
A Simple Risk Score for Identifying Individuals with Impaired Fasting Glucose in the Southern Chinese Population


Abstract
:1. Introduction
2. Methods
2.1. Population for Establishing the Risk Scores
2.2. Population for Validating the Risk Scores
2.3. Data Collection
2.4. Diagnostic Criteria for Impaired Fasting Glucose (IFG)
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Populations

{kind=link}
{kind=link}
| Variable or Statistic | Derivation Sample | Validation Sample 1 | Validation Sample 2 | Validation Sample 3 | P a Value |
|---|---|---|---|---|---|
| N (% of men) | 6033 (32.0) | 1186 (37.8) | 3162 (28.4) | 1289 (28.4) | -- |
| Mean age (year) | 51.6 ± 12.7 | 49.4 ± 13.2 | 57.5 ± 5.2 | 43.6 ± 14.3 | <0.001 |
| BMI(kg/m2) | 23.5 ± 3.4 | 23.0 ± 3.3 | 23.3 ± 3.2 | 24.2 ± 4.0 | 0.04 |
| Waist circumference(cm) | 79.1 ± 9.4 | 77.7 ± 9.3 | 82.4 ± 9.1 | 82.4 ± 12.1 | <0.001 |
| Systolic blood pressure (mmHg) | 123.4 ± 19.7 | 128.6 ± 20.8 | 123.6 ± 17.7 | 120.5 ± 22.9 | 0.002 |
| Diastolic blood pressure (mmHg) | 79.1 ± 10.6 | 81.6 ± 10.3 | 78.2 ± 10.7 | 82.4 ± 14.0 | 0.01 |
| Fast blood glucose (mmol/L) | 5.54 ± 1.49 | 5.63 ± 1.52 | 4.77 ± 1.46 | 4.92 ± 1.35 | 0.03 |
| Number of patients with IFG | 384 | 106 | 95 | 37 | -- |
| IFG (%) | 6.2 | 8.9 | 3.0 | 2.9 | 0.02 |
| Obesity (%) b | 9.0 | 6.9 | 7.1 | 16.9 | 0.01 |
| Central obesity (%) c | 32.4 | 34.6 | 41.6 | 45.5 | 0.02 |
| Hypertension (%) | 32.8 | 33.7 | 34.3 | 30.3 | 0.33 |
| Family history of diabetes (%) | 17.6 | 6.1 | 16.3 | 2.2 | <0.001 |
3.2. Development of the Risk Scores
| Variable or Statistic | Men | Women | ||||
|---|---|---|---|---|---|---|
| β Coefficient | OR (95% CI) | Score | β Coefficient | OR (95% CI) | Score | |
| Age(years): 20–39 | -- | 1.00 | 0 | -- | 1.00 | 0 |
| 40–49 | 1.77 | 5.85 (1.68–20.34) | 18 | 1.10 | 3.00 (1.53–5.90) | 11 |
| 50–59 | 1.95 | 6.99 (2.12–23.03) | 19 | 1.53 | 4.59 (2.42–8.72) | 15 |
| Over 60 | 2.04 | 7.69 (2.33–25.40) | 20 | 1.95 | 7.03 (3.68–13.41) | 20 |
| Waist circumference(cm): men <90,women <80 | -- | 1.00 | 0 | -- | 1.00 | 0 |
| men ≥90,women ≥80 | −0.12 | 0.89 (0.55–1.43) | −1 | 0.54 | 1.72 (1.20–2.48) | 5 |
| Family history of diabetes: | ||||||
| No | -- | 1.00 | 0 | -- | 1.00 | 0 |
| Yes | 0.16 | 1.18 (0.69–2.01) | 2 | 0.46 | 1.58 (1.12–2.22) | 5 |
| BMI: BMI < 24 | -- | 1.00 | 0 | -- | 1.00 | 0 |
| 24 ≤ BMI < 28 | 0.44 | 1.56 (0.93–2.61) | 4 | 0.09 | 1.09 (0.76–1.58) | 1 |
