Health 2017, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- Nehring, I.; Sattel, H.; Al-Hallak, M.; Sack, M.; Henningsen, P.; Mall, V.; Aberl, S. The Child Behavior Checklist as a Screening Instrument for PTSD in Refugee Children. Children 2021, 8, 521. [Google Scholar] [CrossRef]
- Nikendei, C.; Kindermann, D.; Brandenburg-Ceynowa, H.; Derreza-Greeven, C.; Zeyher, V.; Junne, F.; Friederich, H.-C.; Bozorgmehr, K. Asylum seekers’ mental health and treatment utilization in a three months follow-up study after transfer from a state registration-and reception-center in Germany. Health Policy 2019, 123, 864–872. [Google Scholar] [CrossRef]
- Ovitt, N.; Larrison, C.R.; Nackerud, L. Refugees’ Responses to Mental Health Screening: A Resettlement Initiative. Int. Soc. Work 2003, 46, 235–250. [Google Scholar] [CrossRef]
- Polcher, K.; Calloway, S. Addressing the Need for Mental Health Screening of Newly Resettled Refugees: A Pilot Project. J. Prim. Care Community Health 2016, 7, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Poole, D.N.; Liao, S.; Larson, E.; Hedt-Gauthier, B.; Raymond, N.A.; Bärnighausen, T.; Smith Fawzi, M.C. Sequential screening for depression in humanitarian emergencies: A validation study of the Patient Health Questionnaire among Syrian refugees. Ann. Gen. Psychiatry 2020, 19, 5. [Google Scholar] [CrossRef]
- Rasmussen, A.; Verkuilen, J.; Ho, E.; Fan, Y. Posttraumatic stress disorder among refugees: Measurement invariance of Harvard Trauma Questionnaire scores across global regions and response patterns. Psychol. Assess. 2015, 27, 1160–1170. [Google Scholar] [CrossRef]
- Richter, K.; Lehfeld, H.; Niklewski, G. Waiting for Asylum: Psychiatric Diagnoses in the central reception facility in Bavaria. Gesundheitswesen 2015, 77, 834–838. [Google Scholar] [CrossRef]
- Salari, R.; Malekian, C.; Linck, L.; Kristiansson, R.; Sarkadi, A. Screening for PTSD symptoms in unaccompanied refugee minors: A test of the CRIES-8 questionnaire in routine care. Scand. J. Public Health 2017, 45, 605–611. [Google Scholar] [CrossRef]
- Savin, D.; Seymour, D.J.; Littleford, L.N.; Bettridge, J.; Giese, A. Findings from Mental Health Screening of Newly Arrived Refugees in Colorado. Public Health Rep. 2005, 120, 224–229. [Google Scholar] [CrossRef]
- Schweitzer, R.D.; Brough, M.; Vromans, L.; Asic-Kobe, M. Mental Health of Newly Arrived Burmese Refugees in Australia: Contributions of Pre-Migration and Post-Migration Experience. Aust. N. Z. J. Psychiatry 2011, 45, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Seagle, E.E.; Vargas, M. Prevalence of Mental Health Screening and Associated Factors among Refugees and other Resettled Populations ≥ 14 Years of Age in Georgia, 2014–2017. J. Immigrant Minority Health 2019, 21, 1191–1199. [Google Scholar] [CrossRef]
- Shannon, P.J.; Vinson, G.A.; Wieling, E.; Cook, T.; Letts, J. Torture, War Trauma, and Mental Health Symptoms of Newly Arrived Karen Refugees. J. Loss Trauma 2015, 20, 577–590. [Google Scholar] [CrossRef]
- Söndergaard, H.P.; Ekblad, S.; Theorell, T. Self-reported life event patterns and their relation to health among recently resettled Iraqi and Kurdish refugees in Sweden. J. Nerv. Ment. Dis. 2001, 189, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Sondergaard, H.P.; Ekblad, S.; Theorell, T. Screening for post-traumatic stress disorder among refugees in Stockholm. Nord. J. Psychiatry 2003, 57, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Stingl, M.; Knipper, M.; Hetzger, B.; Richards, J.; Yazgan, B.; Gallhofer, B.; Hanewald, B. Assessing the special need for protection of vulnerable refugees: Testing the applicability of a screening method (RHS-15) to detect traumatic disorders in a refugee sample in Germany. Ethn. Health 2019, 24, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Sukale, T.; Hertel, C.; Möhler, E.; Joas, J.; Müller, M.; Banaschewski, T.; Schepker, R.; Kölch, M.G.; Fegert, J.M.; Plener, P.L. Diagnostics and initial assessment in the case of underage refugees. Nervenarzt 2017, 88, 3–9. [Google Scholar] [CrossRef]
- Tay, K.; Frommer, N.; Hunter, J.; Silove, D.; Pearson, L.; San Roque, M.; Redman, R.; Bryant, R.A.; Manicavasagar, V.; Steel, Z. A mixed-method study of expert psychological evidence submitted for a cohort of asylum seekers undergoing refugee status determination in Australia. Soc. Sci. Med. 2013, 98, 106–115. [Google Scholar] [CrossRef]
- Thulesius, H.; Håkansson, A. Screening for posttraumatic stress disorder symptoms among Bosnian refugees. J. Traum. Stress 1999, 12, 167–174. [Google Scholar] [CrossRef]
- Van Os, E.C.C.; Zijlstra, A.E.; Knorth, E.J.; Post, W.J.; Kalverboer, M.E. Recently arrived refugee children: The quality and outcomes of Best Interests of the Child assessments. Int. J. Law Psychiatry 2018, 59, 20–30. [Google Scholar] [CrossRef]
- Van Dijk, D.G.L.; Kortmann, F.A.M.; Kooyman, M.; Bot, J. The Harvard Trauma Questionnaire. A cross-cultural instrument for screening posttraumatic stress disorder in hospitalized refugees. Tijdschr. Psychiatr. 1999, 41, 45–49. [Google Scholar]
- Vergara, A.E.; Miller, J.M.; Martin, D.R.; Cookson, S.T. A Survey of Refugee Health Assessments in the United States. J. Immigr. Health 2003, 7, 67–73. [Google Scholar] [CrossRef]
- Weine, S.M.; Vojvoda, D.; Becker, D.F.; McGlashan, T.H.; Hodzic, E.; Laub, D.; Hyman, L.; Sawyer, M.; Lazrove, S. PTSD Symptoms in Bosnian Refugees 1 Year after Resettlement in the United States. Am. J. Psychiatry 1998, 155, 562–564. [Google Scholar] [CrossRef]
- Willey, S.M.; Gibson-Helm, M.E.; Finch, T.L.; East, C.E.; Khan, N.N.; Boyd, L.M.; Boyle, J.A. Implementing innovative evidence-based perinatal mental health screening for women of refugee background. Women Birth 2020, 33, e245–e255. [Google Scholar] [CrossRef]
- Wulfes, N.; del Pozo, M.A.; Buhr-Riehm, B.; Heinrichs, N.; Kröger, C. Screening for Posttraumatic Stress Disorder in Refugees: Comparison of the Diagnostic Efficiency of Two Self-Rating Measures of Posttraumatic Stress Disorder: Screening for PTSD in Refugees. J. Trauma. Stress 2019, 32, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Yalim, A.C.; Zubaroglu-Ioannides, P.; Sacco, S. Implementation of an Initial Mental Health Assessment for Newly Arrived Refugees. J. Soc. Serv. Res. 2021, 47, 199–206. [Google Scholar] [CrossRef]
- Young, P.; Gordon, M.S. Mental health screening in immigration detention: A fresh look at Australian government data. Australas Psychiatry 2016, 24, 19–22. [Google Scholar] [CrossRef]
- Sweileh, W.M.; Wickramage, K.; Pottie, K.; Hui, C.; Roberts, B.; Sawalha, A.F.; Zyoud, S.H. Bibliometric analysis of global migration health research in peer-reviewed literature (2000–2016). BMC Public Health 2018, 18, 777. [Google Scholar] [CrossRef] [Green Version]
- CDC. Mental Health Technical Instructions for Panel Physicians. Available online: https://www.cdc.gov/immigrantrefugeehealth/panel-physicians/mental-health.html (accessed on 16 December 2021).
