
The Effect of Engagement in Everyday Occupations, Role Overload and Social Support on Health and Life Satisfaction among Mothers


Abstract
:1. Introduction

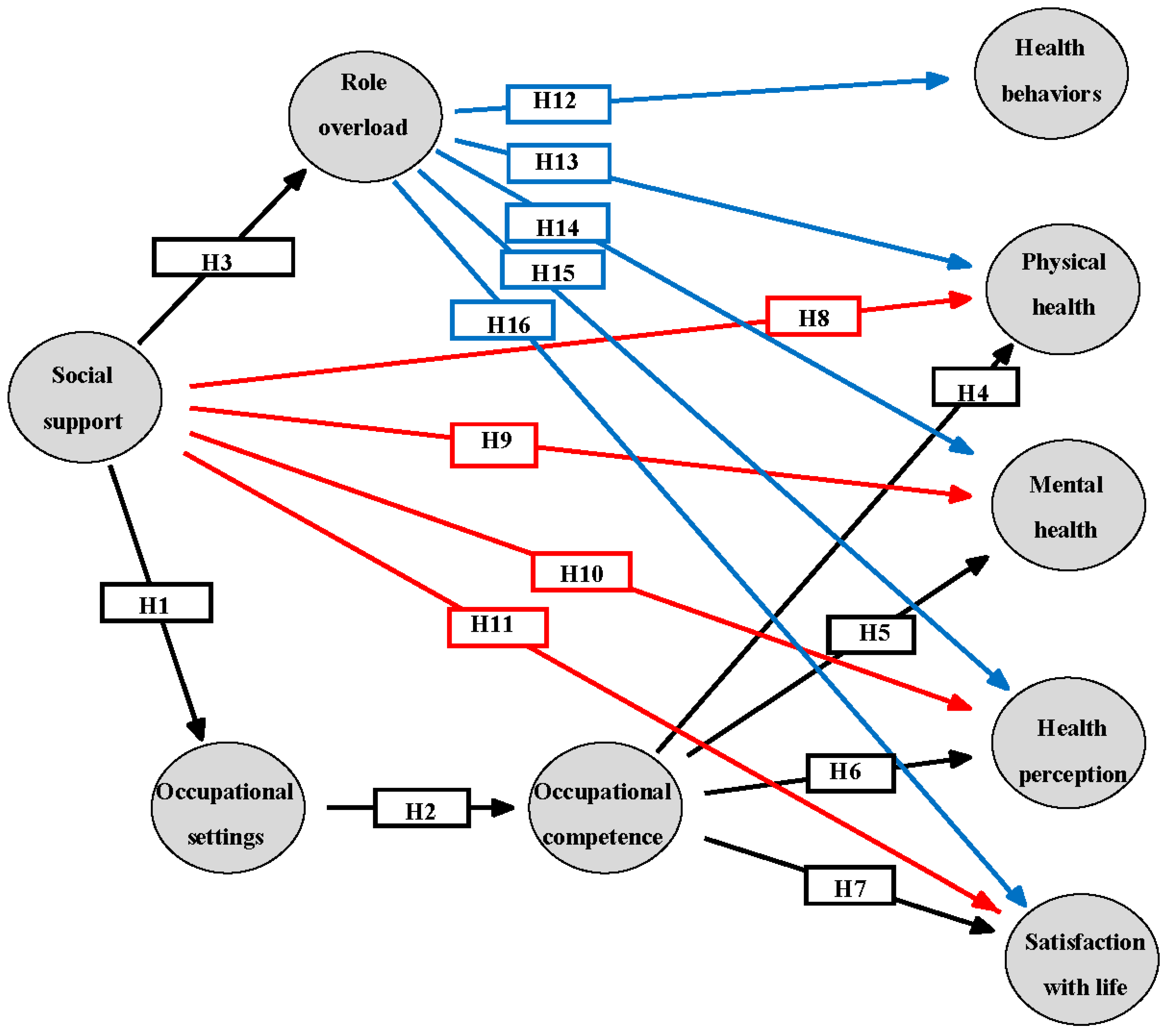
1.1. Occupational Performance (See Figure 1, Hypotheses 1 and 2)
1.2. Occupational Performance, Role Load, Health, and Life Satisfaction (See Figure 1, Hypotheses 3−7 and 12−16)
1.3. Mothers’ Occupations, Role Load, and Health (See Figure 1, Hypotheses 12−16)
1.4. Mothers’ Social Support and Health (See Figure 1, Hypotheses 8−11)
1.5. Mothers’ Socio-Demographic Factors and Health
2. Materials and Methods
2.1. The Study Group
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Sample Characteristics

{kind=link}
{kind=link}
| Variable Name | Levels | Frequency | Percentage |
|---|---|---|---|
| No. of children | 1 | 41 | 27.3 |
| 2 | 67 | 44.7 | |
| 3 | 35 | 23.3 | |
| 4 | 7 | 4.7 | |
| Education | High school | 24 | 16 |
| Bachelor’s degree | 59 | 39.3 | |
| Two Bachelor’s degrees | 6 | 4 | |
| MA | 30 | 20 | |
| PhD | 5 | 3.3 | |
| Other degrees | 26 | 17.3 |
3.2. Distribution of Study Variables
| Variable | Mean | Median | SD | Range (Min−Max) | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| 1. Social support | 27.02 | 27.00 | 4.29 | (15–36) | −0.21 | −0.31 |
| 2. Occupational settings | 67.00 | 67.00 | 11.19 | (39–91) | −0.21 | −0.48 |
| 3. Occupational competence | 69.03 | 68.00 | 10.80 | (44–100) | 0.26 | −0.34 |
| 4. Role overload | 2.35 | 2.40 | 0.41 | (1.40–3.50) | −0.12 | −0.31 |
| 5. Health behaviors | 1.69 | 2.00 | 0.70 | (0–3) | −0.31 | 0.06 |
