
Nursing Students’ Retention of Knowledge by Basic Knowledge Type: An Exploratory Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment
2.3. Data Collection
2.4. Class Contents
2.4.1. Second-Year Class (Health Management) Contents
- To understand the environmental conditions necessary for a normal life;
- To develop an interest in assessments involving an individual’s environment;
- To be able to suggest ways to prevent health issues.
One day in June, while the students were attending a lecture, an evacuation order was issued by Hiroshima City at 15:00 because heavy rains had caused the river near the university to swell above dangerous levels (bank-full stage). Residents had already evacuated to the university’s gymnasiums. The students evacuated to the gymnasium of a junior high school neighboring the university, where each person was given a bottle of mineral water (500 mL) and a blanket. The windows could not be opened because of heavy rains, and the lights went out due to the power outage. The shelter temperature/humidity was 28 °C/90%.
2.4.2. Third-Year Class (Community Health) Contents
- To understand different forms of health crisis management (HCM) and their associated conditions;
- To be interested in the systems used in HCM;
- To think about the different ways in which disaster-related damage can be addressed by HCM.
- Designing initial crisis-response systems: (i) ascertaining the situation, (ii) helping residents make informed decisions, and (iii) participating in relief efforts;
- Explaining the criteria for someone in urgent need of care and ways to treat or manage them;
- Developing strategies to enhance residents’ abilities to help themselves and others;
- Taking systematic approaches to health management for employees in disaster-stricken areas;
- Designing systems for continually adjusting areas where support and dispatched personnel are stationed.
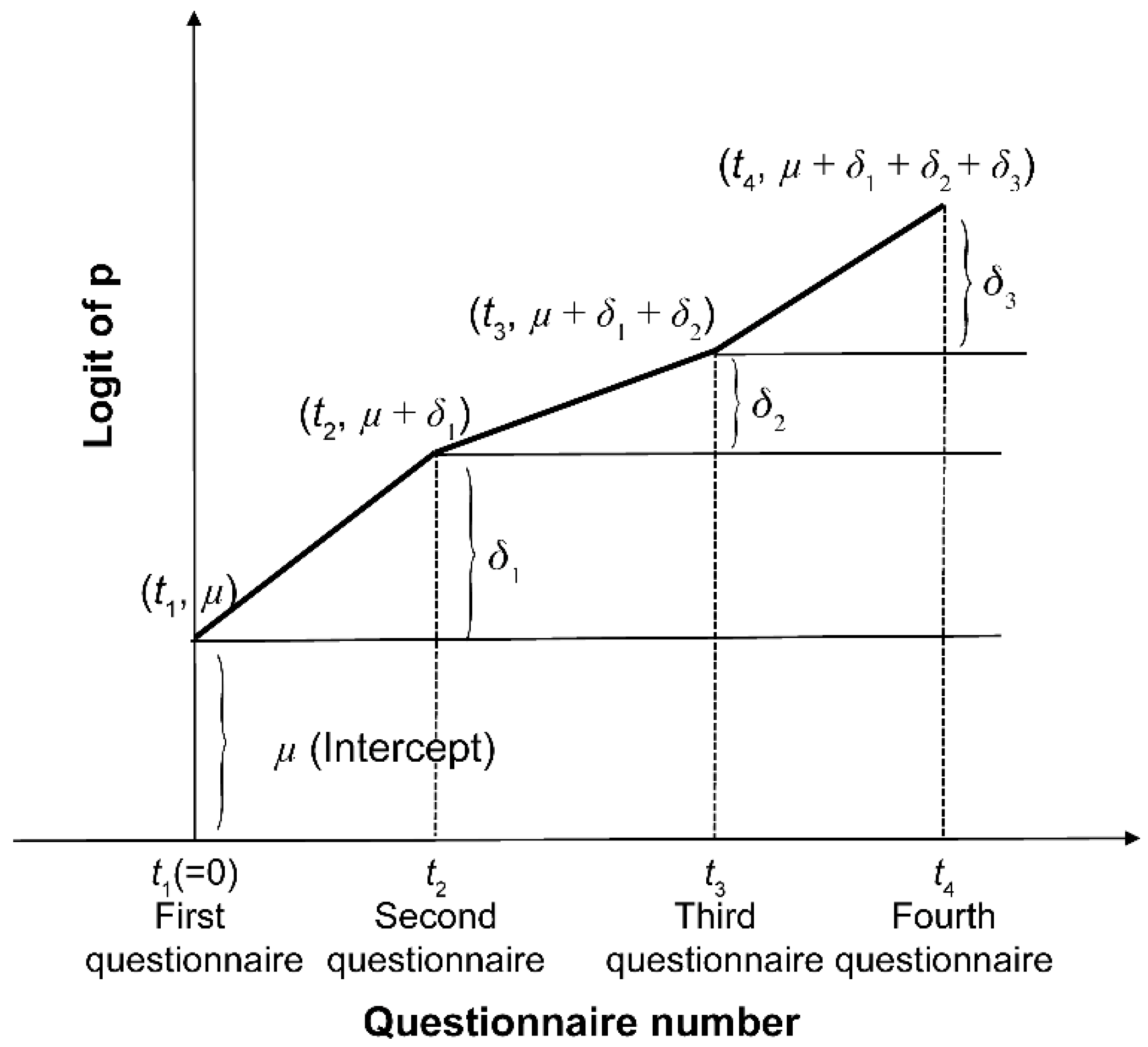
2.5. Analysis Method
2.6. Ethical Considerations
3. Results
- Pattern #1 (the item’s eCAR was higher on the second questionnaire than on the first);
- Pattern #2 (the item’s eCAR was lower in the second questionnaire than the first but higher in the third, a year later);
- Pattern #3 (the item’s eCAR was minimally variable across the four assessment points).
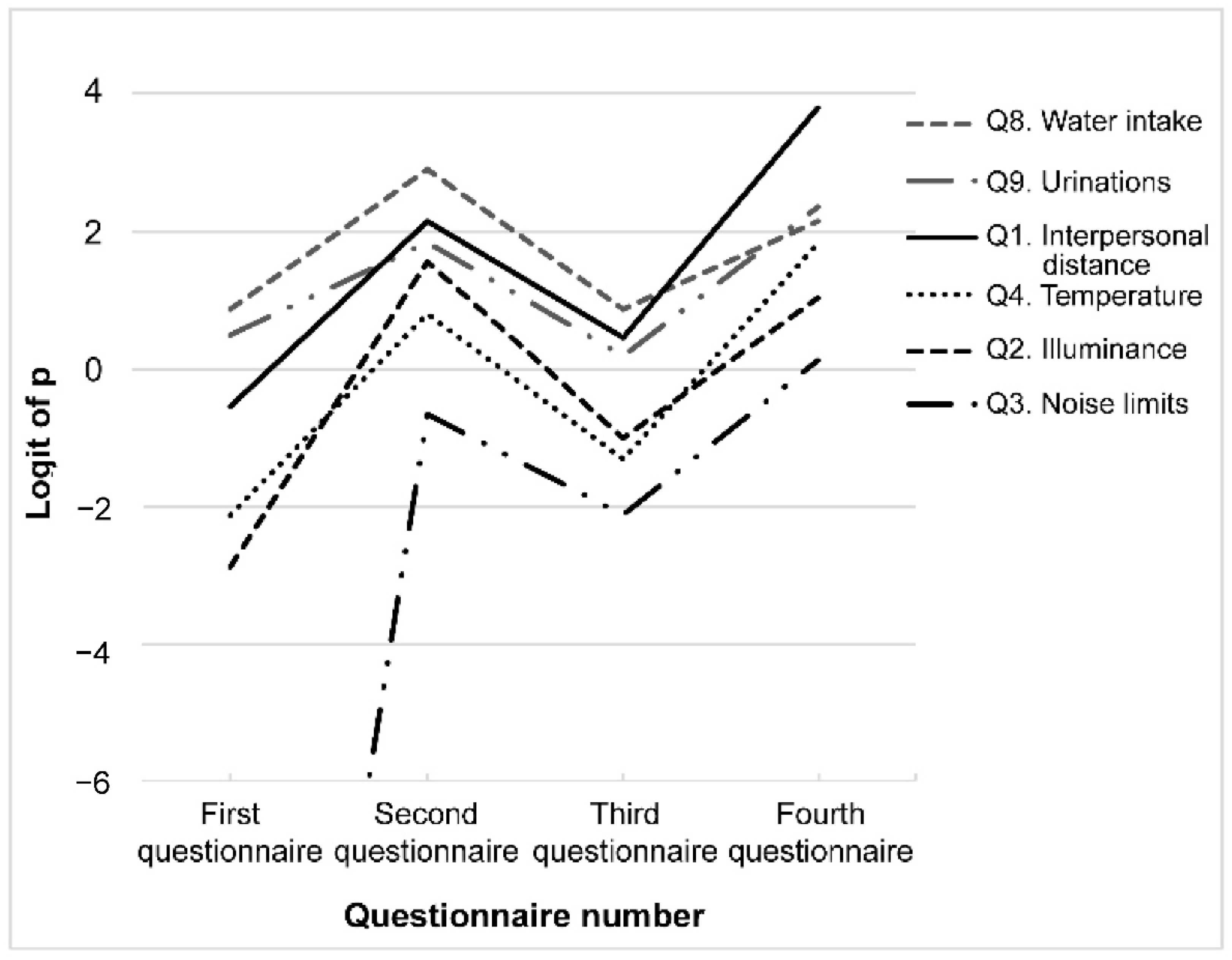
3.1. Pattern #1: eCAR Increased after the First Class (Second > First)
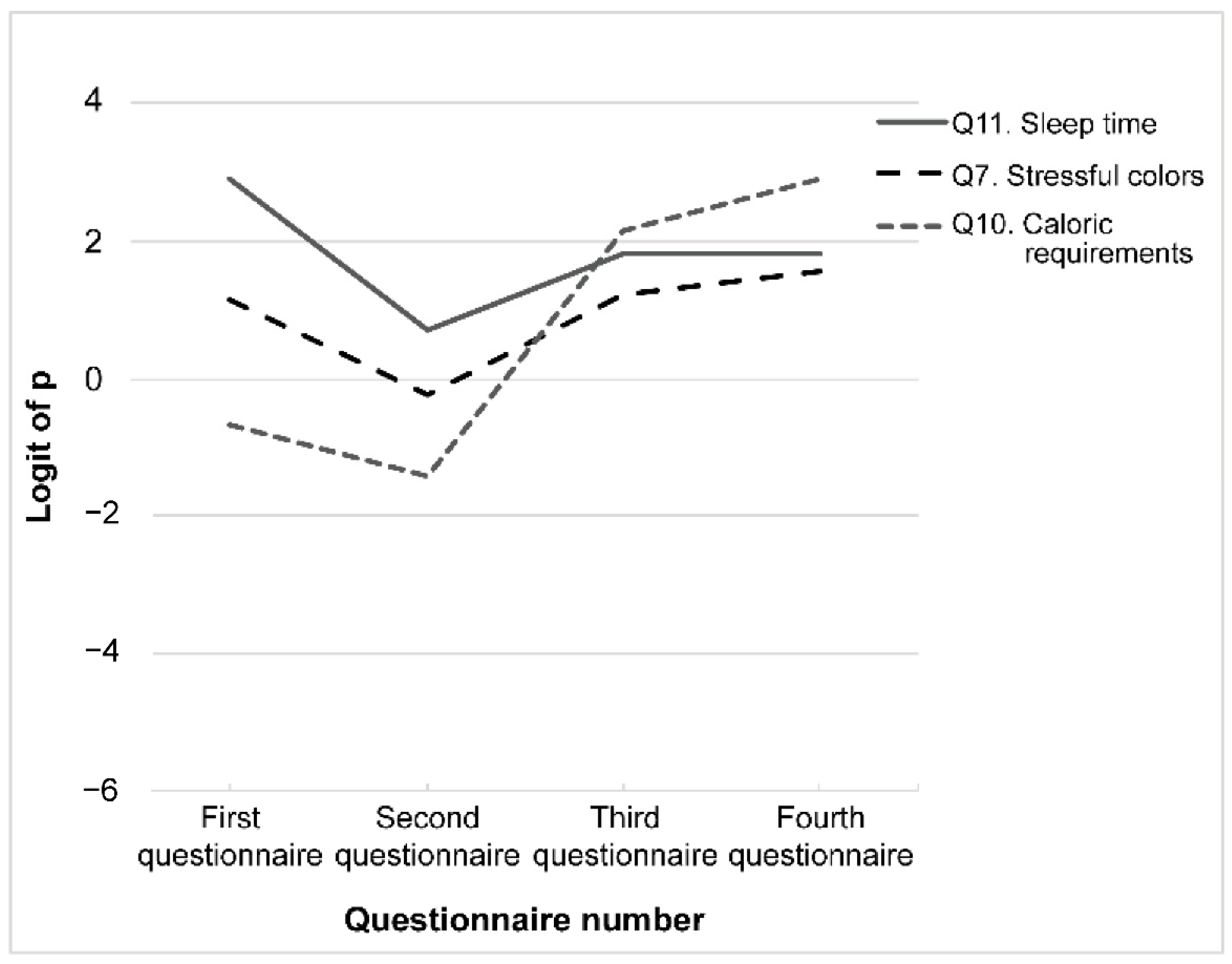
3.2. Pattern #2: eCAR Decreased after the First Class but Increased a Year Later (Third > Second < First)
3.3. Pattern #3: Minimal Variation over Time
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoeve, Y.T.; Jansen, G.; Roodbol, P. The nursing profession: Public image, self-concept and professional identity. J. Adv. Nurs. 2014, 70, 295–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Nursing Association. Nursing Clinical Ladder. Tokyo: Japanese Nursing Association. 2016. Available online: https://www.nurse.or.jp/home/publication/pdf/fukyukeihatsu/jissen.pdf (accessed on 19 May 2021).
