Social Cost of Leptospirosis Cases Attributed to the 2011 Disaster Striking Nova Friburgo, Brazil

Abstract
:1. Introduction

2. Experimental Section
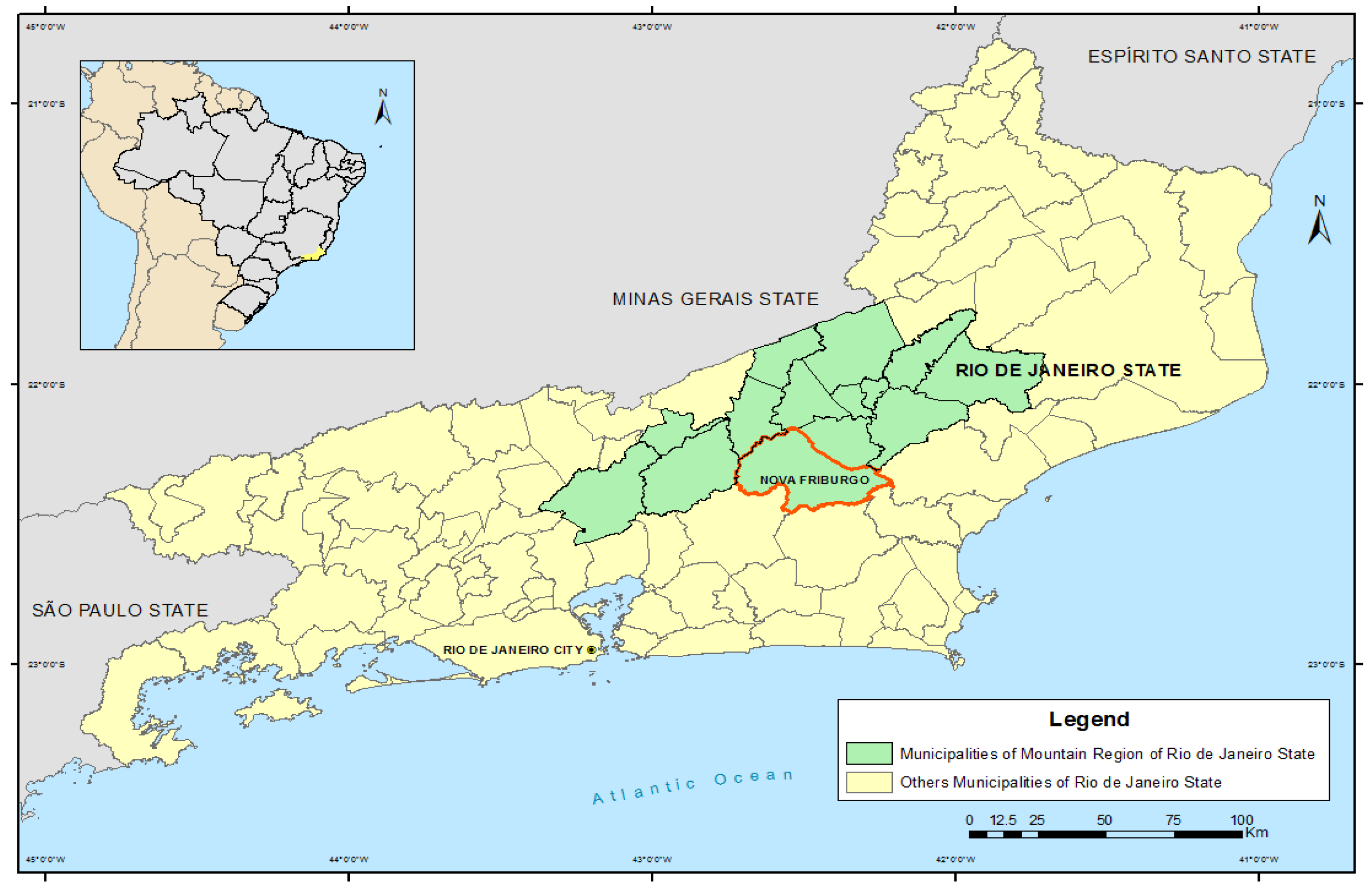
2.1. Scope
2.2. Source of Data
2.3. Costs to the Health System
2.4. Costs to the Society

2.5. Empirical Therapy and Avoided Cost Analysis
2.6. Ethical Criteria
3. Results and Discussion

{kind=link}
| Year | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 * |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Confirmed cases | 3 | 1 | 2 | 2 | 4 | 0 | 9 | 5 | 6 | 7 | 177 |
3.1. Direct Costs to the Health Sector
| Variables | Valid N (%) | Years |
|---|---|---|
| Total number of confirmed cases | 149 | |
| Gender | 149 | |
| Male | 87 (58.39) | |
| Female | 62 (41.61) | |
| Age | 148 | |
| Mean | 33.01 | |
| Median | 31.00 | |
| Standard deviation | 14.01 | |
| Diagnostic tests performed | 159 | |
| Elisa | 133 (83.65) | |
| Mat | 8 (5.03) | |
| Other | 18 (11.32) | |
| Criteria for classification | 149 | |
| Confirmed by clinical/laboratory criteria | 74 (49.66) | |
| Confirmed by clinical/epidemiological criteria | 75 (50.34) | |
| Evolution | 148 | |
| Cure | 148 (100.00) | |
| Death due to leptospirosis | 0 (0.00) | |
| Death due to other causes | 0 (0.00) |
3.2. Costs to Society
| Variables | Valid N (%) | Years |
|---|---|---|
| Total number of confirmed cases | 28 | |
| Gender | 28 | |
| Male | 18 (64.29) | |
| Female | 10 (35.71) | |
| Age | 28 | |
| Mean | 40.93 | |
| Median | 43.50 | |
| Standard deviation | 15.94 | |
| Diagnostic tests performed | 49 | |
| Elisa | 41 (83.67) | |
| Mat | 8 (16.33) | |
| Other | 0 (0.00) | |
| Criteria for classification | 28 | |
| Confirmed by clinical/laboratory criteria | 24 (85.71) | |
| Confirmed by clinical/epidemiological criteria | 4 (14.29) | |
| Evolution | 27 | |
| Cure | 26 (96.30) | |
| Death due to leptospirosis | 0 (0.00) | |
| Death due to other causes | 1 (3.70) |
3.3. Empirical Therapy
3.4. Avoided Cost Analysis
3.5. Total Cost of Illness
| Variables | Hospital | Outpatient |
|---|---|---|
| Confirmed cases | 28 | 149 |
| Variables related to care | ||
| Average length of stay (days) | 6.36 | - |
| Total cost (US$) | 10,736.00 | 1,488.97 |
| Mean cost (US$) | 383.43 | 9.99 |
| Median cost (US$) | 346.44 | 9.79 |
| Empirical therapy | ||
