Maternally Perceived Barriers to and Facilitators of Establishing and Maintaining Tooth-Brushing Routines with Infants and Preschoolers

Abstract
:1. Introduction

2. Experimental Section
2.1. Participants
2.2. Procedure

{kind=link}
| Maternal age in years | Mean 30.66 (sd 3.53; range 22.83–35.00) |
| Infant age in years | Mean 2.22 (sd .16; range 1.92–2.50) |
| Infant gender | 8 Female (50%), 8 male (50%) |
| Ethnicity | 12 White-British (76%)
1 White-Irish (6%) 1 White-other (6%) 1 White/Afro-Caribbean (6%) 1 Pakistani (6%) |
| Marital status | 8 Married (50%)
7 Cohabiting (44%) 1 Divorced (6%) |
| Current employment status | 2 Full-time employment (13%)
6 Part-time employment (37%) 2 Part-time education (13%) 6 Full-time carers (37%) |
| Maternal employment type | 7 Skilled (non-manual) (44%)
6 Unemployed/full-time carer (38%) 2 Partly skilled (12%) 1 Skilled (manual) (6%) |
| Educational record | 8 Higher education (50%) (≥17 years in education)
8 Further education (50%) (14 years in education) |
3. Results and Discussion
3.1. Findings
- (i)
- Perceived maternal self-efficacy for tooth-brushing: Almost a third of the mother’s interviewed (6/16) reported that they it was important to feel confident that they could establish dyadic tooth-brushing routines, which could be defined as ‘self-efficacy’, in order for them to successfully establish twice daily toothbrushing with their child. Some described perceiving the task of establishing dyadic tooth-brushing routines as challenging, but because they saw the task as important, they therefore felt confident they could, and should, establish the routines successfully. For example, Participant 8 says:“…you’ve got to trust yourself a lot more than, like I was a bit ‘oh I don’t know what to do’. But actually you do know what to do.”
- (ii)
- Perceived locus of control for tooth-brushing: Three mothers reported that as a mother, they were the individual who controlled tooth-brushing, not their child. Despite non-compliant behaviours, they felt that they had enough authority to ensure they brushed their infant or preschooler’s teeth regularly and to an adequate level of hygiene. So for example, Participant 1 said:“I’m the parent, she’s not the parent, so I need to make a decision on her behalf…”
- (iii)
- Perceived outcome expectancies of establishing tooth-brushing routines: Three mothers had positive ‘outcome expectations’ and reported that they saw tooth-brushing routines as valuable and necessary and something that could preserve their child’s dental health. Participant 2 described the possible outcomes if a parent fails to establish dyadic tooth-brushing routines:“…I’ve heard a lot of horror stories about kids having to have their teeth pulled out and things like that. There’s absolutely no way at all I want to have that for (infant’s name)… ”
- (iv)
- Perceived maternal stress: Three mothers reported feelings of stress related to difficulties they experienced whilst attempting to establish dyadic tooth-brushing routines. One mother in particular reported that she suffered from Chronic Fatigue Syndrome and that this caused even routine parenting tasks to be tiring and stressful:“I lose it. I try losing it behind closed doors. But ‘cos he knows I’m unwell, he kind of gets to a point when he gets frustrated ‘cos there’s stuff we can’t do. But I get brain tired, and I can’t cope ‘can I do this, I want to do that’. My brain shuts down.”Participant 9
- (v)
- Maternal ability to remember to brush: One mother also reported experiencing some difficulties in remembering to brush her child’s teeth, especially at night:“I’m forgetful. I know you can’t really forget about it. When you’re thinking of everything else, you just forget.”Participant 10
- (i)
- Initiating tooth-brushing early in infancy: Initiating tooth-brushing as early as possible was reported by almost all mothers (13/16). Tooth-brushing routines were initiated either before the first tooth had erupted or as soon as this happened and was reported as being important in helping infants get used to tooth-brushing from as young an age as possible. One mother reported the mechanism by which initiating tooth-brushing as early as possible helped the facilitation of the routine:“…you introduce them to the brush before they realise it’s something that they don’t like.”Participant 9
- (ii)
- Allowing infant or preschooler to have a go at brushing their own teeth: Another strategy employed by over half of mothers (9/16) to maximise compliance during tooth-brushing was allowing their infant or preschooler to have a go at brushing their own teeth during a tooth-brushing session. Participant 1 describes this process of turn-taking during tooth-brushing:“…she gets to have a go, and then we rinse the toothbrush. And then I have another go, and she gets another go, and we rinse the tooth-brush and it goes on.”
