
A Cross-Sectional Study of Heat Wave-Related Knowledge, Attitude, and Practice among the Public in the Licheng District of Jinan City, China

Abstract
:1. Introduction
2. Methods
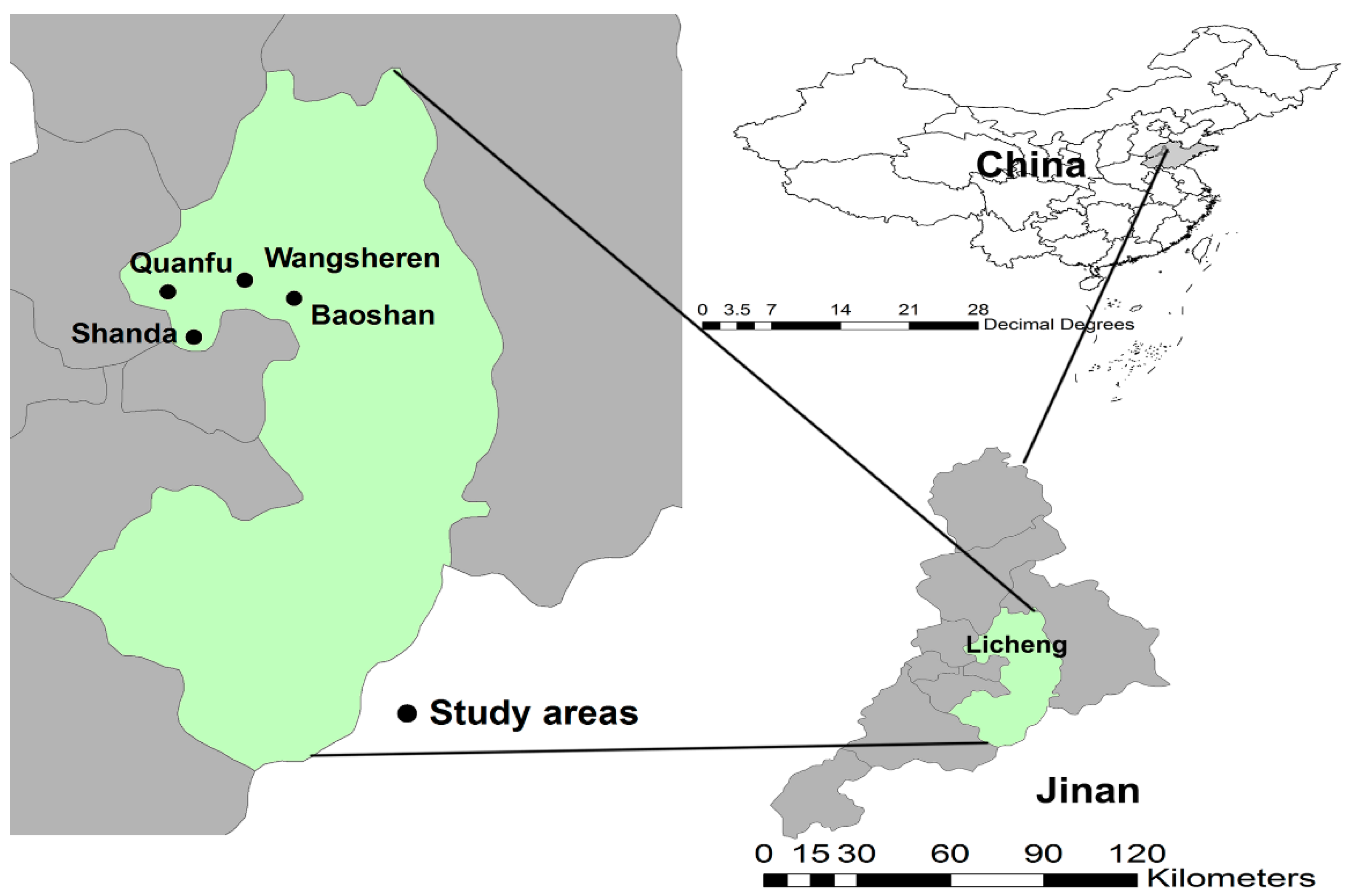
2.1. Study Area and Definition of Heat Waves
2.2. Study Participants
2.3. Data Collection
2.4. Statistical Analysis
3. Ethical Statement
4. Results
4.1. Demographic Information
4.2. Responses to Questions on Heat Wave-Related Knowledge, Attitude, and Practice
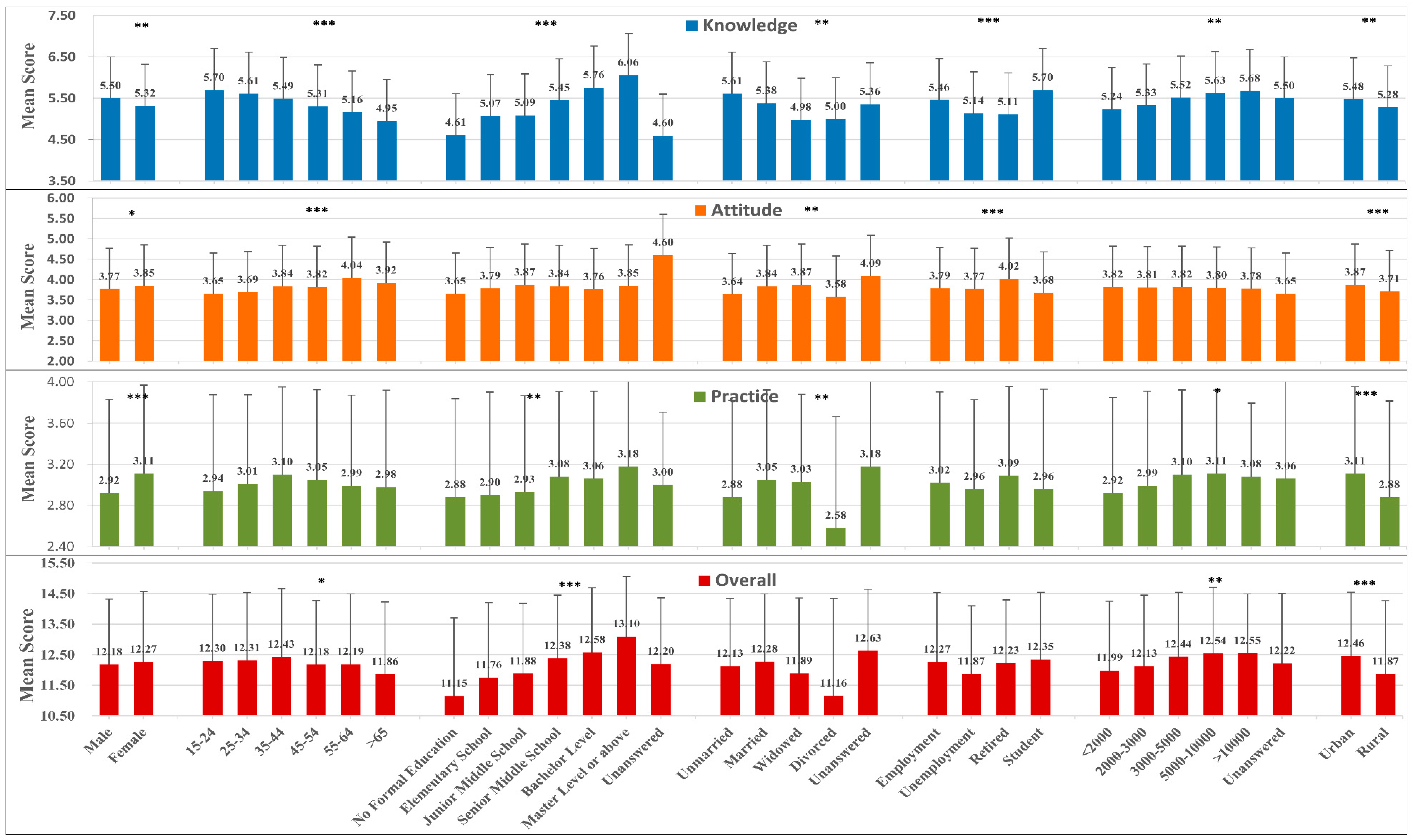
4.3. Mean Scores of Heat Wave-Related Knowledge, Attitude, and Practice
4.4. Assessment of the Overall Score
4.5. Correlation among Heat Wave-Related K, A, and P Scores
4.6. Main and Interactive KAP Effects on Heat Illnesses
4.7. Demographic Characteristics of Participants with a High Level of Practice but a Negative Attitude during Heat Waves
4.8. Reliability and Construct Validity of the Questionnaire
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interests
Abbreviations
| KAP | Knowledge, attitude, and practice |
| SD | Standard deviation |
| OR | Odds ratio |
| aOR | Adjusted odds ratio |
| CI | Confidence interval |
References
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2014 Synthesis Report; IPCC: Geneva, Switzerland, 2014. [Google Scholar]
- White-Newsome, J.L.; McCormick, S.; Sampson, N.; Buxton, M.A.; O’Neill, M.S.; Gronlund, C.J.; Catalano, L.; Conlon, K.C.; Parker, E.A. Strategies to reduce the harmful effects of extreme heat events: A four-city study. Int. J. Environ. Res. Public Health 2014, 11, 1960–1988. [Google Scholar] [CrossRef] [PubMed]
- NWS Office of Climate, Water and Weather Services, the National Climatic Data Center. Summary of Natural Hazard Statistics for 2012 in the United States. Available online: http://www.nws.noaa.gov/os/hazstats/sum12.pdf (accessed on 1 May 2016).
- Moore, R.; Mallonee, S.; Sabogal, R.I.; Zanardi, L.; Redd, J.; Malone, J. From the centers for disease control and prevention. Heat-related deaths—Four states, July-August 2001, and United States, 1979–1999. JAMA 2002, 288, 950–951. [Google Scholar] [PubMed]
- Whitman, S.; Good, G.; Donoghue, E.R.; Benbow, N.; Shou, W.; Mou, S. Mortality in Chicago attributed to the July 1995 heat wave. Am. J. Public Health 1997, 87, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Schar, C.; Jendritzky, G. Climate change: Hot news from Summer 2003. Nature 2004, 432, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Kan, H.; Kovats, S. The impact of the 2003 heat wave on mortality in Shanghai, China. Sci. Total Envirion. 2010, 408, 2418–2420. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, H.Z.; Ou, C.Q.; Lin, G.Z.; Ding, Y.; Zhou, Q.; Shen, J.C.; Chen, P.Y. Impact of heat wave in 2005 on mortality in Guangzhou, China. Biomed. Environ. Sci. 2013, 26, 647–654. [Google Scholar] [PubMed]
