1. Introduction
Excessive exposure to mercury (Hg) during infancy can irreversibly damage normal infant development [
1]. In addition, because infants have a lower toxic metal tolerance than adults, even low-level Hg exposure can be harmful to the infant body [
2]. Recently, Hg levels were found to be higher in populations of Korean adults and school-age children compared with those in Western populations [
3,
4]. Compared with the data on Hg exposure in adults and older children, data on Hg exposure in post-neonatal infants are relatively scarce worldwide, as well as in Korea [
5,
6,
7].
In addition to adversely affecting neurodevelopment, Hg has also been reported to affect the physical growth of infants even at low levels of exposure [
2]. It has been postulated, although not yet established, that Hg can affect growth by damaging cell membranes and disturbing the function of enzymes in various metabolic pathways [
8,
9]. Among the studies investigating the influence of Hg on the growth of infants, the relationship between prenatal Hg exposure and birth outcomes has been most actively investigated using the Hg levels in umbilical cord blood or in maternal or neonate hair as biomarkers for body Hg burden [
10,
11]. There are conflicting reports concerning the significance of the relationship between low levels of prenatal Hg exposure and birth outcomes [
2,
12,
13,
14]. A few of these studies investigated the influence of prenatal Hg exposure on growth during infancy, and all of these studies showed a significant inverse association [
8,
10]. However, regarding the impact of ongoing low levels of postnatal Hg exposure on the growth of the infants, few studies have been available in the literature, although some studies have investigated this issue in representative populations at high levels of Hg exposure [
15,
16,
17].
Infancy, the first 1–2 years after birth, is regarded as the most important postnatal period for the growth of children. In addition, during late infancy, the transitional period of weaning, children are vulnerable to potential risk factors that might negatively affect healthy growth. For example, inadequate ingestion of supplementary food during the weaning period could lead to iron or zinc deficiency and insufficient protein or calorie intake, which have been reported to negatively affect the growth of children [
18,
19]. Low-level methyl Hg exposure during infancy has been shown to result from trans-placental acquisition from the mother, breastfeeding, or the consumption of fish as a complementary food [
20]. Among those potential sources, the latter two are assumed to contribute the most to body Hg burden in late infancy. Although breastfeeding (following fish intake by the mother), and direct fish intake as supplemental nutrition, are reportedly associated with increased Hg exposure in children, there are many beneficial effects of fish intake on infant health [
21], including nervous-system and immunity development. Thus a uniform restriction or avoidance of fish intake by mothers and infants without clear supporting evidence should not be recommended.
Better knowledge of the degree to which feeding and fish intake influence body Hg burden during complementary feeding and of the association between Hg exposure and growth during infancy could help provide a basis for better feeding recommendations for infants. In the literature, epidemiological studies examining the relationships among feeding, fish intake, and Hg exposure in weaning-age infants are limited. Therefore, this study aimed to assess the Hg exposure among healthy weaning infants in Korea using both hair and blood samples and to explore the relationships among Hg exposure, anthropometry, feeding method, and fish intake during infancy.
2. Materials and Methods
2.1. Subjects and Study Design
This study included Korean infants who visited the Pediatric Clinic of Seoul Metropolitan Government-Seoul National University Boramae Medical Center for health examinations and iron deficiency screening from June 2009 to May 2010 or from July 2013 to December 2014. All of the subjects were resided within Seoul city. The subjects were selected based on the following criteria: 6–24 months of age, healthy, no intake of herbal medicine, and no evidence of chronic diseases in the physical examination and medical history. The estimated number of the subjects was greater than 167 from sample size calculation based on our preliminary data (Type I error = 0.05, power = 0.8, partial correlation coefficient between anthropometric parameter and Hg content = −0.227, and assumed drop-out rate: 10%).
For each subject, we obtained information related to feeding from the parents or grandparents by experienced pediatricians using modified validated questionnaires [
22]. Dietary information included the dominant feeding method and its duration from birth to the time of the study, the monthly age at which fish was introduced as a complementary food to the infant, and the species of fish and the frequency of fish intake by the infant and mother (2013/2014 season only;
Table 1, Supplementary
Table S3). The dominant feeding methods were categorized as mostly breastfeeding, mostly formula feeding, mixed feeding, or others. The mostly breastfed infants were defined as those who were exclusively or dominantly breastfed before the introduction of complementary food and were mostly breastfed thereafter with supplemental complementary food until the time of the study or 6–12 months of age. The mixed-fed infants were defined as those who were exclusively or dominantly breastfed for at least 4–6 months after birth and were mostly formula fed thereafter with supplemental complementary food until the time of the study or 6–12 months of age. The mostly formula-fed infants were defined as those who were exclusively or dominantly fed formula for at least 4 to 6 months after birth and were mostly formula fed thereafter with supplemental complementary food until the time of the study or 6–12 months of age. The infants who were not classified as mostly breastfed, mixed fed, or mostly formula fed were defined as having “other” dominant feeding methods. The duration of breastfeeding was counted as the period of exclusive or mostly breastfeeding. The question concerning fish intake in the 2009/2010 season was: “Has your infant been fed fish-containing food regularly on a weekly basis?” In the 2013/2014 season, information on the precise frequency of fish intake was obtained. Thus, the duration of fish intake was ascertained for only infants who ingested fish more than once per week. The questionnaires also required that the names of commonly ingested fish species be recorded in the 2013/2014 season.
Anthropometric measurements were taken with the infant dressed in light clothing by experienced nurses as described previously [
23]. Z-scores for birthweight (BWZ), weight for age (WAZ), height for age (HAZ), and the difference of the weight percentiles between birth and the time of the study (WAZ-BWZ) were calculated using WHO Anthro (version 3.2.2., January 2011), which is available online (
http://www.who.int/childgrowth/software/en/). Other physical examinations were performed by experienced pediatricians.
Hair and blood samples from the subjects were collected with approval from the Boramae Hospital Institutional Review Board (IRB number 20090318/06-2009-32/82, 20130416/16-2013-55/051), and informed consent was obtained for all participants in the study.
