Prevalence of COPD and Tobacco Smoking in Tunisia — Results from the BOLD Study

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Data Collection
2.2.1. Study Outcomes
2.2.2. Definition of COPD Stages
2.2.3. Questionnaire Data
2.3. Statistical Analysis
3. Results
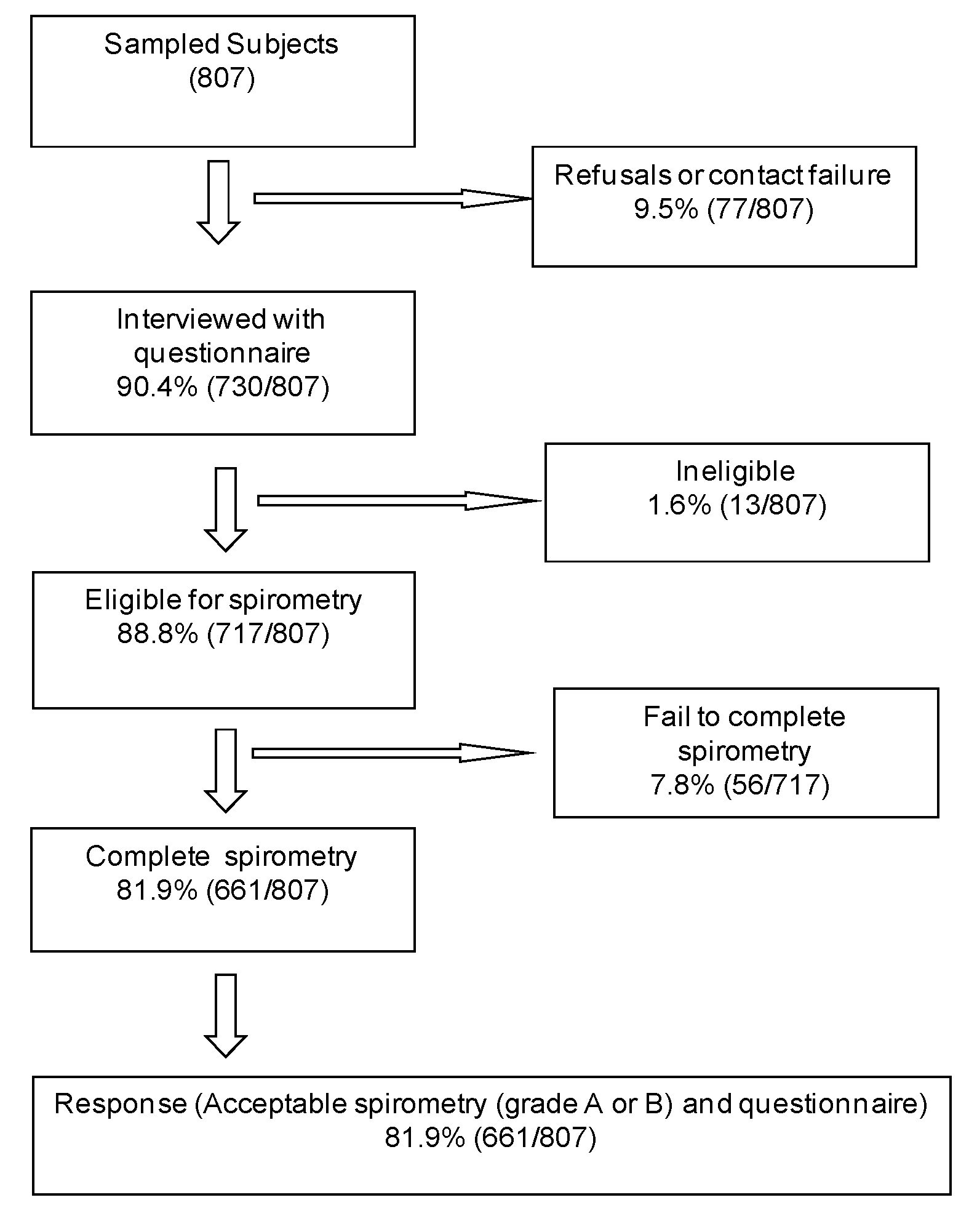
3.1. Sample Demographics


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men | Women | p-value | |
|---|---|---|---|
| Smoking status (pack years) | <0.001 | ||
| Never | 78 (19.6) | 320 (80.4) | |
| 0–10 | 22 (62.9) | 13 (37.1) | |
| 10–20 | 57 (87.7) | 8 (12.3) | |
| 20+ | 152 (93.3) | 11 (6.7) | |
| Lung Function | |||
| FEV1 (L) | 3.1 (0.77) | 2.3 (0.60) | <0.001 |
| FEV1 (%, predicted) | 90.5 (17.34) | 92.3 (17.10) | 0.1913 |
| FVC (L) | 4.0 (0.79) | 2.8 (0.66) | <0.001 |
| FVC (%, predicted) | 89.3 (13.66) | 88.7 (14.63) | 0.5801 |
| FEV1/FVC (%) | 77.8 (8.66) | 81.9 (5.73) | <0.001 |
| 40–49 year | 50–59 year | 60–69 year | 70+ year | All | |
|---|---|---|---|---|---|
| Male gender | |||||
| Never smoker | 24.3 (6.7) | 23.5 (3.5) | 34.4 (5.4) | 25.0 (7.2) | 25.8 (4.1) |
| Former smoker | 16.0 (3.6) | 26.9 (4.0) | 42.0 (6.2) | 37.6 (7.7) | 24.8 (3.0) |
| Current smoker | 59.6 (5.8) | 49.6 (4.8) | 23.6 (3.8) | 37.5 (7.8) | 49.4 (4.2) |
| Female gender | |||||