- Ma, W.; Zeng, W.; Zhou, M.; Wang, L.; Rutherford, S.; Lin, H.; Liu, T.; Zhang, Y.; Xiao, J.; Wang, X.; et al. The short-term effect of heat waves on mortality and its modifiers in China: An analysis from 66 communities. Environ. Int. 2015, 75, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, S.; Han, J.; Zhou, L.; Liu, Y.; Yang, L.; Zhang, Y. Impact of heat waves on nonaccidental deaths in Jinan, China, and associated risk factors. Int. J. Biometeorol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Grothmann, T.; Patt, A. Adaptive capacity and human cognition: The process of individual adaptation to climate change. Global Environ. Change 2005, 15, 199–213. [Google Scholar] [CrossRef]
- Liu, T.; Xu, Y.; Zhang, Y.; Yan, Q.; Song, X.; Xie, H.; Luo, Y.; Rutherford, S.; Chu, C.; Lin, H.; et al. Associations between risk perception, spontaneous adaptation behavior to heat waves and heatstroke in Guangdong province, China. BMC Public Health 2013, 13, 913. [Google Scholar] [CrossRef] [PubMed]
- Akerlof, K.; DeBono, R.; Berry, P.; Leiserowitz, A.; Roser-Renouf, C.; Clarke, K.-L.; Rogaeva, A.; Nisbet, M.C.; Weathers, M.R.; Maibach, E.W. Public perceptions of climate change as a human health risk: Surveys of the United States, Canada and Malta. Int. J. Environ. Res. Public Health 2010, 7, 2559–2606. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Bi, P.; Nitschke, M.; Pisaniello, D.; Newbury, J.; Kitson, A. Perceptions of heat-susceptibility in older persons: Barriers to adaptation. Int. J. Environ. Res. Public Health 2011, 8, 4714–4728. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.A.; Yamamoto, S.; Malik, A.; Sauerborn, R. Households’ perception of climate change and human health risks: A community perspective. Environ. Health 2012, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Kreft, S.; Eckstein, D. Global Climate Risk Index 2014; Germanwatch e.V.: Berlin, Germany, 2013. [Google Scholar]