2.2. Hair Hg Analysis
We collected approximately 120 mg of hair by cutting approximately 3 cm of hair from the back of the infant’s head with sterilized, stainless steel scissors. The hair Hg analysis was performed by Trace Elements, Inc. (Dallas, TX, USA), a professional institution specializing in hair mineral analysis.
The hair samples were washed to eliminate microelements settled inside the hair tissue and pollutants such as dust, sweat, and debris from the atmosphere and outer environment. After the hair samples were placed into 50 mL tubes, 25 mL Triton X-100 was added, and the samples were vigorously vortexed for 5 s. The process was then repeated four times. Next, 25 mL acetone was added, and the samples were again vigorously vortexed for 5 s. Next, 30 mL deionized water was added, and the samples were placed in a large ultrasonic bath and sonicated for 10 min. The sonication process was repeated three times. The acetone wash step was repeated twice, after which the samples were placed into a preheated drying oven (75 ± 5 °C) for 15 min. After that, each hair sample was finely cut into 1–2 mm sections using stainless steel scissors and mixed to ensure homogeneity. The cut hair was weighed to the nearest 0.001 g on an analytical-grade balance (Ohaus Explorer, Ohaus Corporation, Parsippany, NJ, USA) and then placed in a uniquely labeled, single-use, sterile polypropylene test tube. An aliquot of concentrated 70% trace metal-grade nitric acid (Fox Instrapure, Fox Scientific, Alvarado, TX, USA) was dispensed into each test tube. The tubes were then capped with sterile, two-position test tube caps, racked into a sample holder, and placed into a computer-controlled microwave digestion system (MARS 5, CEM Corporation, Matthews, NC, USA). After the microwave digestion procedure was complete, the samples were rehydrated with a diluent consisting of 18 MΩ de-ionized water and a solution of gold and a trace of HCl acid. The samples were then re-capped and mixed in a vortex mixer to ensure a uniform solution. From that point, the finished samples were placed into test tube racks to await analysis. Quantitative analysis was performed by Inductively Coupled Plasma Mass Spectrometry using the Elan 6100 and Elan 9000 analytical systems (Perkin Elmer, Akron, OH, USA).
In-line internal standardization and external calibration using certified standard solutions (Spex Certiprep, Metuchen, NJ, USA) traceable to the National Institute of Standards and Technology were used for the quantitative analysis. The reliability of the analysis performed by Trace Elements Inc. was monitored using four levels of standard material controls (two in an inorganic matrix and two in an organic matrix). The yearly mean Hg value from 2009 through 2014 was 0.11 μg/g (standard deviation = 0.02 μg/g; coefficient of variation n = 18.2%). Proficiency testing was performed on a twice-yearly basis. This laboratory participates in the Quebec Multi-element External Quality Assessment Scheme program administered by the Quebec National Institute of Health in Quebec, Canada.
2.3. Blood Tests
To screen for iron deficiency, complete blood counts, iron/TIBC, and ferritin levels were measured in the hospital laboratory as previously described [
23]. Iron deficiency (ID) was defined as a ferritin value <12 ng/mL and iron deficiency anemia (IDA) as Hg level < 11.0 g/dL with ID.
Blood Hg was examined only in the 2013/2014 season. For the blood Hg analysis, whole blood was collected in a 6 mL trace element K2 EDTA vacutainer tube (Becton Dickinson, Franklin Lakes, NJ, USA) by venipuncture from the cubital fossa or dorsum of the hand. One hundred microliters whole blood was mixed with diluent consisting of 0.05% Triton X-100, 5% butanol, 0.05% EDTA, and 0.5% NH
4OH. The Hg level in the whole blood was determined by Inductively Coupled Plasma Mass Spectrometry (Agilent 7700, Agilent, CA, USA) at the Greencross Reference Laboratory (Yongin-City, Kyunggi-do, Korea). In-line internal standardization and external calibration using certified standard solutions (Agilent, Santa Clara, CA, USA; PerkinElmer, Akron, OH, USA) traceable to the National Institute of Standards and Technology were used for the quantitative analysis. The reliability of the analysis was monitored using three levels (low: 1.49 ± 0.26, mid: 6.35 ± 0.80, high: 7.98 ± 0.80 ug/L) of control materials (ClinChek-Control, Recipe, Germany). The cumulative coefficients of variation of control materials for Hg during study period were 4.54%–4.84%. Proficiency testing was performed twice yearly by the German External Quality Assessment Scheme program (
http://www.g-equas.de/).
2.4. Statistical Analysis
Normality was tested by the Kolmogorov-Smirnov test. Among continuous variables, anthropometric Z-scores showed normal distribution. These values were expressed as means and 95% confidence interval (CIs) and were tested using independent-samples t-test or ANOVA. Other continuous variables including Hg level in hair and blood did not show normal distribution, therefore, they were expressed as medians and corresponding 25th and 75th percentiles (interquartile range, IQR) and were tested using the Mann-Whitney or the Kruskal-Wallis test. Categorical variables were compared using the Chi-squared test. Correlations between continuous variables were tested with Spearman’s rank coefficient. To determine the association between the Hg level and dietary factors, the data were analyzed using ordinal logistic regressions with the Hg content as the dependent variable and age, sex, anthropometric data, feeding method, monthly duration of fish intake, and iron status as explanatory variables. For the association between the hair Hg content and anthropometry, we performed multiple linear regression analysis with the Z-score as the dependent variable and age, sex, gestational age, feeding method, fish intake, iron status, and hair Hg level as explanatory variables. All analyses were conducted using SPSS version 20.0 at significance level (p < 0.05) (SPSS, Chicago, IL, USA).
Table 1.
Demographic, anthropometric, and diet-related parameters and iron status of 252 infants according to the study periods.
Table 1.