- Immigration New Zealand (INZ). Refugee Settlement Health Assessments. Available online: https://www.immigration.govt.nz/assist-migrants-and-students/other-industry-partners/panel-physician-network/refugee-settlement-health-assessments (accessed on 16 December 2021).
- Cowen, T.; Stella, F.; Magahy, K.; Strauss, K.; Morton, J. Sanctuary, Safety and Solidarity: Lesbian, Gay, Bisexual, Transgender Asylum Seekers and Refugees in Scotland; University of Glasgow: Glasgow, UK, 2011. [Google Scholar]
- White, L.C.; Cooper, M.; Lawrence, D. Mental illness and resilience among sexual and gender minority refugees and asylum seekers. Br. J. Gen. Pract 2019, 69, 10–11. [Google Scholar] [CrossRef] [Green Version]
- Women’s Refugee Commission. Disabilities Among Refugees and Conflict-Affected Populations; Women’s Refugee Commission: New York, NY, USA, 2010; ISBN 978-1-58030-072-8. [Google Scholar]
- Purkey, E.; Patel, R.; Phillips, S.P. Trauma-informed care. Can. Fam. Physician 2018, 64, 170–172. [Google Scholar]
- Crocker, E.; Webster, P.D. Developing Patient- and FamilyCentered Vision, Mission, and Philosophy of Care Statements, 2nd ed.; Institute for Patient- and Family-Centered Care: Bethesda, MD, USA, 2012. [Google Scholar]
- Griswold, K.S.; Vest, B.M.; Lynch-Jiles, A.; Sawch, D.; Kolesnikova, K.; Byimana, L.; Kefi, P. “I just need to be with my family”: Resettlement experiences of asylum seeker and refugee survivors of torture. Glob. Health 2021, 17, 27. [Google Scholar] [CrossRef]
- Member Centers of the National Consortium of Torture Treatment Programs (NCTTP). Descriptive, inferential, functional outcome data on 9025 torture survivors over six years in the United States. Torture 2015, 25, 34–60. [Google Scholar]
- Dunn, T.J.; Browne, A.; Haworth, S.; Wurie, F.; Campos-Matos, I. Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement. Int. J. Environ. Res. Public Health 2021, 18, 10331. [Google Scholar] [CrossRef]
- Regmi, P.R.; Aryal, N.; van Teijlingen, E.; Simkhada, P.; Adhikary, P. Nepali Migrant Workers and the Need for Pre-departure Training on Mental Health: A Qualitative Study. J. Immigr Minor. Health 2020, 22, 973–981. [Google Scholar] [CrossRef] [Green Version]
- Grist, R.; Porter, J.; Stallard, P. Mental Health Mobile Apps for Preadolescents and Adolescents: A Systematic Review. J. Med. Internet Res. 2017, 19, e176. [Google Scholar] [CrossRef] [Green Version]
- Magwood, O.; Bellai Dusseault, K.; Fox, G.; McCutcheon, C.; Adams, O.; Saad, A.; Kassam, A. Diagnostic Test Accuracy of Screening Tools for Post-Traumatic Stress Disorder Among Refugees and Asylum Seekers: A Protocol for a Systematic Review of Diagnostic Test Accuracy Studies; Cochrane Equity Methods: Ottawa, ON, Canada, 2021. [Google Scholar]
- Saad, A.; Magwood, O.; Aubry, T.; Alkhateeb, Q.; Hashmi, S.S.; Hakim, J.; Ford, L.; Kassam, A.; Tugwell, P.; Pottie, K. Mobile interventions targeting common mental disorders among pregnant and postpartum women: An equity-focused systematic review. PLoS ONE 2021, 16, e0259474. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, J.; Rousseau, C.; Guzder, J. Cultural Consultation for Refugees. In Encountering the Other in Mental Health Care; Springer: Amsterdam, The Neatherlands, 2014; pp. 245–268. ISBN 978-1-4614-7614-6. [Google Scholar]
- Ng, E.; Pottie, K.; Spitzer, D. Official language proficiency and self-reported health among immigrants to Canada. Health Rep. 2011, 22, 15–23. [Google Scholar] [PubMed]
- Pottie, K.; Hadi, A.; Chen, J.; Welch, V.; Hawthorne, K. Realist review to understand the efficacy of culturally appropriate diabetes education programmes. Diabet. Med. 2013, 30, 1017–1025. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SPIDER | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Sample | Refugees and asylum seekers of all ages | All populations other than refugees and asylum seekers |
| Phenomenon of Interest | Pre-settlement overseas screening approaches or post-arrival (<12 months) approaches for mental health | Screening for other health conditions Routine screening after 1 year post-arrival |
| Design | Experimental and quasi-experimental studies Observational studies Program evaluations Resettlement handbooks and manuals Policy documents Development & validation studies Clinical assessment studies | Systematic reviews Scoping reviews Literature reviews Commentaries/opinion Theoretical papers |
| Evaluation | Characteristics of screening approaches | Estimates of effect Experiences/views |
| Research type | Quantitative, qualitative, or mixed-method documents published in peer-reviewed or grey literature | N/A |
| Other | ||
| Year of publication | 1995–2020 | Prior to 1995 |
| Language of publication | All languages eligible | N/A |
| Study | Design | Setting | Timing of Assessment | Population | Mental Health Condition Assessed and Assessment Tool | Administration Details |
|---|---|---|---|---|---|---|
| Al-Obaidi (2015) [41] | Screening program | Refugee health care programs USA | Post-arrival | Refugees Burma, Haiti, Sudan, Iraq, Afghanistan, Somalia, and Cuba | Mental health assessment was not widely practiced (6/16 refugee-serving organizations). Assessment conducted by asking a few basic questions, e.g., for adults, any history of sleep problems, loss of energy, loss of appetite, feeling depressed, torture; and asking about the story of the refugee’s journey; for children, any history of seizures, learning problems, and head injuries In Denver, screening includes a DSM-based, non-validated questionnaire designed to detect major depression and PTSD The Seattle and New Mexico programs offer the Refugee Health Screener-15 (RHS-15) [PTSD, Depression, Anxiety] | In Denver, the mental health screening is conducted by a master’s level social worker Screening using the RHS-15 administered by health care providers. Clients themselves can complete the form if they have the appropriate level of education Interpreter not present Oral interview Assessment time not reported |
| Arnetz (2014) [42] | Validation study | Community centees USA | Post-arrival | Refugees Age 18–69 years, M = 33.41, SD = 11.29 54% male Iraq | Pre-immigration trauma exposure: Trauma section of Harvard Trauma Questionnaire (HTQ) PTSD: Civilian version of the PTSD Checklist (PCL-C) Depression: Hospital Anxiety and Depression Scale (HADS) | Administered by trained Arabic-speaking research personnel Interpreter present Self-assessment survey 120 min |
| Baird (2020) [43] | Screening program | Nurse-managed urban primary care safety-net clinic USA | Post-arrival | Refugees Mean age 32.8 years, SD = 13.6, Range = 17–72; 46% male. Country of origin not reported | Emotional distress including anxiety, depression, and PTSD: Refugee Health Screener-15 (RHS-15) | Administered by trained Doctor of Nursing Practice (DNP) family nurse practitioners Interpreter present Likert Scale, oral interview 60 min |
| Barbieri (2019) [44] | Validation study | Outpatient clinic and reception centre Italy | Post-arrival | Refugees and asylum seekers Age 18 and older (M = 25.1 years, SD = 6.7); 86% male Participants were from 19 African countries, mainly West Africa | PTSD: Posttraumatic Stress Disorder Checklist (PCL-5) CPTSD: International Trauma Questionnaire (ICD-11) | Administered by cultural mediator, a medical doctor, and a clinical psychologist Interpreter present Oral interview 60–90 min |