| Valid N | 22 | 135 |
| Total cost (US$) | 921.86 | 5,093.01 |
| Mean cost (US$) | 41.90 | 37.72 |
| Median cost (US$) | 46.35 | 26.98 |
| Loss of productivity | ||
| Economically active N | 26 | 129 |
| Loss based on the median income of the county (US$) *,’ | 5,754.08 | 4,581.95–68,729.31 |
| Loss based on the state minimum wage (US$) *,” | 3,753.15 | 2,988.62–44,829.37 |
| Loss based on national minimum wage (US$) *,# | 3,337.29 | 2,655.28–39,829.13 |
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Confalonieri, U.E.; Marinho, D.P. Mudanca climatica global e saude: Perspectivas para o Brasil. Rev. Multiciencia 2007, 8, 48–64. [Google Scholar]
- Pan American Health Organization. Mudanca Climatica e Saude: um perfil do Brasil; Pan American Health Organization Ministry of Health: Brasilia, Brazil, 2009. [Google Scholar]
- Intergovernmental Panel on Climate Change. Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation. A Special Report of Working Groups I and II of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V., Stocker, T.F., Qin, D., Dokken, D.J., Ebi, K.L., Mastrandrea, M.D., Mach, K.J., Plattner, G.K., Allen, S.K., Tignor, M., Midgley, P.M., Eds.; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Laboratorio de Gestao do Territorio. Megacidades, vulnerabilidades e mudancas climaticas: Regiao metropolitana do Rio de Janeiro; Laget: Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Barata, M.M.; Confalonieri, U.E.; Lima, A.C.; Marinho, D.P.; Luigi, G.; Simone, G.C.; Ferreira, I.B.; Pinto, I.V.; Tosta, F.O.; Silva, H.V.; et al. Mapa de vulnerabilidade da populacao do estado do Rio de Janeiro aos impactos das mudancas climaticas nas areas social, saude e ambiente; Department of Environment: Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Barata, M.M.; Confalonieri, U.E.; Marinho, D.P.; Costa, C.N.; Luigi, G.; Tosta, F.O.; Pereira, C.A.; Marincola, F.C. Mapa de vulnerabilidade da populacao dos municipios do Estado do Rio de Janeiro frente as mudancas climaticas; Oswaldo Cruz Foundation: Rio de Janeiro, Brazil, 2013. (in press) [Google Scholar]
- Dourado, F.; Arraes, T.C.; Fernandes e Silva, M. The “Megadesastre” in the mountain region of Rio de Janeiro State—Causes, mechanisms of mass movements and spatial allocation of investments for reconstruction post disaster. Anu. Inst. Geocienc. 2012, 35, 43–54. [Google Scholar]