| 6. Physical health | 76.83 | 79.00 | 14.19 | (19–99) | −1.25 | 1.94 |
| 7. Mental health | 76.07 | 78.50 | 12.93 | (37–98) | −1.14 | 1.16 |
| 8. Health perception | 84.07 | 88.00 | 14.33 | (35–100) | −1.19 | 1.11 |
| 9. Satisfaction with life | 26.93 | 28.00 | 4.70 | (10–34) | −1.17 | 1.59 |
| 10. Mother’s age | 34.25 | 33.00 | 4.78 | (25–45) | 0.32 | −0.52 |
| 11. Education | 15.71 | 16.00 | 2.23 | (12–23) | 0.03 | 0.07 |
| 12. No. children | 2.05 | 2.00 | 0.83 | (1–4) | 0.39 | −0.47 |
| 13. Average children’s age | 5.00 | 3.71 | 3.66 | (1–15.75) | 1.04 | 0.10 |
| 14. Hours at work | 34.89 | 35.00 | 9.82 | (12–62) | −0.02 | −0.06 |
3.3. Correlations between Research Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Social support | (0.63) | 0.24 | 0.29 | 0.39 | 0.10 | 0.21 | 0.14 | 0.11 | 0.50 | 0.03 | 0.16 | 0.16 | 0.06 | 0.05 |
| 2. Occupational settings | 0.17 * | (0.80) | 0.85 | 0.10 | 0.21 | 0.25 | 0.42 | 0.04 | 0.42 | 0.30 | 0.04 | 0.36 | 0.38 | −0.06 |
| 3. Occupational competence | 0.21 * | 0.69 *** | (0.82) | 0.07 | 0.21 | 0.08 | 0.20 | 0.04 | 0.43 | 0.23 | 0.20 | 0.33 | 0.29 | −0.03 |
| 4. Role overload | 0.31 *** | 0.09 | 0.06 | ----- | 0.13 | 0.18 | 0.05 | 0.17 | 0.18 | −0.13 | 0.12 | −0.09 | −0.10 | 0.14 |
| 5. Health behaviors | 0.08 | 0.19 * | 0.19 * | 0.13 | ----- | 0.24 | 0.13 | 0.15 | 0.17 | −0.10 | 0.06 | 0.02 | 0.02 | 0.13 |
| 6. Physical health | 0.14 | 0.19 * | 0.06 | 0.15 | 0.20 * | (0.70) | 0.77 | 0.66 | 0.34 | 0.06 | −0.13 | 0.14 | 0.14 | 0.07 |
