
Brief Counseling on Secondhand Smoke Exposure in Pregnant Women in Argentina and Uruguay

Abstract
:1. Introduction
2. Materials and Methods
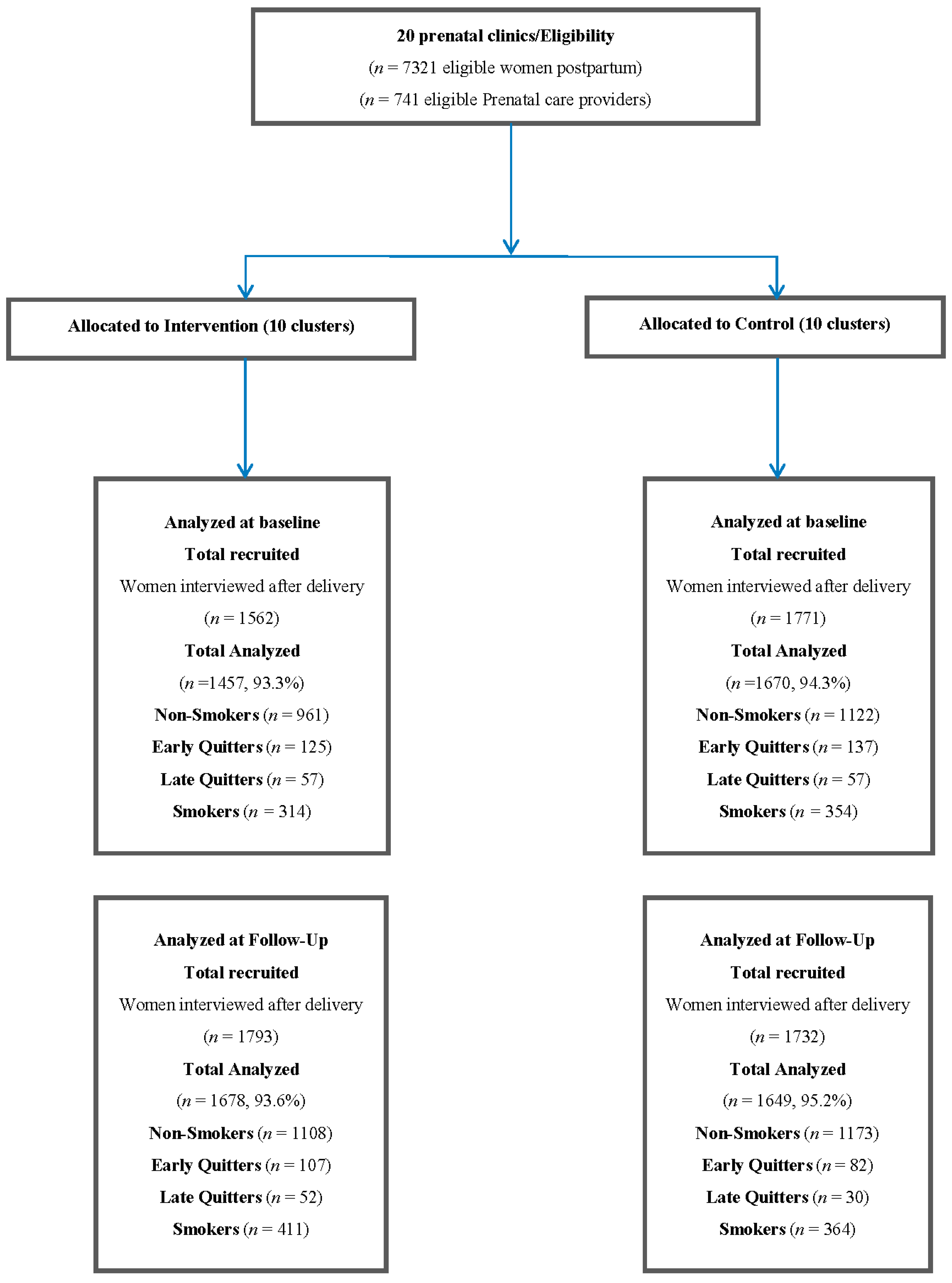
2.1. Study Design and Participants
2.2. Exposure and Outcomes Considered for This Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Strengths and Limitations
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chen, C.; Huang, Y.B.; Liu, X.O.; Gao, Y.; Dai, H.J.; Song, F.J.; Li, W.Q.; Wang, J.; Yan, Y.; Wang, P.S.; et al. Active and passive smoking with breast cancer risk for Chinese females: A systematic review and meta-analysis. Chin. J. Cancer 2014, 33, 306–316. [Google Scholar] [CrossRef]
- Luo, Z.; Julien, P.; Wei, S.Q.; Audibert, F.; Smith, G.N.; Fraser, W.D.; MIROS Study Group. Plasma cotinine indicates an increased risk of preeclampsia in previous and passive smokers. Am. J. Obstet. Gynecol. 2014, 210, 232.e1–232.e5. [Google Scholar] [CrossRef] [PubMed]
- Leonardi-Bee, J.; Britton, J.; Venn, A. Secondhand smoke and adverse fetal outcomes in nonsmoking pregnant women: A meta-analysis. Pediatrics 2011, 127, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D.; Knowledge Synthesis Group. Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Gong, T.-T.; Liu, C.-X.; Wu, Q.-J. Associations between Passive Maternal Smoking during Pregnancy and Preterm Birth: Evidence from a Meta-Analysis of Observational Studies. PLoS ONE 2016, 11, e0147848. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Dadvand, P.; Grellier, J.; Martinez, D.; Vrijheid, M. Environmental risk factors of pregnancy outcomes: A summary of recent meta-analyses of epidemiological studies. Environ. Health 2013, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, C.; Arija Val, V.; Escribano Subías, J.; Canals Sans, J. A longitudinal study on the effects of maternal smoking and secondhand smoke exposure during