- The Tragedy of the Highlands Region in the State of Rio de Janeiro in 2011: Looking for Answers. Available online: http://casoteca.enap.gov.br/index.php?option=com_multicategories&view=article&id=73:the-tragedy-of-the-highlands-region-in-the-state-of-rio-de-janeiro-in-2011-looking-for-answers- (accessed on 19 February 2014).
- Brazilian Institute of Geography and Statistics (IBGE) Malhas Digitais 2012. Available online: ftp://geoftp.ibge.gov.br/malhas_digitais/ (accessed on 15 January 2013).
- Porto, S.S. Saude em Desastres: A Experiencia de Nova Friburgo [CD-ROM]; Vigidesastres: Nova Friburgo, Brazil, 2012. [Google Scholar]
- Brazilian Ministry of Health. Guide to Epidemiological Surveillance, 7th ed.; Ministry of Health: Brasilia, Brazil, 2009. [Google Scholar]
- Brazilian Institute of Geography and Statistics (IBGE) Cidades@ 2012. Available online: http://cidades.ibge.gov.br/xtras/home.php (accessed on 02 October 2013).
- Brazilian Service of Support for Micro and Small Enterprises (Sebrae-RJ). Informacoes socioeconomicas do municipio de Nova Friburgo; Sebrae-RJ: Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Brazililian Ministry of Health. 1st Seminar on Participative Health Administration of the Mountainous Region. of Rio de Janeiro; Ministry of Health: Brasilia, Brazil, 2007. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/07_0155_M.pdf (accessed on 15 October 2013).
- Brazilian National Cadastre of Health Establishments (CNES). Available online: http://cnes.datasus.gov.br (accessed on 10 May 2013).
- Brazilian Management System of Table of Procedures, Drugs, Orthotics, Prosthetics and Special Materials of SUS. Available online: http://sigtap.datasus.gov.br/tabela-unificada/app/sec/inicio.jsp (accessed on 08 December 2013).
- Guia do direito a saude: Sistema Publico de Saude (SUS), Medicamentos e Planos de Saude. Available online: http://www.guiadedireitos.org/downloads/guia_direito_saude.pdf (accessed on 19 February 2014).
- Brazilian Outpatient Information System (SIA). Available online: http://w3.datasus.gov.br/siasih/siasih.php (accessed on 15 November 2013).
- Pereira, C.R. Sergio Arouca National School of Public Health: Rio de Janeiro, Brazil, 2013; E-Mail: carlos.rpereira @ hotmail.com.