Demographic, anthropometric, and diet-related parameters and iron status of 252 infants according to the study periods.
| Characteristics | Total | 2009/2010 | 2013/2014 | p Value a |
|---|
| Subjects, n | 252 | 111 | 141 | |
| Age, months b | 11.1 (10.2, 12.0) | 11.0 (9.9, 12.35) | 11.0 (10.3, 12.0) | 0.571 c |
| Gender, n | | | | |
| | Male | 125 | 55 | 70 | 0.988 |
| | Female | 127 | 56 | 71 | |
| Gestational age, weeks b | 39.0 (38.0, 40.0) | 39.0 (38.0, 40.0) | 39.0 (38.0, 40.0) | 0.972 c |
| | <37 weeks, n | 12 | 5 | 7 | 0.969 |
| Anthropometry, Z-score d | | | | |
| | Birthweight, kg | 3.25 (3.20, 3.30) | 3.28 (3.20, 3.35) | 3.23 (3.17, 3.30) | 0.404 e |
| | birthweight <2.5 kg, n | 9 | 2 | 7 | 0.232 |
| | birthweight | −0.11 (−0.21, −0.01) | −0.04 (−0.21, 0.12) | −0.16 (−0.29, −0.02) | 0.302 e |
| | weight for age | 0.13 (0.02, 0.24) | 0.51 (0.34, 0.69) | 0.53 (0.39, 0.67) | 0.466 e |
| | WAZ-BWZ f | 0.63 (0.51, 0.76) | 0.55 (0.34, 0.76) | 0.69 (0.54, 0.84) | 0.298 e |
| | height for age | 0.55 (0.41, 0.69) | 0.51 (0.28, 0.75) | 0.59 (0.41, 0.77) | 0.290 e |
| Dominant feeding method, n | | | | |
| | mostly breast fed | 144 | 82 | 62 | <0.001 |
| | mixed fed | 31 | 4 | 27 | |
| | mostly formula fed | 66 | 25 | 41 | |
| | others | 11 | 0 | 11 | |
| Duration of mostly breastfeeding, months b | 6.0 (0.0, 10.9) | 9.9 (0, 11) | 6.0 (0, 10.95) | 0.308 c |
| Fish intake (n = 241) | | | | |
| | Presence, n (%) | 134 (55.6) | 61(61.0) | 73 (51.8) | 0.155 |
| | Absence, n | 107 | 39 | 68 | |
| Duration of fish intake, months b | 1.0 (0.0, 2.0) | 1.0 (0.0, 3.0) | 0.0 (0.0, 2.0) | 0.204 c |
| Frequency of fish intake by infants, n | | 141 (100) | |
| | <1/week | | | 68 (48.2) | |
| | 1–2/weeks | | | 62 (44.0) | |
| | ≥3/weeks | | | 11 (7.8) | |
| Iron status, n | | | | |
| | Deficiency | 83 | 52 | 31 | <0.001 |
| | No deficiency | 169 | 59 | 110 | |
| | Iron deficiency anemia | 39 | 24 | 15 | 0.019 |
4. Discussion
Our study shows that the body Hg burden in healthy Korean weaning-age infants residing in Seoul city is usually within the range recommended by the Environmental Protection Agency (EPA) and has been decreasing recently [
24,
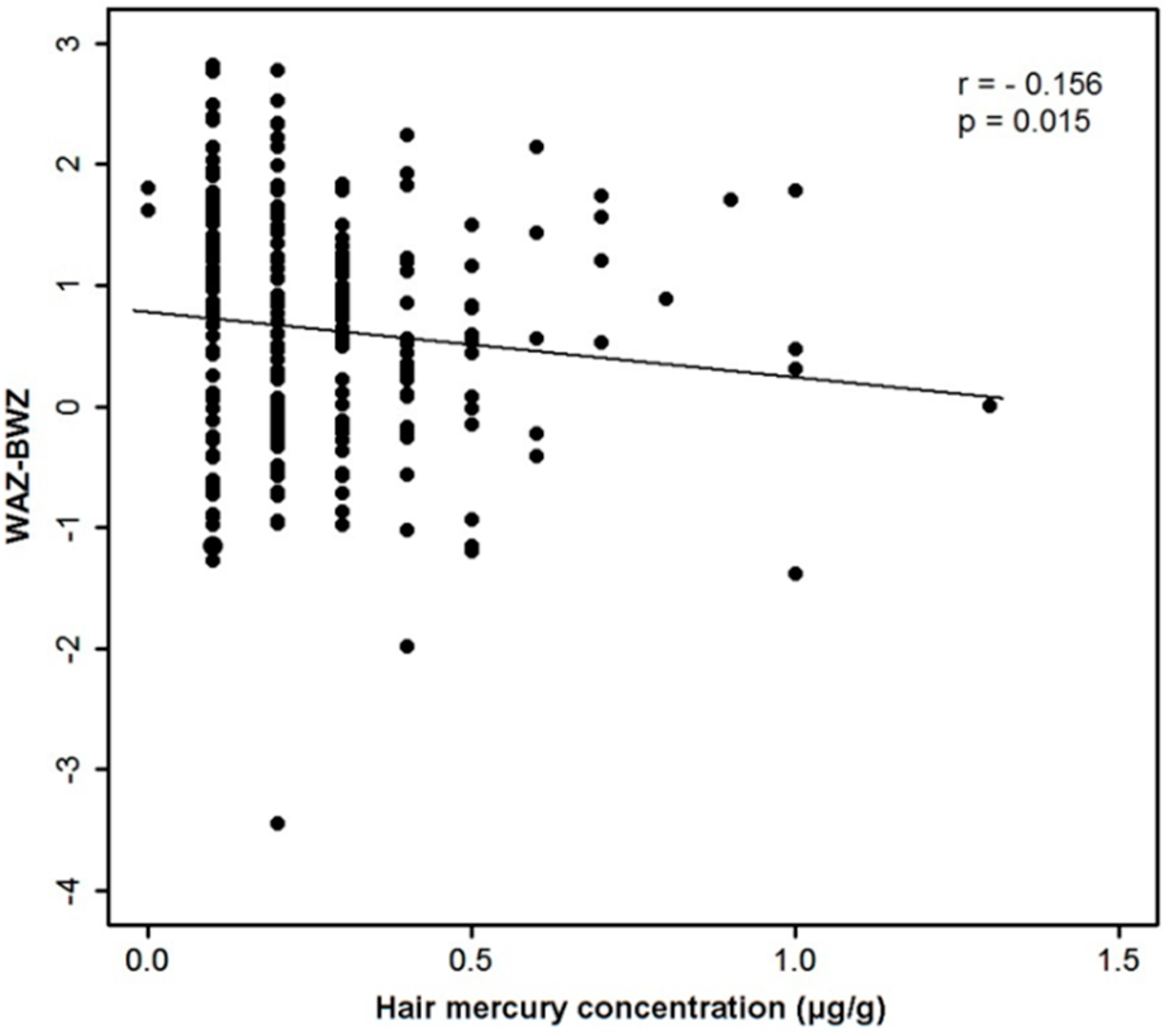
25]. Hg exposure at that level may not significantly affect anthropometry during infancy. Although there was a significant inverse correlation between the hair Hg content and weight gain among our subjects, the association disappeared after adjustment for the feeding method or the duration of breastfeeding, which make a far greater contribution to the anthropometry of infants than the body Hg burden. To our knowledge, this is one of the first reports to clarify the relationship among hair Hg content, anthropometry, and breastfeeding during weaning-age infancy using Hg levels in both hair and blood samples as biomarkers for chronic and recent exposure. In addition, we demonstrated that the Hg content in hair and whole blood is closely correlated with diet patterns in infancy, both breast-milk or formula feeding and the consumption of solids such as fish. Although our investigation was limited because fish intake was not precisely quantified and fish species ingested by infants and mothers was not examined thoroughly, we found significant correlations among feeding, fish intake, and Hg exposure that are comparable with the results of previous reports in older populations.