- Bai, L.; Cirendunzhu; Pengcuociren; Dawa; Woodward, A.; Liu, X.; Baimaciwang; Dazhen; Sang, S.; Wan, F.; et al. Rapid warming in Tibet, China: Public perception, response and coping resources in urban lhasa. Environ. Health 2013, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Dong, X.; Shi, X.; Ren, G.; Dong, X.; Shi, X.; Ren, G. Climate characteristic of high temperature weather in Jinan in recent 50 a. Meteorol. Environ. Sci. 2007, 30, 95–97. [Google Scholar]
- China Statistics Press. Statistical Yearbook of Jinan City; China Statistics Press: Beijing, China, 2012. [Google Scholar]
- Nitschke, M.; Hansen, A.; Bi, P.; Pisaniello, D.; Newbury, J.; Kitson, A.; Tucker, G.; Avery, J.; Grande, E. Risk factors, health effects and behaviour in older people during extreme heat: A survey in south Australia. Int. J. Environ. Res. Public Health 2013, 10, 6721–6733. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, S.C.; Grothmann, T.; Patt, A. A survey of public perception and response to heat warnings across four north American cities: An evaluation of municipal effectiveness adaptive capacity and human cognition: The process of individual adaptation to climate change. Int. J. Biometeorol. 2007, 52, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Patten, S. Health measurement scales: A practical guide to their development and use, 4th edition. Can. J. Psychiatry 2011, 56, 187–188. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; A Person Education Company: Needham Heights, MA, USA, 2001. [Google Scholar]
- Shen, T.; Howe, H.L.; Alo, C.; Moolenaar, R.L. Toward a broader definition of heat-related death: Comparison of mortality estimates from medical examiners’ classification with those from total death differentials during the July 1995 heat wave in Chicago, Illinois. Am. J. Forensic Med. Pathol. 1998, 19, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, H.; Song, G.; Chen, G.; Jiang, L.; Zhao, N.; Zhang, Y.; Chen, B. Diurnal temperature range and daily mortality in Shanghai, China. Environ. Res. 2007, 103, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Alhakami, A.S.; Slovic, P. A psychological study of the inverse relationship between perceived risk and perceived benefit. Risk Anal. 1994, 14, 1085–1096. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, J.P.; Miller, D.C.; Schafer, W.D. Gender differences in risk taking: A meta-analysis. Psychol. Bull. 1999, 125, 367–383. [Google Scholar] [CrossRef]