| Never smoker | 89.4 (3.2) | 90.7 (3.0) | 96.2 (2.8) | 95.2 (4.7) | 91.3 (2.1) |
| Former smoker | 1.5 (1.0) | 2.8 (1.6) | 0 | 0 | 1.5 (0.7) |
| Current smoker | 9.2 (2.8) | 6.5 (2.1) | 3.8 (7.8) | 4.8 (4.7) | 7.3 (1.9) |
| Total | |||||
| Never smoker | 57.1 (4.6) | 54.9 (3.1) | 64.6 (3.5) | 64.2 (5.6) | 58.1 (2.8) |
| Former smoker | 8.7 (2.0) | 15.6 (2.1) | 21.5 (3.5) | 16.6 (3.7) | 13.3 (1.4) |
| Current smoker | 34.2 (4.1) | 29.5 (3.2) | 13.9 (2.5) | 19.2 (4.8) | 28.6 (2.9) |



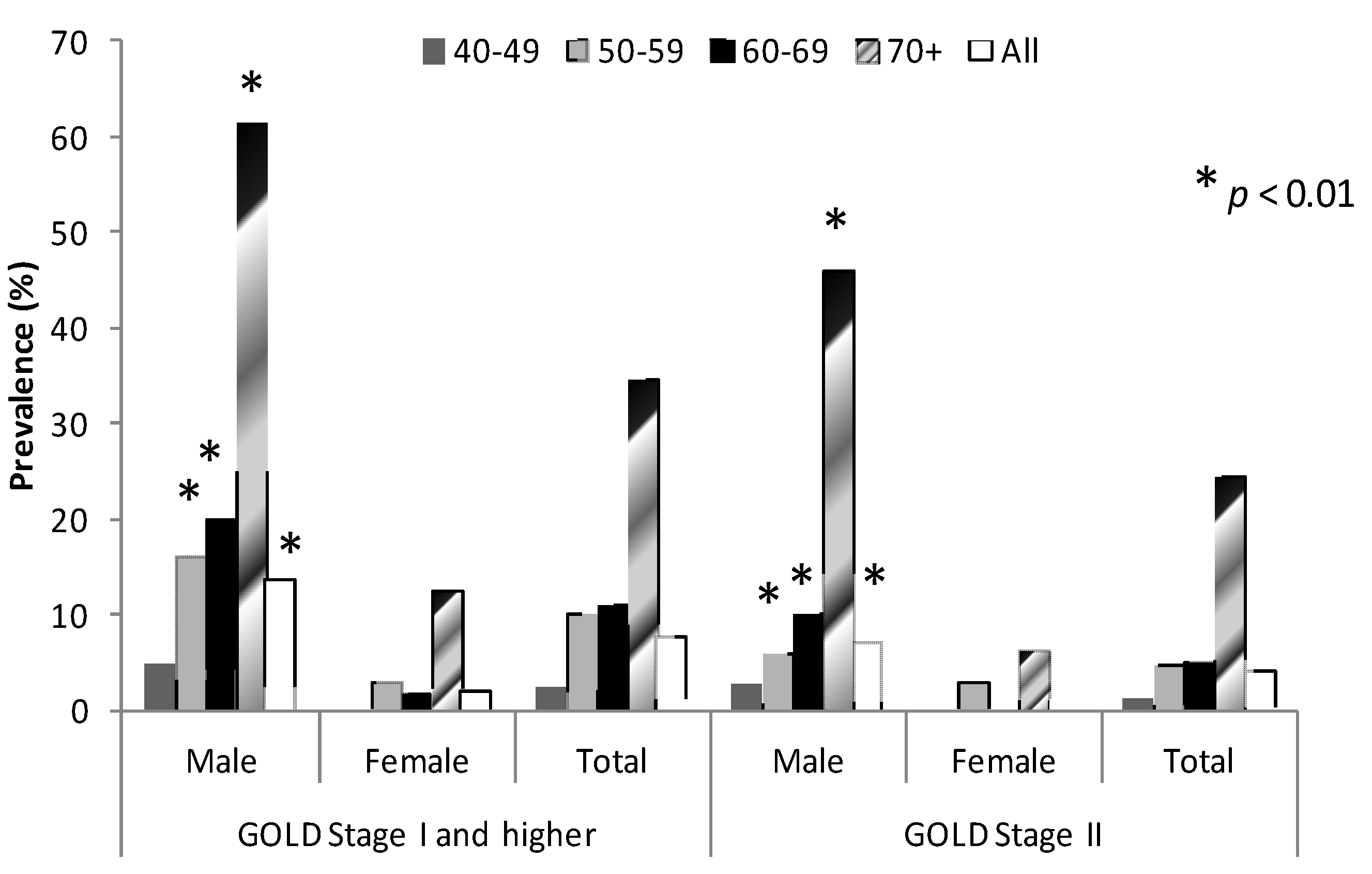
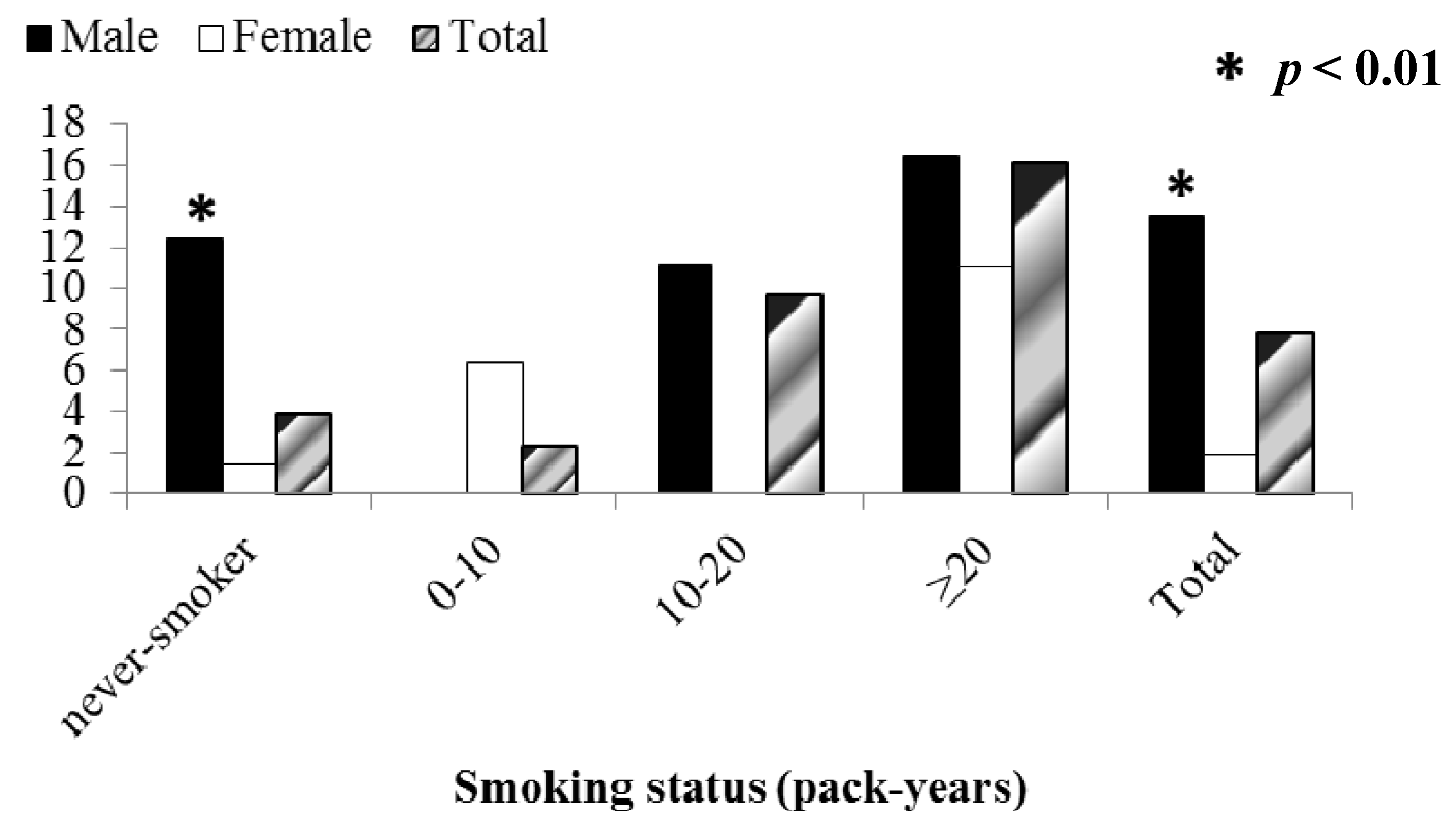
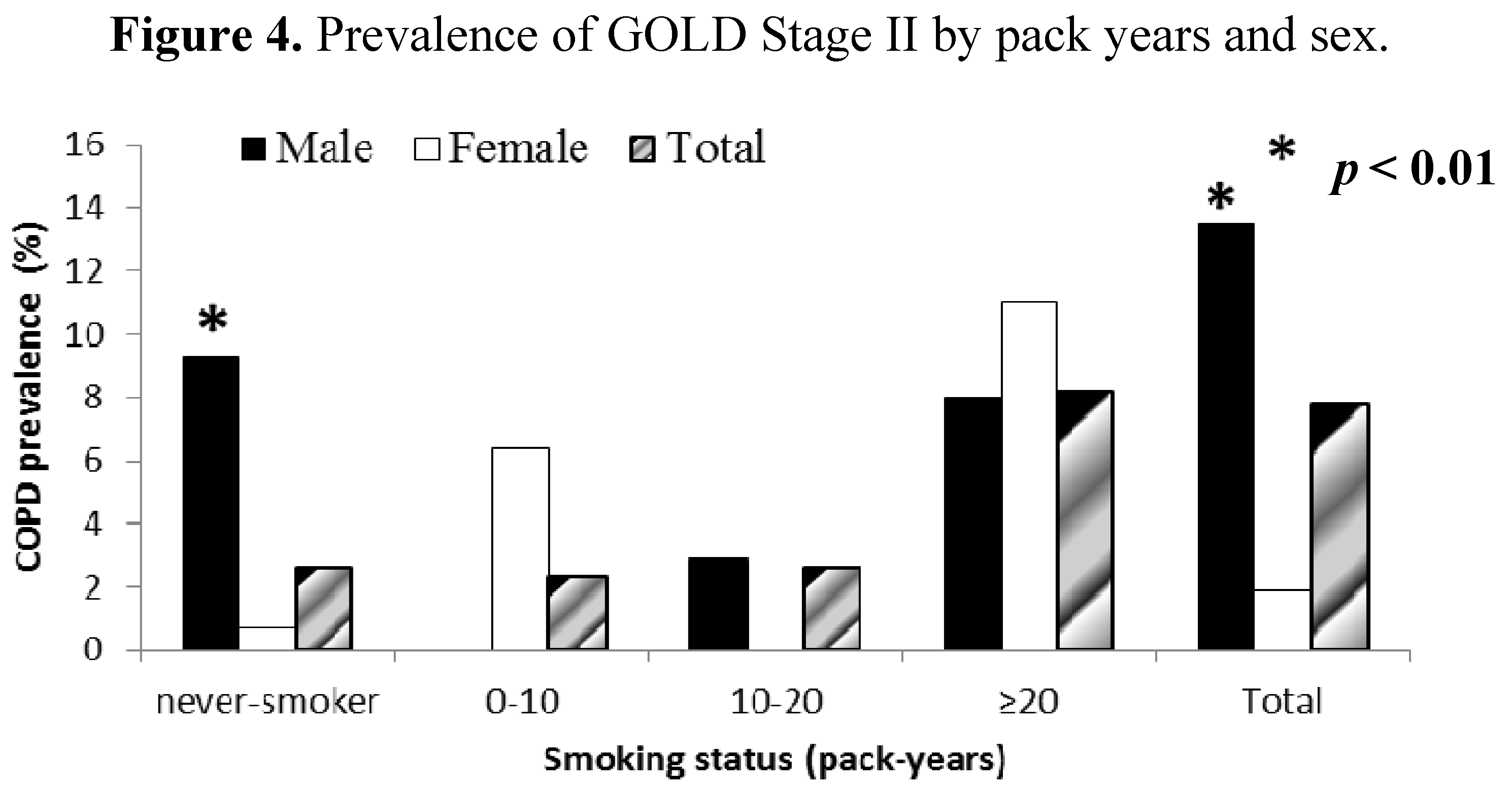
3.2. Risk Factors for COPD
| Unadjusted OR (95% CI) | p-value | Adjusted OR (95% CI) ** | p-value | |
|---|---|---|---|---|
| Sex | ||||
| Male | 1 | 1 | ||
| Female | 0.198 (0.062–0.635) | 0.010 | 0.201 (0.015, 2.733) | 0.210 |
| Age, years | ||||
| 40–49 | 1 | 1 | ||
| 50–59 | 2.090 (0.769–5.677) | 0.137 | 2.105 (0.755, 5.863) | 0.142 |
| 60–69 | 2.472 (0.778–7.853) | 0.116 | 3.519 (0.942, 13.152) | 0.060 |
| ≥70 | 10.403 (2.072–52.222) | 0.007 | 17.670 (2.488, 125.472) | 0.007 |
| Education, years | ||||
| 0 | 1 | 1 | ||
| 1–5 | 0.375 (0.076–1.840) | 0.208 | 0.480 (0.062, 3.698) | 0.455 |
| 6–8 | 0.774 (0.211–2.844) | 0.681 | 1.471 (0.245, 8.827) | 0.653 |