As for the body Hg burden in Korean infants, previous studies reported relatively higher Hg levels in neonates [
8,
26]. In the Mothers and Children’s Environmental Health study conducted in 2006, the geometric mean cord-blood Hg level among 797 neonates was 5.2 μg/L, and the level was more than 5.8 μg/L in as many as 39.1% of the subjects [
8]. Beyond the neonatal age, one study performed in 2006 with 111 Korean mother-child pairs residing in a coastal area revealed that the hair Hg content of children approximately three years of age had a mean of 0.62 μg/g and was >1 μg/g in 17.9% of the children [
5]. That study included only a small, undocumented number of infants. Compared with those previous studies, the Hg content in our subjects was relatively low, and it decreased significantly in 2013/2014 (geometric mean hair Hg: 0.18 μg/g) compared with that in 2009/2010 (geometric mean hair Hg: 0.28 μg/g). No subjects in 2013/2014 showed a blood Hg value greater than the US EPA limit of 5.8 μg/L. The body Hg content in weaning-age infants might be lower than that in neonates, adults, or older children, and it might decrease in pregnant women and babies, probably because of reduced fish intake by pregnant mothers for fear of Hg hazard to the fetus or radiation exposure after March 2011, at which time a nuclear power-plant disaster occurred in Japan. The relatively low Hg levels in our study subjects are still much higher, however, than those in older children in Western countries [
27,
28,
29]. Further studies are needed to document whether this level of Hg exposure leads to adverse neurodevelopmental consequences. Recently, increasing evidence has demonstrated that the cognitive benefits of fish consumption during pregnancy outweigh the toxic effects of Hg exposure [