- McCollum, M.; Kovner, C.T.; Ojemeni, M.T.; Brewer, C.; Cohen, S. Nurses Improve Their Communities’ Health Where They Live, Learn, Work, and Play. Policy Politics Nurs. Pract. 2017, 18, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Logrippo, M.T.; Brienza-Arcilla, D.; Raoji, N.V.; Polakowski, J. A call to act: RN volunteers needed in their communities. Public Health Nurs. 2020, 37, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Fukada, M. Nursing Competency: Definition, Structure and Development. Yonago Acta Med. 2018, 61, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, E.M.; De Bruin, A.B.; Herrler, A.; Verheijen, I.W.; Scherpbier, A.J.; Van Der Vleuten, C.P. Students’ perceptions of anatomy across the undergraduate problem-based learning medical curriculum: A phenomenographical study. BMC Med. Educ. 2013, 13, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.; Cardoso, A.P.; Abrantes, J.L. Motivation and Relationship of the Student with the School as Factors Involved in the Perceived Learning. Procedia Soc. Behav. Sci. 2011, 29, 1707–1714. [Google Scholar] [CrossRef] [Green Version]
- Aguilera-Hermida, A.P. College students’ use and acceptance of emergency online learning due to COVID-19. Int. J. Educ. Res. Open 2020, 1, 100011. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.M. Development and use of the ARCS model of instructional design. J. Instr. Dev. 1987, 10, 2–10. [Google Scholar] [CrossRef]