| 7. Mental health | 0.09 | 0.31 *** | 0.15 | 0.04 | 0.11 | 0.53 *** | (0.67) | 0.54 | 0.69 | 0.09 | −0.16 | 0.15 | 0.12 | −0.22 |
| 8. Health perception | 0.09 | 0.04 | 0.04 | 0.17 * | 0.15 | 0.55 *** | 0.44 *** | ----- | 0.25 | −0.19 | −0.05 | −0.03 | −0.10 | 0.07 |
| 9. Satisfaction with life | 0.36 *** | 0.34 *** | 0.35 *** | 0.16 | 0.15 | 0.26 *** | 0.51 *** | 0.23 ** | (0.82) | 0 | 0.08 | 0.13 | 0.06 | −0.12 |
| 10. Mother’s age | 0.02 | 0.27 *** | 0.21 * | −0.13 | −0.10 | 0.05 | 0.07 | −0.19 * | 0 | ----- | 0.13 | 0.54 | 0.77 | −0.07 |
| 11. Education | 0.13 | 0.04 | 0.18 * | 0.12 | 0.06 | −0.11 | −0.13 | −0.05 | 0.07 | 0.13 | ----- | −0.08 | 0.01 | 0.03 |
| 12. No. children | 0.13 | 0.32 *** | 0.30 *** | −0.09 | 0.02 | 0.12 | 0.12 | −0.03 | 0.12 | 0.54 *** | −0.08 | ----- | 0.63 | −0.07 |
| 13. Children age average | 0.05 | 0.34 *** | 0.26 ** | −0.10 | 0.02 | 0.12 | 0.10 | −0.10 | 0.05 | 0.77 *** | 0.01 | 0.63 *** | ----- | −0.08 |
| 14. Hours at work | 0.04 | −0.05 | −0.03 | 0.14 | 0.13 | 0.06 | −0.18 * | 0.07 | −0.11 | −0.07 | 0.03 | −0.07 | −0.08 | ----- |
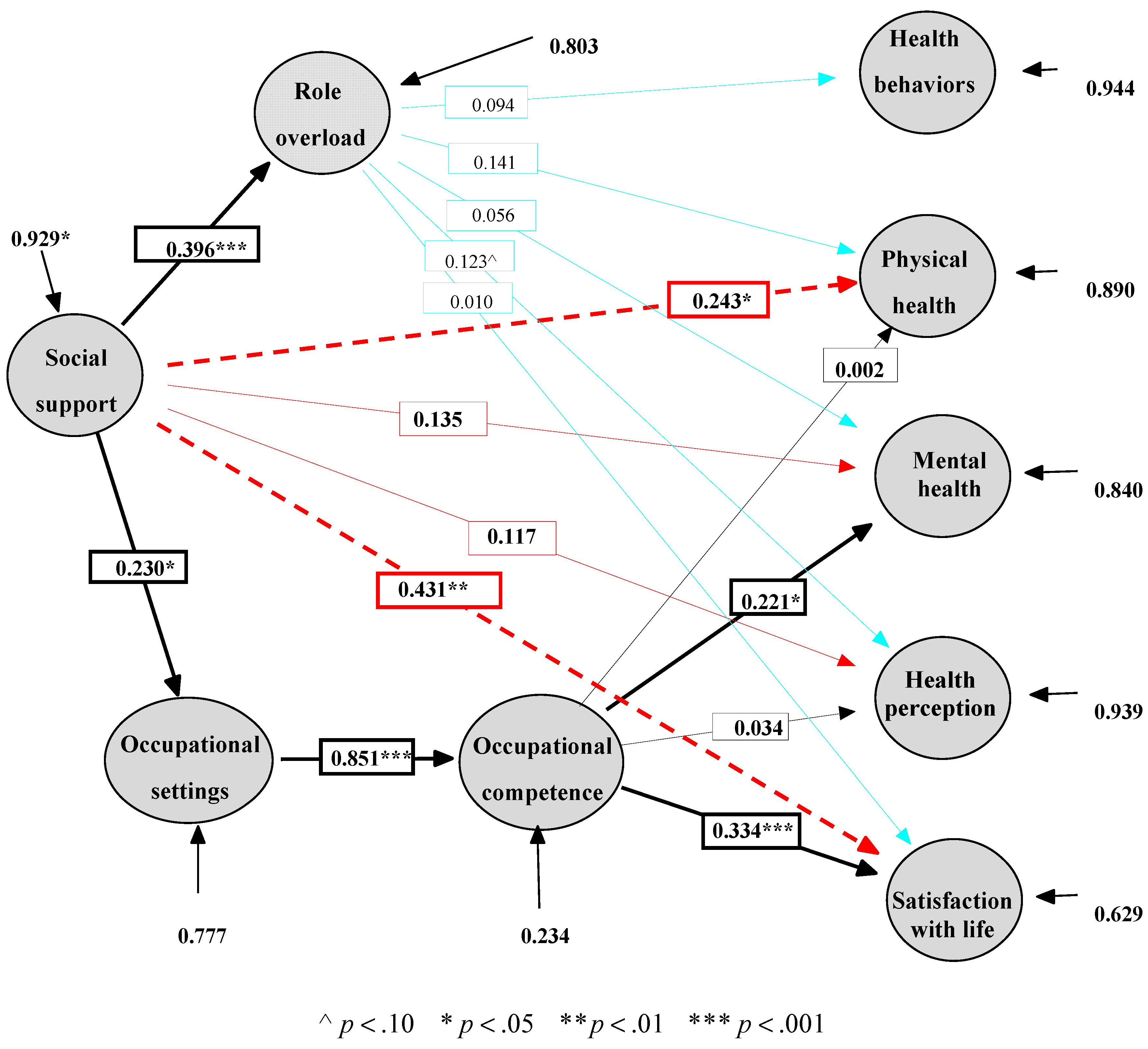
3.4. Testing of the Theoretical Models
| Model | s-b χ2 | df | GFI | SRMSR | CFI a | NFI a | AGFI | PNFI b |
|---|---|---|---|---|---|---|---|---|
| Model I: Occupational competence effects on health and life satisfaction | 39.63 ** | 19 | 0.964 | 0.051 | 0.909 | 0.881 | 0.801 | 0.159 |
| Model II: Model I + the direct effects of social support | 20.84 | 15 | 0.980 | 0.035 | 0.974 | 0.937 | 0.862 | 0.134 |
