
Childhood Injuries in Singapore: Can Local Physicians and the Healthcare System Do More to Confront This Public Health Concern?


Abstract
:1. Introduction
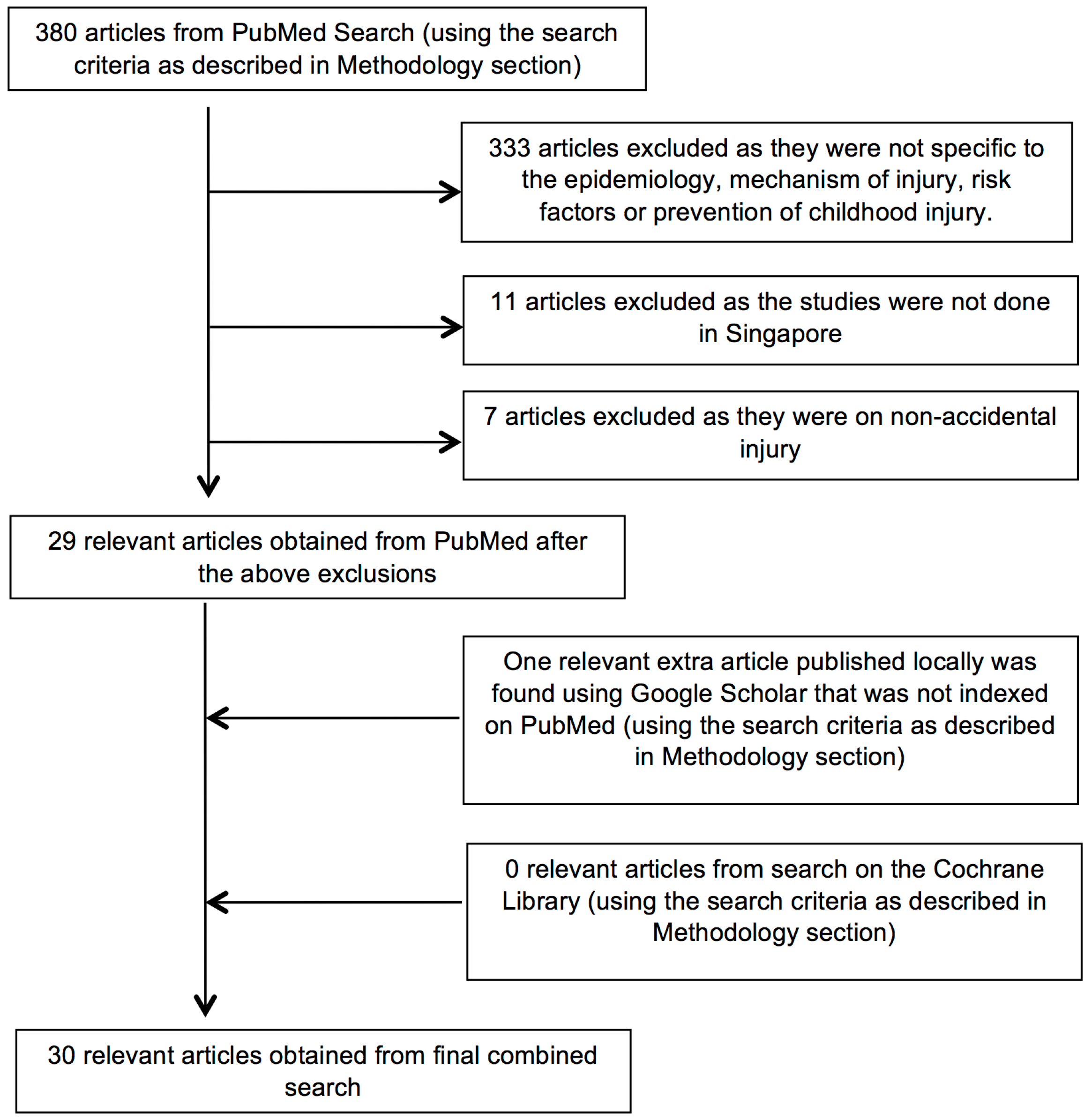
2. Materials and Methods
- Search 1:
- (child OR children OR childhood OR infant OR toddler OR paediatric OR pediatric OR paediatrics OR pediatrics)
- Search 2:
- (accident OR accidents OR trauma OR injury OR injuries)
- Search 3:
- (Singapore OR “Singapore” [Mesh])
3. Results
Part A—Epidemiology, Mechanisms and Risk Factors of Childhood Injuries
Review
Nation-Wide and Community Studies
Childhood Injuries Treated at Emergency Departments (ED)
Childhood Injuries Related to Specific Devices or Accessories
Playground-Related Injuries
Injuries Related to Drowning
Specific Injuries
4. Discussion
4.1. Part B—Prevention Strategies and Recommendations from the Studies Reviewed
4.1.1 Home Injuries
Education Strategies
Engineering Strategies
4.1.2. Childcare Products and Footwear
Education Strategies
Engineering Strategies
Enforcement Strategies
4.1.3. Playground-Injuries
Education Strategies
Engineering Strategies
4.1.4. Transport Related (Child Restraint, Helmets, Cycling, Pedestrian)
Education Strategies
Engineering Strategies
Enforcement Strategies
4.1.5. Drowning and Near Drowning
Education Strategies
Engineering Strategies
Enforcement Strategies
4.1.6. Healthcare Professionals
Education Strategies
4.1.7. Establishment of a Surveillance Database; Public Education and Legislation
Education Strategies
Engineering Strategies
Enforcement Strategies
4.2. Appraisal and Grading of the Recommendations on Prevention of Childhood Injuries in Singapore
5. Conclusions
5.1. What Is Already Known about This Topic
5.2. What This Study Adds
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organisation. Global Burden of Disease, 2004 Update. Available online: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/ (accessed on 15 March 2016).