| Barnes (2001) [40] | Screening program | Local health department not affiliated with a hospital, combined with home visits USA | Post-arrival | Refugees Age 18–74 46.4% male Vietnam, Cuba, Bosnia, and African countries | Depression: DSM-IV criteria psychiatric interview | Administered by psychiatric residents with multi-national immigrant backgrounds (Africa and India) Interpretation provided by a paid interpreter (Vietnamese), administrative assistant (Bosnian), or nurse (Spanish). Family members also acted as interpreters (e.g., Farsi) Oral interview Assessment time not reported |
| Bertelsen (2018) [45] | Screening program | Primary care torture treatment centre USA | Post-arrival | Asylum seekers Mean age of 36.6 years (SD10.2) 66.2% male Majority from Sub-Saharan Africa (Guinea, Burkina Faso, and Democratic Republic of Congo being the most represented). Minority from Asia (with the Nepal and Tibet accounting for the majority of these) | PTSD: Harvard Trauma Questionnaire (HTQ) Major depressive disorder: Patient Health Questionnaire-9 (PHQ-9) | Administered by mental health professionals Interpreter present Oral interview Assessment time not reported |
| Bjarta (2018) [46] | Validation study | Asylum accommodations and health and service centres Sweden | Post-arrival | Refugees and asylum seekers aged 18 years and older; 72% male Afghanistan, Syria, Iraq, Iran, Eritrea, and Somalia | PTSD, depression, anxiety: Refugee Health Screener (RHS-13) Depression: Patient Health Questionnaire 9 (PHQ-9) Generalized anxiety: Generalized Anxiety Disorder 7 (GAD-7) PTSD: Primary Care PTSD-4 (PC-PTSD-4) Quality of life: World Health Organization Quality of Life–Brief Version (WHOQOL-BREF) | Self-assessment facilitated by bilingual administration staff Interpreter (bilingual staff) present Tablet. Audio support was available in Arabic, Dari, Farsi, and Tigrinya for individuals with low reading proficiency Assessment time not reported |
| Boyle (2019) [47] | Screening program | Refugee antenatal clinic Australia | Post-arrival | Refugees of childbearing age (below 35 years old) 100% female Afghanistan, Myanmar, Iraq, the Republic of South Sudan, and Sri Lanka. | Depression and anxiety: Edinburgh Postnatal Depression Scale (EPDS) Perinatal mental health: Monash Psychosocial Screening Tool | Self-assessment. Clinic staff available for assistance Interpreter present if needed Electronic via tablet 6–10 min |
| Brink (2016) [48] | Validation study | Primary care clinic USA | Post-arrival | Karen Refugees Aged 18–80 (M = 38.09, SD 13.82) 30% male Burma | PTSD and MDD: PTSD and MDD portions of the structured clinical interview for DSM disorders (SCID-CV for DSM-IV) | A physician with mental health training and a Karen interpreter administered the measures Oral interview and Likert-scale questionnaire Assessment time not reported |
| Buchwald (1995) [49] | Screening program | Ten refugee public health clinics USA | Post-arrival | Refugees Aged 16–85 yo (average age 31) 95% male Vietnam | Depression: Vietnamese Depression Scale | Administered by trained community health nurse Interpreter present Self-assessment 5 min |
| Churbaji (2020) [50] | Validation study | University hospital Germany | Post-arrival | Refugees Mean age 33.5 yo 75% male Syria, Iraq, Palestine | Depression and PTSD: Mini International Neuropsychiatric Interview (MINI) Depression: Patient Health Questionnaire, 9 (PHQ-9) PTSD: Harvard Trauma Questionnaire (HTQ) | Not reported |
| Cook (2015) [51] | Screening program | Primary care clinic USA | Post-arrival | Arabic-speaking Karen refugees Aged 18 yo and over (mean age: 35 (SD 14.6) 51% male | Four semi-structured items which asked retrospectively about lifetime experiences of primary and secondary war trauma and torture | Administered by trained research assistants (social work trainees) Interpreter present Oral interview Assessment time not reported |
| Di Pietro (2021) [52] | Validation study | Second-line reception centre Italy | Post-arrival | Unaccompanied migrant minors Age 12–18 yo 100% male Bangladesh, Egypt, Gambia, Senegal, Benin, Tunisia, Guinea Bissau, Morocco | Overall psychological needs: Unaccompanied Migrant Minors Questionnaire (AEGIS-Q) | Interpreter not present Self-administered with cultural mediator 20 min |
| Durieux-Paillard (2006) [53] | Validation study | Migrant health centre (University Hospital) Switzerland | Post-arrival | Asylum seekers Age 16 years or older | MDD and PTSD: Mini International Neuropsychiatric Interview (MINI) | Nurses without mental health training Interpreter present Oral interview 45 min |
| El Ghaziri (2019) [54] | Screening program | Centre for primary care and public health Switzerland | Post-arrival | Refugee families Members over age 8 yo 40–60% female Syria | Risk behaviours: ASSIST Support: Multidimensional Scale of Perceived Social Support (MSPSS) Parent-child relationship: Family Peer Relationship Questionnaire, Arabic version (A-FPRQ) Adults: major depressive disorder, panic disorder, posttraumatic stress disorder, generalized anxiety: Mini International Neuropsychiatric Interview (MINI) Children: major depressive disorder, panic disorder, separation anxiety, posttraumatic stress disorder: Mini International Neuropsychiatric Interview for Kids (MINI Kid) | Research assistant Interpreter present (research assistant) Administration mode not reported Assessment time not reported |
| Eytan (2007) [55] | Validation study | Primary care clinic Switzerland | In transition | Refugees Mean age 30 yo 75% male 33 countries, mostly Africa and Central or Eastern Europe | Major depressive episodes and PTSD: Mini International Neuropsychiatric Interview (MINI) | Administered by trained nurse Interpreter present Oral interview Assessment time not reported |
| Eytan (2002) [56] | Screening program | IME assessment Switzerland | In transition | Refugees, median age 24 yo 72% male Kosovo | MDD and PTSD: Mini International Neuropsychiatric Interview (MINI) | Administered by trained nurse Interpreter present Oral interview Assessment time not reported |
| Geltman (2005) [57] | Screening program | Unaccompanied Refugee Minors Program (URMP) sites USA | Post-arrival | Refugee minors, mean age 17.6 yo 84% male Sudan | PTSD: Harvard Trauma Questionnaire (HTQ) and Child Health Questionnaire (CHQ) | Administered by staff Interpreter not present Oral interview and self-assessment Assessment time not reported |
| Green (2021) [58] | Screening program | Primary care “office” USA | Post-arrival | Refugees, age 4–18 yo 56% male Bhutan, Burma, Democratic Republic of Congo/Burundi, Iraq, Somalia | PTSD, depression, trauma: Strengths and Difficulties Questionnaire (SDQ) | Administered by interpreters Interpreter present Oral interview Assessment time not reported |
| Hanes (2017) [59] | Screening program | Hospital refugee health service Australia | Post-arrival | Refugees Age 2–16 yo mean age 9.4 yo 49% male Top 7 countries: Burma, Afghanistan, Sudan, Ethiopia Congo, Somalia, Iran | Adverse childhood experiences: Strengths and Difficulties Questionnaire (SDQ) | Interpreter present Self-administered Assessment time not reported |