- Motta, R.S. Manual Para Valoracao Economica de Recursos Ambientais; IPEA: Rio de Janeiro, Brazil, 1997. [Google Scholar]
- Brazilian Ministry of Social Security. Statistical Yearbooks. Available online: http://www.previdencia.gov.br/estatisticas/menu-de-apoio-estatisticas-seguranca-e-saude-ocupacional-tabelas/ (accessed on 17 November 2013).
- Brazilian Official Gazette of the Union. Medida Provisoria n° 516 de 30 de Dezembro de 2010; Official Gazette of the Union: Brasilia, Brazil, 2010. [Google Scholar]
- Brazilian Official Gazette of the Union. Lei n° 12.382 de 25 de Fevereiro de 2011; Official Gazette of the Union: Brasilia, Brazil, 2011. [Google Scholar]
- Brazilian Official Gazette of the Union. Lei n° 5.950 de 13 de abril de 2011; Official Gazette of the Executive: Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Getulio Vargas Foundation. Center of Social Policies. Renda Media. Available online: http://www.cps.fgv.br/cps/bd/nbrics/NBRICS_Rankings_Listagem-ultimorenda_site.xlsx (accessed on 15 October 2013).
- Medicos Param Unidades do SUS em 21 Estados Nesta Terca. Available online: http://www1.folha.uol.com.br/cotidiano/995624-medicos-param-unidades-do-sus-em-21-estados-nesta-terca.shtml (accessed on 15 October 2013).
- The Nursing Salary of Nurses. 2012. Available online: http://aenfermagem.com.br/materia/salario-de-enfermagem/ (accessed on 15 October 2013).
- Dourados Now. Salary of Community Health Agents. Available online: http://www.douradosagora.com.br/noticias/politica/piso-salarial-de-agentes-omunitarios-de-saude-esta-pronto-para-ir-a-plenario (accessed on 15 October 2013).
- Salariometro. Available online: http://www.salariometro.sp.gov.br/ (accessed on 20 October 2013).
- Anvisa List Prices of Medicines. 2011. Available online: http://portal.anvisa.gov.br/wps/portal/anvisa/anvisa/regulado/!ut/p/c4/04_SB8K8xLLM9MSSzPy8xBz9CP0os3hnd0cPE3MfAwMDMydnA093Uz8z00B_A3cXQ_2CbEdFAMyIKzk!/?1dmy&urile=wcm%3Apath%3A/anvisa+portal/anvisa/pos+-+comercializacao+-+pos+-+uso/regulacao+de+marcado/publicacao+regulacao+economica/listas+de+precos+de+medicamentos+03 (accessed on 15 October 2013).
- Pereira, C.A.; Barata, M.M. Estimated social cost of leptospirosis cases that occurred in 2008 in Brazil. (In press)
- Brazilian Information System for Notifiable Diseases (SINAN). Available online: http://dtr2004.saude.gov.br/sinanweb/ (accessed on 12 December 2013).
- Picardeau, M.; Bertherat, E.; Jancloes, M.; Skouloudis, A.N.; Durski, K.; Hartskeerl, R.A. Rapid tests for diagnosis of leptospirosis: Current tools and emerging technologies. Diagn. Microbiol. Infect. Dis. 2013, 78, 1–8. [Google Scholar]
- Musso, D.; Lascolab, B. Diagnostic biologique de la leptospirose. Revue Francophone Des. Laboratoires 2013, 449, 39–46. [Google Scholar] [CrossRef]
- Brazilian Mortality Information System (SIM). Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/obt10rj.def (accessed on 17 December 2013).
- Souza, V.M.; Arsky, M.L.; Castro, A.P.; Araujo, W.N. Years of potential life lost and hospitalization costs associated with leptospirosis in Brazil. Rev. Saude Publica 2011, 45, 1001–1008. [Google Scholar] [CrossRef]
- Goarant, C.; Laumond-Barny, S.; Perez, J.; Vernel-Pauillac, F.; Chanteau, S.; Guigon, A. Outbreak of leptospirosis in New Caledonia: Diagnosis issues and burden of disease. Trop Med. Int. Health 2009, 14, 926–929. [Google Scholar] [CrossRef]
- Freitas, C.M.; Ximenes, E.F. Floods and public health—A review of the recent scientific literature on the causes, consequences and responses to prevention and mitigation. Cienc Saude Colet 2012, 17, 1601–1615. [Google Scholar] [CrossRef]
- Marengo, J.A.; Nobre, C.A.; Salati, E.; Ambrizzi, T. Caracterizacao do clima atual e definicao das alteracoes climaticas para o territorio brasileiro ao longo do Seculo XXI; Ministry of Environment: Brasilia, Brazil, 2007. Available online: http://mudancasclimaticas.cptec.inpe.br/~rmclima/pdfs/prod_probio/Sumario.pdf (accessed on 13 December 2013).
