1. Introduction
Organ transplant systems are in need of fundamental changes if they are to provide increasing levels of service delivery under more demanding circumstances and severe budget constraints. Current organ transplant structures do not make the best use of their resources resulting in suboptimal care processes and resource overuse [
1,
2].
In response to the challenge of how to best optimize the resource utilization in organ transplant processes, there is an increasing interest, according to published literature, in the analysis of productivity and efficiency achieved in health care systems [
3,
4].
With regards to this challenge two are the main purposes of this paper: (1) to provide formal methods to conduct quantitative appraisal of the performance observed in health care delivery systems and (2) to further investigate the effect of systems processes and internal structures on this performance.
The organ donation process constitutes an interesting case of study in a triangulation approach as it entails a very delicate and complex set of processes involving several highly specialized experts working in disparate organizations with rather different structures and resources. It demands lots of resources that must be efficiently managed.
With regards to the existing limitations observed in parametric models, this paper develops an approach to compute technical efficiency providing enough flexibility in the model structure to allow for: (1) multi-output analysis of technical efficiency as well as (2) the modeling of complex data structures present in longitudinal observations or hierarchical business units in health care.
With regards to the second purpose of the paper, understand the impact of internal processes within health care units in the observed performance, a qualitative research study was conducted whereby each service unit was characterized based on the Baldrige criteria.
The rest of the paper is structured as follows:
Section 2 provides a formal method to conduct quantitative analysis of technical efficiency in a set of organ donation and transplant service units.
Section 3 characterizes organizational routines and processes within those service units.
Section 4 builds upon previous sections to build causal models explaining the relationship between organizational routines and observed performance and
Section 5 offers the paper’s conclusions.
The present analysis can help to promote organizational characteristics that offer the best decision making in the organ transplant process and therefore to optimize the resource utilization in organ transplant processes.
2. Theory Development
Organ transplant systems are adaptive because, unlike mechanical systems, they are composed of individuals—patients and clinicians—who have the capacity to learn and change as a result of experience. Their actions in delivering organs are not always predictable, and tend to change both their local and larger environments. The unpredictability of behavior in complex adaptive systems can be seen as contributing to huge variation in the delivery of health care [
5].
This calls for systemic approaches in which health care services follow a Service-Dominant (S-D) logic [
6,
7]. Organ donation, an instance of this type of healthcare servicing, fits in the foundational premises for S-D logic as suggested in Vargo and Akaka [
8] in the sense that organ donation is a service in which some competences, donation capabilities, are applied for the benefit of others. There exists an indirect service exchange between provider and adopter mediated by hospitals and physicians. Operant resources, such as surgeons, are key to the service in contrast to operand resources which play a secondary role in determining effectiveness [
9].
Value is always co-created in organ donation processes by several parties engaged in close collaboration, each of them offering a specific core competence [
10]. There is no single entity fully responsible for value delivery. Customers, in this case experts at the receiving hospital, play an active role by deciding under which conditions a donation is to be performed according to medical characteristics. In most cases, they even travel to the donating hospital to harvest organs by themselves.
In the following discussions the organ donation service will be described in terms of two basic constructs in S-D logic: service systems and service interactions occurring between them. It is increasingly evident that patient outcomes are not solely a function of efficacious clinical interventions and practices. Delivery-system research may be viewed as the systematic study of healthcare organizations, including interchanges with their external environments (e.g., markets, regulators, competitors) and interactions among internal components (e.g., employees, technology, work processes, culture), that affect how care is organized and provided [
1].
The difficulty in the design of the organ transplant process where many different specialists take part has much to do with the way the transfer of knowledge is provided [
11,
12] and in structures where the tacit component is high [
13,
14,
15] in contexts where there is a clear description of the structures and results [
16]. Besides, for the structure designs to be efficient, they must be able to adapt to new scenarios and dynamics [
17]. This way they will be aligned with the evolution of scientific and technological possibilities by maintaining optimal response time standards.
Besides, the need to maintain and generate dynamic capabilities in system processes together with the need to manage tacit knowledge, difficult to turn explicit, makes necessary the use of coordination mechanisms that exceed excellent organizational routines and that warranty the proper climate to promote interdependent and multidisciplinary processes [
18].