| Hauff (1995) [60] | Screening program | n/a Norway | Post-arrival | Refugees Age over 15 yo 79% male Vietnam | Psychiatric disorders: Symptom Checklist 90 (SCL-90) and Present State Examination (PSE) | Researcher Interpreter present Oral interview Assessment time not reported |
| Heenan (2019) [61] | Screening program | Specialist immigrant health service within a children’s hospital Australia | Post-arrival | Refugee children Age 7 months to 16 years old 64.8% male Syria, Iraq | Mental health (including PTSD) and development screening was conducted, but no assessment tool is described | Refugee health program nurses Primary care health assessment Assessment time not reported |
| Hirani (2018) [62] | Screening program | Tertiary refugee health service Australia | Post-arrival | Adolescent refugees Age 12–17 years old (mean age 14; 49% male) 15 countries (Middle East, Africa, Asia) | Psychosocial assessment: Home, Education/Eating, Activities, Drugs, Sexuality, Suicide/mental health’ (HEADSS) Questionnaire | Interviewer Interpreter present Oral interview 25–60 min |
| Hobbs (2002) [63] | Screening program | Public health hospital New Zealand | Post-arrival | Asylum seekers Age 0–60+ years old 68.1% male Middle Eastern countries | Symptoms, or history of symptoms, of psychological illness: Auckland Public Health Protection Asylum Seekers Screening | Clinic staff Health screening Assessment time not reported |
| Hocking (2018) [64] | Validation study | Asylum seeker welfare centre Australia | Post-arrival | Refugees 19–82 yo, median age 33 69.8% male Mostly from countries in Africa and Asia | Major depressive disorder (MDD) and post-traumatic stress disorder (PTSD): Mental Health Screening Tool for Asylum seekers and Refugees (STAR-MH) | Administered by trained non-mental health workers Interpreter present Oral interview 6 min |
| Hollifield (2013) [65] | Validation study | Public health centre USA | Post-arrival | Refugees Age over 14 yo 50% male Bhutan, Burma, and Iraq | Anxiety, depression, PTSD: Refugee Health Screener-15 (RHS-15) | Administered by physicians or public health clinic staff Interpreter present Oral interview 4–12 min |
| Hollifield (2016) [66] | Validation study | Public health centre USA | Post-arrival | Refugees Age over 14 yo 50% male Bhutan, Burma, and Iraq | Anxiety and depression: Hopkins Symptom Checklist 25 (HSCL-25) PTSD: Posttraumatic Symptom Scale- Self Report (PSS-SR) Anxiety, depression, PTSD: Refugee Health Screener-15 (RHS-15) | Administered by trained public health nurses Interpreter not present Oral interview Assessment time not reported |
| Hough (2019) [39] | Screening program | Refugee clinic Lebanon | Pre-departure | Refugees 18 years and above 50% male Syria | General mental health: Global Mental Health Assessment Tool (GMHAT) | Administered by healthcare professionals (psychiatrist, general physician, pediatrician, and two nurses) Administrators served as translators Computerized tool 15–20 min |
| International Organization for Migration (IOM) (2020) [4] | Screening program | IOM migration health assessment clinics Lebanon, Turkey, and Jordan | Pre-departure | Refugees: majority younger than 30 (67.1%), with the highest number in the under-10 age group 51.2% male | Not described | Not described |
| Jakobsen (2017) [67] | Validation study | Setting not reported Norway | Post-arrival | Unaccompanied adolescent asylum seekers Age 15–18 years old (mean: 16.2) 100% male Afghanistan, Somalia | PTSD, anxiety, and depression: combined Hopkins Symptom Checklist-25 (HSCL-25) and Harvard Trauma Questionnaire (HTQ- IV) | Interpreter present Self-administered via laptop computer Assessment duration not reported |
| Javanbakht (2019) [68] | Screening program | Primary care clinic USA | Post-arrival | Refugees Age 18–65 yo 52.9% male Syria | PTSD: PTSD Checklist Civilian version (PCL-C) Anxiety and depression: Hopkins Symptom Checklist 25 items (HSCL-25) | Research assistant Interpreter present (research assistant) Self-assessment 20 min (5–10 min per tool) |
| Johnson-Agbakwu (2014) [69] | Screening program | Refugee women’s health clinic with a behavioural health partnership USA | Post-arrival | Refugees Age 18 years and older 100% female Iraq, Burma, Somalia | Anxiety, depression, PTSD: Refugee Health Screener-15 (RHS-15) | Cultural health navigator (served as interpreter) Oral interview 5–10 min |
| Kaltenbach (2017) [70] | Validation study | Refugee accommodation Germany | In transition | Refugees Age over 12 yo, median age 28.79 yo Majority from Syria, minority from Afghanistan, Albania, Kosovo, Serbia, Iraq, Macedonia, Somalia, Georgia | PTSD, depression, anxiety: Refugee Health Screener-15 (RHS-15) Semi-structured interview: PTSD: Post-traumatic Stress Disorder Checklist-5 (PCL-5) Depression: Refugee Health Screener (RHS-15)—only the first 13 questions Trauma exposure: Life Events Checklist (LEC-5) Psychological distress: semi-structured interview via Brief Symptom Inventory -18 | RHS Self-administered Interpreter present if needed 10–30 min Semi-structured interview by a clinical psychologist Interpreter present Oral interview 90 min |
| Kennedy (1999) [71] | Screening program | Primary care clinic (University Hospital) USA | Post-arrival | Adult refugees and their children | Depression, anxiety, and PTSD: A set of questions about history of imprisonment, trauma, or torture + a 25-item, self-administered symptom checklist that surveys for symptoms of depression, anxiety, and PTSD. The checklist was developed by Dawn Noggle, PhD, of the International Rescue Committee in Arizona. In addition, parents are asked standard questions about their children’s adjustment and symptoms of stress or depression | Administered by nurse or physician Interpreter present Self-assessment symptom checklist Assessment time not reported |
| Kleijn (2001) [72] | Validation study | Psychiatric clinic Netherlands | Post-arrival | Refugees 81% male Arabic, Farsi, or Serbo-Croatian speaking regions | PTSD: The Harvard Trauma Questionnaire (HTQ) Depression and Anxiety: Hopkins Symptoms Checklist-25(HSCL-25) | Administered by psychologist or psychiatrist Interpreter present Self-assessment Assessment time not reported |
| Kleinert (2019) [73] | Screening program | Primary care centre within a reception centre Germany | Post-arrival | Refugee and asylum seekers median age of all patients was 26 years, SD 18.529 51% of asylum-seeker patients and 49% of resettlement-refugee patients were female Iraq, Syria, Afghanistan, Georgia, Iran | Mental and behavioural disorders classified by ICD 10: Digital Communication Assistance Tool (DCAT) | General practitioners and nurses Digital Communication Assistance Tool (DCAT) via tablet No interpreter present Self-assessment Assessment time not reported |
| Kroger (2016) [74] | Screening Program | Reception centre Germany | Post-arrival | Refugees and asylum seekers Average age 30.5 88.2% male Balkan States, Middle East, Northern Africa, rest of Africa | PTSD: Post-traumatic Diagnostic Scale-8 (PDS-8) Depression: Patient Health Questionnaire (PHQ-8) | Administered by psychological psychotherapist, medical assistant, or psychology undergraduate students Interpreter present Oral interview 15–90 min |
| LeMaster (2018) [75] | Screening program | Local resettlement agencies USA | Post-arrival | Refugees Mean age 33.4 Iraq | PTSD: civilian version of the PTSD Checklist (PCL-C) and Harvard Trauma Questionnaire (HTQ) Depression: Hospital Anxiety and Depression Scale | Administered by a trained Arabic-speaking interviewer Interpreter present Oral interview 120 min |