21]. Therefore, the monitoring of Hg exposure through seafood consumption needs to be balanced with education efforts regarding the beneficial effects of unsaturated fatty acids on the neurodevelopment of children through ingestion of oily fish.
So far, the results concerning the influence of Hg exposure on the growth of children are debatable [
2]. A significant inverse association between Hg exposure and growth has been observed in some, but not all, studies of both populations with relatively low levels of Hg exposure and definitively high levels of Hg exposure [
12,
15,
16,
17]. Incomplete adjustment for other factors influencing the growth of children might be one of the possible explanations for the discordant results among the studies. In a study of 171 infants in the Faroe Islands with high levels of Hg exposure (the geometric mean of cord-blood Hg was 20.3 μg/L) [
15], the weight of infants at 18 months was independently associated with postnatal Hg exposure through breastfeeding apart from prenatal Hg exposure. The association remained significant after adjustment for the adverse influence of breastfeeding itself on growth. However, in this study, the biomarker for postnatal Hg exposure was not directly measured but was instead estimated from the cord-blood Hg and the duration of breastfeeding. Therefore, our study is probably one of the first to investigate the influence of directly measured, low-level Hg exposure during the postnatal period on growth while considering the confounding effect of breastfeeding. We suggest that to document the influence of Hg exposure on the postnatal growth of infants, adjustment should be made for the breastfeeding effect.
The relative slow growth in breastfed infants compared with formula-fed infants during the first few years of life are well documented [
30,
31,
32,