- Oliveira, D.S.; Guimaraes, M.J.; Medeiros, Z. Productive model for leptospirosis. Revista de Patologia Tropical 2009, 38, 17–26. [Google Scholar]
- Melo, C.B.; Reis, R.B.; Ko, A.I.; Barreto, C.M.; Lima, A.P.; Silva, A.M. Geographical distribution of leptospirosis in Aracaju, State of Sergipe from 2001 to 2007. Rev. Soc. Bras. Med. Trop 2011, 44, 475–480. [Google Scholar] [CrossRef]
- Fensterseifer, T. A responsabilidade do estado pelos danos causados as pessoas atingidas pelos desastres ambientais ocasionados pelas mudancas climaticas: Uma analise a luz dos deveres de protecao ambiental do estado e da correspondente proibicao de insuficiencia na tutela do direito fundamental ao ambiente. In Biblioteca Virtual da Defensoria publica do Estado de Sao Paulo; 2011; 1, pp. 1–27. Available online: http://www.defensoria.sp.gov.br/dpesp/Repositorio/31/Documentos/12.pdf (accessed on 12 December 2013). [Google Scholar]
- Suputtamongkol, Y.; Pongtavornpinyo, W.; Lubell, Y.; Suttinont, C.; Hoontrakul, S.; Phimda, K.; Losuwanaluk, K.; Suwancharoen, D.; Silpasakorn1, S.; Chierakul, W.; et al. Strategies for diagnosis and treatment of suspected leptospirosis: A cost-benefit analysis. PLoS Negl. Trop. Dis. 2010, 4, 1–6. [Google Scholar]
- Freitas, C.M.; Carvalho, M.L.; Ximenes, E.F.; Arraes, E.F.; Gomes, J.O. Socio-environmental vulnerability, disaster risk-reduction and resilience-building—Lessons from the earthquake in Haiti and torrential rains in the mountain range close to Rio de Janeiro in Brazil. Cien Saude Colet 2012, 17, 1577–1586. [Google Scholar] [CrossRef]
- State Department of Health of Sao Paulo. Epidemiological Surveillance Center “Prof. Alexandre Vranjac”. In Caderno de Vigilancia Epidemiologica: Vigilancia Epidemiologica em Saude Ambiental; State Department of Health of Sao Paulo: Sao Paulo, Brazil, 2013. Available online: ftp://ftp.cve.saude.sp.gov.br/doc_tec/DOMA/doma13_caderno_ambiental.pdf (accessed on 13 December 2013). [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pereira, C.; Barata, M.; Trigo, A. Social Cost of Leptospirosis Cases Attributed to the 2011 Disaster Striking Nova Friburgo, Brazil. Int. J. Environ. Res. Public Health 2014, 11, 4140-4157. https://doi.org/10.3390/ijerph110404140
Pereira C, Barata M, Trigo A. Social Cost of Leptospirosis Cases Attributed to the 2011 Disaster Striking Nova Friburgo, Brazil. International Journal of Environmental Research and Public Health. 2014; 11(4):4140-4157. https://doi.org/10.3390/ijerph110404140
Chicago/Turabian StylePereira, Carlos, Martha Barata, and Aline Trigo. 2014. "Social Cost of Leptospirosis Cases Attributed to the 2011 Disaster Striking Nova Friburgo, Brazil" International Journal of Environmental Research and Public Health 11, no. 4: 4140-4157. https://doi.org/10.3390/ijerph110404140