| Lillee (2015) [76] | Screening program | Humanitarian entrant health service Australia | Post-arrival | Refugees Age 18–70 48.7% male Africa, South-Eastern and South-Western Asia | Non-specific psychological distress: The Kessler Psychological Distress Scale (K10) PTSD: PTSD treatment screener | Administered by physicians Interpreter present Oral interview or self-assessment 10–15 min |
| Loutan (1999) [77] | Screening program | University Hospital Switzerland | Post-arrival | Refugees Median age 27 67% male Yugoslavia, Somalia, Angola, Sri-Lanka | Physical and psychological symptoms and previous exposure to traumatic events: No name; short questionnaire developed and tested at the Policlinic | Administered by trained nurses (who were multilingual) Interpreter not present Oral interview 15 min |
| Masmas (2008) [78] | Screening program | Reception centre Denmark | Post-arrival | Asylum seekers, average age 32 years (16–73 years) 71% male Afghanistan, Iraq, Iran, Syria, and Chechnya | PTSD: International Classification of Disease Codes (ICD-10) Overall psychological health: WHO’s General Health Questionnaire | Administered by trained health care professionals Translator available if needed Oral interview 60 min |
| McLeod (2005) [79] | Screening program | Refugee resettlement centre medical clinic New Zealand | Post-arrival | Refugees: majority 20–34 years old 53.2% male, 34 different nationalities, majority Iraqi, Somali, Ethiopian | Psychosocial assessment—screening tool not reported | Administered by trained health care professionals Administration details not reported |
| Mewes 2018 [80] | Validation study | Asylum accommodation or at meeting points for asylum seekers Germany | Post-arrival | Asylum seekers Aged 18 years and older (M = 31.9 years SD 7.8), 67% male Most participants came from Iran, Afghanistan, Syria, or African countries | PTSD and depression: Process of Recognition and Orientation of Torture Victims in European Countries to Facilitate Care and Treatment (PROTECT) Questionnaire PTSD: Posttraumatic Diagnostic Scale (PDS) Depression: Patient Health Questionnaire-9 (PHQ9) | Self-assessment The software ‘MultiCasi’ was used via a laptop with touchscreen Interpreter present Assessment time not reported |
| Morina (2017) [81] | Screening program | Clinical setting outpatient clinic Switzerland | Post-arrival | Refugees Aged 28–64 (mean 50.07, SD 8.65) 77% male Afghanistan, Sri Lanka, Iraq, Turkey, Sudan | PTSD: Posttraumatic Diagnostic Scale based on DSM-5 (PDS) Depression: Hopkins Symptom Checklist-25 (HSCL-25) Quality of Life: EUROHIS-QoL Questionnaire | Interview with therapist Interpreter present Oral interview Assessed in 24 min or Computer assisted self-interviews using multi-adaptive psychological screening software (MAPSS) Tablet Assessed in 9 min |
| Nehring (2021) [82] | Validation study | Reception camp Germany | Post-arrival | Refugee children Age 4–14 years (mean: 8.9 years (SD: 2.8)) tijana59.0% male Syria | PTSD: Child Behaviour Checklist (CBCL) | Child and adolescent psychiatrists Interpreter and native speaking doctors were present Oral interview with parents and children The duration of all examinations lasted 1–2 days for one family |
| Nikendei (2019) [83] | Screening program | Outpatient clinic Germany | Post-arrival | Asylum seekers Age over 18 yo Asia, Africa, Eastern Europe | PTSD: Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) Depression: Patient Health Questionnaire-2 (PHQ-2) General anxiety: Generalized Anxiety Disorder (GAD-2) Panic symptoms: PHQ-PD Social well-being: World Health Organization- Five Well-Being Index (WHO-5) Alcohol and drug addiction: three screening questions derived from the screening questions from the SCID (Structured Clinical Interview) | Research assistant Interpreter available Self-assessment Assessment time not reported |
| Ovitt (2003) [84] | Screening program | Resettlement office or at participants’ homes USA | Post-arrival | Refugees Ages 29–72 yo 50% male Bosnia | Anxiety and depression: The Hopkins Symptom Checklist-25 (HSCL-25) and a client questionnaire | Psychiatrist or medical doctor Interpreter not present Oral interview Assessment time not reported |
| Polcher (2016) [85] | Screening program | Community health centre USA | Post-arrival | Refugees Ages 18 yo or older tijana41% male Bhutan, Iraq, Somalia, Congo, Sudan, Burma, Iran, and Eritrea | Anxiety, depression and PTSD: Refugee Health Screener–15 (RHS-15) | Administered by trained interpreters and medical assistants Interpreter present Oral interview 10–15 min |
| Poole (2020) [86] | Validation study | Refugee camp Greece | In transition | Refugees Mean age 30 years, range 18–61. 59% male Syria | Major Depressive Disorder (MDD): Patient Health Questionnaires (PHQ-2 and PHQ-8) | Administered by research personnel Arabic-English interpreter present Oral interview Assessment time not reported |
| Rasmussen (2015) [87] | Validation study | Primary care clinic USA | Post-arrival | Asylum seekers Mean age 34.9 yo 59% male West Africa, Himalayan Asia, and Central Africa | PTSD: Harvard Trauma Questionnaire (HTQ) | Administered by trained interpreters Interpreter present Oral interview Assessment time not reported |
| Richter (2015) [88] | Screening program | Central reception facilities Germany | Post-arrival | Asylum seekers Mean age 31.9 years old, SD 10.6 66.8% male Iran, Russia, Afghanistan, and Iraq | General psychiatric assessment: Structured diagnostic interview MINI-International Neuropsychiatric Interview (MINI-Plus) Essen Trauma Inventory (ETI) Brief Symptom Inventory (BSI) Montgomery-Asberg Depression Scale (MADRS) WHO-5 Pittsburgh Sleep Quality Index (PSQI) | Administered by a physician Interpreter present Oral interview 3 h (two 1.5 h sessions) |
| Salari (2017) [89] | Validation study | Primary care clinic Sweden | Post-arrival | Refugees Ages 9–18 97.6% male Majority from Afghanistan. Others from Iran, Syria, Iraq, Pakistan, Somalia, Eritrea, Ethiopia, Libya, and Lebanon | PTSD: Children’s Revised Impact of Event Scale (CRIES-8) | Clinicians and nurses Interpreter present if needed Self-assessment Assessment time not reported |
| Savin (2005) [90] | Screening program | Primary care clinic USA | Post-arrival | Refugees Ages 18 years old and over (mean age 27.4) 51.5% male 24 countries of origin: most frequently Bosnia, Russia, Ukraine, Sudan, Somalia, Ethiopia, Afghanistan, Burma, Vietnam, Iran, and Iraq | PTSD, anxiety, depression: 25-item psychiatric symptom checklist derived from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) | Administered by a team composed of a case manager from a publicly funded resettlement agency, a primary care nurse experienced with culturally diverse populations, a primary care physician, and if needed, a psychologist or psychiatrist. Nurses primarily administered the screening tool Interpreter present Oral interview Assessment time not reported |
| Schweitzer (2011) [91] | Screening program | Settlement service Australia | Post-arrival | Refugees Mean age 34.13 yo (range 18–80 yo) 43.9% male Burma | Pre-migration trauma: HTQ Depression, anxiety, somatization: Hopkins Symptom Checklist-37 (HSCL-37) Post-migration stressors: Post-migration Living Difficulties Checklist | Researchers and counsellors Interpreter present Oral interview 2–3 h |
