Spatial Analysis of the Home Addresses of Hospital Patients with Hepatitis B Infection or Hepatoma in Shenzhen, China from 2010 to 2012



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
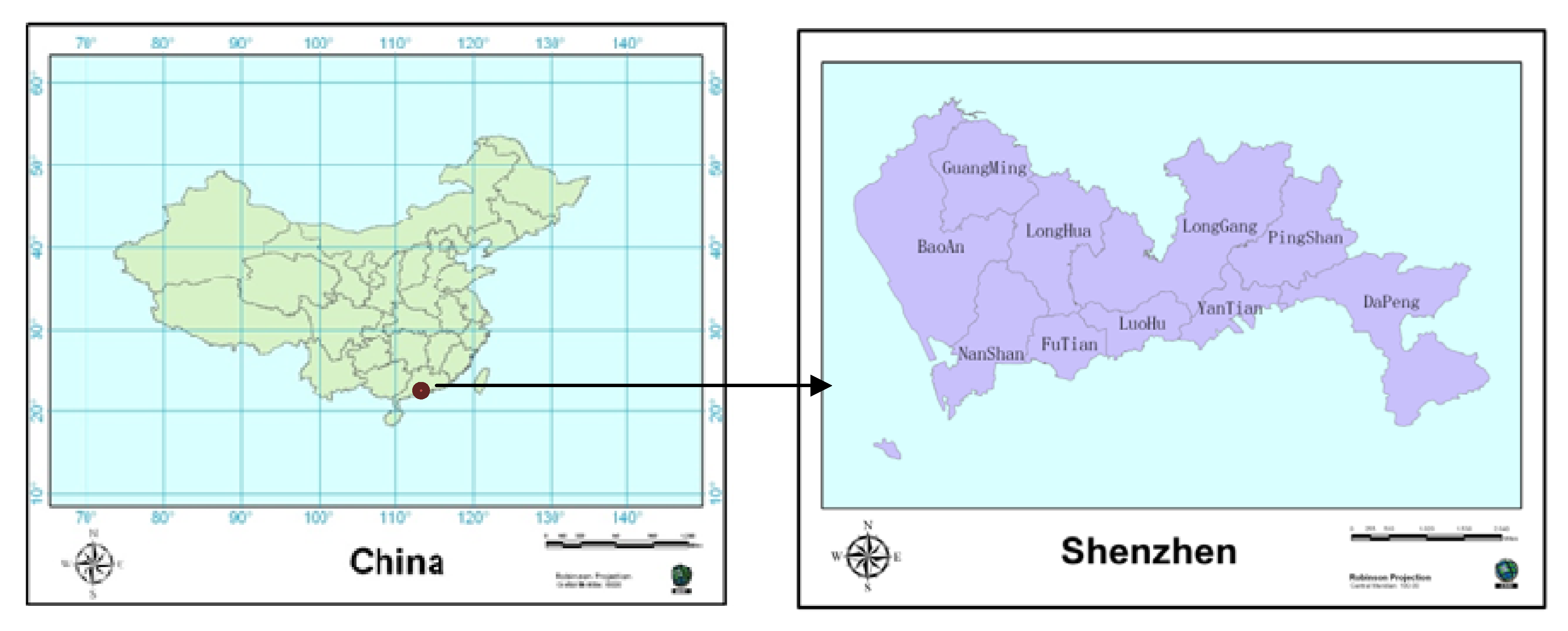
2.1. Study Area

2.2. Data
2.3. Methods
 statistic [20,21] for each disease case in Shenzhen during 2010–2012 to distinguish either high or low cluster values spatially with ArcGIS 10. The Getis-Ord local statistic is given as follows:
statistic [20,21] for each disease case in Shenzhen during 2010–2012 to distinguish either high or low cluster values spatially with ArcGIS 10. The Getis-Ord local statistic is given as follows:
 statistic is a z-score, so no further calculations are required. The hotspot map can identify significant spatial clusters of high values (hot spots) and low values (cold spots). Spatial cluster analysis tests the spatial distribution of disease patterns in a particular geographical environment, with the cluster coefficient C = S2/X, where X is the average number of cases in each area, for the corresponding variance. If C < 1, then the spatial distribution of the cases is uniform; if C = 1, then the spatial distribution is random, and if C > 1, then the spatial distribution of the cases represents an aggregated distribution. In local Moran’s I analysis, COType fields with significantly (p < 0.05) high levels of clustering are expressed as HH, and those with significantly (p < 0.05) low levels of clustering are expressed as LL. If the Z-score is <1.96, then there is a significant level (p < 0.05) of spatial outliers. The output elements for the classification field for COType indicate whether high value elements and surrounding elements are lower (HL), or whether low elements and surrounding elements are high value elements (LH).