- Akompab, D.; Bi, P.; Williams, S.; Grant, J.; Walker, I.; Augoustinos, M. Awareness of and attitudes towards heat waves within the context of climate change among a cohort of residents in adelaide, Australia. Int. J. Environ. Res. Public Health 2013, 10, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Akompab, D.A.; Bi, P.; Williams, S.; Grant, J.; Walker, I.A.; Augoustinos, M. Heat waves and climate change: Applying the health belief model to identify predictors of risk perception and adaptive behaviours in Adelaide, Australia. Int. J. Environ. Res. Public Health 2013, 10, 2164–2184. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.A.; Reid, D.A.; Tobin, A.E. Heatwave hyponatraemia: A case series at a single victorian tertiary centre during January 2014. Int. Med. J. 2015, 45, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Emslie, C.; Fuhrer, R.; Hunt, K.; Macintyre, S.; Shipley, M.; Stansfeld, S. Gender differences in mental health: Evidence from three organisations. Soc. Sci. Med. 2002, 54, 621–624. [Google Scholar] [CrossRef]
- Wanka, A.; Arnberger, A.; Allex, B.; Eder, R.; Hutter, H.P.; Wallner, P. The challenges posed by climate change to successful ageing. Z. Gerontol. Geriatrie 2014, 47, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Kovats, R.S. Will climate change really affect our health? Results from a European assessment. Post Reprod. Health 2004, 10, 139–144. [Google Scholar]
- Pascal, M.; Wagner, V.; Le Tertre, A.; Laaidi, K.; Honore, C.; Benichou, F.; Beaudeau, P. Definition of temperature thresholds: The example of the french heat wave warning system. Int. J. Biometeorol. 2013, 57, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Smargiassi, A.; Goldberg, M.S.; Plante, C.; Fournier, M.; Baudouin, Y.; Kosatsky, T. Variation of daily warm season mortality as a function of micro-urban heat islands. J. Epidemiol. Community Health 2009, 63, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Zhao, M.; Han, R.; Sun, Y. Strategy of adaptation to extreme high temperature in summer of Jinan city under expansion and urban heat island effect. Modern Urban Res. 2014, 4, 67–72. [Google Scholar]
- Goggins, W.B.; Chan, E.Y.; Ng, E.; Ren, C.; Chen, L. Effect modification of the association between short-term meteorological factors and mortality by urban heat islands in Hong Kong. PLoS ONE 2012, 7, e38551. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Zheng, Y.; Tang, X.; Guo, C.; Li, L.; Song, G.; Zhen, X.; Yuan, D.; Kalkstein, A.J.; Li, F.; et al. The urban heat island and its impact on heat waves and human health in Shanghai. Int. J. Biometeorol. 2010, 54, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, K.M.; Endlicher, W.R. Urban and rural mortality rates during heat waves in Berlin and Brandenburg, Germany. Environ. Pollut. 2011, 159, 2044–2050. [Google Scholar] [CrossRef] [PubMed]