| 9–11 | 0.798 (0.329–1.934) | 0.595 | 0.932 (0.112, 7.761) | 0.944 |
| ≥12 | 0.602 (0.142–2.545) | 0.464 | 0.881 (0.273, 2.839) | 0.820 |
| Smoking Status | ||||
| Never smoker | 1 | |||
| Former smoker | 2.164 (0.667, 7.022) | 0.182 | 0.426 (0.041, 4.429) | 0.449 |
| Current smoker | 3.301 (1.127, 8.150) | 0.030 | 0.641 (0.084, 4.885) | 0.648 |
| Smoking pack-years | ||||
| 10 year increase | 1.252 (1.093–1.435) | 0.003 | 1.176 (0.941, 1.470) | 0.141 |
| Body Mass Index | ||||
| <20 | 4.673 (1.032, 21.159) | 0.046 | 6.610 (1.439, 30.354) | 0.019 |
| 20–25 | 1 | 1 | ||
| 25–30 | 0.536 (0.145, 1.977) | 0.324 | 0.821 (0.267, 2.527) | 0.714 |
| 30–35 | 0.743 (0.282, 1.960) | 0.524 | 1.299 (0.401, 4.208) | 0.642 |
| >35 | 0.271 (0.069, 1.063) | 0.060 | 0.660 (0.177, 2.466) | 0.512 |
| Occupational dust exposure | ||||
| 10 year increase | 1.288 (0.978, 1.697) | 0.069 | 0.996 (0.689, 1.441) | 0.983 |
| Childhood breathing problems | ||||
| No | 1 | 1 | ||
| Yes | 0.956 (0.099, 9.242) | 0.967 | 1.666 (0.195, 14.235) | 0.620 |
| Family history of pulmonary disease | ||||
| No | 1 | 1 | ||
| Yes | 0.190 (0.024, 1.508) | 0.108 | 0.194 (0.018, 2.114) | 0.164 |
3.3. Lifetime Diagnosis of COPD and Respiratory Symptoms
| Doctor-Diagnosed COPD | |||
|---|---|---|---|
| Male | Female | Total | |
| Age, year% | |||