- World Health Organisation; UNICEF. World Report on Child Injury Prevention, 2008. Available online: http://www.who.int/violence_injury_prevention/child/injury/world_report/en/ (accessed on 15 March 2016).
- World Health Organisation. Injuries and Violence. The Facts 2014. Available online: http://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/ (accessed on 15 March 2016).
- Theurer, W.M.; Bhavsar, A.L. Prevention of unintentional childhood injury. Am. Fam. Physician 2013, 87, 502–509. [Google Scholar] [PubMed]
- World Health Organisation. Global Health Observatory Data Repository, Child Health. Available online: http://apps.who.int/gho/data/node.main.CHILDHEALTH?lang=en (accessed on 15 March 2016).
- Centers for Disease Control and Prevention, National Centre for Health Statistics. Table 81—Initial Injury-Related Visits to Hospital Emergency Departments, by Sex, Age and Intent and Mechanism of Injury: United States, Average Annual, Selected Years 2005–2006 through 2010–2011. Available online: http://www.cdc.gov/nchs/data/hus/2014/081.pdf (accessed on 15 March 2016).
- Ministry of Health Singapore. Health Statistics, Singapore Health Facts, Top 10 Conditions of Hospitalization. Available online: https://www.moh.gov.sg/content/moh_web/home/statistics/Health_Facts_Singapore/Top_10_Conditions_of_Hospitalisation.html (accessed on 15 March 2016).
- Singhealth. What to Do for Common Childhood Injuries—Advice from the Children’s Emergency Physician. Available online: http://www.singhealth.com.sg/patientcare/conditionsandtreatments/pages/injuries-child.aspx (accessed on 15 March 2016).
- Ong, M.E.; Ooi, S.B.; Manning, P.G. A review of 2517 childhood injuries seen in a Singapore Emergency Department in 1999—Mechanisms and Injury prevention suggestions. Singap. Med. J. 2003, 44, 12–19. [Google Scholar]
- Immigration and Checkpoints Authority Singapore, Registry of Births and Deaths. Report on Registration of Births and Death 2014. Available online: http://www.ica.gov.sg/page.aspx?pageid=492 (accessed on 15 March 2016).