- Vitek, J.D.; Berta, S.M. Improving perception of and response to natural hazards: The need for local education. J. Geogr. 1982, 81, 225–228. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Category | n | Proportion (%) |
|---|---|---|---|
| Sex | Male | 1021 | 45.6 |
| Female | 1220 | 54.4 | |
| Age (years) | 15–24 | 263 | 11.7 |
| 25–34 | 564 | 25.2 | |
| 35–44 | 399 | 17.8 | |
| 45–54 | 436 | 19.5 | |
| 55–64 | 276 | 12.3 | |
| ≥65 | 303 | 13.5 | |
| Education level | No formal education | 100 | 4.5 |
| Elementary school | 200 | 8.9 | |
| Junior middle school | 543 | 24.2 | |
| Senior middle school | 667 | 29.8 | |
| Bachelor level | 654 | 29.2 | |
| Master level or above | 71 | 3.2 | |
| Unanswered | 6 | 0.2 | |
| Marital status | Unmarried | 363 | 16.2 |
| Married | 1764 | 78.7 | |
| Divorced | 13 | 0.6 | |
| Widowed | 89 | 4.0 | |
| Unanswered | 12 | 0.5 | |
| Labor force status | Employed * | 1505 | 67.2 |
| Unemployed | 230 | 10.3 | |
| Retired | 322 | 14.4 | |
| Student | 184 | 8.2 | |
| Monthly income (RMB) | <2000 | 562 | 25.1 |
| 2000–3000 | 758 | 33.8 | |
| 3000–5000 | 616 | 27.5 | |
| 5000–10,000 | 225 | 10.0 | |
| >10,000 | 40 | 1.8 | |
| Unanswered | 40 | 1.8 | |
| Hukou | Urban | 1379 | 61.5 |
| Rural | 862 | 38.5 |
| Items | Question | Category | n (%) |
|---|---|---|---|
| Knowledge | Can sprinklers in open grounds and fans play a role in cooling? | Yes | 1845 (82.3) |
| No | 378 (16.9) | ||
| If you wear dark clothes, will you feel cool in summer? | Yes | 603 (26.9) | |
| No | 1614 (72.1) | ||
| Should windows and doors be opened at noon on hot days? | Yes | 859 (38.3) | |
| No | 1357 (60.6) | ||
| Are fever, fatigue, and chest tightness common symptoms of heat stroke? | Yes | 1858 (82.9) | |
| No | 363 (16.2) | ||
| Can some medicines increase the risk of heatstroke? | Yes | 946 (42.2) | |
| No | 1252 (55.9) | ||
| Can death be caused by high temperature? | Yes | 1891 (84.4) | |
| No | 332 (14.8) | ||
| Is the greenhouse effect mainly caused by the depletion of the ozone layer? | Yes | 1617 (72.2) | |
| No | 582 (26) | ||
| Can green plants play a role in cooling? | Yes | 1877 (83.8) | |
| No | 350 (15.6) | ||
| Attitude | Do you intend to take sunstroke prevention measures if a temperature warning is released? | Very much | 570 (25.4) |
| Much | 926 (41.3) | ||
| Some | 524 (23.4) | ||
| So so | 201 (9.0) | ||
| Not at all | 20 (0.9) | ||