| Model III: Model II + the effects of role overload | 17.21 | 10 | 0.984 | 0.030 | 0.968 | 0.948 | 0.828 | 0.090 |

4. Discussion
4.1. The Effect of Occupational Settings and Occupational Competence on Health and Life Satisfaction
4.2. The Effect of Social Support on Health and Life Satisfaction
4.3. The Effect of Role Overload on Health and Life Satisfaction
4.4. Limitations and Recommendations for Future Studies
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hocking, C. Contribution of occupation to health and well-being. In Willard & Spackman’s Occupational Therapy, 11th ed.; Crepeau, E.B., Cohn, E.S., Schell, B.A.B., Eds.; Wolters Kluwer/Lippincott: Philadelphia, PA, USA, 2009; Chapter 5; pp. 45–54. [Google Scholar]
- Townsend, E.A.; Polatajko, H. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-Being, and Justice through Occupation, 2nd ed.; CAOT Publications ACE: Ottawa, ON, Canada, 2013. [Google Scholar]
- Law, M.; Steinwender, S.; Leclair, L. Occupation, health and well-being. Can. J. Occup. Ther. 1998, 65, 81–91. [Google Scholar] [CrossRef]
- Law, M.; Cooper, B.; Strong, S.; Stewart, D.; Rigby, P.; Letts, L. Person-environment-occupation model: A transactive approach to occupational performance. Can. J. Occup. Ther. 1996, 63, 9–23. [Google Scholar] [CrossRef]
- Kielhofner, G.; Mallinson, T.; Crawford, C.; Nowak, M.; Rigby, M.; Henry, A.; Walens, D. A User’s Manual for the Occupational Performance History Interview— Version 2.1 OPHI-II; University of Illinois at Chicago: Chicago, IL, USA, 2004. [Google Scholar]