statistic is a z-score, so no further calculations are required. The hotspot map can identify significant spatial clusters of high values (hot spots) and low values (cold spots). Spatial cluster analysis tests the spatial distribution of disease patterns in a particular geographical environment, with the cluster coefficient C = S2/X, where X is the average number of cases in each area, for the corresponding variance. If C < 1, then the spatial distribution of the cases is uniform; if C = 1, then the spatial distribution is random, and if C > 1, then the spatial distribution of the cases represents an aggregated distribution. In local Moran’s I analysis, COType fields with significantly (p < 0.05) high levels of clustering are expressed as HH, and those with significantly (p < 0.05) low levels of clustering are expressed as LL. If the Z-score is <1.96, then there is a significant level (p < 0.05) of spatial outliers. The output elements for the classification field for COType indicate whether high value elements and surrounding elements are lower (HL), or whether low elements and surrounding elements are high value elements (LH).3. Results and Discussion
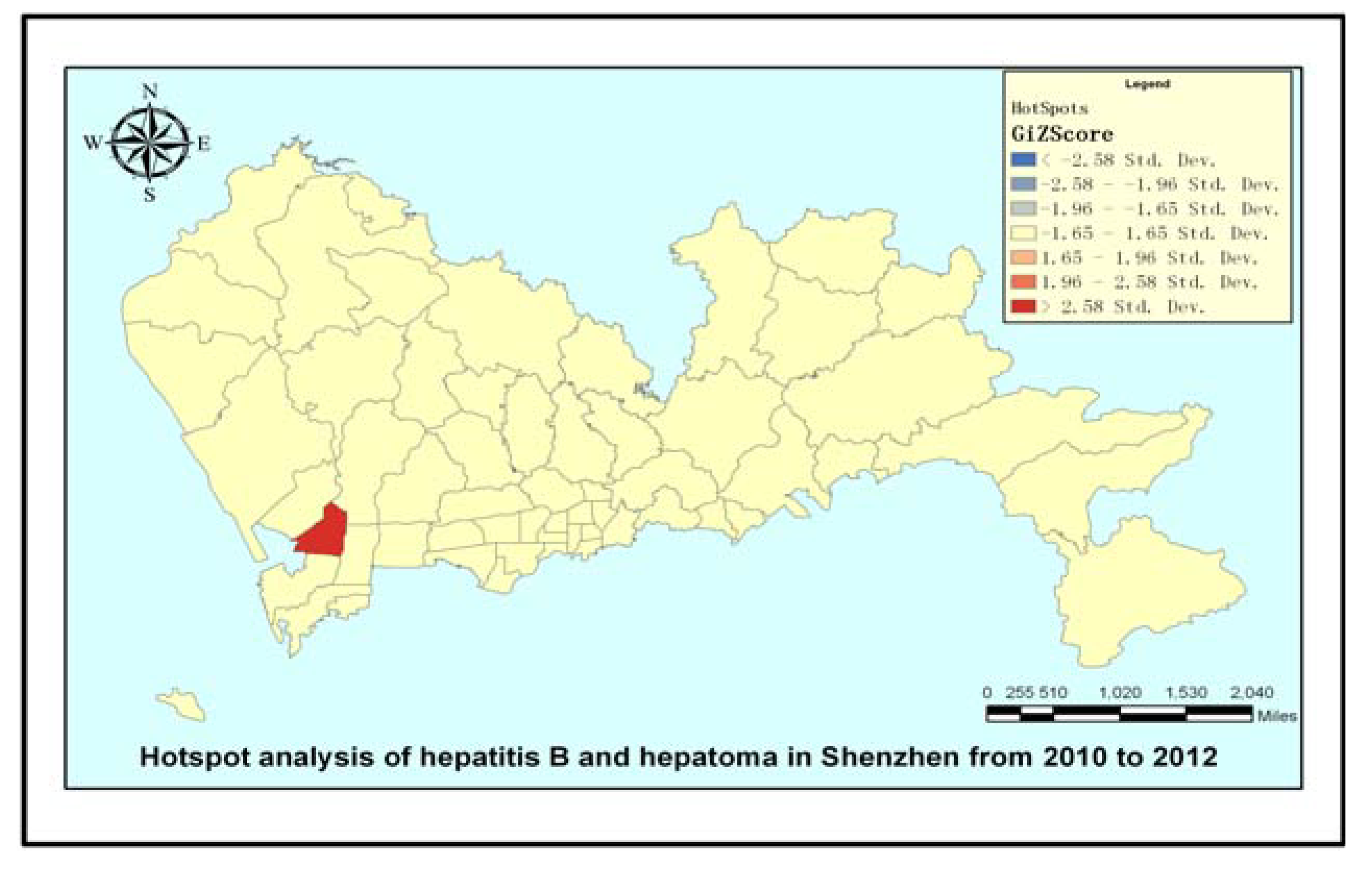
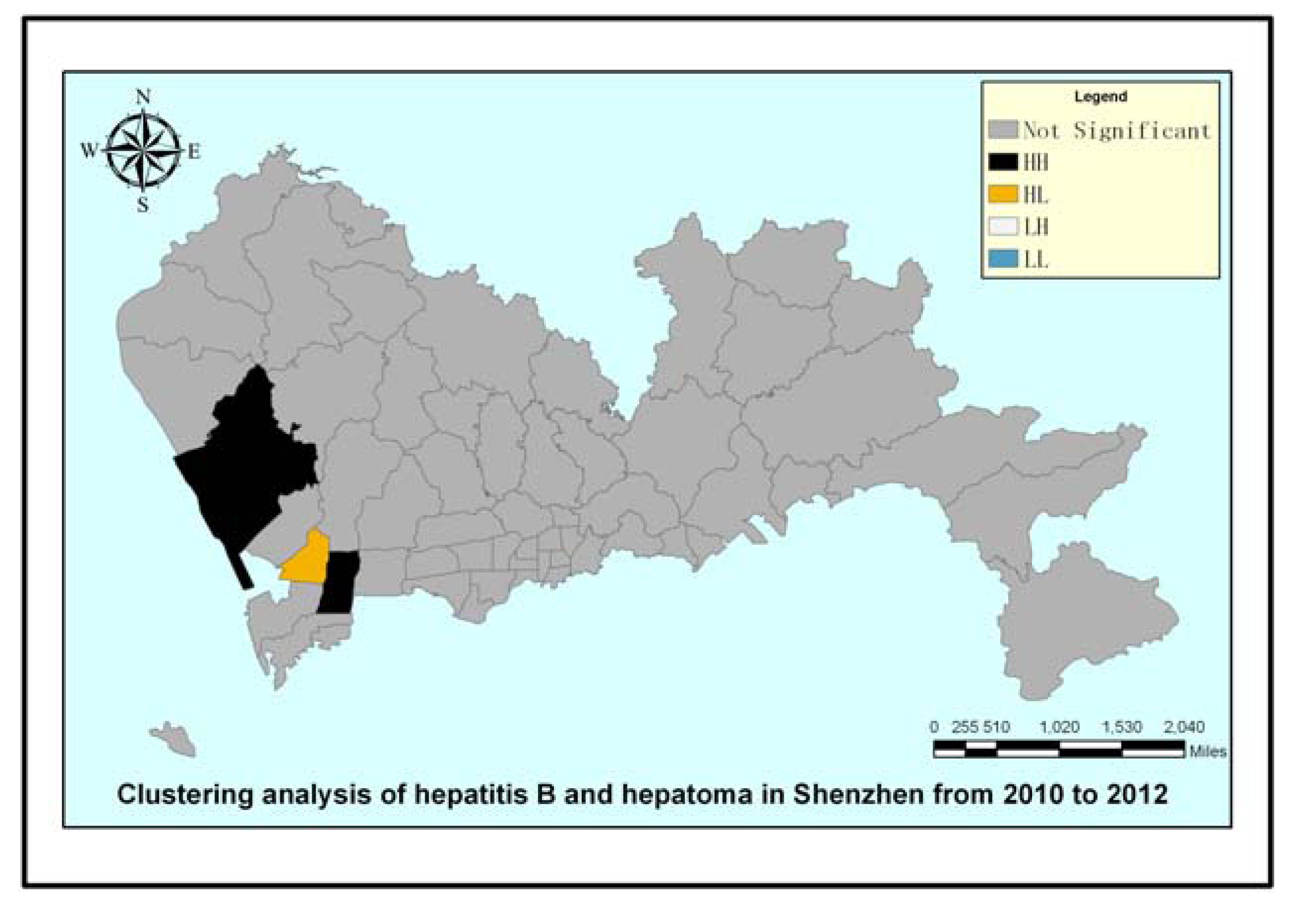
 ) tool in ArcGIS software to draw a hot spot map. The only red region is the Nantou sub-district, which was identified as having a significantly high value. The map reflects hepatoma cases gathered in the Nantou sub-district in the geographical space scale. In the map of Figure 4, the black regions of the Xixiang sub-district and Yuehai sub-district have significant levels of high value (HH) clustering, whereas the yellow region of the Nantou sub-district is mainly composed of significantly high values of low around the outliers (HL) clustering. The other sub-districts showed no significant spatial agglomeration effect. Based on Figure 3 and Figure 4, we can conclude that the Nanshan district had a higher hepatoma incidence rate than other districts in Shenzhen during 2010–2012. Prevention and intervention measures should focus on these areas for its agglomeration; we should pay more attention to these areas in the health resource allocation. To a great extent, medical convenient depends on the spatial location and distribution of medical services.