pregnancy on neonatal neurobehavior. Early Hum. Dev. 2012, 88, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Evlampidou, I.; Bagkeris, M.; Vardavas, C.; Koutra, K.; Patelarou, E.; Koutis, A.; Chatzi, L.; Kogevinas, M. Prenatal Second-Hand Smoke Exposure Measured with Urine Cotinine May Reduce Gross Motor Development at 18 Months of Age. J. Pediatr. 2015, 167, 246–252.e2. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Leung, P.W.; McCauley, L.; Ai, Y.; Pinto-Martin, J. Mother’s environmental tobacco smoke exposure during pregnancy and externalizing behavior problems in children. Neurotoxicology 2013, 34, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Clifford, A.; Lang, L.; Anstey, K. Is exposure to secondhand smoke associated with cognitive parameters of children and adolescents? A systematic literature review. Ann. Epidemiol. 2013, 23, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.; Althabe, F.; Onyamboko, M.; Kaseba-Sata, C.; Castilla, E.E.; Freire, S.; Garces, A.L.; Parida, S.; Goudar, S.S.; Kadir, M.M.; et al. Tobacco use and secondhand smoke exposure during pregnancy: An investigative survey of women in 9 developing nations. Am. J. Public Health 2008, 98, 1833–1840. [Google Scholar] [CrossRef] [PubMed]
- Tong, V.T.; Morello, P.; Alemán, A.; Johnson, C.; Dietz, P.M.; Farr, S.L.; Mazzoni, A.; Berrueta, M.; Colomar, M.; Ciganda, A.; et al. Pregnant women’s secondhand smoke exposure and receipt of screening and brief advice by prenatal care providers in Argentina and Uruguay. Matern. Child Health J. 2015, 19, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations for the Prevention and Management of Tobacco Use and Second-Hand Smoke Exposure in Pregnancy; World Health Organization: Geneva, Switzerland, 2013; Available online: http://www.who.int/tobacco/publications/pregnancy/guidelinestobaccosmokeexposure/en/ (accessed on 20 July 2016).