- Kielhofner, G. Model of Human Occupation: Theory and Application, 4th ed.; Lippincott, Williams and Wilkins: Baltimore, MD, USA, 2008. [Google Scholar]
- Baum, M.C.; Christiansen, C.H. Person-environment-occupation-performance: An occupation-based framework for practice. In Occupational Therapy: Performance, Participation, and Well-Being, 3rd ed.; Christiansen, C.H., Baum, M.C., Haugen, B., Eds.; Slack: Thorofare, NJ, USA, 2005; Chapter 11. [Google Scholar]
- Coverman, S. Role overload, role conflict, and stress: Addressing the consequences of multiple role demands. Soc. Forces 1989, 67, 965–982. [Google Scholar] [CrossRef]
- Booth, A.; Johnson, D.R.; Granger, D.A. Testosterone, marital quality, and role overload. J. Marriage Fam. 2005, 67, 483–498. [Google Scholar] [CrossRef]
- Goldberg, W.A.; Greenberger, E.; Hamill, S.; O’Neil, R. Role demands in the lives of employed single mothers with preschoolers. J. Fam. Issues 1992, 13, 312–333. [Google Scholar] [CrossRef]
- Glynn, K.; Maclean, H.; Forte, T.; Cohen, M. The Association between role overload and women’s mental health. J. Womens Health 2009, 18, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Kane, P. Women and Occupational Health, World Health Organization, Geneva, Switzerland. Available online: http://apps.who.int/iris/handle/10665/65855?mode=full&submit_simple=Show+full+item+record (accessed on 6 June 2014).
- U.S. Census Bureau. Fertility of American Women: 2010—Detailed Tables; U.S. Census Bureau: Suitland, MD, USA, 2010. Available online: http://www.census.gov/hhes/fertility/data/cps/2010.html (accessed on 7 April 2014).