| 40–49 | 1.1 (0.7) | 4.6 (1.5) | 2.8 (0.9) |
| 50–59 | 2.4 (1.4) | 7.0 (1.9) | 4.6 (1.4) |
| 60–69 | 3.2 (2.5) | 3.8 (2.8) | 3.5 (2.4) |
| 70+ | 9.4 (6.8) | 0 | 4.1 (3.0) |
| All | 2.3 (0.8) | 4.8 (0.9) | 3.5 (0.7) |
| Pack-Years% | |||
| Never-smoker | 3.3 (1.5) | 4.2 (0.9) | 4.0 (0.8) |
| 0–10 | 0 | 6.2 (5.7) | 2.0 (2.0) |
| 10–20 | 3.3 (2.5) | 19.8 (17.2) | 5.3 (3.4) |
| 20+ | 1.8 (0.9) | 9.2 (7.2) | 2.3 (0.8) |
| Total | 2.3 (0.8) | 4.8 (0.9) | 3.5 (0.7) |
| COPD defined as | ||||
|---|---|---|---|---|
| LLN Stage I+ (n = 33) | LLN Stage II (n = 30) | GOLD Stage I+ (n = 51) | GOLD Stage II (n = 39) | |
| Cough | 13 (39.39) | 13 (43.33) | 19 (37.25) | 17 (43.59) |
| Sputum | 18 (54.55) | 17 (56.67) | 25 (49.02) | 22 (56.41) |
| Wheezing | 20 (60.61) | 20 (60.67) | 25 (49.02) | 22 (56.41) |
| Dyspnea | 12 (36.36) | 12 (40.00) | 16 (31.37) | 16 (41.03) |
| Chronic cough with phlegm † | 7 (21.21) | 7 (23.33) | 10 (19.61) | 9 (23.08) |
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Abdallah, F.C.B.; Taktak, S.; Chtourou, A.; Mahouachi, R.; Kheder, A.B. Burden of Chronic Respiratory Diseases (CRD) in Middle East and North Africa (MENA). World Allergy Organ. J. 2011, 4, S6–S8. [Google Scholar]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Maalej, M.; Bouacha, H.; Ben Miled, T.; Ben Kheder, A.; el Gharbi, B.; Nacef, T. Chronic bronchitis in Tunisia: Epidemiological aspect. Tunis. Med. 1986, 64, 457–460. [Google Scholar]