- Ho, Y.Y.; Lim, W.Y.R. Educating Adult Learners: Bridging Learners’ Characteristics and the Learning Sciences. In Diversity and Inclusion in Global Higher Education; Sanger, C.S., Gleason, N.W., Eds.; Palgrave Macmillan: Singapore, 2020; pp. 97–115. [Google Scholar] [CrossRef] [Green Version]
- Paul, J.; Jefferson, F. A Comparative Analysis of Student Performance in an Online vs. Face-to-Face Environmental Science Course from 2009 to 2016. Front. Comput. Sci. 2019, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Sela, Y.; Grinberg, K.; Shapiro, Y.; Nissanholtz-Gannot, R. A cross-sectional study on preferred employment settings of final-year nursing students in Israel. Hum. Resour. Health 2020, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Hiromi, K.; Rahman, M.; Mika, I.; Chieko, K. Effectiveness of a Basic Education Program on Radiation Related Health Concerns for Nurses of Public Health and School Health in Japan. Iran. J. Public Health 2020, 49, 6. [Google Scholar] [CrossRef]
- Kawasaki, H.; Yamasaki, S.; Masuoka, Y.; Iwasa, M.; Fukita, S.; Matsuyama, R. Remote Teaching Due to COVID-19: An Exploration of Its Effectiveness and Issues. Int. J. Environ. Res. Public Health 2021, 18, 2672. [Google Scholar] [CrossRef] [PubMed]
- Sphere Association. The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response, 4th ed.; Sphere Association: Geneva, Switzerland, 2018; Available online: https://spherestandards.org/wp-content/uploads/Sphere-Handbook-2018-EN.pdf (accessed on 12 April 2022).