- Avrech Bar, M.; Labock-Gal, D.; Jarus, T. Occupational performance, social support and life satisfaction in single mothers compared with married mothers. Isr. J. Occup. Ther. 2011, 20, 195–218. [Google Scholar]
- Hunter, H.M.; Blair, S.E.E. The magic, mess and muddles of becoming a mother—An occupational perspective. Occupation 2000, 8, 7–15. [Google Scholar]
- Francis-Connolly, E. Toward understanding of mothering: A comparison of two motherhood stages. Am. J. Occup. Ther. 2000, 54, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Avrech Bar, M.; Rubin, V.; Gavrieal-Tyjchman, G.; Jarus, T. The validity and reliability of the modified version of the Role Checklist (M-RCL). Scand. J. Occup. Ther. 2013, 20, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Koniak-Griffin, D.; Logsdon, M.C.; Hines-Martin, V.; Turner, C.C. Contemporary mothering in a diverse society. JOGNN 2006, 35, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Pearson, Q.M. Role overload, job satisfaction, leisure satisfaction, and psychological health among employed women. J. Counsel. Dev. 2008, 86, 57–63. [Google Scholar] [CrossRef]
- Doumas, D.; Margolin, G.; John, R.S. The relationship between daily marital interaction, work and health-promoting behaviours in dual earner couples: An extension of the work-family spillover model. J. Fam. Issues 2003, 24, 3–20. [Google Scholar] [CrossRef]
- Stuart, G.; Garrison, M. The influence of daily hassles and role balance on health status: A study of mothers of grade school children. Women Health 2002, 36, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Leahy-Warren, P.; McCarthy, G.; Corcoran, P. First-time mothers: Social support, maternal parental self-efficacy and postnatal depression. J. Clin. Nurs. 2012, 21, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Umberson, D. Women, stress, and health. In Women and Health; Goldman, M.B., Hatch, M.C., Eds.; Academic press: San Diego, CA, USA, 2000; pp. 553–562. [Google Scholar]
- Börjesson, B.; Paperin, C.; Lindel, M. Maternal support during the first year of infancy. J. Adv. Nurs. 2004, 45, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Arborelius, E.U.; Bremberg, S.G. Supportive and nonsupportive qualities of child health nurses’ contacts with strained infant mothers. Scand. J. Caring Sci. 2003, 17, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Tardy, R.W. But I am a good mom: The social construction of motherhood through health-care conversations. J. Contemp. Ethnogr. 2000, 29, 433–473. [Google Scholar] [CrossRef]
- McDonough, P.; Walters, V.; Strohschein, L. Chronic stress and the social patterning of women’s health in Canada. Soc. Sci. Med. 2002, 54, 767–782. [Google Scholar] [CrossRef]
- Rowland Hogue, C.J. Gender, race, and class: From epidemiologic association to etiologic hypotheses. In Women and Health; Goldman, M.B., Hatch, M.C., Eds.; Academic press: San Diego, CA, USA, 2000; pp. 15–23. [Google Scholar]
- Goldman, M.B.; Hatch, M.C. An overview of women and health. In Women and Health; Goldman, M.B., Hatch, M.C., Eds.; Academic press: San Diego, CA, USA, 2000; pp. 5–14. [Google Scholar]
- Matthews, S.; Power, C. Socio-economic gradients in psychological distress: A focus on women, social roles and work-home characteristics. Soc. Sci. Med. 2002, 54, 799–810. [Google Scholar] [CrossRef]
- Sanders, M.J.; Morse, T. The ergonomics of caring for children: An exploratory study. Am. J. Occup. Ther. 2005, 59, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Kielhofner, G.; Mallinson, T.; Forsyth, K.; Lai, J.-S. Psychometric properties of the second version of the Occupational Performance History Interview (OPHI-II). Am. J. Occup. Ther. 2001, 55, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Oakley, F. The Model of Human Occupation in Psychiatry; Unpublished master’s project; Virginia Commonwealth University: Richmond, CA, USA, 1982. [Google Scholar]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-Item Short-Form health survey (SF-36): I, Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J. Am. Soc. Nephrol. 2001, 12, 2797–2806. [Google Scholar] [PubMed]