| Seagle (2019) [92] | Screening program | Outpatient clinics USA | Post-arrival | Administrative sample, 64% refugees Age 14 years and older 42.6% male Cuba, Burma, Afghanistan, Bhutan, Iraq, Somalia, Iran, Ethiopia, Syria | Not reported; however, the authors state that clinicians may consider the use of the Refugee Health Screener-15 (RHS-15), Harvard Trauma Questionnaire (HTQ), Vietnamese Depression Scale (VDS), New Mexico Refugee Symptom Checklist 121 (NMRSCL-121), and the Hopkins Symptom Checklist 25 (HSCL-25) Georgia public health officials recommend use of the RHS-15 | Administered by clinicians Interpreter present Self-assessment and oral interview Time of assessment was variable |
| Shannon (2015) [93] | Screening program | Primary care clinic USA | Post-arrival | Refugees Mean age 35.27 51.4% male Burma | PTSD, distress, somatic complaints, depression: unspecified 32-item questionnaire | Administered by trained research staff Interpreter present Self-assessment 45 min |
| Sondergaard (2001) [94] | Screening program | Reception centre Sweden | Post-arrival | Refugees Ages 18–48, mean age 35 yo 63% male Iraq | PTSD: Questionnaire developed uniquely for this study, based on the Holmes-Rahe Life Event Questionnaire | Assessor background not reported Interpreter not present Self-assessment Assessment duration not reported |
| Sondergaard (2003) [95] | Validation study | Reception centre Sweden | Post-arrival | Refugees Ages 18–48, mean age 35 yo 63% male Iraq | Mental health screen using Health Leaflet: Harvard Trauma Questionnaire (HTQ), Impact of Event Scale (IES-22), General Health Questionnaire (GHQ-28), Hopkins Symptoms Checklist (HSCL-25) PTSD: Structured Clinical Interview for DSM Disorders (SCID) or Clinician Administered PTSD Scale for DSM-5 (CAPS) Depression: Hopkins Symptoms Checklist (HSCL-25) | Administered by case manager Interpreter not present Self-assessment Assessment time not reported |
| Stingl (2019) [96] | Screening program | Reception centre (RC) & communal accommodation (CU) Germany | Post-arrival | Refugees Mean age 25.6 (RC), 28.9 (CU) 92.9% (RC), 69.8% (CU) male Afghanistan, Algeria, Ethiopia, Eritrea, Iraq, Iran, Somalia, Syria | Depression, anxiety, and PTSD: Refugee Health Screener (RHS-15) | Administered by doctorate students and a linguist Interpreter present Written Likert-scale 4–12 min |
| Sukale (2017) [97] | Screening program | Clearing and pre-clearing institution Germany | Post-arrival | Refugee minors Age 16.24 years, SD 1.03 100% male Syria, Afghanistan, Iran, Somalia, Sudan, Iraq | Providing Online Resource and Trauma Assessment (PORTA) screening tool, which comprises of disorder-specific questionnaires: Trauma: CATS Depression and Anxiety: Refugee Health Screener (RHS-15) + Patient Health Questionnaire-9 (PHQ-9) Behavioural problems: Strengths and Difficulties Questionnaire Self harm and suicidality: SITBI | Self-administered Interpreter present if needed Online questionnaire via computer (PORTA) 30–90 min |
| Tay (2013) [98] | Screening program | Reception centre Australia | In transition | Asylum seekers Mean age 39 65% male 18 countries- majority from Iran, Ghana, Zimbabwe, Afghanistan, and China | PTSD and depression: Structured Clinical Interview for DSM-IV (SCID) PTSD: Harvard Trauma Questionnaire (HTQ) Depression: Hopkins Symptoms Checklist (HSCL-25) | Assessment by psychologists Interpreter present Oral interview 120 min |
| Thulesius (1999) [99] | Validation study | Asylum centre (refugees) and Healthcare clinic (Swedish comparison group) Netherlands | Post-arrival | Refugees Mean age 33.7 58% male Bosnia-Herzegovina | PTSD and depression: Modified Posttraumatic Symptom Scale (PTSS-10-70) | Assessor background not reported Interpreter not present Self-assessment Assessment time not reported |
| van Os (2018) [100] | Screening program | National intermediary organizations Netherlands | Post-arrival | Refugees and asylum seekers—16 unaccompanied children (15–18 years) and 11 accompanied children (4–16 years) 63% male 44% from Afghanistan | Well-being and child development: Best Interests of the Child (BIC-Q), Strengths and Difficulties Questionnaire (SDQ) Stressful life events: Stressful Life Events (SLE) PTSD: Reactions of Adolescents on Traumatic Stress (RATS) | Assessment by trained professionals Interpreter present Self-assessment and oral interview 180–240 min |
| Van Dijk (1999) [101] | Validation study | Psychiatric hospital Netherlands | Post-arrival | Refugees Mean age 35.7 years, range 17–70 67% male Diverse nationalities (country not specified) | PTSD: Harvard Trauma Questionnaire (HTQ), Hopkins Symptom Check List-90 (HSCL-90), DSM-IV | Administered by psychiatrists and psychological assistants Interpreter present Oral interview Assessment time not reported |
| Vergara (2003) [102] | Screening program | Refugee health program USA | Post-arrival | 26,374 refugees, or 38.1% of all refugees, resettling in the United States during fiscal year 1997 No additional characteristics reported | 3/9 sites offered mental status examinations during the domestic refugee health assessment. Specific mental health conditions and assessment tools not reported | Not reported |
| Weine (1998) [103] | Screening program | Primary care clinic USA | Post-arrival | Refugees Ages 13–59 yo 50% male Bosnia | PTSD: PTSD Symptoms Scale, the Communal Traumatic Experiences Inventory, the Global Assessment of Functioning (DSM-IV), and the Symptoms Checklist 90 (SCL-90-R) | Administered by mental health professionals Interpreter present Oral interview 60–120 min |
| Willey (2020) [104] | Screening program | Refugee antenatal clinic Australia | Post-arrival | Women from a refugee background or considered refugee-like, i.e., arrived in Australia on a spousal visa from a refugee-source country such as Afghanistan | Depression and anxiety: Edinburgh Postnatal Depression Scale (EPDS) Perinatal mental health: Monash Psychosocial Screening Tool | Administered by maternal care staff (midwives, bi-cultural workers) Interpreter present Electronic tablet 10 min |
| Wulfes (2019) [105] | Validation study | Refugee accommodations Germany | Post-arrival | Refugee and asylum seekers Ages 17–90 yo, average age 32.9 64.4% male Syria, Iraq, Afghanistan, Iran, Sudan | 1. Posttraumatic stress screening: PQ 2. Traumatic events: a list of events that was modified from those included in the Posttraumatic Diagnostic Scale (PDS) 3. Posttraumatic stress symptoms: PDS-8 4. Depression: Patient Health Questionnaire 9 (PHQ-9) 5. Axis I disorders: Structured Clinical Interview for DSM Disorders (SCID) | Administered by staff without medical or psychological health training I nterpreter not present Self-assessment Assessment time not reported |
| Yalim (2021) [106] | Screening program | Refugee resettlement agency/home visit USA | Post-arrival | Refugees Aged 18 years and older (mean age 36.38 years, SD 12.5) Majority from Democratic Republic of Congo, Iraq, Syria, and Eritrea | PTSD, depression, anxiety: Refugee Health Screener (RHS-15) | Administered by research personnel Interpreter present Oral interview or self-assessment, depending on the literacy level of the participant 20–30 min |