| BMI ≥ 28 | 0.93 | 2.54 (1.33–4.86) | 9 | 0.49 | 1.63 (1.00–2.64) | 5 |
| Hypertension: No | -- | 1.00 | 0 | -- | -- | -- |
| Yes | 0.78 | 2.19 (1.43–3.35) | 8 | -- | -- | -- |
| Maximum score | 38 | 35 | ||||
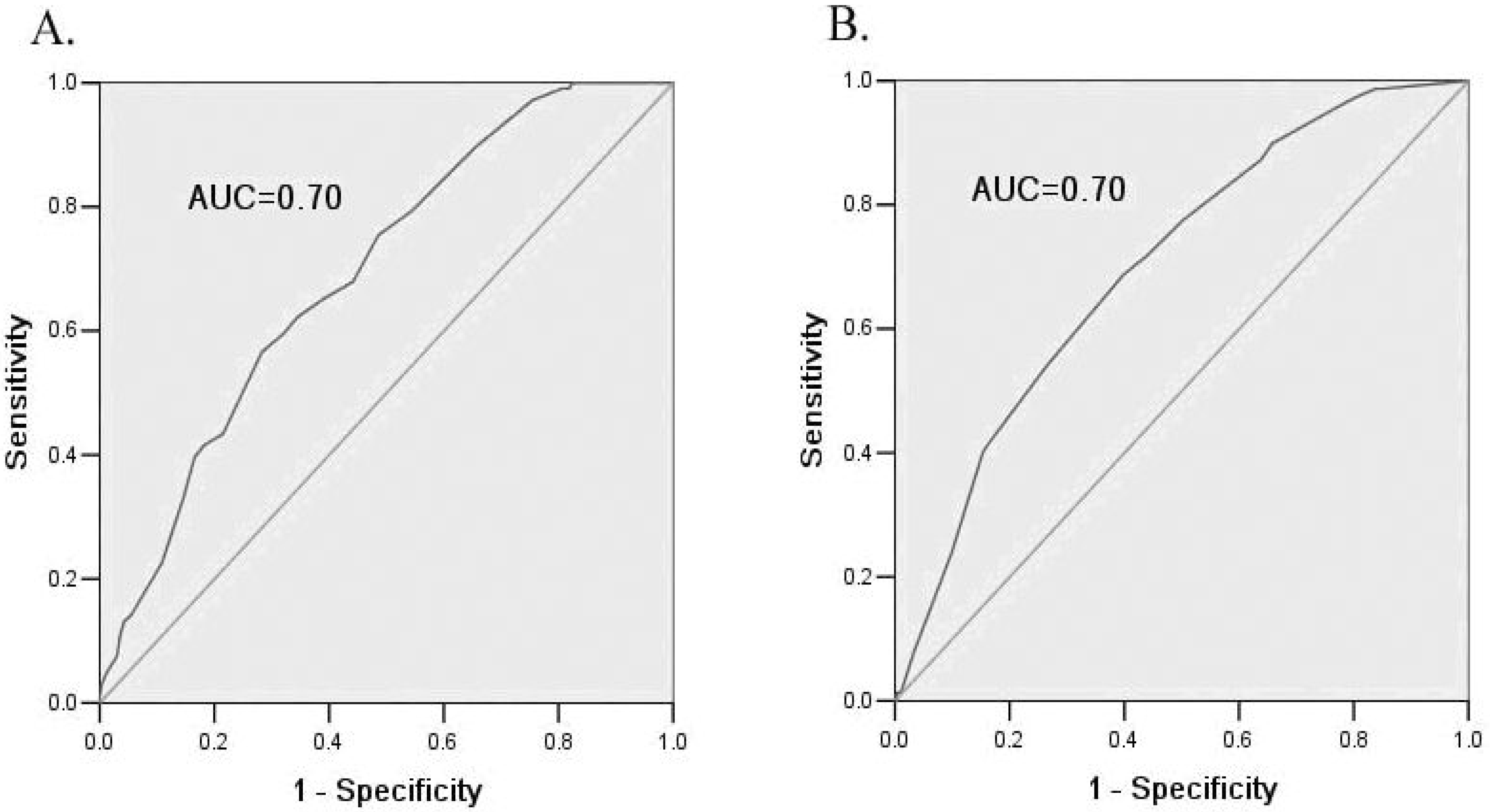
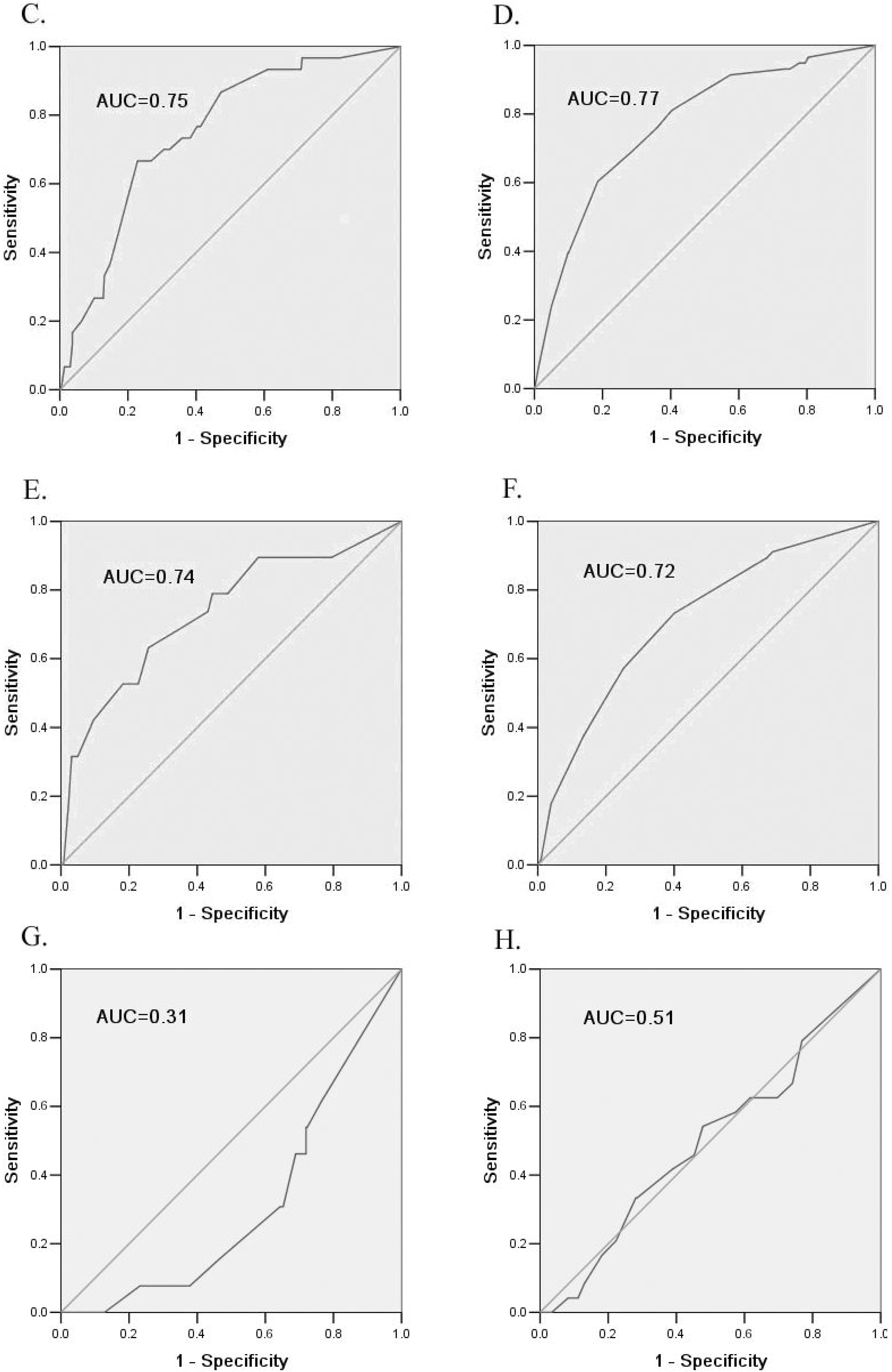
3.3. Internal and External Validation of the Risk Scores
| Validation | Model for Men | Model for Women |
|---|---|---|
| Internal validation studies in the derivation sample | ||
| Goodness of fit(P value) | 0.40 | 0.38 |
| ROC c-statistic(95% CI) | 0.70 (0.65–0.74) | 0.70 (0.67–0.73) |
| External validation studies in the validation sample 1 | ||
| Goodness of fit(P value) | 0.59 | 0.96 |
| ROC c-statistic(95% CI) | 0.75 (0.67–0.83) | 0.77 (0.71–0.83) |
| External validation studies in the validation sample 2 | ||
| Goodness of fit(P value) | 0.78 | 0.56 |
| ROC c-statistic(95% CI) | 0.74 (0.61–0.86) | 0.72 (0.65–0.78) |
| External validation studies in the validation sample 3 | ||
| Goodness of fit(P value) | 0.49 | 0.54 |
| ROC c-statistic(95% CI) | 0.31 (0.20–0.43) | 0.50 (0.38–0.61) |


| Total Score | Number (%) | Sensitivity(%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|
| Derivation sample | |||||
| Model for men | |||||
| ≥23 | 747 (50.5) | 75.5 | 51.4 | 12 | 97 |
| Model for women | |||||
| ≥16 | 1755 (52.1) | 77.5 | 49.8 | 10 | 97 |
| Validation sample 1 | |||||
| Men (≥23) | 136 (41.5) | 73.3 | 64.1 | 13 | 97 |
| Women (≥16) | 255 (44.4) | 81.0 | 59.7 | 19 | 96 |
| Validation sample 2 | |||||
| Men (≥23) | 430 (51.7) | 78.9 | 51.0 | 6 | 99 |
| Women (≥16) | 1254 (58.1) | 89.3 | 41.8 | 5 | 99 |
| Validation sample 3 | |||||
| Men (≥23) | 160 (41.1) | 30.8 | 48.8 | 2 | 96 |
| Women (≥16) | 362 (40.5) | 41.7 | 59.0 | 4 | 96 |
3.4. Comparison of the Current Risk Scores with Other Existing Scores for Pre-Diabetes
| Derivation Population (Publication Year) | Predictors Involved | Optimal Cut-Off Value (Range) | Area under the (95%CI) | Sensitivity at the Optimal Cut-Off Value (%) | Specificity at the Optimal Cut-off Value (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In Original Population | In the Population of This Study | p Value * | In Original Population | In the Population of This Study | In Original Population | In the Population of This Study | ||||||