- Mannino, D.M.; Gagnon, R.C.; Petty, T.L.; Lydick, E. Obstructive lung disease and low lung function in adults in the United States: Data from the National Health and Nutrition Examination Survey, 1988–1994. Arch. Intern. Med. 2000, 160, 1683–1689. [Google Scholar] [CrossRef]
- Kim, D.S.; Kim, Y.S.; Chung, K.-S.; Chang, J.H.; Lim, C.-M.; Lee, J.H.; Uh, S.-T.; Shim, J.J.; Lew, W.J. Prevalence of chronic obstructive pulmonary disease in Korea: A population-based spirometry survey. Am. J. Respir. Crit. Care Med. 2005, 172, 842–847. [Google Scholar] [CrossRef]
- Pena, V.S.; Miravitlles, M.; Gabriel, R.; Jimenez-Ruiz, C.A.; Villasante, C.; Masa, J.F.; Viejo, J.L.; Fernandez-Fay, L. Geographic variations in prevalence and underdiagnosis of COPD: Results of the IBERPOC multicentre epidemiological study. Chest 2000, 118, 981–989. [Google Scholar] [CrossRef]
- Halbert, R.J.; Isonaka, S.; George, D.; Iqbal, A. Interpreting COPD prevalence estimates: What is the true burden of disease? Chest 2003, 123, 1684–1692. [Google Scholar] [CrossRef]