| Young (2016) [107] | Screening program | Detention centres Australia | Post-arrival | Asylum seekers and refugees (detainees) All ages 73% male | Depression, anxiety, and PTSD: Self-rated Kessler 10 (K-10) The Harvard Trauma Questionnaire (HTQ) The Clinician-rated Health of the Nation Outcome Scores (HoNOS) The Clinician-rated Health of the Nation Child and Adolescent Outcome Scores (HoNOSCA) | Administered by mental health professionals (nurse or psychologist) Interpreter present Self-assessment Assessment time not reported |
| Screening Tool | Studies | Mental Health Conditions Assessed | Administrator | Languages | |
|---|---|---|---|---|---|
| 1 | Family Peer Relationship Questionnaire, Arabic version (A-FPRQ) | El Ghaziri 2019 | OTHER | unspecified | unspecified |
| 2 | Unaccompanied Migrant Minors Questionnaire (AEGIS-Q) | Di Pietro 2020 | OTHER | unspecified | unspecified |
| 3 | Al-Obaidi et al. DSM-based non-validated questionnaire | Al-Obaidi 2015 | Depression, PTSD | Master’s level social worker | unspecified |
| 4 | Arab Acculturation Scale | LeMaster 2018 | PTSD, Depression, OTHER | unspecified | unspecified |
| 5 | Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) | El Ghaziri 2019 | Substance Use Disorder | unspecified | unspecified |
| 6 | Best Interests of the Child (BIC-Q) | van Os 2018 | Disruptive Behaviour Disorders, Depression | unspecified | Arabic, Dari, Farsi, Somali |
| 7 | Brief Symptom Inventory-18 (BSI-18) | Kaltenbach 2017 Richter 2015 | Depression, PTSD, Somatoform Disorders | unspecified | Albanian, Arabic, Farsi, Kurdish, Russian, Serbian, Somali |
| 8 | Child Behaviour Checklist (CBCL) | Nehring 2021 | PTSD | MHS | German |
| 9 | Child Health Questionnaire (CHQ) | Geltman 2005 | OTHER | Community health worker (CHW) | English |
| 10 | Children’s Revised Impact of Event Scale (CRIES-8) | Salari 2017 | PTSD | Primary care provider (PCP) | Arabic, Dari, Farsi, Kurdish/Sorani, Swedish |
| 11 | Communal Traumatic Experiences Inventory (CTEI) | Weine 1998 | PTSD, Depression | Mental health specialist (MHS), PCP, lay person (LAY) | Croatian |
| 12 | Cook et al. author-developed interview | Cook 2015 | OTHER | Research assistants trained Master’s or Ph.D. level social work students | unspecified |
| 13 | Digital Communication Assistance Tool (DCAT) | Kleinert 2019 | PTSD, Depression, Anxiety, Substance Use Disorder, Disruptive Behaviour Disorders, Somatoform Disorders, OTHER | Self-assessment, PCP | Modern Standard Arabic, Arabic Syrian, Arabic Egyptian, Arabic Tunisian, Arabic Moroccan, Turkish, Persian, Kurdish Sorani, Kurdish Kurmanji, Kurdish Feyli, Pashto Kandahari, Pashto Mazurka |
| 14 | Edinburgh Postnatal Depression Scale (EPDS) | Boyle 2019 Willey 2020 | Depression | MHS, PCP, CHW, LAY | unspecified |
| 15 | Essen Trauma Inventory (ETI) | Richter 2015 | Trauma | MHS | German |
| 16 | Eytan et al. (2002) author-developed interview | Eytan 2002 | Health Conditions, Presence of Symptoms and Previous Exposure to Trauma | Nurses | French, German, Italian, Spanish, Portuguese, English |
| 17 | Family Assessment Device (FAD) | El Ghaziri 2019 | OTHER | unspecified | unspecified |
| 18 | Geltman et al. author-developed ad-hoc assessment | Geltman 2005 | Emotionally Traumatic Exposures | Staff from local URMO agencies | English |
| 19 | Generalized Anxiety Disorder 7 (GAD-7) | Bjarta 2018 | Anxiety | MHS, PCP, CHW | Arabic, Dari |
| 20 | GB | El Ghaziri 2019 | OTHER | unspecified | unspecified |
| 21 | General Health Questionnaire (GHQ-28) | Sondergaard 2003 | Depression | Self-rating | unspecified |
| 22 | Global Assessment of Functioning Scale (DSM-IV) | Weine 1998 | OTHER | MHS, PCP, CHW | Croatian |
| 23 | Global Mental Health Assessment Tool (GMHAT) | Hough 2019 | Anxiety, Depression, Substance Use Disorders, Disruptive Behaviour Disorders | PCP, MHS | English, Arabic |
| 24 | Hospital Anxiety and Depression Scale (HADS) | Arnetz 2014 LeMaster 2018 | Anxiety, Depression | CHW | Arabic |
| 25 | Hassles Scale | LeMaster 2018 | OTHER | CHW | unspecified |
| 26 | Home, Education/Eating, Activities, Drugs, Sexuality, Suicide/mental health (HEADSS) Questionnaire | Hirani 2016 | OTHER | unspecified | English |
| 27 | Health Leaflet (HL) | Sondergaard 2003 | PTSD | Self-assessment | unspecified |
| 28 | Kennedy et al. author-developed tool | Kennedy 1999 | Depression, Anxiety, PTSD | Self-assessment | unspecified |
| 29 | Clinician-rated Health of the Nation Outcome Scores (HoNOS) | Young 2016 | Depression, Substance Use Disorders, Disruptive Behaviour Disorders | MHS, PCP | unspecified |
| 30 | Clinician-rated Health of the Nation Child and Adolescent Outcome Scores (HoNOSCA) | Young 2016 | Depression, Substance Use Disorders, Disruptive Behaviour Disorders | MHS, PCP | unspecified |
| 31 | Hopkins Symptom Checklist-25 (HSCL-25) | Jakobsen 2017 Javanbakht 2019 Kleijn 2001 Ovitt 2003 Schweitzer 2011 Sondergaard 2003 Tay 2013 Van Dijk 1999 | Anxiety, Depression | MHS, PCP, CHW | Arabic, Farsi, Russian, Bosnian-Serbo-Croatian |
| 32 | Harvard Trauma Questionnaire (HTQ) | Arnetz 2014 Bertelsen 2018 Churbaji 2020 Geltman 2005 Jakobsen 2017 Kleijn 2001 LeMaster 2018 Rasmussen 2015 Schweitzer 2011 Sondergaard 2003 Tay 2013 Young 2016 Van Dijk 1999 | PTSD | MHS, PCP, CHW | Arabic, Cambodian, Dutch, English, Farsi, French, Laotian, Russian, Serbo-Croatian, Vietnamese |
| 33 | Impact of Event Scale (IES-22) | Sondergaard 2003 | Trauma | Self-rating | unspecified |
| 34 | Interpersonal Support Evaluation Checklist (ISEL) | LeMaster 2018 | OTHER | CHW | unspecified |
| 35 | ICD-11 International Trauma Questionnaire (ITQ) | Barbieri 2019 | PTSD | MHS, PCP, CHW | Arabic, English, French |
| 36 | Kaltenbach et al. author-developed questionnaire | Kaltenbach 2017 | Daily Functioning | Clinical psychologists | unspecified |
| 37 | Karen Mental Health Screener | Brink 2016 | PTSD, Depression | PCP | Karenic |
| 38 | Self-rated Kessler 10 (K-10) | Lillee 2015 Young 2016 | OTHER | Self-administered (SA) | English, Kurdish, Pashto |
| 39 | Life Events Checklist (LEC-5) | Kaltenbach 2017 | OTHER | unspecified | Arabic, Albanian, Farsi, Kurdish, Russian, Serbian, Somali |
| 39 | Loutan et al. author-developed questionnaire | Loutan 1999 | Anxiety, Depression, PTSD, and Traumatic Events | Nurse | French, English, Italian, Spanish and German |
| 40 | Multi-Adaptive Psychological Screening Software (MAPSS) | Morina 2017 | Depression, PTSD | MHS, PCP | Arabic, Farsi, Tamil, Turkish |
| 41 | Mini International Neuropsychiatric Interview (MINI) | Churbaji 2020 Durieux-Paillard 2006 El Ghaziri 2019 Eytan 2007 Kaltenbach 2017 Richter 2015 | Depression, Anxiety, Substance Use Disorders, Disruptive Behaviour Disorders, PTSD, Somatoform Disorders | MHS, PCP | 70+ languages |
| 42 | Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) | El Ghaziri 2019 | Depression, Anxiety, Substance Use Disorders, Disruptive Behaviour Disorders, PTSD, Somatoform Disorders | MHS, PCP | 70+ languages |
| 43 | Monash Health Psychosocial Needs Assessment (Psychosocial Screening Tool) | Boyle 2019 Willey 2020 | OTHER | MHS, PCP, CHW, LAY, Self-administered | unspecified |
| 44 | Montgomery-Asberg Depression Scale (MADRS) | Richter 2015 | Depression | MHS, PCP | unspecified |