- Dowswell, T.; Towner, E.M.; Simpson, G.; Jarvis, S.N. Preventing childhood unintentional injuries—What works? A literature review. Inj. Prev. 1996, 2, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Towner, E.; Dowswell, T.; Jarvis, S. Updating the evidence. A systematic review of what works in preventing childhoods unintentional injuries: Part 1. Inj. Prev. 2001, 7, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Towner, E.; Dowswell, T.; Jarvis, S. Updating the evidence. A systematic review of what works in preventing childhoods unintentional injuries: Part 2. Inj. Prev. 2001, 7, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Bergman, A.B.; Rivara, F.P. Sweden’s experience in reducing childhood injuries. Pediatrics 1991, 88, 69–74. [Google Scholar] [PubMed]
- Kyu, H.H.; Pinho, C.; Wagner, J.A.; Brown, J.C.; Bertozzi-Villa, A.; Charlson, F.J.; Coffeng, L.E.; Dandona, L.; Erskine, H.E.; Ferrari, A.J.; et al. Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013. Findings from the Global Burden of Disease 2013 Study. JAMA Pediatr. 2016, 170, 267–287. [Google Scholar] [PubMed]
- Thein, M.M.; Lee, B.W.; Bun, P.Y. Childhood injuries in Singapore: A community nationwide study. Singap. Med. J. 2005, 46, 116–121. [Google Scholar]
- Thein, M.M.; Lee, B.W.; Bun, P.Y. Knowledge, attitude and practices of childhood injuries and their prevention by primary caregivers in Singapore. Singap. Med. J. 2005, 46, 122–126. [Google Scholar]
- Snodgrass, A.M.; Ang, A. Unintentional injuries in infants in Singapore. Singap. Med. J. 2006, 47, 376–382. [Google Scholar]
- Chong, S.L.; Chew, S.Y.; Feng, J.X.; Teo, P.Y.; Chin, S.T.; Liu, N.; Ong, M.E. A prospective surveillance of paediatric head injuries in Singapore: A dual-centre study. Br. Med. J. 2016, 6, e010618. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.Y.; Nah, S.A.; Lee, Y.T.; Lin, Y.C.; Chiang, L.W. Pedestrian injuries in children: who is most at risk? Singap. Med. J. 2015, 56, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Ngo, A.; Ng, K.C.; Sim, T.P. Otorhinolaryngeal foreign bodies in children presenting to the emergency department. Singap. Med. J. 2005, 46, 172–178. [Google Scholar]
- Ho, L.; Heng, J.T.; Lou, J. Accidental ingestions in childhood. Singap. Med. J. 1998, 39, 5–8. [Google Scholar]
- Tripathi, M.; Tyebally, A.; Feng, J.X.; Chong, S.L. A review of stroller-related and pram-related injuries to children in Singapore. Inj. Prev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Thein, M.M.; Lee, J.; Tay, V.; Ling, S.L. Infant walker use, injuries, and motor development. Inj. Prev. 1997, 3, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.; Ang, A.; Heng, D.; Chen, J.; Wong, H.B. Evaluation of playground injuries based on ICD, E codes, international classification of external cause of injury codes (ICECI), and abbreviated injury scale coding systems. Asia Pac. J. Public Health 2007, 19, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Mahedev, A.; Soon, M.Y.; Lam, K.S. Monkey bars are for monkeys: A study on playground equipment related extremity fractures in Singapore. Singap. Med. J. 2004, 45, 9–13. [Google Scholar]
- Leung, K.W.; Mahedev, A. The cost of sustaining playground related extremity fractures in Singapore. Injury 2011, 42, 352–355. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.Y.; Kumar, S.G.; Mahadev, A. Severity of play-ground related fractures: More than just playground factors? J. Pediatr. Orthop. 2013, 33, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Tyebally, A.; Ang, S.Y. Kids can’t float: Epidemiology of paediatric drowning and near-drowning in Singapore. Singap. Med. J. 2010, 51, 429–433. [Google Scholar]
- Vasanwala, F.F. Childhood injuries in Singapore—A Review. Singap. Fam. Phys. 2010, 36, 47–55. [Google Scholar]