| USA (2008) | Age, sex, BMI, hypertension, family history of diabetes, resting heart rate | 5 (0–16) | 0.74 | 0.66 (0.63–0.68) | 0.04 | 87.0 | 92.0 | 43.3 | 26.4 | |||
| Shanghai, China (2009) | Age, waist circumference, family history of diabetes, systolic blood pressure | 5 (4–11.7) | 0.70 | 0.67 (0.64–0.70) | 0.06 | 68.2 | 68.5 | 61.7 | 54.9 | |||
| Chengdu, China (2010) | Age, occupational physical activity, family history of diabetes, BMI, central obesity, hypertension, leisure physical activity, gestational diabetes, number of deliveries | Men: 5 (0–18) | Men: 0.72 (0.69–0.74) | Men: 0.66 (0.61–0.72) | 0.06 | Men: 74.1 | Men: 73.3 | Men: 58.4 | Men: 54.2 | |||
| Women: 6 (0–22) | Women: 0.73 (0.71–0.75) | Women: 0.67 (0.63–0.71) | Women: 75.6 | Women: 44.5 | Women: 65.6 | Women: 76.1 | ||||||
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Davidson, M.B. Metabolic syndrome/insulin resistance syndrome/pre-diabetes: New section in diabetes care. Diabetes Care 2003, 26. [Google Scholar] [CrossRef]
- King, H.; Aubert, R.E.; Herman, W.H. Global burden of diabetes, 1995–2025: Prevalence, numerical estimates, and projections. Diabetes Care 1998, 21, 1414–1431. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.A.; Hillier, T.A.; Brown, J.B. Progression from newly acquired impaired fasting glusose to type 2 diabetes. Diabetes Care 2007, 30, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Mayige, M.; Ogbera, A.O.; Sobngwi, E.; Kengne, A.P. Screening for hyperglycemia in the developing world: Rationale, challenges and opportunities. Diabetes Res. Clin. Pract. 2012, 98, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Perreault, L.; Kahn, S.E.; Christophi, C.A.; Knowler, W.C.; Hamman, R.F. Regression from pre-diabetes to normal glucose regulation in the diabetes prevention program. Diabetes Care 2009, 32, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.R.; Li, G.W.; Hu, Y.H.; Wang, J.X.; Yang, W.Y.; An, Z.X.; Hu, Z.X.; Lin, J.; Xiao, J.Z.; Cao, H.B.; et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T.; Hamalainen, H.; Ilanne-Parikka, P.; Keinanen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.D.; Vijay, V. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, J.L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M. Acarbose for prevention of type 2 diabetes mellitus: The STOP-NIDDM randomised trial. Lancet 2002, 359, 2072–2077. [Google Scholar] [CrossRef] [PubMed]