Drucker [
19] considers that one of the main elements to incentivize productivity and performance in structures is the association of people that work together for similar purposes. Pisano [
20] suggests that although there are no universal formulas to favor the transfer of knowledge and learning, the existent ones depend each time more on the organizational structures. A group of authors [
21,
22,
23] suggests that the link between incremental uncertainty and more informal coordination models drives to the achievement of higher performance in system processes.
Technical efficiency represents the ability of the observed health care unit to maximize the results of the service delivery subject to some resources and constraints, or conversely the ability to maintain the service delivery with lower levels of resource consumption.
Seminal papers on the measurement of technical efficiency like [
24] and [
25] stated the importance of productive efficiency for policy and economic planning purposes. Twenty years later [
26] introduced Data Envelopment Analysis (DEA), a methodology able to assess the relative efficiency of multi-input multi-output production units.
At its most basic form DEA computes technical efficiency scores as descriptive measures of the relative technical efficiency of observed decision making units in comparison to a best-practice production frontier. Being of a non-parametric nature DEA does not impose any functional form on the production model, arguably a key aspect for its widespread application in a variety of contexts from banking [
27,
28,
29], production planning [
30], R&D performance [
31,
32] and agricultural economics [
33] among others [
34].
In some circumstances it might be of interest to ask whether observed firms can improve their importance and if so, by how much. According to [
35], such questions can only be answered by inference which in order to be meaningful requires coherent, well-defined statistical models.
The majority of the results presented in the reviewed literature adopting parametric models to conduct efficiency analysis adopt however model structures which are too simplistic, e.g., conventional ordinary least square regression models, to characterize the rich variety present in health care deliveries [
36,
37,
38,
39,
40,
41,
42]. Moreover, conventional parametric models do not allow for multi-output response analysis, arguably an important limitation in the analysis of complex, multidimensional services.
With regards to the existing limitations observed in parametric models, this paper follows a parametric multilevel modeling approach to compute the technical efficiency achieved by the service delivery systems under study.