- (iii)
- Infant/preschooler modelling parent’s tooth-brushing behaviour: Approximately half of mother’s interviewed (7/16) reported that they used a tooth-brushing technique in which they brushed their own teeth whilst allowing their infant or preschooler to observe whilst they were doing it. So for example, Participant 10 described:“I stand her on the toilet and I brush mine …she does hers. And she copies. She copies a lot. So she does hers, and then I do mine, and then I say ‘let mummy do it’, and she lets me do hers for her.”.”
- (iv)
- Creating a game out of a tooth-brushing session: Another strategy, reported by approximately one-third of mothers (6/16) was turning tooth-brushing into a fun game (e.g., singing a song whilst brushing). Participant 15 describes how she used fun songs about tooth-brushing to make the activity enjoyable for her infant:“I sing like a daft song, like that one on CBeebies [children’s television programme]. Or I do that song, you know the one in Grease…‘brusher, brusher, brusher’…”
- (v)
- Disciplining infant/preschooler if non-compliant during tooth-brushing: Approximately a third of mothers (6/16) reported that sometimes it was necessary to discipline their infant or preschooler (e.g., by withholding privileges) when they exhibited non-compliant behaviours during tooth-brushing. For example, Participant 8 describes how she withholds privileges like bedtime stories before having to resort to more punitive discipline:“…just give him a few chances and then it’s like ‘do it or you’ll lose your stories’. But if it’s too bad then it’s like ‘we’ll count to 3 and then daddy’s going to hold you down and do it for you.”
- (vi)
- Restraining infant/preschooler if physically non-compliant during tooth-brushing: The more punitive strategy of physically restraining an infant or preschooler, to ensure tooth-brushing had been completed effectively, was reported by just over one third (6/16) of mothers. This technique was usually employed when infants displayed non-compliant behaviours in response to tooth-brushing (e.g., tantrums). Participant 14 describes how her husband would provide physical restraint in order to ensure their daughter had her teeth brushed properly:“…he [husband] has to like hold her in a head lock and she just screams, it’s awful!”
- (vii)
- Routinisation of tooth-brushing: Routinisation of tooth-brushing, and the embedding of tooth-brushing into a wider repertoire of routine hygiene behaviours was also reported as being important to the maintenance of the behaviour by just under one-third of mothers (5/16). Participant 9 describes how she has embedded tooth-brushing onto a full repertoire of bed-time routine behaviours:“…it was just kind of like part of bath, teeth, stories, and bed. It was just kind of the routine that we did it. And we still have the same routines now. Bath and teeth, stories and bed.”
- (iix)
- Maternal perseverance with tooth-brushing when faced with difficulties: A quarter of mothers (4/16) also reported that it was important to persevere in the face of difficulties when trying to establish and maintain dyadic tooth-brushing routines. These difficulties tended to be around difficult, non-compliant behaviours that disrupted tooth-brushing sessions. Participant 10 describes how she had to persevere with brushing her daughter’s teeth in order to get her used to the routine:“Like don’t give in really. That is the main thing and I think she got used to brushing her teeth’ cos I stuck to it every day. It’s just persistence really. Like make sure you do it every day so they get used to it.”
- (ix)
- Providing rewards for infant compliance during tooth-brushing: One mother (Participant 9) also reported that it was important to provide rewards for her infant when they exhibited compliant behaviours during tooth-brushing. The use of this positive parenting strategy to encourage infant compliance during tooth-brushing was used by this mother in conjunction with other strategies such as withholding privileges, mainly bedtime stories:Researcher. “So you use the story as a reward?”Participant. “He loves books. So…a lot of the ‘I don’t want to’ is dealt with by ‘that’s fine but then I don’t want to read a story for you’ ”
- (i)
- Infant/preschooler wanting to brush themselves causes non-compliance during tooth-brushing: The most common difficult, non-compliant behaviour that inhibited tooth-brushing was where the child wanted to/attempted to man-handle the tooth-brush and brush their own teeth, which was reported by half of mothers (8/16). Participant 14 describes how time consuming it sometimes was to give in to her daughter desire for autonomy during tooth-brushing:“…just lately ‘cos she’s Miss Independent it’s really hard to like [brush teeth]. Like she won’t let me do them, and she’s strong. You can’t, like she has to brush them herself so it takes about 10 minutes. And she wants to do it…”
- (ii)
- General dislike of tooth-brushing causes non-compliance: General dislike of tooth-brushing was reported by approximately half of mothers (7/16) as being a barrier to twice-daily dyadic tooth-brushing. This general dislike was reported by some mothers as resulting in difficult, non-compliant behaviours such as tantrums. So for example, Participant 6 described how her son would physically struggle during tooth-brushing because he disliked it so much:“…he just struggles. Like I get the toothbrush in his mouth and I literally just go like, dead quick. But that’s as much as I can do, ‘cos he just like struggles about. Yeah, he’s a nightmare.”