) tool in ArcGIS software to draw a hot spot map. The only red region is the Nantou sub-district, which was identified as having a significantly high value. The map reflects hepatoma cases gathered in the Nantou sub-district in the geographical space scale. In the map of Figure 4, the black regions of the Xixiang sub-district and Yuehai sub-district have significant levels of high value (HH) clustering, whereas the yellow region of the Nantou sub-district is mainly composed of significantly high values of low around the outliers (HL) clustering. The other sub-districts showed no significant spatial agglomeration effect. Based on Figure 3 and Figure 4, we can conclude that the Nanshan district had a higher hepatoma incidence rate than other districts in Shenzhen during 2010–2012. Prevention and intervention measures should focus on these areas for its agglomeration; we should pay more attention to these areas in the health resource allocation. To a great extent, medical convenient depends on the spatial location and distribution of medical services.


4. Conclusions

Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nelson, P.K.; Mathers, B.M.; Cowie, B.; Hagan, H.; Jarlais, D.D.; Horyniak, D.; Degenhardt, L. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet 2011, 378, 571–583. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P. Health and social cohesion: Why care about income inequality? BMJ 1997, 314, 1037–1040. [Google Scholar] [CrossRef]
- Gesler, W. The uses of spatial analysis in medical geography: A review. Soc. Sci. Med. 1986, 23, 963–973. [Google Scholar] [CrossRef]
- Jacquez, G.M. Spatial analysis in epidemiology: Nascent science or a failure of GIS? J. Geogr. Syst. 2000, 2, 91–97. [Google Scholar] [CrossRef]
- Hjalmars, U.L.F.; Kulldorff, M.; Gustafsson, G.; Nagarwalla, N. Childhood leukaemiain Sweden: Using GIS and a spatial scan statisticfor cluster detection. Stat. Med. 1996, 15, 707–715. [Google Scholar] [CrossRef]
- Rushton, G. Public health, GIS, and spatial analytic tools. Annu. Rev. Public Health 2003, 24, 43–56. [Google Scholar] [CrossRef]
- Martin, S.W.; Michel, P.; Middleton, D.; Holt, J.; Wilson, J. Investigation of clusters of giardiasis using GIS and a spatial scan statistic. Int. J. Health Geogr. 2004, 3. [Google Scholar] [CrossRef] [Green Version]
- Clarke, K.C.; McLafferty, S.L.; Tempalski, B.J. On epidemiology and geographic information systems: A review and discussion of future directions. Emerg. Infect. Dis. 1996, 2, 85–92. [Google Scholar]
- Moore, D.A.; Carpenter, T.E. Spatial analytical methods and geographic information systems: Use in health research and epidemiology. Epidemiol. Rev. 1999, 21, 143–161. [Google Scholar] [CrossRef]