For example, hierarchical linear models (HLMs) offer a powerful approach to conduct longitudinal analyses across three or more levels [
39]. These models are also commonly known by other names, such as mixed-effects regression models and multilevel models [
37,
42]. They are able to recognize the hierarchical structures present in complex service delivery systems.
The Baldrige quality criteria have been applied to stimulate actions for total quality management at firms and analyze the results [
43,
44,
45]. In 1998 the criteria were extended in the United States to health services [
46].
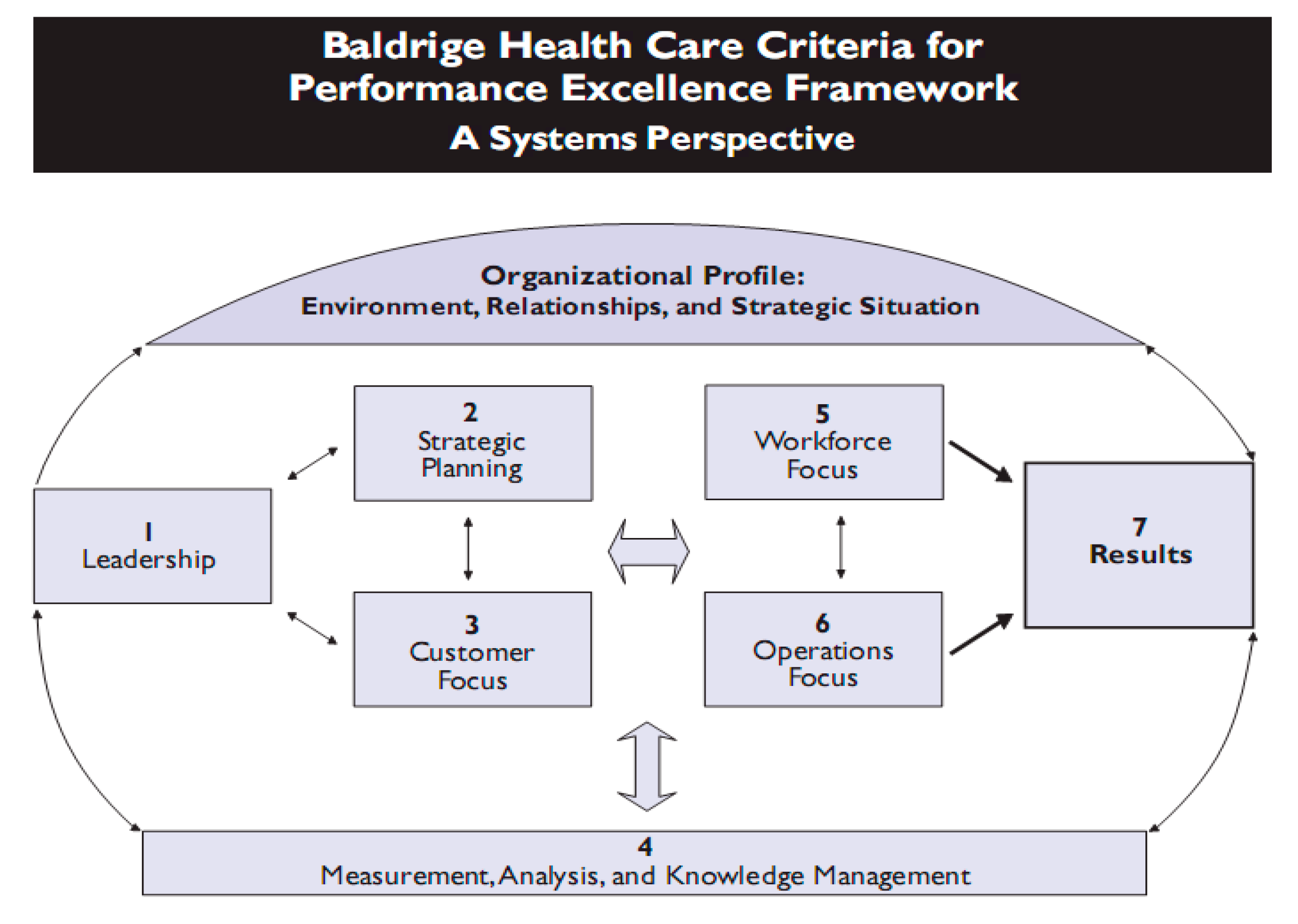
The framework for Baldrige criteria for excellence in performance presents a managerial model based on the quality [
43] and the orientation to an effective performance to improve processes [
47]. The model is organized in seven interrelated components: (1) leadership, (2) focus on customers and the rest of interest groups, (3) strategic planning (4) the management of human resources (5) the management of the information and data analysis, (6) the management of processes (7) and the management of results for final performance. Many health institutions today are using Baldridge’s criteria as a tool to self-evaluate the effects of the quality practices in their organizations [
48].
Figure 1 offers a conceptualization of the Baldrige criteria. To achieve quality in the delivery of healthcare services the following are needed:
According to the previous literature review, the following hypotheses are proposed:
H1
To reach best results, processes must be oriented to the achievement of objectives
H2
More efficient organizations in terms of coordination reach best results
H3
High levels of organizational routines and processes positively moderate the resulting technical efficiency.
Figure 1.
The Baldrige model.
Figure 1.
The Baldrige model.
5. Discussion, Conclusions and Future Areas of Research
Two have been the main purposes of this paper: (1) provide formal methods to conduct quantitative analysis of technical efficiency in organ transplant and (2) further investigate the impact of internal processes within organ transplant units in the observed performance.
Organ transplant systems present two important characteristics: interdependence and capacity of adaptation. Both characteristics make the management and evaluation of these systems complex. The present work has taken as an example of this complex healthcare system the donation and transplant system in a region of Spain.