33]. Although toxic contaminants such as Hg or polychlorinated biphenyls above certain levels might contribute to the relative slow growth in breastfed infants [
15], low-level exposure to contaminants such as that among our subjects might not significantly affect the postnatal growth of infants. Recently, the relatively slow growth pattern of breastfed infants has been regarded as physiological, whereas the accelerated early growth pattern of formula-fed infants can be regarded as a risk factor for future obesity [
30,
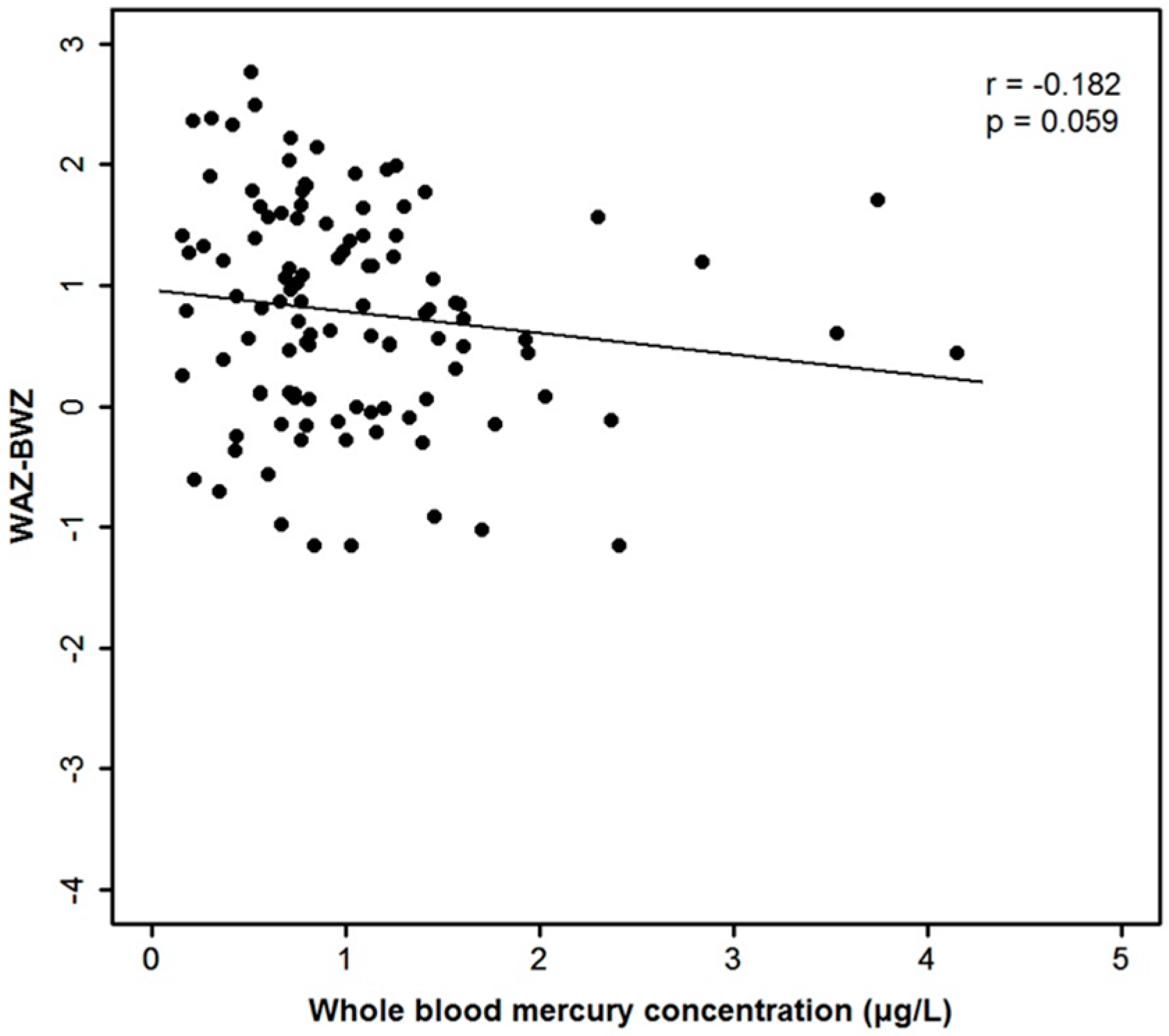
34]. One of the limitations of our study is that the cord-blood Hg level was not measured at birth. Hence, the association between prenatal Hg exposure and the anthropometry of neonates or infants could not be evaluated. The number of low birth weight infants was significantly higher, however, in the group of infants with the lowest hair Hg content compared with that in the other groups (
Table 3,
p = 0.013). Furthermore, the hair and blood Hg contents of the infants were not significantly correlated with growth at birth. Thus, if postnatal Hg exposure in infants is assumed to be correlated with prenatal Hg exposure [
5,
35], it is possible that prenatal growth might not be inversely correlated with prenatal Hg content in our study population.
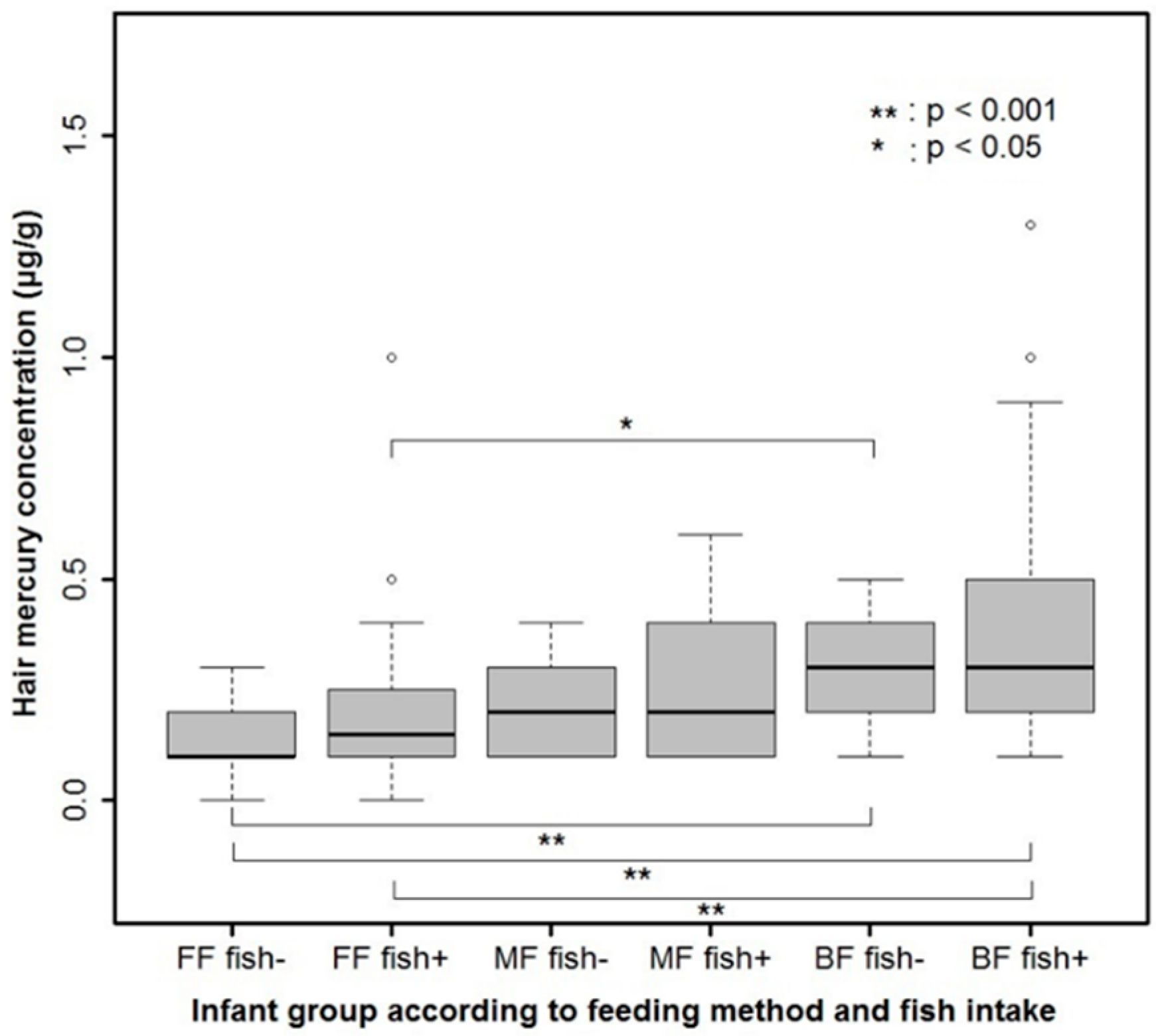
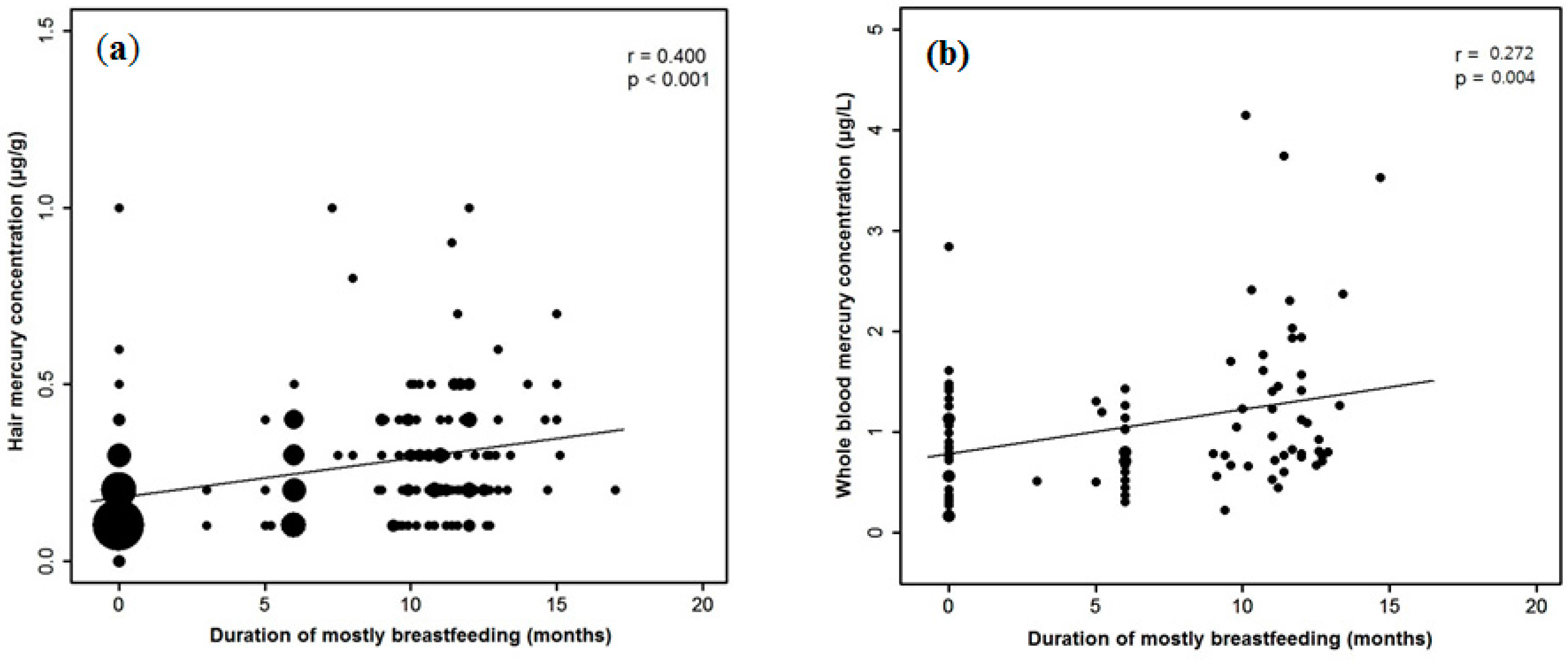
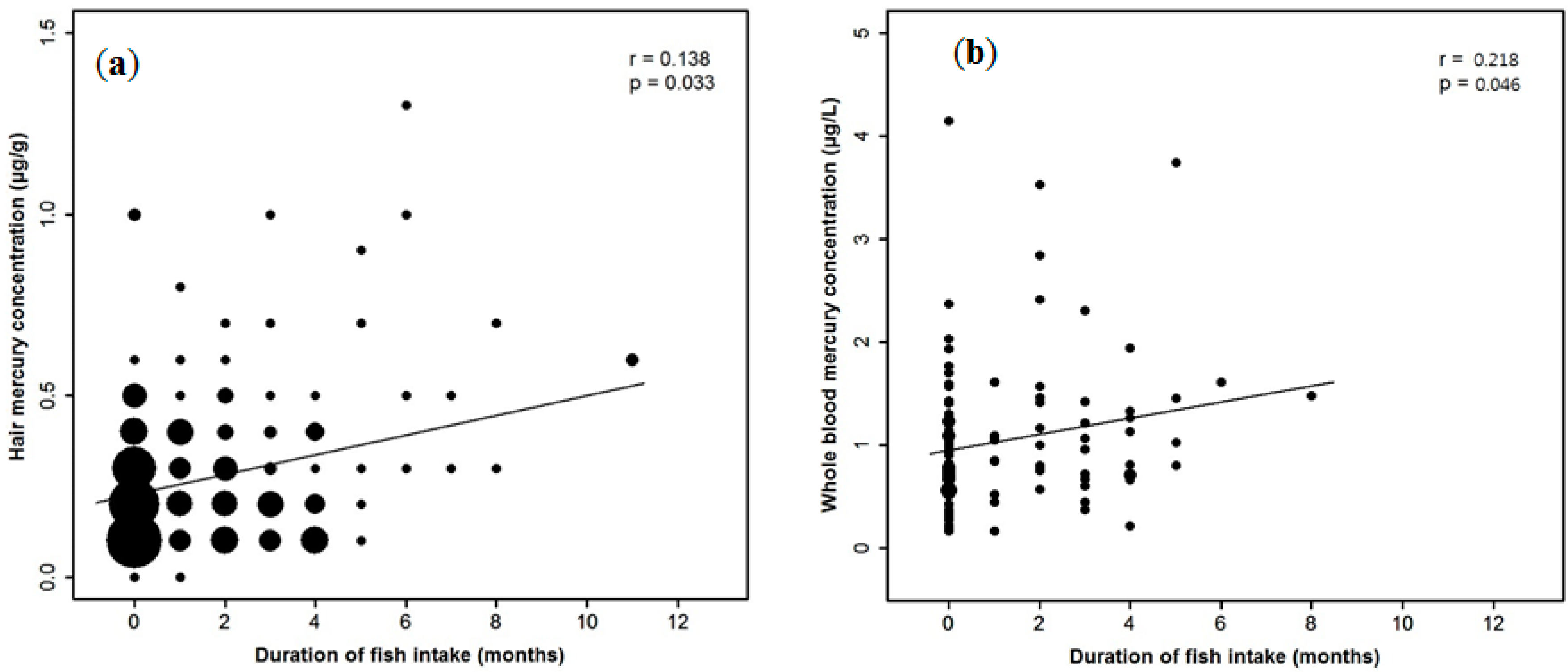
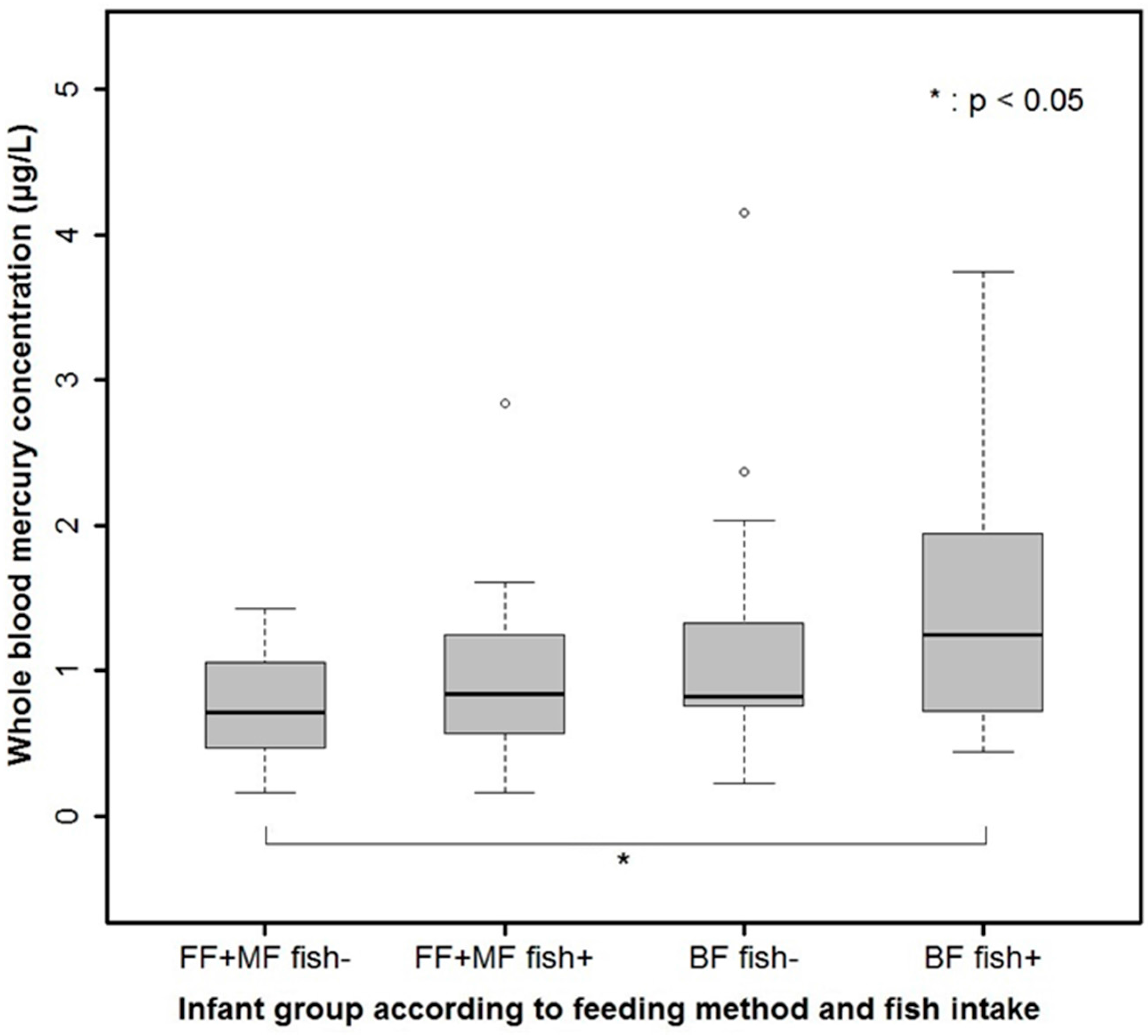
In our study, the feeding method or duration of breastfeeding and the duration of fish intake were independently and significantly correlated with the Hg content of both the hair and the blood in late infancy. The duration of breastfeeding might reflect the amount of Hg exposure from the mother, which is probably mainly associated with