- Rytkönen, M.J. Not all maps are equal: GIS and spatial analysis in epidemiology. Int. J. Circumpolar Health 2004, 63, 9–24. [Google Scholar]
- Goodchild, M.F. Geographical information-science. Int. J. Geogr. Inf. Syst. 1992, 6, 31–45. [Google Scholar]
- Karsentg, E.; Leventhal, A. Health geographic information systems (HGIS)—A tool for health planning and epidemiology. Harefuah 2002, 141, 1070–1075. [Google Scholar]
- Bojanović, A.; Bošnjaković, P.; Stojanović, M.; Marković, M.; Mrvić, M.; Radić, S.; Radovanović, Z. Precision TACE in therapy of primary malignant tumors of liver/hepatocellular carcinoma (HCC). Acta Chir. Iugosl. 2009, 56, 143–148. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef]
- Kew, M.C. Epidemiology of hepatocellular carcinoma. Toxicology 2002, 27, 35–38. [Google Scholar] [CrossRef]
- Bosch, F.X.; Ribes, J.; Borràs, J. Epidemiology of primary liver cancer. Semin. Liver Dis. 1999, 19, 271–285. [Google Scholar] [CrossRef]
- Davila, J.A.; Petersena, N.J.; Nelson, H.A.; El-Serag, H.B. Geographic variation within the United States in the incidence of hepatocellular carcinoma. J. Clin. Epidemiol. 2003, 56, 487–493. [Google Scholar]
- Richards, T.B.; Croner, C.M.; Rushton, G.; Brown, C.K.; Fowler, L. Geographic information systems and public health: Mapping the future. Public Health Rep. 1999, 114, 359–373. [Google Scholar] [CrossRef]
- Zhou, X.N. Disease Mapping. In Spatial Epidemiology; Beijing Science Press: Beijing, China, 2009; pp. 237–239. [Google Scholar]
- Getis, A.; Ord, J.K. The analysis of spatial association by use of distance statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Getis, A.; Ord, J.K. Local Spatial Statistics: An Overview. In Spatial Analysis: Modeling in a GIS Environment; Longley, P., Batty, M., Eds.; John Wiley & Sons: Cambridge, UK, 1996; pp. 269–285. [Google Scholar]
- Ciccone, A. Agglomeration effects in Europe. Eur. Econ. Rev. 2002, 46, 213–227. [Google Scholar] [CrossRef]
- Getis, A.; Ord, J.K. Local spatial autocorrelation statistics: Distributional issues and an application. Geogr. Anal. 2010, 27, 286–306. [Google Scholar] [CrossRef]
- Getis, A.; Ord, J.K. Testing for local spatial autocorrelation in the presence of global autocorrelation. J. Reg. Sci. 2001, 41, 411–432. [Google Scholar]
- Evans, A.A.; Chen, G.; Ross, E.A.; Shen, F.M.; Lin, W.Y.; London, W.T. Eight-year follow-up of the 90,000-person Haimen city cohort: Hepatocellular carcinoma mortality, risk factors, and gender differences. Cancer Epidemiol. Biomark. Prev. 2002, 11, 369–376. [Google Scholar]