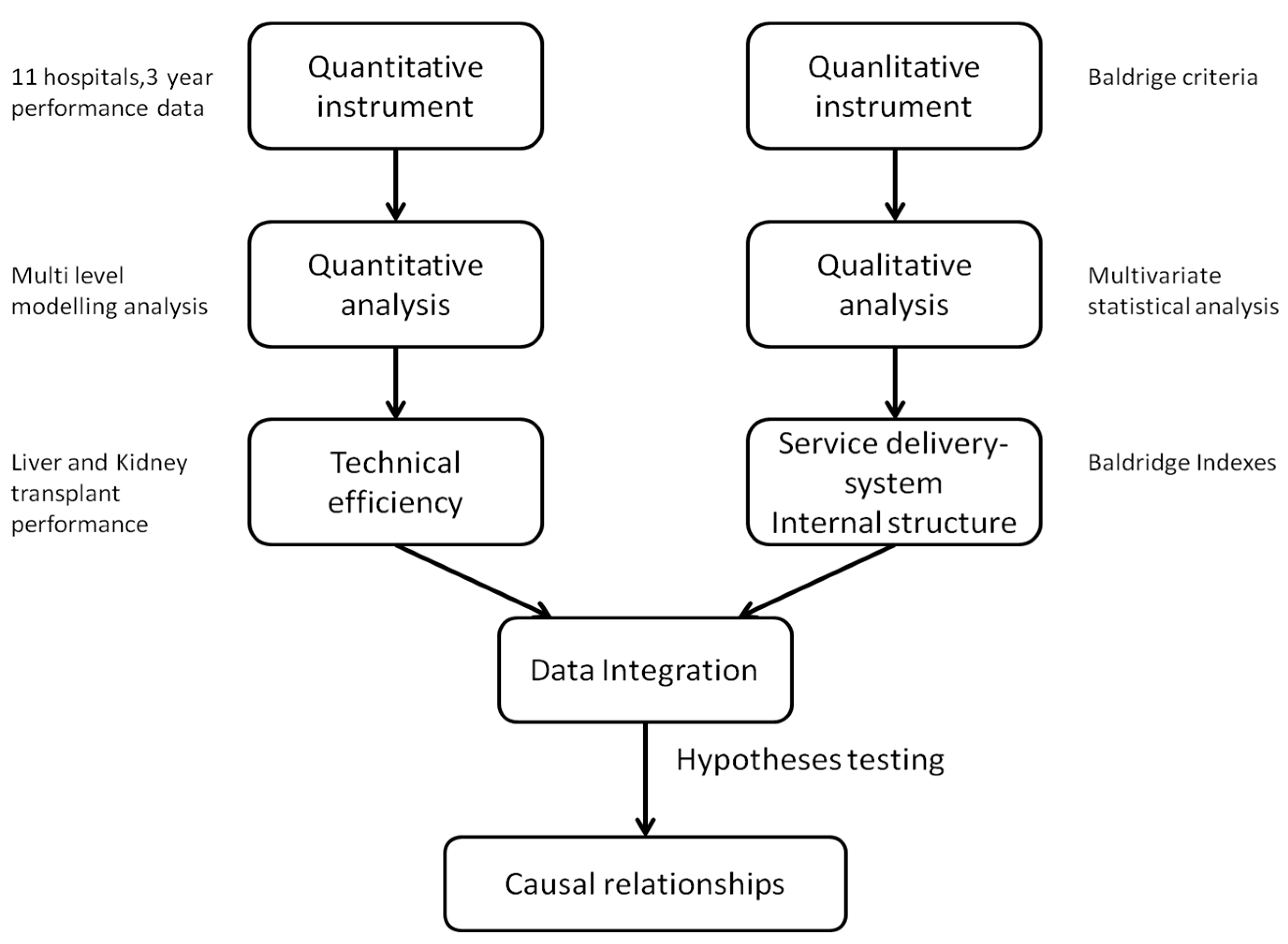
This paper adopts a mixed method research since it combines in the research process elements of qualitative and quantitative research in order to achieve breadth and depth of understanding and validation. By considering the barriers observed in parametric models, this paper follows a parametric multilevel modeling approach to calculate the technical efficiency reached in donation and transplant healthcare service delivery system.
An initial quantitative exploration based in the technical efficiency concept is followed by several qualitative analyses aimed at explaining in more depth the mechanisms underlying the phenomena under observation. For this second part, concepts coming from the relational coordination framework and the Baldrige quality model have been applied. From the reviewed literature and the results obtained in the present work it is possible to argue that the excellence in the offering of services in donation and transplant requires: (1) excellence in the management of operational processes and (2) putting into action relational coordination mechanisms amongst the systems involved.
In relation to both components, the operational and relational one, to achieve excellence in healthcare delivery systems, it is possible to implement in practice mechanisms for the measurement of both components by making use of mixed methods, including both quantitative and qualitative tools. This way, the operational component is estimated by making use of the technical efficiency and the relational one by making use of the Baldrige indexes.