- Chong, S.L.; Barbier, S.; Liu, N.; Ong, G.Y.; Ng, K.C.; Ong, M.E. Predictors for moderate to severe paediatric head injury derived from a surveillance registry in the emergency department. Injury 2015, 46, 1270–1274. [Google Scholar] [CrossRef] [PubMed]
- Ponampalam, R.; Tan, H.H.; Ng, K.C.; Lee, W.Y.; Tan, S.C. Demographics of toxic exposures presenting to three public hospital emergency departments in Singapore 2001–2003. Int. J. Emerg. Med. 2009, 2, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.B.; Tey, I.K.; Lokino, E.S.; Yap, R.T.; Tawng, D.K. Escalators, rubber clogs, and severe foot injuries in children. J. Pediatr. Orthop. 2010, 30, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.; Arjandas, M.; Lim, K.B.; Lee, E.H. Heelys injuries in children. Singap. Med. J. 2006, 47, 373–375. [Google Scholar]
- Ng, I.; Seow, E.; Lee, L.; Ho, L. Closed head injuries in children following the use of a sarong cradle. Singap. Med. J. 1997, 38, 517–519. [Google Scholar]
- Wu, R.S.; Chan, J.X.; Chong, S.L.; Ong, G.Y.; Ng, K.C. Toy safety in Singapore: Where are we now? Singap. Med. J. 2013, 54, 639–642. [Google Scholar] [CrossRef]
- Tan, R.M. The epidemiology and prevention of drowning in Singapore. Singap. Med. J. 2004, 45, 324–329. [Google Scholar]
- Lau, L.L.; Mahadev, A.; Hui, J.H. Common lower limb sport-related overuse injuries in young athletes. Ann. Acad. Med. Singap. 2008, 37, 315–319. [Google Scholar] [PubMed]
- Tan, B.H.; Mahadev, A. Radial neck fractures in children. J. Orthop. Surg. 2011, 19, 209–212. [Google Scholar]
- Chew, E.M.; Chong, A.K. Hand fractures in children: Epidemiology and misdiagnosis in a tertiary referral hospital. J. Hand Surg. Am. 2012, 37, 1684–1688. [Google Scholar] [CrossRef] [PubMed]
- Satku, M.; Puhaindran, M.E.; Chong, A.K. Characteristics of Fingertip Injuries in Children in Singapore. Hand Surg. 2015, 20, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Singapore Police Force. Media Release, December 2011, Changes to Seat Belts Rules and Testing Curriculum for Learner Riders. Available online: http://www.spf.gov.sg/mic/2011/12/20111223 (accessed on 20 March 2016).
- Heng, K.W.; Lee, A.H.; Zhu, S.; Tham, K.Y.; Seow, E. Helmet use and bicycle-related trauma in patients presenting to an acute hospital in Singapore. Singap. Med. J. 2006, 47, 367–372. [Google Scholar]
- Lee, Y.L.; Yip, W.K.; Goh, B.W.; Chiam, E.P.; Ng, H.P. Fall prevention among children in the presence of caregivers in a paediatric ward: A best practice implementation. Int. J. Evid. Based Healthc. 2013, 11, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ebell, M.H.; Siwek, J.; Weiss, B.D.; Woolf, S.H.; Susman, J.; Ewigman, B.; Bowman, M. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am. Fam. Phys. 2004, 69, 548–556. [Google Scholar] [CrossRef]
- Sim, T.P.; Ng, K.C. Childhood injuries: Prevention is always better than cure. Singap. Med. J. 2005, 46, 103–105. [Google Scholar]
- Yen, H.L.; Wong, J.T. Rehabilitation for traumatic brain injury in children and adolescents. Ann. Acad. Med. Singap. 2007, 36, 62–66. [Google Scholar] [PubMed]
- Chan, C.C.; Lui, P.K.; Chow, C.B.; Cheng, J.C.; Wong, T.W. Surveillance of unintentional child injury in Hong Kong. Hong Kong Med. J. 2006, 12, S41–S43. [Google Scholar] [CrossRef]
- Chan, C.C.; Cheng, J.C.; Wong, T.W.; Chow, C.B.; Luis, B.P.; Cheung, W.L.; Chan, K. An international comparison of childhood injuries in Hong Kong. Inj. Prev. 2000, 6, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Family Health Service (Hong Kong). Childhood Injuries and Injury Surveillance in Hong Kong. Available online: http://www.fhs.gov.hk/english/archive/MCHconference2012/presentations/21.pdf (accessed on 3 June 2016).