- (iii)
- Closed mouth/refusal to open mouth inhibits tooth-brushing: A less common, difficult, non-compliant behaviour was refusal to open the mouth which was reported by a quarter of mothers (4/16). This made inserting the tooth-brush into the infant’s or preschooler’s mouth more difficult, and would have inhibited further stages of tooth-brushing such as the removal of food debris. Some mother reported that they coped with this difficulty by trying to force the tooth-brush into their child’s mouth, like Participant 12 for example:“…she would open her mouth, and sometimes she wouldn’t open her mouth. And I used to have to kind of force the brush gently.”
“…doing the kind of ‘eee’ and ‘ahh’ has helped to at least get her mouth in the right position for me to get in there…”
- (iv)
- Attempting to man-handle toothbrush prevents tooth-brushing: Some mothers (3/16) reported that their infant or preschooler sometimes attempted to man-handle the tooth-brush by grabbing at it whilst their mother was trying to brush their teeth. This behaviour was reported by these mothers as acting as a barrier to successful completion of tooth-brushing sessions. In some cases this tooth-brush grabbing was due to infant and preschooler desires to brush their own teeth. However, in other cases it may have been that some were not grabbing at the tooth-brush because they wanted to brush themselves, but rather because they were just grabbing at a moving object as infants and preschoolers tend to. Or they may have been grabbing the tooth-brush in order to remove it from their mouth because of a dislike of tooth-brushing. So for example, Participant 1 describes that her daughter would try to remove the tooth-brush from her mouth when she had grown tired of having her teeth brushed:“…when she’s had enough she’ll try taking the toothbrush away from me, so she won’t let me do it anymore.”
- (v)
- Infant/preschooler sleeping prevents parent from brushing their teeth: Some mothers (2/16) reported that if their infant or preschooler was sleeping they did not feel they could wake then in order to brush their teeth. This may have been due to parents being concerned about being able to get them to go back to sleep again, as Participant 2 describes:“I’ve skipped brushing his teeth ‘cos he’s in the car, he’s falling asleep, so I’m like, ‘I’m not waking you up to brush your teeth’.”
- (vi)
- Disliking toothpaste taste causes non-compliance during tooth-brushing: Some mothers (2/16) also reported that their infant or preschooler sometimes did not like the taste of toothpaste and that this could disrupt tooth-brushing routines. This finding concurs with anecdotal evidence from dentists that sometimes young children find the taste of certain toothpastes to be too strong, as Participant 11 describes about her own son:Participant. “It’s a bit hard not to use the children’s one ‘cos he doesn’t like the adult one.”Researcher. “Is that ‘cos of the taste?”Participant. “Yeah, it’s a bit too strong for him.”