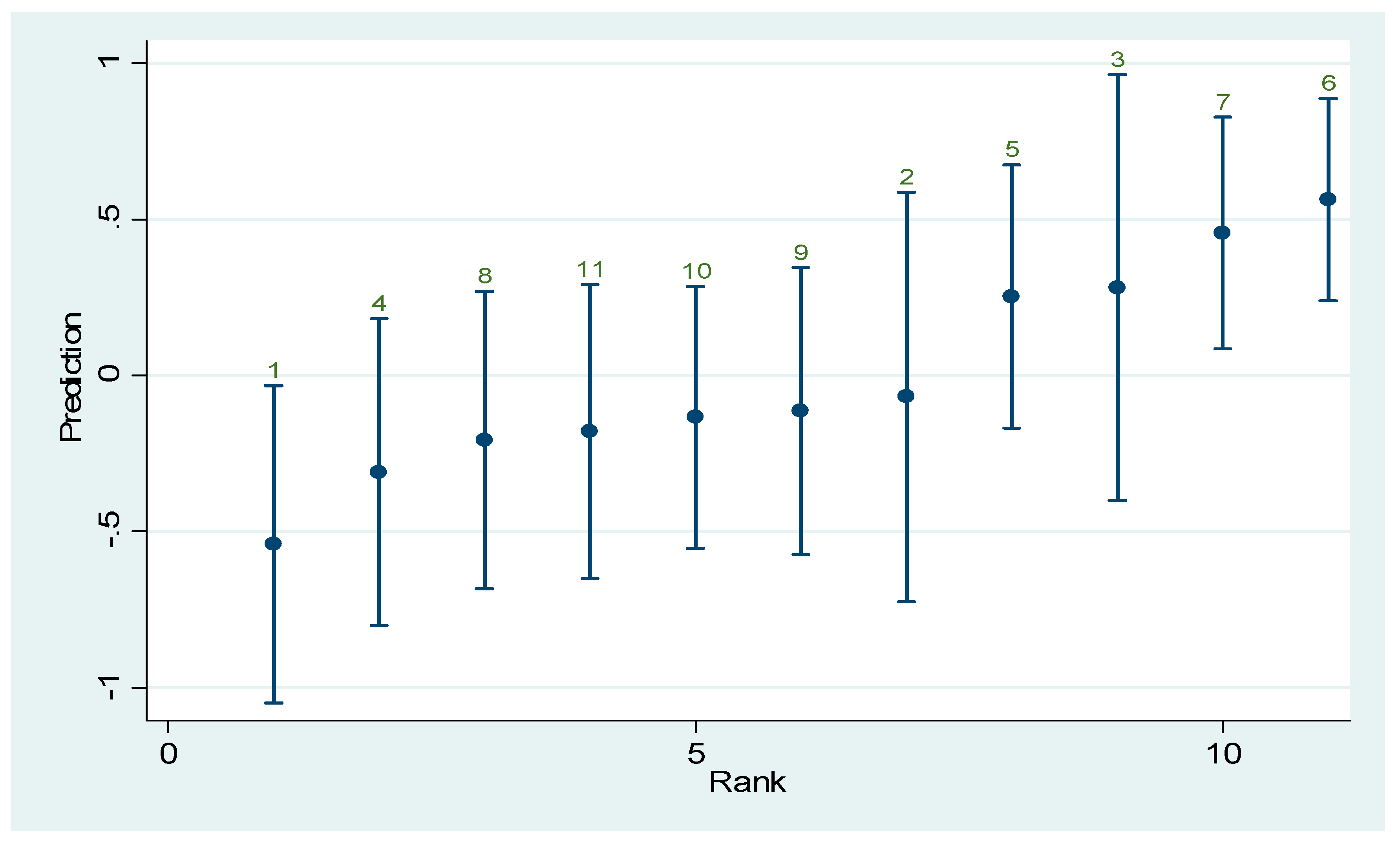
An important conclusion from this work is the existent relation prooved between the levels related to the Baldrige indexes and the technical efficiency observed in the donor and transplant units in the 11 analyzed hospitals in this study. This way it is possible to conclude how high levels in the Baldrige indicators become a necessary condition to get a high level in the service delivery.
As future areas of research we could consider to widen the simple to other health regions to analyze dependencies to a regional level and identify quantitative relationships amongst Baldrige indicators and the observed technical efficiency in other kind of transplants. Having more data could enable the development of detailed analysis about the importance of each Baldrige construct.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