{kind=link}
| Reference | Study Population | Settings | Main Results | Key Recommendations |
|---|---|---|---|---|
| Nationwide and Community Studies | ||||
| Thein et al. 2005 [16] | 1293 households 2322 children. under 15 years of age | Cross-sectional nationwide community. Survey of households. | Prevalence of injury: 19.5% |
|
| Location of injury | ||||
| ||||
| Location of home injury | ||||
| ||||
| Household hazards | ||||
| ||||
| Increasing incidence of injuries, which corresponded to the increasing number of hazards identified in the household. | ||||
| Thein et al. 2005 [17] | 1293 households 2322 children under 15 years of age. | Cross-sectional nationwide community survey of households. | Main caregiver |
|
| ||||
| Information source on child safety | ||||
| ||||
| Education level is a clear predictor of the mother’s appropriate knowledge and practice on the prevention of childhood injury. | ||||
| Mothers with tertiary education were three times more likely to have the correct knowledge on injury prevention and first aid compared to mothers with primary education or no education (Rate-Ratio 3.1, 95% CI 2.1–4.6). | ||||
| Snodgrass et al. 2006 [18] | 405 infants aged 1 year old or younger, with unintentional injury | 3 ED, 2 polyclinics (primary care centres), HSA. | Infant injuries: 7.7% of total attendances. |
|
| Age range of study population | ||||
| ||||
| Home injuries: 91% | ||||
| Falls-related injuries: 77% | ||||
| Main locations of home injuries | ||||
| ||||
| Objects involved in injury | ||||
| ||||
| 17.9% required hospital admission. | ||||
| Lack of safety features (e.g., non-slip mats, safety barriers, cot rails and seat belts) in 96.1% of fall-related injuries. | ||||
| Childhood Injuries treated at Emergency Departments (ED) | ||||
| Ong et al. 2003 [9] | 2517 Children aged 12 year and below presenting with trauma. | ED of a tertiary children’s hospital. | Mechanism of injury |
|
| ||||
| Hospital admission rate of all injuries: 21.5% 42.5% of road traffic injuries caused by car collisions. | ||||
| Cause of home injuries | ||||
| ||||
| Home injuries | ||||
| ||||
| Pre-school children (under the age of 5 years) as compared to school-going children (aged 6–12 years), had a higher proportion of | ||||
| ||||
| School-going children (aged 6–12 years) as compared to pre-school children (under the age of 5 years), had a higher occurrence of injuries sustained at: | ||||
| ||||
| Children aged 6–12 years had a higher likelihood of being admitted (p = 0.04) or referred for an outpatient follow-up with a specialist (p < 0.0001) compared to children aged below 5 years, whom are more likely to be discharged (p < 0.0001) | ||||
| Chong at al. 2016 [19] | 1049 Children aged less than 16 years. Admitted for head injury. | ED of 2 tertiary children’s hospital. | Mechanisms of injury |
|
| ||||
| Percentage of falls-related injuries at home: 52.2% | ||||
| With every metre increase in the height of fall: | ||||
| ||||
| 75% of road users not using helmets or restraints. | ||||
| Odds ratio of causing death, need for airway or neurosurgical intervention, compared to falls-related head injury: | ||||
| ||||
| Multivariate logistics regression analysis of factors being associated with a poor outcome: | ||||
| ||||
| Feng et al. 2015 [20] | 261 Children aged 16 years or less. Admitted for injuries sustained as pedestrians. | ED of a tertiary children’s hospital. | Gender |
|
| ||||
| Age group | ||||
| ||||
| Site of accident | ||||
| ||||
| 67.8% of all subjects were unaccompanied by an adult. | ||||
| Factors associated with major trauma | ||||
| ||||
| Ngo et al. 2005 [21] | 353 Children aged less than 16 years presenting with suspected foreign body (FB) in the ear, nose or throat. | ED of a tertiary children’s hospital. | Age group (in years) |
|
| ||||