“I have to wait for (husband) to come back and he does it…”Participant 14
“…definitely get along to the groups, the support groups. You can make friendships that aren’t just important to you personally, but also for the benefit of your children. And I think it helps you to cope with your life better, just generally.”Participant 5
- (i)
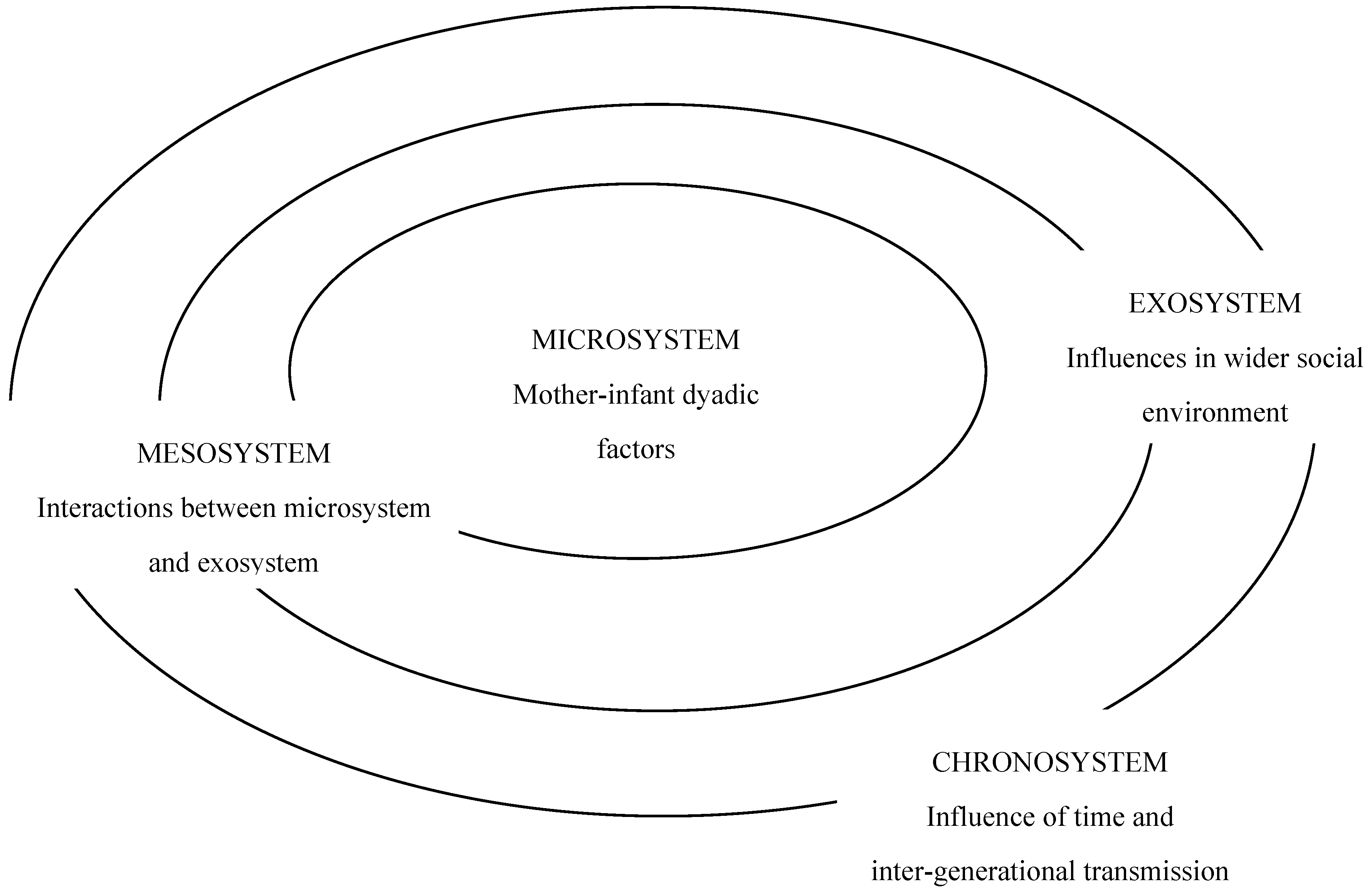
- Support provided by co-parent when establishing tooth-brushing routines: This sub-theme, although reported as lying within the ‘exosystem’ of Bronfenbrenner’s ecological model, could potentially be located within the ‘microsystem’. However, for the purposes of these analyses the ‘microsystem’ was conceptualised as any factors lying within the infant-principle caregiver dyad. Although co-parents (i.e., fathers) provided support with tooth-brushing within the family home environment, mothers in this study had significantly greater care-giving responsibilities than co-parents
Researcher. “And does your husband help out with things like tooth-brushing?”Participant. “yeah, he does. And she’s [infant] fine with it.”
- (ii)
- Professional advice received about tooth-brushing and establishing the routines: Three-quarters of mothers (12/16) spoke about having received some kind of advice about infant dental health from healthcare professionals such as health visitors and dentists. However, this advice was reported to be minimal and mainly related to the age when tooth-brushing should be initiated. So for example, Participant 4’s dentist advised her to introduce her baby as soon as possible to allow her to get used to it:Researcher. “Has the dentist given you any advice about how to care for (infant’s) teeth?”Participant. “I remember him saying just let her chew on the brush, like when she’s quite young…”
“I went to the weaning thing and one of the things at the weaning was about dental. I don’t remember it being particularly effective in telling me what to do, possibly ‘cos we’d already started [tooth-brushing]. But, erm, I think we definitely got leaflets about what they should and shouldn’t be eating.”