| Practice | Do you drink water only when you are thirsty? | Yes | 1258 (56.1) |
| No | 983 (43.9) | ||
| Do you try to arrange outdoor activities at cooler times? | Yes | 1986 (88.6) | |
| No | 255 (11.4) | ||
| When you go out, do you implement good sunstroke prevention measures? | Yes | 1793 (80) | |
| No | 448 (20) | ||
| Do you pay more attention to the elderly, children, or weaker family members? | Yes | 2021 (90.2) | |
| No | 218 (9.8) |
| Variable | Knowledge Score | Attitude Score | Practice Score |
|---|---|---|---|
| Knowledge score | 1 | ||
| Attitude score | 0.068 * | 1 | |
| Practice score | 0.239 * | 0.214 * | 1 |
| Variable | Category | Heat Lllness in the Current Year | |||||
|---|---|---|---|---|---|---|---|
| Without Heat Illness n (%) | With Heat Illness n (%) | Model I OR (95% CI) | Model II aOR (95% CI) | Model III OR (95% CI) | Model IV aOR (95% CI) | ||
| Knowledge | <3 | 69 (80.2) | 17 (19.8) | 1 | 1 | ||
| 3–5 a | 711 (77.7) | 204 (22.3) | 1.17 (0.68–2.02) | 1.14 (0.66–1.98) | |||
| >5 | 904 (83.4) | 180 (16.6) | 0.81 (0.47–1.41) | 0.74 (0.42–1.29) | |||
| Attitude | <3 | 167 (79.1) | 44 (20.9) | 1 | 1 | ||
| ≥3 | 1562 (80.8) | 371 (19.2) | 0.92 (0.64–1.32) | 0.92 (0.64–1.32) | |||
| Practice | <3 | 358 (79.6) | 92 (20.4) | 1 | 1 | ||
| ≥3 | 1370 (80.9) | 323 (19.1) | 0.97 (0.74–1.27) | 0.98 (0.74–1.28) | |||
| Knowledge × Attitude | <3 × <3 | 2 (9.5) | 19 (90.5) | 1 | 1 | ||
| 3–5 × <3 | 24 (24.2) | 75 (75.8) | 3.04 (0.66–14.01) | 2.30 (0.48–10.89) | |||
| >5 × <3 | 18 (19.8) | 73 (80.2) | 2.34 (0.50–10.99) | 1.75 (0.36–8.44) | |||
| <3 × ≥3 | 16 (23.2) | 53 (76.8) | 2.87 (0.60–13.65) | 2.17 (0.44–10.65) | |||
| 3-5 × ≥3 | 190 (22.1) | 668 (77.9) | 0.31 (0.06–1.59) | 0.43 (0.08–2.26) | |||
| >5 × ≥3 | 165 (16.4) | 841 (83.6) | 0.27 (0.05–1.44) | 0.36 (0.06–1.93) | |||
| Knowledge × Practice | <3 × <3 | 11 (23.9) | 35 (76.1) | 1 | 1 | ||
| 3-5 × <3 | 54 (23.1) | 180 (76.9) | 0.95 (0.45–2.01) | 0.87 (0.41–1.86) | |||
| >5 × <3 | 27 (15.8) | 144 (84.2) | 0.59 (0.27–1.32) | 0.52 (0.23–1.16) | |||
| <3 × ≥3 | 7 (15.9) | 37 (84.1) | 0.60 (0.21–1.73) | 0.54 (0.18–1.59) | |||
| 3–5 × ≥3 | 160 (22.1) | 563 (77.9) | 1.57 (0.52–4.78) | 1.77 (0.57–5.49) | |||
| >5 × ≥3 | 156 (16.8) | 770 (83.2) | 1.79 (0.57–5.64) | 1.97 (0.61–6.28) | |||
| Attitude × Practice | <3 × <3 | 11 (12.2) | 79 (87.8) | 1 | 1 | ||
| <3 × ≥3 | 81 (22.4) | 280 (77.6) | 2.59 * (1.22–5.53) | 2.69 * (1.27–5.68) | |||
| ≥3 × <3 | 33 (27.3) | 88 (72.7) | 2.01 * (1.01–3.98) | 2.08 * (1.05–4.09) | |||