- Chen, C.J.; Liang, K.Y.; Chang, A.S.; Chang, Y.C.; Lu, S.N.; Liaw, Y.F.; Chang, W.Y.; Sheen, M.C.; Lin, T.M. Effects of hepatitis B virus, alcohol drinking, cigarette smoking and familial tendency on hepatocellular carcinoma. Hepatology 1991, 13, 398–406. [Google Scholar] [CrossRef]
- Hassan, M.M.; Hwang, L.Y.; Hatten, C.J.; Swaim, M.; Li, D.; Abbruzzese, J.L.; Beasley, P.; Patt, Y.Z. Risk factors for hepatocellular carcinoma: Synergism of alcohol with viral hepatitis and diabetes mellitus. Hepatology 2002, 36, 1206–1213. [Google Scholar] [CrossRef]
- Kuper, H.; Tzonou, A.; Kaklamani, E.; Hsieh, C.C.; Lagiou, P.; Adami, H.O.; Trichopoulos, D.; Stuver, S.O. Tobacco smoking, alcohol consumption and their interaction in the causation of hepatocellular carcinoma. Int. J. Cancer 2000, 85, 498–502. [Google Scholar] [CrossRef]
- Austin, H.; Delzell, E.; Grufferman, S.; Levine, R.; Morrison, A.S.; Stolley, P.D.; Cole, P. A case-control study of hepatocellular carcinoma and the hepatitis B virus, cigarette smoking, and alcohol consumption. Cancer Res. 1986, 46, 962–966. [Google Scholar]
- Mori, M.; Hara, M.; Wada, I.; Hara, T.; Yamamoto, K.; Honda, M.; Naramoto, J. Prospective study of hepatitis B and C viral infections, cigarette smoking, alcohol consumption, and other factors associated with hepatocellular carcinoma risk in Japan. Am. J. Epidemiol. 2000, 151, 131–139. [Google Scholar] [CrossRef]
- Chiang, C.T.; Lian, I.B.; Su, C.C.; Tsai, K.Y.; Lin, Y.P.; Chang, T.K. Spatiotemporal trends in oral cancer mortality and potential risks associated with heavy metal content in Taiwan soil. Int. J. Environ. Res. Public Health 2010, 7, 3916–3928. [Google Scholar] [CrossRef]
- Farrington, C.P.; Kanaan, M.N.; Gay, N.J. Estimation of the basic reproduction number for infectious diseases from age-stratified serological survey data. Appl. Stat. 2001, 50, 251–292. [Google Scholar]
- Peng, W.; Chen, Y.; Jiang, Q.; Zheng, Y. Spatial analysis of hepatocellular carcinoma and socioeconomic status in China from a population-based cancer registry. Cancer Epidemiol. 2010, 34, 29–33. [Google Scholar] [CrossRef]
- Joshi, S.; Song, Y.M.; Kim, T.H.; Cho, S.I. Socio-economic status and the risk of liver cancer mortality: A prospective study in Korean men. Public Health 2008, 122, 1144–1151. [Google Scholar] [CrossRef]
- Soobader, M.J.; LeClere, F.B.; Hadden, W.; Maury, B. Using aggregate geographic data to proxy individual socioeconomic status: Does size matter? Am. J. Public Health 2001, 91, 632–636. [Google Scholar] [CrossRef]