- Baan, C.A.; Ruige, J.B.; Stolk, R.P.; Witteman, J.C.; Dekker, J.M.; Heine, R.J.; Feskens, E.J. Performance of a predictive model to identify undiagnosed diabetes in a health care setting. Diabetes Care 1999, 22, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.J.; Little, P.S.; Hales, C.N.; Kinmonth, A.L.; Wareham, N.J. Diabetes risk score: Towards earlier detection of type 2 diabetes in general practice. Diabetes Metab. Res. Rev. 2000, 16, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J.; Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Glumer, C.; Carstensen, B.; Sandbaek, A.; Lauritzen, T.; Jorgensen, T.; Borch-Johnsen, K. A Danish diabetes risk score for targeted screening: The Inter99 study. Diabetes Care 2004, 27, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Aekplakorn, W.; Bunnag, P.; Woodward, M.; Sritara, P.; Cheepudomwit, S.; Yamwong, S.; Yipintsoi, T.; Rajatanavin, R. A risk score for predicting incident diabetes in the Thai population. Diabetes Care 2006, 29, 1872–1877. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Hoffmann, K.; Boeing, H.; Linseisen, J.; Rohrmann, S.; Mohlig, M.; Pfeiffer, A.F.; Spranger, J.; Thamer, C.; Haring, H.U.; et al. An accurate risk score based on anthropometric, dietary, and lifestyle factors to predict the development of type 2 diabetes. Diabetes Care 2007, 30, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.; Cai, T.; Hsu, H.; Su, T.; Chang, W.; Chen, M.; Lee, Y.; Hu, F.B. A prediction model for type 2 diabetes risk among Chinese people. Diabetologia 2009, 52, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.; So, W.; Tong, P.; Ma, R.; Kong, A.; Ozaki, R.; Chow, C.; Cockram, C.; Chan, J. A simple risk score to identify Southern Chinese at high risk for diabetes. Diabet. Med. 2010, 27, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.G.; Dong, Y.H.; Pang, Z.C.; Nan, H.R.; Wang, S.J.; Ren, J.; Zhang, L.; Tuomilehto, J.; Qiao, Q. A simple Chinese risk score for undiagnosed diabetes. Diabet. Med. 2010, 27, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Snehalatha, C.; Vijay, V.; Wareham, N.J.; Colagiuri, S. Derivation and validation of diabetes risk score for urban Asian Indians. Diabetes Res. Clin. Pract. 