- Lewin-Epstein, N.; Sagiv-Schifter, T.; Shabtal, E.L.; Shmueli, A. Validation of the 36-item short-form health survey (Hebrew version) in the adult population of Israel. Med. Care 1998, 36, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Paul-Dauphin, A.; Guillemin, F.; Virion, J.M.; Briancon, S. Bias and precision in visual analogue scales: A randomized controlled trial. Am. J. Epidemiol. 1999, 150, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-rated health status as a health measure: The predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E. Review of the satisfaction with life scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Anaby, D.; Jarus, T.; Zumbo, D.B. Psychometric evaluation of the Hebrew language version of the satisfaction with life scale. Soc. Indic. Res. 2010, 96, 267–274. [Google Scholar] [CrossRef]
- Vassar, M. A note on the score reliability for the satisfaction with life scale: An RG study. Soc. Indic. Res. 2008, 86, 47–57. [Google Scholar] [CrossRef]
- Pascoe, J.M.; French, J. The reliability and validity of the Maternal Social Support Index for primiparous mothers: A brief report. Fam. Med. 1990, 22, 228–230. [Google Scholar] [PubMed]
- McCurdy, K. Can home visitation enhance maternal social support? Am. J. Community Psychol. 2001, 29, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Froom, P.; Melamed, S.; Triber, I.; Ratson, N.Z.; Hermoni, D. Predicting self-reported health: The CORDIS study. Prev. Med. 2004, 39, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control. Mabat Survey of Health Condition and Nutrition; The Gertner Institue: Tel Hashomer, Israel, 2003. (In Hebrew) [Google Scholar]
- Ashkenazi, Y.; Gross, R. Health Condition of Women in Israel: Review of Data Women’s Health in Israel; Myers-JDC-Brookdale Institute: Jerusalem, Israel, 2004. (In Hebrew) [Google Scholar]
- Mi-Ami, N. A Background Document on Addiction to Smoking Cigarettes; The Knesset—Research and information center: Jerusalem, Israel. Available online: http://www.knesset.gov.il/mmm/doc.asp?doc= m00594&type=doc (accessed on 5 December 2011).
- Husten, C.G.; Malarcher, A.M. Cigarette smoking: Trends, determinants, and health effects. In Women and Health; Goldman, M.B., Hatch, M.C., Eds.; Academic press: San Diego, CA, USA, 2000; pp. 563–577. [Google Scholar]
- Brezis, M. Position Paper and Recommendations on Promoting Physical Activity in Israel. National Council for Health Promotion. Available online: http://www.hadassah.org.il/media/1920578/______________________________.pdf (accessed on 15 April 2012).
- Dion, P.A. Interpreting Structural Equation Modeling results: A reply to Martin and Cullen. J. Bus. Ethics 2008, 83, 365–368. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Bentler, P.M. EQS: Structural Equation Program Manual; Multivariate Software Inc.: Encino, CA, USA, 1995. [Google Scholar]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Boomsma, A. Reporting analyses of covariance structures. Struct. Equ. Model. 2000, 7, 461–483. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis with Readings, 6th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Central Bureau of Statistics. Living Area Clusters by Socio-Economic Level of the Population. Available online: http://www.cbs.gov.il/mifkad/hesber/mavo13.doc (accessed on 5 September 2012).
- Bedian, A.G.; Day, D.V.; Kelloway, K.E. Correcting for measurement error attenuation in structural equation models: Some important reminders. Educ. Psychol. Meas. 1997, 57, 785–799. [Google Scholar] [CrossRef]
- Griffin, S.D.; Price, V.J. Living with lifting: Mothers’ perceptions of lifting and back strain in childcare. Occup. Ther. Int. 2000, 7, 1–20. [Google Scholar] [CrossRef]
- Olson, J.A. Mothering co-occupations in caring for infants and young children. In Mothering Occupations: Challenge, Agency and Participation; Esdaile, S.A., Olson, J.A., Eds.; F.A. Davis: Philadelphia, PA, USA, 2004; pp. 28–51. [Google Scholar]