| ≥3 × ≥3 | 290 (18.4) | 1281 (81.6) | 0.30 * (0.13–0.67) | 0.29 * (0.13–0.64) | |||
| p-value for main effect of knowledge | 0.006 | 0.001 | |||||
| p-value for the interaction of attitude ≥3 × practice ≥3 | 0.003 | 0.002 | |||||
| Characteristic | Category | n | Proportion (%) |
|---|---|---|---|
| Sex | Male | 61 | 49.2 |
| Female | 63 | 50.8 | |
| Age (years) | 15–34 | 56 | 45.2 |
| 35–54 | 44 | 35.5 | |
| 55–74 | 20 | 16.1 | |
| 75–86 | 4 | 3.2 | |
| Education level | Senior middle school or lower | 83 | 66.9 |
| Higher education | 41 | 33.1 | |
| Marital status | Unmarried | 36 | 29 |
| Married | 24 | 19.4 | |
| Divorced | 96 | 77.4 | |
| Widowed | 4 | 3.2 | |
| Labor force status | Employed | 87 | 70.2 |
| Unemployed | 12 | 9.7 | |
| Retired | 15 | 12.1 | |
| Student | 10 | 8.1 | |
| Monthly income (RMB) | <2000 | 36 | 29 |
| 2000–3000 | 42 | 33.9 | |
| 3000–5000 | 28 | 22.6 | |
| 5000–10,000 | 14 | 11.3 | |
| >10,000 | 4 | 3.2 | |
| Hukou | Urban | 66 | 53.2 |
| Rural | 58 | 46.8 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Xu, X.; Ding, G.; Zhao, Y.; Zhao, R.; Xue, F.; Li, J.; Gao, J.; Yang, J.; Jiang, B.; et al. A Cross-Sectional Study of Heat Wave-Related Knowledge, Attitude, and Practice among the Public in the Licheng District of Jinan City, China. Int. J. Environ. Res. Public Health 2016, 13, 648. https://doi.org/10.3390/ijerph13070648
Li J, Xu X, Ding G, Zhao Y, Zhao R, Xue F, Li J, Gao J, Yang J, Jiang B, et al. A Cross-Sectional Study of Heat Wave-Related Knowledge, Attitude, and Practice among the Public in the Licheng District of Jinan City, China. International Journal of Environmental Research and Public Health. 2016; 13(7):648. https://doi.org/10.3390/ijerph13070648
Chicago/Turabian StyleLi, Jing, Xin Xu, Guoyong Ding, Yun Zhao, Ruixia Zhao, Fuzhong Xue, Jing Li, Jinghong Gao, Jun Yang, Baofa Jiang, and et al. 2016. "A Cross-Sectional Study of Heat Wave-Related Knowledge, Attitude, and Practice among the Public in the Licheng District of Jinan City, China" International Journal of Environmental Research and Public Health 13, no. 7: 648. https://doi.org/10.3390/ijerph13070648
APA StyleLi, J., Xu, X., Ding, G., Zhao, Y., Zhao, R., Xue, F., Li, J., Gao, J., Yang, J., Jiang, B., & Liu, Q. (2016). A Cross-Sectional Study of Heat Wave-Related Knowledge, Attitude, and Practice among the Public in the Licheng District of Jinan City, China. International Journal of Environmental Research and Public Health, 13(7), 648. https://doi.org/10.3390/ijerph13070648