| Ear FB | ||||
| ||||
| Throat FB | ||||
| ||||
| Nasal FB | ||||
| ||||
| Ho et al. 1998 [22] | 112 Children admitted to the paediatric ward for accidental poisoning. | A paediatric ward in a tertiary hospital. | Demographics |
|
| ||||
| Type of ingestion | ||||
| ||||
| Mean hospital stay: 2.4 days | ||||
| Most common reason for unsupervised child: Caregiver pre-occupied with housework (23%) | ||||
| Majority of the medications was | ||||
| ||||
| Childhood Injuries related to Specific Devices or Accessories | ||||
| Tripathi et al. 2016 [23] | 248 Children aged less than 6 years. Pram or stroller related injuries. | Injury surveillance database of a tertiary children’s hospital ED. | Median age: 12.5 months. |
|
| Type of injury | ||||
| ||||
| Location of injury | ||||
| ||||
| Mechanism of injury | ||||
| ||||
| 20.1% required procedural intervention. | ||||
| 17.7% admitted for head injury. | ||||
| 1.6% admitted for procedure under LA. | ||||
| Injuries requiring procedural intervention were significantly associated with older age (p < 0.001) compared with children who were younger. | ||||
| Entrapment injuries were significantly associated with the indication for intervention within the ED (p < 0.001) compared with other mechanisms of injury. | ||||
| Thein et al. 1997 [24] | 185 Parents or caregivers of infants aged 7 to 10 months attending developmental assessment. | A polyclinic (primary care centre). | 90% used walkers regularly. |
|
| Walker-using group | ||||
| ||||
| Group not using walker | ||||
| ||||
| Playground-Related Injuries | ||||
| Tan et al. 2007 [25] | 19,094 Children up to 16 years of age with unintentional injuries. | 3 ED, 2 polyclinics (primary care centres), HSA. | Incidence of play-ground related injuries: 8.5% |
|
| Increasing male predominance with increasing age groups (p = 0.006) | ||||
| Mechanism of injury | ||||
| ||||
| Major sites of injury | ||||
| ||||
| Commonest causative playground equipment | ||||
| ||||
| Risk of sustaining an upper limb fracture at a playground was highest amongst children who were between 6 to 10 years of age compared to the other age groups (p < 0.001). | ||||
| Falls arising from more than 1m in height had a 4.1 times higher risk of an injury involving upper limb fractures (OR = 4.1, p < 0.001) compared to falls from less than 1 m in height. | ||||
| Children who were not accompanied by any caregivers were 1.4 times more likely to sustain upper limb fractures (p < 0.05) compared to children whom are accompanied by caregivers. | ||||
| Mahadev et al. 2004 [26] | 390 Children with playground-related extremity fractures. | A tertiary children’s hospital | Male:Female ratio = 2:1 |
|
| Mean age: 7 years | ||||
| Contribution of the type of equipment to extremity fractures. | ||||
| ||||
| Location of injury | ||||
| ||||
| Leung et al. 2011 [27] | 226 All playground related extremity fractures. | A tertiary children’s hospital. | Mean age: 7.5 years. |
|
| Ratio between male:female = 2:1 | ||||
| Location of injury | ||||
| ||||
| Site of injury | ||||
| ||||
| Contribution of the type of equipment to extremity fractures: | ||||
| ||||
| Type of treatment rendered | ||||
| ||||
| 1.2% of all cases required admission. | ||||
| Cost involved: $247.50–$3792.50 per patient. | ||||
| Lam et al. 2013 [28] | 267 Children less than 17 years old with playground-related fractures. | A tertiary children’s hospital. | Mean age: 7 years. |
|
| Incidence of upper limb fractures: 95.5% | ||||
| Contribution of the type of equipment to extremity fractures | ||||
| ||||
| The presence of any supervision significantly correlate with a lower incidence of major fracture compared to injuries sustained in the absence of any supervision (p = 0.000). | ||||