- Lewis, B.; Ridge, D. Mothers reframing physical activity: Family oriented politicism, transgression and contested expertise in Australia. Soc. Sci. Med. 2005, 60, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Hale, C.J.; Hannum, J.W.; Espelage, D.L. Social support and physical health: The importance of belonging. J. Am. Coll. Health 2005, 53, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Vincent, R.; Hocking, C. Factors that might give rise to musculoskeletal disorders when mothers lift children in the home. Physiother. Res. Int. 2013, 18, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Primeau, L. Divisions of household work, routines, and child care occupations in families. J. Occup. Sci. 2000, 7, 19–28. [Google Scholar] [CrossRef]
- Churchill, S.; Stoneman, Z. Correlates of family routines in Head Start Families. Early Child Res. Pract. 2004, 6, 1–15. [Google Scholar]
- Evans, J.; Rodger, S. Mealtimes and bedtimes: Window to family routines and rituals. J. Occup. Sci. 2008, 15, 98–104. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits. Human needs and the self determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Reis, H.T.; Sheldon, K.M.; Gable, S.L.; Roscoe, J.; Ryan, R.M. Daily well-being: The role of autonomy, competence, and relatedness. Pers. Soc. Psychol. B. 2000, 26, 419–435. [Google Scholar] [CrossRef]
- Kenney, J.W.; Bhattacharjee, A. Interactive model of women’s stressors, personality traits and health problems. J. Adv. Nurs. 2000, 32, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Wilkins-Haug, L.; Erickson, K.; Hill, L.; Power, M.; Holzman, G.B.; Schulkin, J. Obstetrician-gynecologists’ opinions and attitudes on the role of genetics in women’s health. J. Women Health Gen. B 2000, 9, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Wu, S.Z.; Liu, Y.Y. Association between social support and health outcomes: A meta-analysis. Kaohsiung J. Med. Sci. 2003, 19, 345–350. [Google Scholar] [CrossRef]
- Hyyppä, M.T.; Mäki, J. Individual-level relationships between social capital and self-rated health in a bilingual community. Prev. Med. 2001, 32, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Knesebeck, O.V.D.; Geyer, S. Emotional support, education and self-rated health in 22 European countries. BMC Public Health 2007, 7. [Google Scholar] [CrossRef]
- Gevir, D.; Goldstand, S.; Weintraub, N.; Parush, S. A comparison of time use between mothers of children with and without disabilities. OTJR 2006, 26, 117–127. [Google Scholar] [CrossRef]
- Doyal, L. What Makes Women Sick? Gender and Political Economy of Health; Macmillian Press: London, UK, 1995. [Google Scholar]
- Anaby, D.; Jarus, T.; Backman, C.L.; Zumbo, B.D. The role of occupational characteristics and occupational imbalance in explaining well-being. Appl. Res. Qual. Life 2010, 5, 81–104. [Google Scholar] [CrossRef]
- McMunn, A.; Bartley, M.; Kuh, D. Women’s health in mid-life: Life course social roles and agency as quality. Soc. Sci. Med. 2006, 63, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Hammell, K.W. Dimensions of meaning in the occupations of daily life. Can. J. Occup. Ther. 2004, 71, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.; Hocking, C.; Smythe, L. The interconnected meanings of occupation: The call, being-with, possibilities. J. Occup. Sci. 2010, 17, 140–149. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bar, M.A.; Jarus, T. The Effect of Engagement in Everyday Occupations, Role Overload and Social Support on Health and Life Satisfaction among Mothers. Int. J. Environ. Res. Public Health 2015, 12, 6045-6065. https://doi.org/10.3390/ijerph120606045
Bar MA, Jarus T. The Effect of Engagement in Everyday Occupations, Role Overload and Social Support on Health and Life Satisfaction among Mothers. International Journal of Environmental Research and Public Health. 2015; 12(6):6045-6065. https://doi.org/10.3390/ijerph120606045
Chicago/Turabian StyleBar, Michal Avrech, and Tal Jarus. 2015. "The Effect of Engagement in Everyday Occupations, Role Overload and Social Support on Health and Life Satisfaction among Mothers" International Journal of Environmental Research and Public Health 12, no. 6: 6045-6065. https://doi.org/10.3390/ijerph120606045
APA StyleBar, M. A., & Jarus, T. (2015). The Effect of Engagement in Everyday Occupations, Role Overload and Social Support on Health and Life Satisfaction among Mothers. International Journal of Environmental Research and Public Health, 12(6), 6045-6065. https://doi.org/10.3390/ijerph120606045