- Schretlen, D.J.; Munro, C.A.; Anthony, J.C.; Pearlson, G.D. Examining the range of normal intraindividual variability in neuropsychological test performance. J. Int. Neuropsychol. Soc. 2003, 9, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Siegelman, N.; Bogaerts, L.; Frost, R. Measuring individual differences in statistical learning: Current pitfalls and possible solutions. Behav. Res. Methods 2017, 49, 418–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 18 February 2022).
- Murre, J.M.J.; Dros, J. Replication and Analysis of Ebbinghaus’ Forgetting Curve. PLoS ONE 2015, 10, e0120644. [Google Scholar] [CrossRef]
- Maniago, J.D.; Feliciano, E.E.; Santos, A.M.; Agunod, C.L.; Adolfo, C.S.; Vasquez, B.A.; Albougami, A.; Almazan, J.U. Barriers in performing physical assessment among nursing students: An integrative review. Int. J. Nurs. Sci. 2021, 8, 120–129. [Google Scholar] [CrossRef]
- Jung, C.-C.; Chen, N.-T.; Hsia, Y.-F.; Hsu, N.-Y.; Su, H.-J. Influence of Indoor Temperature Exposure on Emergency Department Visits Due to Infectious and Non-Infectious Respiratory Diseases for Older People. Int. J. Environ. Res. Public Health 2021, 18, 5273. [Google Scholar] [CrossRef]
- Kim, J.S.; Gu, M.O.; Chang, H. Effects of an evidence-based practice education program using multifaceted interventions: A quasi-experimental study with undergraduate nursing students. BMC Med. Educ. 2019, 19, 71. [Google Scholar] [CrossRef]
- Tlali, T.V.; Baliyan, S.P. Gender, Age and Faculty Differences in Learning Practices among Undergraduates at the National University of Lesotho: Way Forward to Improve Learning. Creat. Educ. 2021, 12, 2253–2276. [Google Scholar] [CrossRef]
- Ashcroft, T.J.; Lutfiyya, Z.M. Nursing educators’ perspectives of students with disabilities: A grounded theory study. Nurse Educ. Today 2013, 33, 1316–1321. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Question ID (Shorthand) | Question [Unit] |
|---|---|---|
| Reference values: Interpersonal environment | Q1 (interpersonal distance) | How much distance should be maintained in interpersonal interactions (in public or social settings)? [m] |
| Q2 (illuminance) | How bright should patients’ rooms be in a hospital ward? Please give respective values for daytime and nighttime in lux. [lx] | |
| Q3 (noise limits) | What are the reference levels for community noise in the daytime and nighttime? Please give each value in decibels. [dB] | |
| Q4 (temperature) | What temperature should be maintained indoors in the summer ensure comfort? [°C] | |
| Q5 (humidity) | What humidity should be maintained indoors in the summer ensure comfort? [%] | |
| Reference values: Physiological/internal | Q6 (discomfort index) | In terms of discomfort index, above what value is perceived as uncomfortable? |
| Q7 (stressful colors) | Which colors provoke stress? | |
| Q8 (water intake) | How much water does a person need per day? [mL/d] | |
| Q9 (urinations) | How many times does a person urinate per day? [times/d] | |