- Althabe, F.; Aleman, A.; Berrueta, M.; Morello, P.; Gibbons, L.; Colomar, M.; Tong, V.T.; Dietz, P.M.; Farr, S.L.; Ciganda, A.; et al. A multifaceted strategy to implement brief smoking cessation counselling during antenatal care in Argentina and Uruguay: A cluster randomized trial. Nicotine Tob. Res. 2016, 18, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Althabe, F.; Alemán, A.; Mazzoni, A.; Berrueta, M.; Morello, P.; Colomar, M.; Ciganda, A.; Becú, A.; Gibbons, L.; Llambi, L.; et al. Tobacco cessation intervention for pregnant women in Argentina and Uruguay: Study protocol. Reprod. Health 2013, 10, 10–44. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Tong, E.K.; Mao, Z.; Hu, T.W.; Lee, A.H. A Clustered Randomized Controlled Trial to Reduce Secondhand Smoke Exposure Among Nonsmoking Pregnant Women in Sichuan Province, China. Nicotine Tob. Res. 2016, 18, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Tong, V.T.; Dietz, P.M.; Rolle, I.V.; Kennedy, S.; Thomas, W.; England, L. Clinical interventions to reduce secondhand smoke exposure among pregnant women: A systematic review. Tob. Control 2015, 24, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hsia, J.; Tu, X.; Xia, Y.; Zhang, L.; Bi, Z.; Liu, H.; Li, X.; Stanton, B. Exposure to secondhand tobacco smoke and interventions among pregnant women in China: A systematic review. Prev. Chronic Dis. 2015, 12, E35. [Google Scholar] [CrossRef] [PubMed]
- Passey, M.E.; Longman, J.M.; Robinson, J.; Wiggers, J.; Jones, L.L. Smoke-free homes: What are the barriers, motivators and enablers? A qualitative systematic review and thematic synthesis. BMJ Open 2016, 17, e010260. [Google Scholar] [CrossRef] [PubMed]
- Uruguay 2008 Ley N° 18.256. Poder Legislativo. Available online: https://legislativo.parlamento.gub.uy/temporales/leytemp9782645.htm (accessed on 29 July 2016).
- Argentina 2011. Ley 26.687. Poder Legislativo. Available online: http://www.msal.gob.ar/tabaco/index.php/component/content/article/4-destacados-slide/82-argentina-tiene-una-ley-nacional-de-control-de-tabaco (accessed on 29 July 2016).
- Stigler, S.M. Regression towards the mean, historically considered. Stat. Methods Med. Res. 1997, 6, 103–114. [Google Scholar] [PubMed]
- Cooke, M.; Mattick, R.P.; Campbell, E. The dissemination of a smoking cessation program to 23 antenatal clinics: The predictors of initial program adoption by managers. Aust. N. Z. J. Public Health 1999, 23, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Lowe, J.B.; Balanda, P.K.; Stanton, W.R.; Del Mar, C.; O’Connor, V. Dissemination of an efficacious antenatal smoking cessation program in public hospitals in Australia: A randomized controlled trial. Health Educ. Behav. 2002, 29, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Jeong, B.Y.; Lim, M.K.; Yun, E.H.; Oh, J.K.; Park, E.Y.; Lee, D.H. Tolerance for and potential indicators of second-hand smoke exposure among nonsmokers: A comparison of self-reported and cotinine verified second-hand smoke exposure based on nationally representative data. Prev. Med. 2014, 67, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Galán, I.; Mayo, E.; López, M.J.; Pérez-Ríos, M.; Fu, M.; Martínez-Sánchez, J.M.; Schiaffino, A.; Moncada, A.; Montes, A.; Nebot, M.; et al. Validity of self-reported exposure to second-hand smoke in hospitality venues. Environ. Res. 2014, 133, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Max, W.; Sung, H.Y.; Shi, Y. Who is exposed to secondhand smoke? Self-reported and serum cotinine measured exposure in the U.S., 1999–2006. Int. J. Environ. Res. Public Health 2009, 6, 1633–1648. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intervention Group (10 Clusters) | Control Group (10 Clusters) | Intervention Effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Rate (n = 1143) | Follow-Up Period Rate (n = 1267) | OR † | p-Value * | Baseline Rate (n = 1316) | Follow-Up Period Rate (n = 1285) | OR † | p-Value * | ROR ‡ (95% CI) | p-Value § | |