| 45 | Multidimensional Scale of Perceived Social Support (MSPSS) | El Ghaziri 2019 | OTHER | MHS, PCP, CHW | unspecified |
| 46 | Nikendei et al. author-developed interviews | Nikendei 2019 | Substance Use | Research personnel | English, German, French, Persian, Arabic, Turkish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 47 | Ovitt et al. author-developed client questionnaire | Ovitt 2003 | OTHER | ||
| 48 | Primary Care PTSD-4 (PC-PTSD-4) | Bjarta 2018 | PTSD | MHS, PCP, CHW, LAY, SA | Arabic, Dari |
| 49 | PC-PTSD-5 | Nikendei 2019 | PTSD | Trained research assistants | English, German, French, Persian, Arabic, Turkish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 50 | PTSD Checklist for DSM-5 (PCL-5) | Barbieri 2019 Kaltenbach 2017 | PTSD | MHS, PCP | Arabic, Albanian, Farsi, Kurdish, Russian, Serbian, Somali |
| 51 | Civilian version of the PTSD Checklist (PCL-C) | Arnetz 2014 Javanbakht 2019 LeMaster 2018 | PTSD | CHW | Arabic |
| 52 | Posttraumatic Diagnostic Scale (PDS) | Kroger 2016 Mewes 2018 Wulfes 2019 | PTSD | MHS, Self-assessment | German, Arabic, Persian, Kurdish, Turkish, English |
| 53 | Patient Health Questionnaire (PHQ-2) | Kroger 2016 Nikendei 2019 Poole 2020 | Depression | Trained research assistants | English, German, French, Persian, Arabic, Turkish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 54 | Patient Health Questionnaire (PHQ-8) | Poole 2020 | Depression | Research personnel | |
| 55 | Patient Health Questionnaire (PHQ-9) | Bertelsen 2018 Bjarta 2018 Churbaji 2020 Mewes 2018 Wulfes 2019 | Depression | MHS, PCP, Self-assessment | Arabic, Dari, Farsi, English, Kurdish |
| 56 | Patient Health Questionnaire—Panic Disorders (PHQ-PD) | Nikendei 2019 | Panic Symptoms | Trained research assistants | English, German, French, Persian, Arabic, Turkish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 57 | Parentification Inventory (PI) | El Ghaziri 2019 | OTHER | MHS, PCP, CHW | unspecified |
| 58 | Post-Migration Living Difficulties Checklist (PMLDC) | Schweitzer 2011 | OTHER | CHW | unspecified |
| 59 | Process of Recognition and Orientation of Torture Victims in European Countries to Facilitate Care and Treatment (PROTECT) Questionnaire | Mewes 2018 Wulfes 2019 | PTSD, Depression | MHS, PCP, LAY | English, German, Farsi, French, Persian, Arabic, Turkish, Kurdish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 60 | Present State Examination (PSE) | Hauff 1995 | PTSD, psychiatric disorders | The first author | unspecified |
| 61 | Providing Online Resource and Trauma Assessment’ (PORTA) | Sukale 2017 | Trauma, Depression, Anxiety, Behavioural Problems, Self- Harm/Suicidality | Self-administered | German, English, French, Arabic, Dari/Farsi, Pashto, Tigrinja, Somali |
| 62 | PTSD Symptoms Scale (PSS) | Weine 1998 | PTSD | MHS, CHW, LAY | Croatian |
| 63 | Posttraumatic Symptom Scale (PTSS-10-70) | Thulesius 1999 | PTSD | unspecified | English, Serbo-Croatian |
| 64 | Reactions of Adolescents on Traumatic Stress (RATS) | van Os 2018 | PTSD | unspecified | Arabic, Dari, Farsi, Somali |
| 65 | Resilience Scale | LeMaster 2018 | OTHER | CHW | unspecified |
| 66 | Refugee Health Screener-13 (RHS-13) | Bjarta 2018 Kaltenbach 2017 | Depression, Anxiety, SOM, PTSD, OTHER | MHS | Amharic, Arabic, Albanian, Burmese, Cuban Spanish, Farsi, French, Haitian Creole, Karen, Kurdish, Mexican Spanish, Nepali, Russian, Spanish, Serbian, Somali, Swahili, Tigrinya |
| 67 | Refugee Health Screener-15 (RHS-15) | Al-Obaidi 2015 Baird 2020 Hollifield 2013 Hollifield 2016 Johnson-Agbakwu 2014 Kaltenbach 2017 Polcher 2016 Stingl 2019 Yalim 2020 | Depression, Anxiety, Somatoform Disorders, PTSD, OTHER | MHS, PCP, CHW | Amharic, Arabic, Albanian, Burmese, Cuban, English, Farsi, French, Haitian Creole, Karen, Kurdish, Mexican Spanish, Nepali, Russian, Spanish, Serbian, Somali, Swahili, Tigrinya |
| 68 | Refugee Trauma History Checklist (RTHC) | Sigvardsdotter 2017 | OTHER | MHS, PCP | English, Arabic |
| 69 | Savin et al. author-developed checklist derived from the DSM-IV | Savin 2005 | Depression, Anxiety, PTSD | PCP, MHS | English |
| 70 | S-DAS | El Ghaziri 2019 | Disruptive Behaviour Disorders, OTHER | MHS, PCP, CHW | unspecified |
| 71 | Structured Clinical Interview for DSM-IV (SCID) | Brink 2016 Tay 2013 Wulfes 2019 | Depression, Anxiety, PTSD, Substance Use Disorders, Disruptive Behaviour Disorders, Somatoform Disorders | MHS, PCP | Danish, French, German, Greek, Hebrew, Karen, Italian, Portuguese, Spanish, Swedish, Turkish, Zulu |
| 72 | SCL-90-R | Hauff 1995 Weine 1998 | Depression, Anxiety, Somatoform Disorders, Disruptive Behaviour Disorders, OTHER | MHS, PCP, CHW | Croatian |
| 73 | Strength and Difficulty Questionnaire (SDQ) | Green 2021 Hanes 2017 van Os 2018 | OTHER | CHW, LAY | 75+ languages |
| 74 | SF-10 | El Ghaziri 2019 | Depression, Anxiety, Disruptive Behaviour Disorders | MHS, PCP, CHW | unspecified |
| 75 | SF-12 | El Ghaziri 2019 | Depression, Anxiety, Disruptive Behaviour Disorders | MHW, PCP, CHW | unspecified |
| 76 | Shannon et al. author-developed questionnaire | Shannon 2015 | Depression, PTSD, OTHER | Master’s-level and doctoral-level research assistant, professional Karen interpreters | English and Karen |
| 77 | Stressful Life Events (SLE) | van Os 2018 | OTHER | unspecified | Arabic, Dari, Farsi, Somali |
| 78 | Sondergaard et al. (2001) author-developed questionnaire | Sondergaard 2001 | PTSD, Anxiety, Depression, OTHER | Professionals working with refugees | Arabic and Sorani |
| 79 | STAR-MH | Hocking 2018 | Depression, PTSD | CHW | English |
| 80 | Trauma Exposure Questionnaire by Nickerson et al. | Barbieri 2019 | PTSD | PCP | Arabic, English, French |
| 81 | Vietnamese Depression Scale (VDS) | Buchwald 1995 | Depression | PCP | Vietnamese |
| 82 | WHO-5 | Nikendei 2019 Richter 2015 | Social Well-Being | LAY, MHS, PCP | English, German, French, Persian, Arabic, Turkish, Kurmanji (Northern Kurdish), Urdu, Hausa, Russian, Serbian, Albanian, Macedonian, Georgian, Mandinka, Tigrinya |
| 83 | WHO General Health Questionnaire | Masmas 2008 | Psychological Health Status | PCP, MHS | unspecified |
| 84 | World Health Organization Quality of Life Brief Version (WHOQOL-Bref) | Bjarta 2018 | OTHER | MHS, PCP, CHW, LAY, SA | 28 languages (who.int) |
| 85 | World Health Organization PTSD screener | Lillee 2015 | PTSD | unspecified | English, Kurdish, Pashto |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magwood, O.; Kassam, A.; Mavedatnia, D.; Mendonca, O.; Saad, A.; Hasan, H.; Madana, M.; Ranger, D.; Tan, Y.; Pottie, K. Mental Health Screening Approaches for Resettling Refugees and Asylum Seekers: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 3549. https://doi.org/10.3390/ijerph19063549
Magwood O, Kassam A, Mavedatnia D, Mendonca O, Saad A, Hasan H, Madana M, Ranger D, Tan Y, Pottie K. Mental Health Screening Approaches for Resettling Refugees and Asylum Seekers: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(6):3549. https://doi.org/10.3390/ijerph19063549
Chicago/Turabian StyleMagwood, Olivia, Azaad Kassam, Dorsa Mavedatnia, Oreen Mendonca, Ammar Saad, Hafsa Hasan, Maria Madana, Dominique Ranger, Yvonne Tan, and Kevin Pottie. 2022. "Mental Health Screening Approaches for Resettling Refugees and Asylum Seekers: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 6: 3549. https://doi.org/10.3390/ijerph19063549