the fish intake of the mother. Therefore, the fish intake of both the mother and the infant are important sources of Hg exposure in late infancy. The recommended amount, frequency, starting age, and type of fish intake as a complementary food by infants who continue breastfeeding after exclusively or mostly breastfeeding for the first six months of life, may need to be determined with caution, and the information regarding the balance of Hg and unsaturated fatty acid intake via oily fish should be given to parents. In our study, Hg exposure significantly decreased in the 2013/2014 season compared with that in the 2009/2010 season, which can be explained by the significant difference in the breastfeeding rate between the two periods. In addition, although not statistically significant, there was a tendency for children enrolled in 2009/2010 to start eating fish earlier and more frequently than those enrolled in 2013/2014. Since the fish intake patterns of children are usually associated with those of their mothers, Hg exposure through breastfeeding, which is closely associated with the fish-intake pattern of the mother, might also be higher in the children examined in 2009/2010. In our study, a precise history of the frequencies and type of fish intake by the mothers and infants was taken only in 2013/2014; thus, a direct comparison of the amount of fish intake between the two periods was not possible. However, the proportion of mothers who ate fish more than once per week and more than three times per week was 19/95 (20.0%) and 4/95 (4.2%), respectively, which is far less than the 33/63 (52.4%) and 9/63 (14.3%) pregnant women residing in Seoul who did so in a 2004 study [
36]. The Hg exposure in the general Korean population has also been reported to be decreasing through 2008–2011 [
25].