2005, 70, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, M.; de Berardis, G.; Rossi, M.C.; Sacco, M.; Belfiglio, M.; Pellegrini, F.; Tognoni, G.; Valentini, M.; Nicolucci, A. Use of the diabetes risk score for opportunistic screening of undiagnosed diabetes and impaired glucose tolerance: The IGLOO (impaired glucose tolerance and long-term outcomes observational) study. Diabetes Care 2005, 28, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Hypponen, E.; Power, C. Type 2 diabetes mellitus in midlife estimated from the Cambridge Risk Score and body mass index. Arch. Intern. Med. 2006, 166, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.; Edwards, A.M.; Bomback, A.S.; Ballantyne, C.M.; Brillon, D.; Callahan, M.A.; Teutsch, S.M.; Mushlin, A.I.; Kern, L.M. Development and validation of a patient self-assessment score for diabetes risk. Ann. Intern. Med. 2009, 151, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Qiu, Q.; Tan, L.L.; Liu, T.; Deng, X.Q.; Chen, Y.M.; Chen, W.; Yu, X.Q.; Hu, B.J.; Chen, W.Q. Prevalence and determinants of diabetes and impaired fasting glucose among urban community-dwelling adults in Guangzhou, China. Diabetes Metab. 2009, 35, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, Q.; Wang, H.; Chen, W.; Johnson, R.J.; Dong, X.; Li, H.; Ba, S.; Tan, J.; Luo, N.; et al. Prevalence and risk factors of chronic kidney disease: A population study in the Tibetan population. Nephrol. Dial. Transplant. 2011, 26, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.J.; Mainous, A.R.; Everett, C.J.; Carter, R.E. Tool to assess likelihood of fasting glucose impairment (TAG-IT). Ann. Fam. Med. 2008, 6, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.B.; Zeng, W.; Ouyang, L.Y.; Liu, Y.; Luan, R.S.; Zhang, T.J.; Xu, J.B.; Zhao, S.Q.; Li, X.J.; Huang, B.; et al. Development of evaluation tool for the risk level of abnormal glucose metabolism morbidity in middle-aged and elder populations. Zhonghua Yi Xue Za Zhi 2010, 90, 839–843. (In Chinese) [Google Scholar] [PubMed]
- Yu, J.; Zhou, J.; Li, Y. The Screening Model Construction and its validity evaluation for population with impaired glucose Regulation in community. Chin. J. Prev. Contr. Chron. Dis. 2009, 17, 139–141. [Google Scholar]
- Cooperative Meta-analysis Group of China Obesity Task Force. Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Chin. J. Epidemiol. 2002, 23, 5–10. [Google Scholar]
- International Diabetes Foundation. IDF Consensus Worldwide Definition of the Metabolic Syndrome. Available online: http://www.idf.org/webdata/docs/IDF_Meta_def_final.pdf (accessed on 21 January 2015).