- Jacobsen, K.H.; Koopman, J.S. The effects of socioeconomic development on worldwide hepatitis A virus seroprevalence patterns. Int. J. Epidemiol. 2005, 34, 600–609. [Google Scholar]
- Balbi, M.; Donadon, V.; Ghersetti, M.; Grazioli, S.; Valentina, G.D.; Gardenal, R.; Mas, M.D.; Casarin, P.; Zanette, G.; Miranda, C.; et al. Alcohol and HCV chronic infection are risk cofactors of Type 2 diabetes mellitus for hepatocellular carcinoma in Italy. Int. J. Environ. Res. Public Health 2010, 7, 1366–1378. [Google Scholar] [CrossRef]
- Boulos, M.N. Towards evidence-based, GIS-driven national spatial health information infrastructure and surveillance services in the United Kingdom. Int. J. Health Geogr. 2004, 3. [Google Scholar] [CrossRef] [Green Version]
- Kistemann, T.; Dangendorf, F.; Schweikart, J. New perspectives on the use of geographical information systems (GIS) in environmental health sciences. Int. J. Hyg. Environ. Health 2002, 205, 169–181. [Google Scholar] [CrossRef]
- Bédard, Y.; Henriques, W.D. Modern information technologies in environmental health surveillance. An overview and analysis. Can. J. Public Health 2002, 93, 29–33. [Google Scholar]
- Miranda, M.L.; Dolinoy, D.C.; Overstreet, M.A. Mapping for prevention: GIS models for directing childhood lead poisoning prevention programs. Environ. Health Perspect. 2002, 110, 947–953. [Google Scholar]
- Bédard, Y.; Gosselin, P.; Rivest, S.; Proulx, M.J.; Nadeau, M.; Lebel, G.; Gagnon, M.F. Integrating GIS components with knowledge discovery technology for environmental health decision support. Int. J. Med. Inform. 2003, 70, 79–94. [Google Scholar] [CrossRef]
- Peek-Asa, C.; Ramirez, M.R.; Shoaf, K.; Seligson, H.; Kraus, J.F. GIS mapping of earthquake-relateddeaths and hospital admissions from the 1994 Northridge, California, earthquake. Ann. Epidemiol. 2000, 10, 5–13. [Google Scholar] [CrossRef]
- Reissman, D.B.; Staley, F.; Curtis, G.B.; Kaufmann, R.B. Use of geographic information system technology to aid health department decision making about child hood lead poisoning prevention activities. Environ. Health Perspect. 2001, 109, 89–94. [Google Scholar] [CrossRef]
- Astorri, F.; Beaubien, S.E.; Ciotoli, G.; Lombardi, S. An assessment of gas emanation hazard using a geographic information system and geostatistics. Health Phys. 2002, 82, 358–366. [Google Scholar] [CrossRef]