- Menezes, A.M.B.; Perez-Padilla, R.; Jardim, J.B.; Muino, A.; Lopez, M.V.; Valdivia, G.; de Oca, M.M.; Talamo, C.; Hallal, P.C.; Victora, C.G. Chronic obstructive pulmonary disease in five Latin American cities (the Platino study): A prevalence study. Lancet 2005, 366, 1875–1881. [Google Scholar] [CrossRef]
- Fukuchi, Y.; Nishimura, M.; Ichinose, M.; Adachi, M.; Nagai, A.; Kuriyama, T.; Takahashi, K.; Nishimura, K.; Ishioka, S.; Aizawa, H.; et al. COPD in Japan: The nippon COPD epidemiology study. Respirology 2004, 9, 458–465. [Google Scholar] [CrossRef]
- Schirnhofer, L.; Lamprecht, B.; Vollmer, W.M.; Allison, M.J.; Studnicka, M.; Jensen, R.L.; Buist, S. COPD prevalence in Salzburg, Austria: Results from the burden of obstructive lung disease (BOLD) study. Chest 2007, 131, 29–36. [Google Scholar] [CrossRef]
- Buist, A.S.; Vollmer, W.M.; Sullivan, S.D.; Weiss, K.B.; Lee, T.A.; Menezes, A.M.B.; Crapo, R.O.; Jensen, R.L.; Burney, P.G.J. The burden of Obstructive Lung Disease Initiative (BOLD): Rationale and design. J. Chronic Obstr. Pulm. Dis. 2005, 2, 277–283. [Google Scholar] [CrossRef]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.B.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (The BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Medical Section of the American Lung Association. Standardization of spirometry: 1994 update. Am. J. Respir. Crit. Care Med. 1994, 152, 1107–1136.