| SHS at home | 23.1 | 19.6 | 0.83 (0.63–1.09) | 0.1809 | 23.1 | 18.0 | 0.73 (0.55–0.97) | 0.0286 | 1.14 (0.77–1.69) | 0.5103 |
| SHS at work ** | 20.3 | 9.8 | 0.42 (0.17–1.04) | 0.0610 | 11.3 | 13.9 | 1.26 (0.43–3.71) | 0.6788 | 0.33 (0.08–1.37) | 0.1269 |
| Always or sometimes around smokers indoors (home, work, public places) | 40.4 | 41.8 | 1.03 (0.77–1.38) | 0.8367 | 48.1 | 45.5 | 0.93 (0.69–1.25) | 0.6246 | 1.11 (0.73–1.69) | 0.6213 |
| Intervention Group (5 Clusters) | Control Group (5 Clusters) | Intervention Effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Argentina | Baseline Rate (n = 700) | Follow-Up Period Rate (n = 792) | OR † | p-Value * | Baseline Rate (n = 768) | Follow-Up Period Rate (n = 705) | OR † | p-Value * | ROR ‡ (95% CI) | p-Value § |
| SHS at home | 25.7 | 17.8 | 0.65 (0.5–0.84) | 0.0012 | 24.7 | 15.1 | 0.55 (0.43–0.7) | <0.0001 | 1.18 (0.82–1.69) | 0.3659 |
| SHS at work ** | 25.3 | 9.1 | 0.28 (0.1–0.81) | 0.0186 | 12.9 | 14.4 | 1.13 (0.34–3.73) | 0.8389 | 0.25 (0.05–1.23) | 0.0881 |
| Always or sometimes around smokers indoor (home, work, public places) | 38.7 | 39.4 | 0.99 (0.62–1.57) | 0.9500 | 51.6 | 47.2 | 0.89 (0.53–1.5) | 0.673 | 1.1 (0.5–2.21) | 0.7849 |
| Uruguay | (n = 443) | (n = 475) | OR † | p-Value * | (n = 548) | (n = 580) | OR † | p-Value * | ROR ‡ (95% CI) | p-Value § |
| SHS at home | 19.0 | 22.5 | 1.25 (0.93–1.68) | 0.1446 | 21.0 | 21.6 | 1.02 (0.77–1.36) | 0.8944 | 1.22 (0.81–1.85) | 0.3372 |
| SHS at work | 9.1 | 11.3 | 1.08 (0.43–2.73) | 0.8665 | 6.1 | 12.1 | 2.11 (0.19–23.34) | 0.5427 | 0.51 (0.04–6.74) | 0.6117 |
| Always or sometimes around smokers indoor (home, work, public places) | 43.1 | 45.7 | 1.11 (0.89–1.38) | 0.3563 | 43.1 | 43.4 | 0.98 (0.84–1.14) | 0.8027 | 1.13 (0.87–1.47) | 0.3678 |
| Intervention Group (10 Clusters) | Control Group (10 Clusters) | Intervention Effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Rate (n = 1143) | Follow-Up Period Rate (n = 1267) | OR † | p-Value * | Baseline Rate (n = 1316) | Follow-Up Period Rate (n = 1285) | OR † | p-Value * | ROR ‡ (95% CI) | p Value § | |
| Always or sometimes try to avoid breathing smoke expelled by people smoking near you | 86.8 | 87.4 | 1.07 (0.89–1.29) | 0.4719 | 87.6 | 87.4 | 0.99 (0.7–1.4) | 0.9525 | 1.08 (0.73–1.6) | 0.6905 |
| There are rooms where smoking is forbidden | 91.5 | 92.6 | 1.16 (0.9–1.51) | 0.2486 | 89.5 | 93.4 | 1.61 (1.2–2.15) | 0.0015 | 0.72 (0.49–1.07) | 0.1062 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alemán, A.; Morello, P.; Colomar, M.; Llambi, L.; Berrueta, M.; Gibbons, L.; Buekens, P.; Althabe, F. Brief Counseling on Secondhand Smoke Exposure in Pregnant Women in Argentina and Uruguay. Int. J. Environ. Res. Public Health 2017, 14, 28. https://doi.org/10.3390/ijerph14010028
Alemán A, Morello P, Colomar M, Llambi L, Berrueta M, Gibbons L, Buekens P, Althabe F. Brief Counseling on Secondhand Smoke Exposure in Pregnant Women in Argentina and Uruguay. International Journal of Environmental Research and Public Health. 2017; 14(1):28. https://doi.org/10.3390/ijerph14010028
Chicago/Turabian StyleAlemán, Alicia, Paola Morello, Mercedes Colomar, Laura Llambi, Mabel Berrueta, Luz Gibbons, Pierre Buekens, and Fernando Althabe. 2017. "Brief Counseling on Secondhand Smoke Exposure in Pregnant Women in Argentina and Uruguay" International Journal of Environmental Research and Public Health 14, no. 1: 28. https://doi.org/10.3390/ijerph14010028
APA StyleAlemán, A., Morello, P., Colomar, M., Llambi, L., Berrueta, M., Gibbons, L., Buekens, P., & Althabe, F. (2017). Brief Counseling on Secondhand Smoke Exposure in Pregnant Women in Argentina and Uruguay. International Journal of Environmental Research and Public Health, 14(1), 28. https://doi.org/10.3390/ijerph14010028