| In those group of injuries sustained in the presence of supervision, it was found that supervision from parents (18.8%) (p = 0.004) or siblings (16.7%) resulted in a lower incidence of major fractures, compared to grandparents (27.3%) or domestic helpers (25.9%). | ||||
| Increased incidence in major fractures occurring in children with a Body-Mass Index (BMI) at either ends of the extreme (10 percentile or less and 95 percentile or more) (37.9%) compared to those with a BMI between 11 to 94 percentile (27.3%) (p = 0.074). | ||||
| Injuries Related to Drowning | ||||
| Tyebally et al. 2010 [29] | 38 All children seen for drowning and near-drowning. | ED of Singapore Health Services network; HSA | Median age: 6.3 years |
|
| Males: 57.9% | ||||
| Mortality rate: 23.7% | ||||
| Major locations where injury was sustained | ||||
| ||||
| In 47.4% of the cases, there was no safety features at location of the injury. | ||||
| Only 23.6% of the injuries were witnessed by caregivers; | ||||
| 100% of the near drowning cases at swimming pool survived when lifeguard was present. | ||||
| Proposed Recommendation | Evidence Rating | |
|---|---|---|
| Home injuries | ||
| 1. | Raising awareness and reducing common home hazards such as furniture hazards, dangling electrical cord, exposed sharp objects [15,19,30]. | C |
| 2. | Providing education and interventional programs on first aid and fall prevention strategies [16,17]. | C |
| 3. | Dissuading local families from nursing infants or children in adult beds and to encourage the use of proper cots [18]. | C |
| 4. | Increasing the usage of safety gates, non-slip mats, door-stopper or self-closing hinges [18,41]. | C |
| 5. | Regular education to both caregivers and children on poison prevention and proper storage of drugs and chemicals at home (with proper labels and securely locked cupboards) [22,32]. | C |
| 6. | Manufacturing of drugs in child-proof containers, opaque blister packs or strips [22]. | C |
| Childcare products and footwear | ||
| Prams and Strollers | ||
| 7. | Safety checks with appropriate adjustments to ensure a stable and well-balanced structure and absence of any exposed joints or hinges prior to each use [23]. | C |
| 8. | Providing constant supervision of children and ensuring the use of safety harness [23]. | C |
| 9. | Ensuring presence of mandatory safety features which are in compliance with international safety standards or certifications [23]. | C |
| 10. | Special labels and cues sited near injury prone locations such as stairways and escalators; installation of barricades at their exits [23]. | C |
| Escalator Safety and use of rubber clogs | ||
| 11. | Essential safety features on escalators with regular maintenance and lubrication of side panels [33]. | C |
| 12. | Supervision and accompaniment of children by an adult; disallow playing while on escalators [33]. | C |
| 13. | To be mindful of the possibility of any clothing with strings or straps that may be trapped while travelling [33]. | C |
| 14. | Ensuring safe distance between child and sides of escalator; hold onto handrail and face forward [33]. | C |
| Heelys™, infant walkers, toys, high chairs | ||
| 15. | Wearing of safety gear and close supervision by an adult when using Heelys™ [34]. | C |
| 16. | Avoiding the use of infant walkers; consider safer alternative of a crib or playpen [17,24]. | C |
| 17. | Routine inspection of toys for potential hazards; replace or repair damaged toys immediately [35]. | C |
| 18. | Adhere to the recommended age group of each toy in their selection for their children [35]. | C |
| 19. | Ensure fastening of seatbelts with the use of high chairs [9]. | C |
| Sarong cradles | ||
| 20. | The dangers and potential morbidity in the use of sarong cradles should be publicized and have its usage discouraged [17,18,35]. | C |