- Enright, P.L.; Studnicka, M.; Zielinski, J. Spirometry to detect and manage chronic obstructive pulmonary disease and asthma in the primary care setting. Eur. Respir. Mon. 2005, 31, 1–14. [Google Scholar]
- Global Strategy for the Diagnosis, Management, and Prevention of COPD. Available online: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html (accessed on 10 December 2013).
- Hankinson, J.L.; Odencrantz, J.R.; Fedan, K.B. Spirometric reference values from a sample of the general U.S. population. Am. J. Respir. Crit. Care Med. 1999, 159, 179–187. [Google Scholar] [CrossRef]
- Vollmer, W.M.; Gıslason, B.; Burney, P.; Enright, P.L.; Gulsvik, A.; Kocabase, A.; Buist, A.S. Comparison of spirometry criteria for the diagnosis of COPD: Results from the BOLD study. Eur. Respir. J. 2009, 34, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Zhong, N.; Wang, C.; Yao, W.; Chen, P.; Kang, J.; Huang, S.; Chen, B.; Wang, C.; Ni, D.; Zhou, Y.; et al. Prevalence of chronic obstructive pulmonary disease in China, a large population-based survey. Am. J. Respir. Crit. Care Med. 2007, 176, 753–760. [Google Scholar] [CrossRef]
- Lundback, B.; Lindberg, A.; Lindstrom, M.; Ronmark, E.; Jonsson, A.C.; Jonsson, E.; Larsson, L.-G.; Andersson, S.; Sandstrom, T.; Larsson, K. Not 15 but 50% of smokers develop COPD?—Report from the obstructive lung disease in Northern Sweden studies. Respir. Med. 2003, 97, 115–122. [Google Scholar] [CrossRef]
- Tzanakis, N.; Anagnostopoulou, U.; Filaditaki, V.; Christaki, P.; Siafakas, N. COPD group of the Hellenic Thoracic Society. Prevalence of COPD in Greece. Chest 2004, 125, 892–900. [Google Scholar] [CrossRef]
- Feenstra, T.L.; van Gunugten, M.L.; Hoogenveen, R.T.; Wouters, E.F.; Rutten-van Molken, M.P. The impact of aging and smoking on the future burden of chronic obstructive pulmonary disease: A model analysis in the Netherlands. Am. J. Respir. Crit. Care Med. 2001, 164, 590–596. [Google Scholar] [CrossRef]
- Hardie, J.A.; Buist, A.S.; Vollmer, W.M.; Ellingsen, I.; Bakke, P.S.; Mørkve, O. Risk of over-diagnosis of COPD in asymptomatic elderly never-smokers. Eur. Respir. J. 2002, 20, 1117–1122. [Google Scholar] [CrossRef]
- Hnizdo, E.; Glindmeyer, H.W.; Petsonk, E.L.; Enright, P.; Buist, A.S. Case definitions for chronic obstructive pulmonary disease. Chronic Obstr. Pulm. Dis. 2006, 3, 95–100. [Google Scholar] [CrossRef]
- Pauwels, R.A.; Buist, A.S.; Calverley, P.M.A.; Jenkins, C.R.; Hurd, S.S. Global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 163, 1256–1276. [Google Scholar] [CrossRef]
- Hemminki, K.; Li, X.; Sundquist, K.; Sundquist, J. Familial risks for chronic obstructive pulmonary disease among siblings based on hospitalisations in Sweden. J. Epidemiol. Community Health 2008, 62, 398–401. [Google Scholar] [CrossRef]
- Kurmi, O.P.; Semple, S.; Simkhada, P.; Smith, W.C.S.; Ayres, J.G. COPD and chronic bronchitis risk of indoor air pollution from solid fuel: A systematic review and meta-analysis. Thorax 2010, 65, 221–228. [Google Scholar] [CrossRef]
- Lamprecht, B.; McBurnie, M.A.; Vollmer, W.M.; Gudmundsson, G.; Welte, T.; Nizankowska-Mogilnicka, E.; Studnicka, M.; Bateman, E.; Anto, J.M.; Burney, P.; et al. COPD in never smokers: Results from the population-based burden of obstructive lung disease study. Chest 2011, 139, 752–763. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Wang, C.; Yao, W.; Chen, P.; Kang, J.; Huang, S.; Chen, C.; Wang, D.; Ni, X.; Wang, D.; et al. COPD in Chinese nonsmokers. Eur. Respir. J. 2009, 33, 509–518. [Google Scholar] [CrossRef]