- (iii)
- Non-professional advice received about tooth-brushing and establishing the routines: Some mothers (3/16) reported that they had received advice from family members and friends, although this advice was about parenting more generally, rather than being specifically about dental health and tooth-brushing routines. So, as Participant 3 describes how she and her friends with young children would support one another and swap advice:“I’ve got friends that have children, so they would say how it was going and you would say how it [tooth-brushing] was going, and we’d give each other advice. If you’d gone through that already. You can share ideas.”
- (iv)
- General social support with establishing tooth-brushing routines and coping with child-rearing: Approximately two-thirds of mothers (10/16) interviewed reported that the social support they received from friends and family had been important in determining how well they coped more generally with caring for their infant. For example, Participant 5 described how important the parenting support groups she attended had been to her:“…definitely get along to the groups, the support groups. You can make friendships that aren’t just important to you personally, but also for the benefit of your children. And I think it helps you to cope with your life better, just generally.”
“…for me it’s just the norm and expected to brush your teeth twice a day. Whereas I’ve spoken to people over past few years and they only brush their teeth once day which is very strange to me. So culturally it’s from childhood, definitely.”
3.2. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Aunger, R. Tooth brushing as routine behaviour. Int. Dent. J. 2007, 57, 364–376. [Google Scholar]
- Huebner, C.; Riedy, C. Behavioral determinants of brushing young children’s teeth: Implications for anticipatory guidance. Pediatr. Dent. 2010, 32, 48–55. [Google Scholar]
- Amin, M.S.; Harrison, R.L. Understanding parents’ oral health behaviors for their young children. Qual. Health Res. 2009, 19, 116–127. [Google Scholar] [CrossRef]
- Nations, M.K.; Calvasina, P.G.; Martin, M.N.; Dias, H.F. Cultural significance of primary teeth for caregivers in northeast Brazil. Cad. Saude Publica 2008, 24, 800–808. [Google Scholar] [CrossRef]
- Riedy, C.A.; Weinstein, P.; Milgrom, P.; Bruss, M. An ethnographic study for understanding children’s oral health in a multicultural community. Int. Dent. J. 2001, 51, 305–312. [Google Scholar] [CrossRef]
- Hoeft, K.S.; Masterson, E.E.; Barker, J.C. Mexican American mothers’ initiation and understanding of home oral hygiene for young children. Pediatr. Dent. 2009, 31, 395–404. [Google Scholar]
- Folayan, M.; Owotade, F.; Adejuyigbe, E.; Sen, S.; Lawal, B.; Ndukwe, K. The timing of eruption of the primary dentition in Nigerian children. Am. J. Phys. Anthropol. 2007, 134, 443–448. [Google Scholar] [CrossRef]
- NHS. Teething Tips and Toothcare. Available online: http://www.nhs.uk/conditions/pregnancy-and-baby/pages/teething-and-tooth-care.aspx#close (accessed on 16 October 2009).
- Scher, A.; Sharabany, R. Parenting anxiety and stress: Does gender play a part at 3 months of age? J. Genetic Psychol. 2005, 166, 203–214. [Google Scholar] [CrossRef]
- Lejano, R.P.; Stokols, D. Social ecology, sustainability, and economics. Ecol. Econ. 2013, 89, 1–6. [Google Scholar] [CrossRef]
- Stokols, D. The Social Ecological Paradigm of Wellness Promotion. In Promoting Human Wellness: New Frontiers for Research, Practice, and Policy; University of California Press: Oakland, CA, USA, 2000; pp. 21–37. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Bronfenbrenner, U. Making Human Beings Human: Bioecological Perspectives on Human Development; Sage Publications, Inc.: New York, NY, USA, 2005. [Google Scholar]
- Bronfenbrenner, U.; Morris, P.A. The Bioecological Model of Human Development; John Wiley & Sons, Inc.: Hoboken, New Jersey, USA, 2006. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- NVivo 10. Nvivo qualitative data analysis software; Version 10; QSR Internation PTY, Limited: Warrington. UK, 2012.