- Chalmers, J.; MacMahon, S.; Mancia, G.; Whitworth, J.; Beilin, L.; Hansson, L.; Neal, B.; Rodgers, A.; Ni Mhurchu, C.; Clark, T. 1999 World Organization-international society of hypertension guidelines for the management of hypertension. J. Hypertens. 1999, 17, 151–183. [Google Scholar] [PubMed]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.J.; Taub, N.A.; Khunti, K.; Gardiner, E.; Hiles, S.; Webb, D.R.; Srinivasan, B.T.; Davies, M.J. The Leicester Risk Assessment score for detecting undiagnosed type 2 diabetes and impaired glucose regulation for use in a multiethnic UK setting. Diabet. Med. 2010, 27, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Heikes, K.E.; Eddy, D.M.; Arondekar, B.; Schlessinger, L. Diabetes risk calculator: A simple tool for detecting undiagnosed diabetes and pre-diabetes. Diabetes Care 2008, 31, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Xin, Z.; Yuan, J.; Hua, L.; Ma, Y.H.; Zhao, L.; Lu, Y.; Yang, J.K. A simple tool detected diabetes and prediabetes in rural Chinese. J. Clin. Epidemiol. 2010, 63, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Glumer, C.; Vistisen, D.; Borch-Johnsen, K.; Colagiuri, S. Risk scores for type 2 diabetes can be applied in some populations but not all. Diabetes Care 2006, 29, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Glumer, C.; Borch-Johnsen, K.; Colagiuri, S. Can a screening programme for diabetes be applied to another population? Diabet. Med. 2005, 22, 1234–1238. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Engelgau, M.M.; Valdez, R.; Benjamin, S.M.; Cadwell, B.; Narayan, K.M. Costs of screening for pre-diabetes among US adults: A comparison of different screening strategies. Diabetes Care 2003, 26, 2536–2542. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Liu, T.; Qiu, Q.; Ding, P.; He, Y.-H.; Chen, W.-Q. A Simple Risk Score for Identifying Individuals with Impaired Fasting Glucose in the Southern Chinese Population. Int. J. Environ. Res. Public Health 2015, 12, 1237-1252. https://doi.org/10.3390/ijerph120201237
Wang H, Liu T, Qiu Q, Ding P, He Y-H, Chen W-Q. A Simple Risk Score for Identifying Individuals with Impaired Fasting Glucose in the Southern Chinese Population. International Journal of Environmental Research and Public Health. 2015; 12(2):1237-1252. https://doi.org/10.3390/ijerph120201237
Chicago/Turabian StyleWang, Hui, Tao Liu, Quan Qiu, Peng Ding, Yan-Hui He, and Wei-Qing Chen. 2015. "A Simple Risk Score for Identifying Individuals with Impaired Fasting Glucose in the Southern Chinese Population" International Journal of Environmental Research and Public Health 12, no. 2: 1237-1252. https://doi.org/10.3390/ijerph120201237
APA StyleWang, H., Liu, T., Qiu, Q., Ding, P., He, Y.-H., & Chen, W.-Q. (2015). A Simple Risk Score for Identifying Individuals with Impaired Fasting Glucose in the Southern Chinese Population. International Journal of Environmental Research and Public Health, 12(2), 1237-1252. https://doi.org/10.3390/ijerph120201237