- Silva, G.E.; Sherill, D.L.; Guerra, S.; Barbee, R.A. Asthma as a risk factor for COPD in a longitudinal study. Chest 2004, 126, 59–65. [Google Scholar] [CrossRef]
- Hagstad, S.; Ekerljung, L.; Lindberg, A.; Backman, H.; Rönmark, E.; Lundbäck, B. COPD among non-smokers—Report from the Obstructive Lung Disease in Northern Sweden (OLIN) studies. Respir. Med. 2012, 106, 980–988. [Google Scholar] [CrossRef]
- Pembroke, T.P.I.; Farhat, R.; Hart, C.L.; Smith, G.D.; Stansfeld, S.A. Psychological distress and chronic obstructive pulmonary disease in the Renfrew and Paisley (MIDSPAN) study. J. Epidemiol. Community Health 2006, 60, 789–792. [Google Scholar] [CrossRef]
- Varkey, A.B. Chronic obstructive pulmonary disease in women: Exploring gender differences. Curr. Opin. Pulm. Med. 2004, 10, 98–103. [Google Scholar] [CrossRef]
- Celli, B.R.; Halbert, R.J.; Isonaka, S.; Schau, B. Population impact of different definitions of airway obstruction. Eur. Respir. J. 2003, 22, 268–273. [Google Scholar] [CrossRef]
- Stanojevic, S.; Wade, A.; Stocks, J. Reference values for lung function: past, present and future. Eur. Respir. J. 2010, 36, 12–19. [Google Scholar] [CrossRef]
- Hansen, J.E.; Sun, X.-G.; Wasserman, K. Spirometric criteria for airway obstruction: Use percentage of FEV1/FVC ratio below the fifth percentile, not <70%. Chest 2007, 131, 349–355. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van de Grinten, C.M.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Jithoo, A.; Bateman, E.D.; Lombard, C.J.; Beyers, N.; Allison, M. Prevalence of COPD in South Africa: Results from the BOLD Study. Proc. Am. Thorac. Soc. 2006, 3, A545. [Google Scholar] [CrossRef]
- Kocabas, A.; Hancioglu, A.; Turkyilmaz, S.; Unalan, T.; Umut, S.; Cakir, B.; Vollmer, W.; Buist, S. Prevalence of COPD in Adana, Turkey (BOLD-Turkey Study). Proc. Am. Thorac. Soc. 2006, 3, A543. [Google Scholar] [CrossRef]
- Tabka, Z.; Hassayoune, H.; Guénard, H.; Zebidi, A.; Commenges, D.; Essabah, H.; Salamon, R.; Varene, P. Valeurs de référence spirométriques chez la population tunisienne. Tunis. Med. 1995, 73, 125–131. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Daldoul, H.; Denguezli, M.; Jithoo, A.; Gnatiuc, L.; Buist, S.; Burney, P.; Tabka, Z.; Harrabi, I. Prevalence of COPD and Tobacco Smoking in Tunisia — Results from the BOLD Study. Int. J. Environ. Res. Public Health 2013, 10, 7257-7271. https://doi.org/10.3390/ijerph10127257
Daldoul H, Denguezli M, Jithoo A, Gnatiuc L, Buist S, Burney P, Tabka Z, Harrabi I. Prevalence of COPD and Tobacco Smoking in Tunisia — Results from the BOLD Study. International Journal of Environmental Research and Public Health. 2013; 10(12):7257-7271. https://doi.org/10.3390/ijerph10127257
Chicago/Turabian StyleDaldoul, Hager, Meriam Denguezli, Anamika Jithoo, Louisa Gnatiuc, Sonia Buist, Peter Burney, Zouhair Tabka, and Imed Harrabi. 2013. "Prevalence of COPD and Tobacco Smoking in Tunisia — Results from the BOLD Study" International Journal of Environmental Research and Public Health 10, no. 12: 7257-7271. https://doi.org/10.3390/ijerph10127257
APA StyleDaldoul, H., Denguezli, M., Jithoo, A., Gnatiuc, L., Buist, S., Burney, P., Tabka, Z., & Harrabi, I. (2013). Prevalence of COPD and Tobacco Smoking in Tunisia — Results from the BOLD Study. International Journal of Environmental Research and Public Health, 10(12), 7257-7271. https://doi.org/10.3390/ijerph10127257