| 21. | Dedicated supervision by a responsible adult; ensuring the usage of proper sarong length; routine inspections for potential defects; usage of an appropriate protective material around the area of the cradle, to reduce sarong-related injuries [35]. | C |
| Playground injuries | ||
| 22. | Review of the heights of common playground equipment to ensure that they are age-appropriate [25]. | C |
| 23. | Restricting the maximum height of any hanging equipment to 1500 mm [18,26]. | C |
| 24. | Prominent displays of safety advice on the use of equipment in the playground [25]. | C |
| 25. | Monkey bars should be substituted with safer equipment [18,25,26,27]. | C |
| 26. | Maintaining the child’s BMI within the recommended limits [28]. | C |
| Transportation-related injuries | ||
| 27. | More publicity efforts to boost the awareness on the updated legislation in Singapore with regards to the obligatory usage of appropriate child restraints or booster seats in cars for anyone below the height of 1.35 m [16,17,18,19,42]. | C |
| 28. | Stricter enforcement of the child restraint seat law [18]. | C |
| 29. | Introduction of child safety programs at the ED [19]. | C |
| 30. | Mandatory use of helmets while riding bicycles at all times; wearing of proper footwear for cycling [18,43]. | C |
| 31. | Not allowing young children to manoeuvre roads or car parks alone but to ensure that they are properly supervised [20]. | C |
| Drowning and near drowning | ||
| 32. | Avoid having water-filled pails at home or to ensure that children do not have access to these pails or ponds at home [18,29,30]. | C |
| 33. | Adult supervision should always be present when bathing infants or toddlers [29]; and when children are at swimming pools, seas or any water features [29,37]. | C |
| 34. | Having adequate essential safety features at swimming pools and sea-side [29,37]. | C |
| 35. | Considering formal legislatures of the need for lifeguards and pool fencing [18,29,37]. | C |
| 36. | Acquiring of swimming skills and access to aquatic safety education among all children [37]. | C |
| Role of healthcare professionals and nation-wide initiatives | ||
| 37. | Advocates of health education and provision of injury prevention advice during antenatal or postnatal visits, as well as immunization and developmental assessment sessions [16,17]. | C |
| 38. | Education of caregiver on fall prevention strategies to increase their awareness and preventing inpatient falls in children [44]. | C |
| 39. | Establishment of a robust injury surveillance database for epidemiological analysis and enabling targeted future initiatives for safety campaigns and injury prevention [18,25]. | C |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, A.C.W.; Low, S.G.; Vasanwala, F.F. Childhood Injuries in Singapore: Can Local Physicians and the Healthcare System Do More to Confront This Public Health Concern? Int. J. Environ. Res. Public Health 2016, 13, 718. https://doi.org/10.3390/ijerph13070718
Ong ACW, Low SG, Vasanwala FF. Childhood Injuries in Singapore: Can Local Physicians and the Healthcare System Do More to Confront This Public Health Concern? International Journal of Environmental Research and Public Health. 2016; 13(7):718. https://doi.org/10.3390/ijerph13070718
Chicago/Turabian StyleOng, Alvin Cong Wei, Sher Guan Low, and Farhad Fakhrudin Vasanwala. 2016. "Childhood Injuries in Singapore: Can Local Physicians and the Healthcare System Do More to Confront This Public Health Concern?" International Journal of Environmental Research and Public Health 13, no. 7: 718. https://doi.org/10.3390/ijerph13070718
APA StyleOng, A. C. W., Low, S. G., & Vasanwala, F. F. (2016). Childhood Injuries in Singapore: Can Local Physicians and the Healthcare System Do More to Confront This Public Health Concern? International Journal of Environmental Research and Public Health, 13(7), 718. https://doi.org/10.3390/ijerph13070718