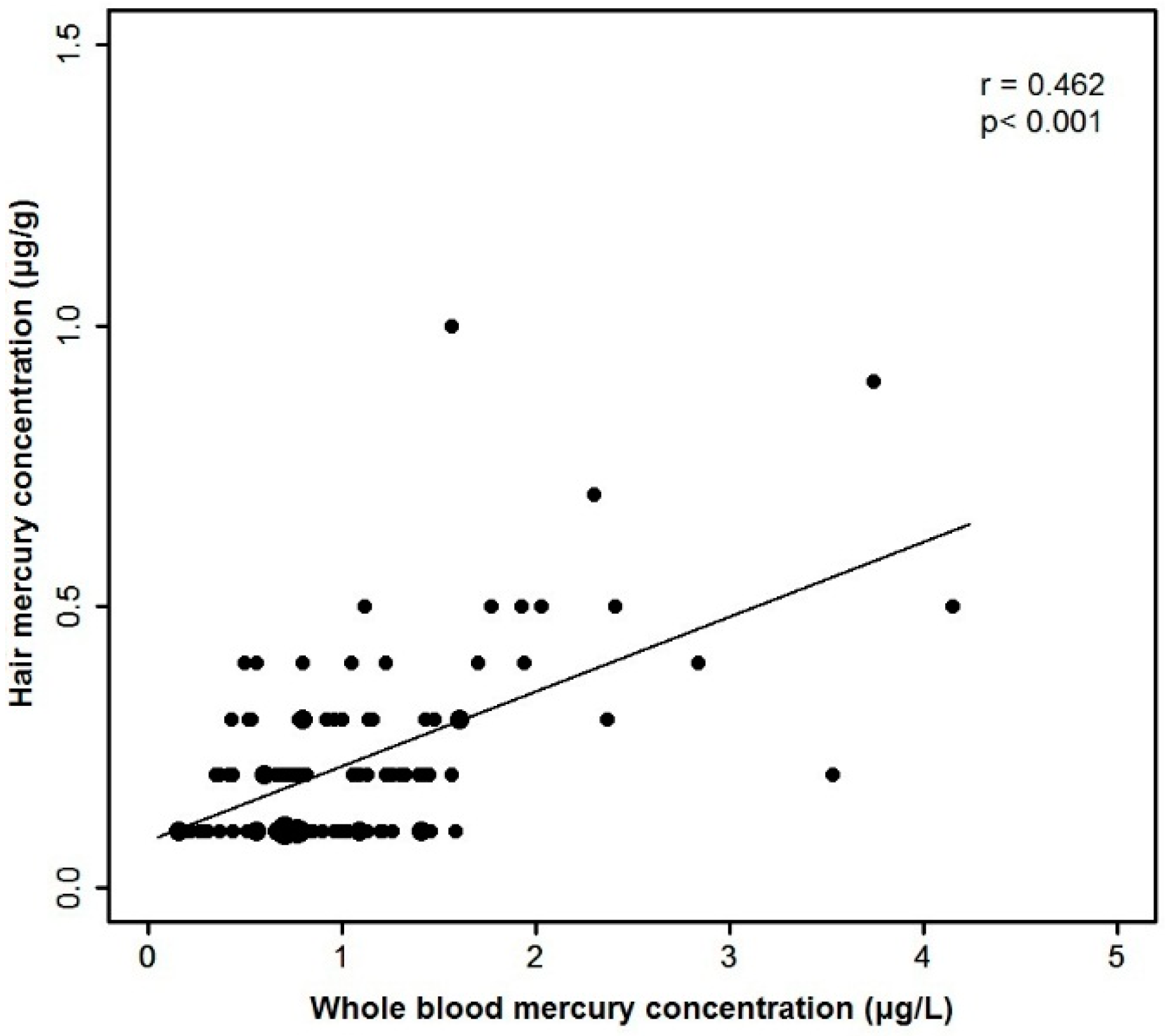
Finally, the hair Hg content was strongly correlated with the blood Hg content in late infancy, which is compatible to the results of many previous studies in adults [
37,
38]. The ratio between the hair and blood Hg concentrations (median 202.7) is also close to the ratios of the Hg contents of maternal hair and cord blood found in previous studies [
10,
38,
39]. Although both hair and blood Hg levels have been considered reliable biomarkers for the body burden of methyl Hg, they represent different time frames and, thus, might not necessarily be correlated [
40]. While the whole-blood Hg content represents recent Hg exposure with a half-life of approximately 60 days, the hair Hg content represents previous chronic exposure of varying duration [
41]. If a 3 cm length of hair is examined, the resulting Hg content might represent approximately three months of exposure in adults and about five months of exposure in infants [
42]. This difference between the two biomarkers were reflected in slightly different results between hair Hg- and blood Hg-related analyses in our study, although the major results of the analyses on Hg content and diet were in agreement between the hair and blood-related analyses. For example, the median duration of fish intake in the 2013/2014 season was less than one month, which might explain the observation that the blood Hg content, but not the hair Hg content, significantly correlated with the duration of fish intake by the infants during the 2013/2014 season (
Table 3,
Figure S3); blood Hg content more accurately reflects recent exposure compared with the hair Hg content. This was also reflected in the finding that the blood Hg level of mixed-fed infants (who were mostly formula fed during late infancy) and formula-fed infants were not significantly different in contrast to the result of hair Hg related analyses (Supplementary
Table S1 and
Table S2).


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