| Q10 (caloric requirements) | How many calories does a person need per day, that is, what is their Estimated Energy Requirement? Write the value for a young adult male or female in their 20s of (physical) activity level II. [kcal/d] | |
| Q11 (sleep time) | How many hours should a person sleep to stay healthy? [h/d] |
| Reference Values | Question | Parameter | Estimate | Standard Error | z Value |
|---|---|---|---|---|---|
| Interpersonal environment | Q1. Interpersonal distance | (Intercept) | −1.030 | 0.301 | −3.423 |
| δ1 | 2.704 | 0.472 | 5.733 *** | ||
| δ2 | −1.709 | 0.450 | −3.801 *** | ||
| δ3 | 3.349 | 0.767 | 4.366 *** | ||
| Q2. Illuminance | (Intercept) | −2.890 | 0.593 | −4.873 | |
| δ1 | 4.438 | 0.688 | 6.452 *** | ||
| δ2 | −2.577 | 0.460 | −5.601 *** | ||
| δ3 | 2.059 | 0.425 | 4.841 *** | ||
| Q3. Noise limits | (Intercept) | −18.566 | 863.945 | −0.021 | |
| δ1 | 17.879 | 863.945 | 0.021 | ||
| δ2 | −1.447 | 0.515 | −2.810 ** | ||
| δ3 | 2.245 | 0.507 | 4.432 *** | ||
| Q4. Temperature | (Intercept) | −2.140 | 0.432 | −4.959 | |
| δ1 | 2.913 | 0.517 | 5.633 *** | ||
| δ2 | −2.095 | 0.432 | −4.848 *** | ||
| δ3 | 3.134 | 0.501 | 6.256 *** | ||
| Q5. Humidity | (Intercept) | −0.176 | 0.266 | −0.601 | |
| δ1 | 1.206 | 0.402 | 3.003 ** | ||
| δ2 | 0.518 | 0.460 | 1.126 | ||
| δ3 | 1.036 | 0.625 | 1.659 | ||
| Physiological /Internal | Q6. Discomfort index | (Intercept) | −4.035 | 1.009 | −3.990 |
| δ1 | 0.711 | 1.239 | 0.574 | ||
| δ2 | 2.373 | 0.778 | 3.051 *** | ||
| δ3 | 0.168 | 0.410 | 0.409 | ||
| Q7. Stressful colors | (Intercept) | 1.122 | 0.308 | 3.647 | |
| δ1 | −1.369 | 0.407 | −3.361 *** | ||
| δ2 | 1.466 | 0.413 | 3.546 *** | ||
| δ3 | 0.328 | 0.470 | 0.699 | ||
| Q8. Water intake | (Intercept) | 0.856 | 0.290 | 2.955 | |
| δ1 | 2.035 | 0.660 | 3.083 ** | ||
| δ2 | −2.035 | 0.660 | −3.083 ** | ||
| δ3 | 1.284 | 0.520 | 2.471 * | ||
| Q9. Urination | (Intercept) | 0.464 | 0.272 | 1.707 | |
| δ1 | 1.348 | 0.468 | 2.878 ** | ||
| δ2 | −1.637 | 0.465 | −3.520 *** | ||
| δ3 | 2.166 | 0.538 | 4.023 *** | ||
| Q10. Caloric requirements | (Intercept) | −0.693 | 0.281 | −2.467 | |
| δ1 | −0.738 | 0.438 | −1.685 | ||
| δ2 | 3.571 | 0.547 | 6.531 *** | ||
| δ3 | 0.750 | 0.734 | 1.023 | ||
| Q11. Sleep time | (Intercept) | 2.890 | 0.593 | 4.873 | |
| δ1 | −2.197 | 0.656 | −3.348 *** | ||
| δ2 | 1.119 | 0.474 | 2.363 * | ||
| δ3 | 3.440 × 10−16 | 0.539 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawasaki, H.; Yamasaki, S.; Fukita, S.; Iwasa, M.; Iki, T. Nursing Students’ Retention of Knowledge by Basic Knowledge Type: An Exploratory Study. Int. J. Environ. Res. Public Health 2022, 19, 5461. https://doi.org/10.3390/ijerph19095461
Kawasaki H, Yamasaki S, Fukita S, Iwasa M, Iki T. Nursing Students’ Retention of Knowledge by Basic Knowledge Type: An Exploratory Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5461. https://doi.org/10.3390/ijerph19095461
Chicago/Turabian StyleKawasaki, Hiromi, Satoko Yamasaki, Susumu Fukita, Mika Iwasa, and Tomoko Iki. 2022. "Nursing Students’ Retention of Knowledge by Basic Knowledge Type: An Exploratory Study" International Journal of Environmental Research and Public Health 19, no. 9: 5461. https://doi.org/10.3390/ijerph19095461