- Maantay, J. Mapping environmental injustices: Pitfalls and potential of geographic information systems in assessing environmental health and equity. Environ. Health Perspect. 2002, 110, 161–171. [Google Scholar] [CrossRef]
- Scholten, H.J.; de Lepper, M.J.C. The benefits of the application of geographical information systems in public and environmental health. World Health Stat. Q. 1991, 44, 160–170. [Google Scholar]
- Roper, W.L.; Mays, G.P. GIS and public health policy: A new frontier for improving community health. J. Public Health Manag. Pract. 1999, 5, 15–26. [Google Scholar]
- Perry, B.; Gesler, W. Physical access to primary health care in Andean Bolivia. Soc. Sci. Med. 2000, 50, 1177–1188. [Google Scholar] [CrossRef]
- Higgs, G.; Richards, W. The use of geographical information systems in examining variations in sociodemographic profiles of dental practice catchments: A case study of a Swansea practice. Prim. Dent. Care 2002, 9, 63–69. [Google Scholar] [CrossRef]
- McLafferty, S.L. GIS and health care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef]
- Ruger, J.P.; Ng, N.Y. Emerging and transitioning countries’ role in global health. St. Louis Univ. J. Health Law Policy 2010, 3, 253–289. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hu, T.; Du, Q.; Ren, F.; Liang, S.; Lin, D.; Li, J.; Chen, Y. Spatial Analysis of the Home Addresses of Hospital Patients with Hepatitis B Infection or Hepatoma in Shenzhen, China from 2010 to 2012. Int. J. Environ. Res. Public Health 2014, 11, 3143-3155. https://doi.org/10.3390/ijerph110303143
Hu T, Du Q, Ren F, Liang S, Lin D, Li J, Chen Y. Spatial Analysis of the Home Addresses of Hospital Patients with Hepatitis B Infection or Hepatoma in Shenzhen, China from 2010 to 2012. International Journal of Environmental Research and Public Health. 2014; 11(3):3143-3155. https://doi.org/10.3390/ijerph110303143
Chicago/Turabian StyleHu, Tao, Qingyun Du, Fu Ren, Shi Liang, Denan Lin, Jiajia Li, and Yan Chen. 2014. "Spatial Analysis of the Home Addresses of Hospital Patients with Hepatitis B Infection or Hepatoma in Shenzhen, China from 2010 to 2012" International Journal of Environmental Research and Public Health 11, no. 3: 3143-3155. https://doi.org/10.3390/ijerph110303143
APA StyleHu, T., Du, Q., Ren, F., Liang, S., Lin, D., Li, J., & Chen, Y. (2014). Spatial Analysis of the Home Addresses of Hospital Patients with Hepatitis B Infection or Hepatoma in Shenzhen, China from 2010 to 2012. International Journal of Environmental Research and Public Health, 11(3), 3143-3155. https://doi.org/10.3390/ijerph110303143