- Adair, P.; Pine, C.; Burnside, G.; Nicoll, A.; Gillett, A.; Anwar, S.; Broukal, Z.; Chestnutt, I.; Declerck, D.; Ping, F. Familial and cultural perceptions and beliefs of oral hygiene and dietary practices among ethnically and socio-economically diverse groups. Community Dent. Health 2004, 21, 102–111. [Google Scholar]
- Sanders, M.R.; Woolley, M. The relationship between maternal self-efficacy and parenting practices: Implications for parent training. Child: Care Health Dev. 2005, 31, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.; Hesketh, K.; Silverii, A.; Abbott, G. Maternal self-efficacy regarding children’s eating and sedentary behaviours in the early years: Associations with children’s food intake and sedentary behaviours. Int. J. Pediatr. Obes. 2010, 5, 501–508. [Google Scholar] [CrossRef]
- Erikson, E.H. Identity and the Life Cycle: Selected Papers; International Universities Press Inc: New York, NY, USA, 1968. [Google Scholar]
- Newman, B.M.; Newman, P.R. Development through Life: A Psychosocial Approach; Wadsworth Publication Co.: Belmont, CA, USA, 2008. [Google Scholar]
- Emerson, E.; Einfeld, S. Emotional and behavioural difficulties in young children with and without developmental delay: A bi-national perspective. J. Child Psychol. Psychiatry 2010, 51, 583–593. [Google Scholar] [CrossRef]
- Ginsburg, K.R.; Committee on Communications; Committee on Psychosocial Aspects of Child and Family Health. The importance of play in promoting healthy child development and maintaining strong parent-child bonds. Pediatrics 2007, 119, 182–191. [Google Scholar] [CrossRef]
- Vygotsky, L. Mind in Society: The Development of Higher Psychological Processes; Harvard University Print: Cambridge, MA, USA, 1978. [Google Scholar]
- Shearer, D.M.; Thomson, W.M. Intergenerational continuity in oral health: A review. Community Dent. Oral Epidemiol. 2010, 38, 479–486. [Google Scholar] [CrossRef]
- DeVellis, R. Scale Development: Theory and Applications, 2nd ed.; AGE Publications, Inc: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Bandura, A. Guide for Constructing Self-Efficacy Scales. In Self-Efficacy Beliefs of Adolescents; Urdan, T., Pajares, F., Eds.; Information Age Publishing: Scottsdale, AZ, USA, 2006; Volume 5, pp. 307–337. [Google Scholar]
- Bloomfield, L.; Kendall, S.; Applin, L.; Attarzadeh, V.; Dearnley, K.; Edwards, L.; Hinshelwood, L.; Lloyd, P.; Newcombe, T. A qualitative study exploring the experiences and views of mothers, health visitors and family support centre workers on the challenges and difficulties of parenting. Health Soc. Care Community 2005, 13, 46–55. [Google Scholar] [CrossRef]
- Kendall, S.; Bloomfield, L. Developing and validating a tool to measure parenting self-efficacy. J. Adv. Nurs. 2005, 51, 174–181. [Google Scholar] [CrossRef]
- Bloomfield, L.; Kendall, S. Testing a parenting programme evaluation tool as a pre- and post-course measure of parenting self-efficacy. J. Adv. Nurs. 2007, 60, 487–493. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Elison, S.; Norgate, S.; Dugdill, L.; Pine, C. Maternally Perceived Barriers to and Facilitators of Establishing and Maintaining Tooth-Brushing Routines with Infants and Preschoolers. Int. J. Environ. Res. Public Health 2014, 11, 6808-6826. https://doi.org/10.3390/ijerph110706808
Elison S, Norgate S, Dugdill L, Pine C. Maternally Perceived Barriers to and Facilitators of Establishing and Maintaining Tooth-Brushing Routines with Infants and Preschoolers. International Journal of Environmental Research and Public Health. 2014; 11(7):6808-6826. https://doi.org/10.3390/ijerph110706808
Chicago/Turabian StyleElison, Sarah, Sarah Norgate, Lindsey Dugdill, and Cynthia Pine. 2014. "Maternally Perceived Barriers to and Facilitators of Establishing and Maintaining Tooth-Brushing Routines with Infants and Preschoolers" International Journal of Environmental Research and Public Health 11, no. 7: 6808-6826. https://doi.org/10.3390/ijerph110706808
APA StyleElison, S., Norgate, S., Dugdill, L., & Pine, C. (2014). Maternally Perceived Barriers to and Facilitators of Establishing and Maintaining Tooth-Brushing Routines with Infants and Preschoolers. International Journal of Environmental Research and Public Health, 11(7), 6808-6826. https://doi.org/10.3390/ijerph110706808