
The Effects of Age, Period, and Cohort on Mortality from Ischemic Heart Disease in China


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
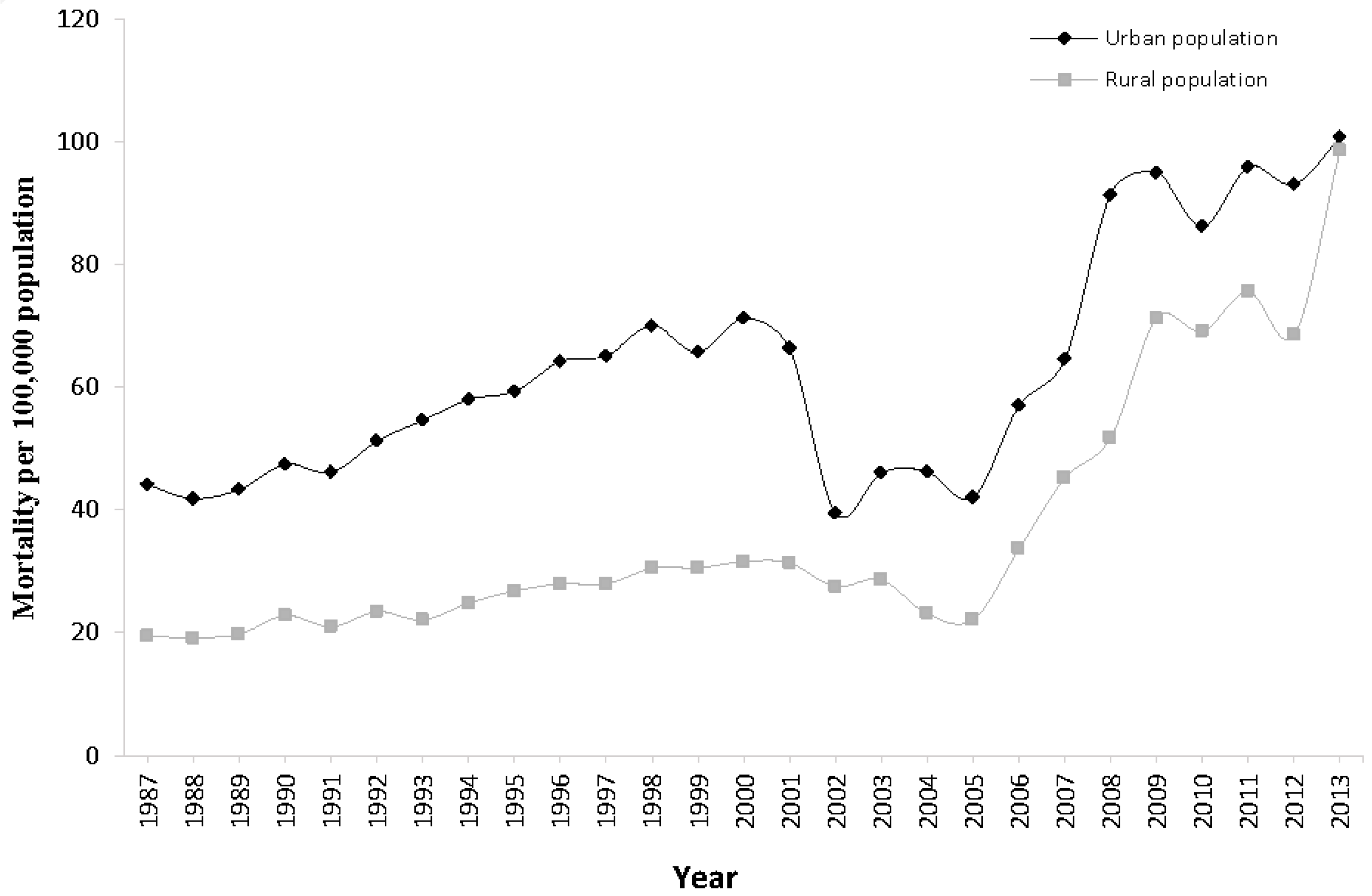
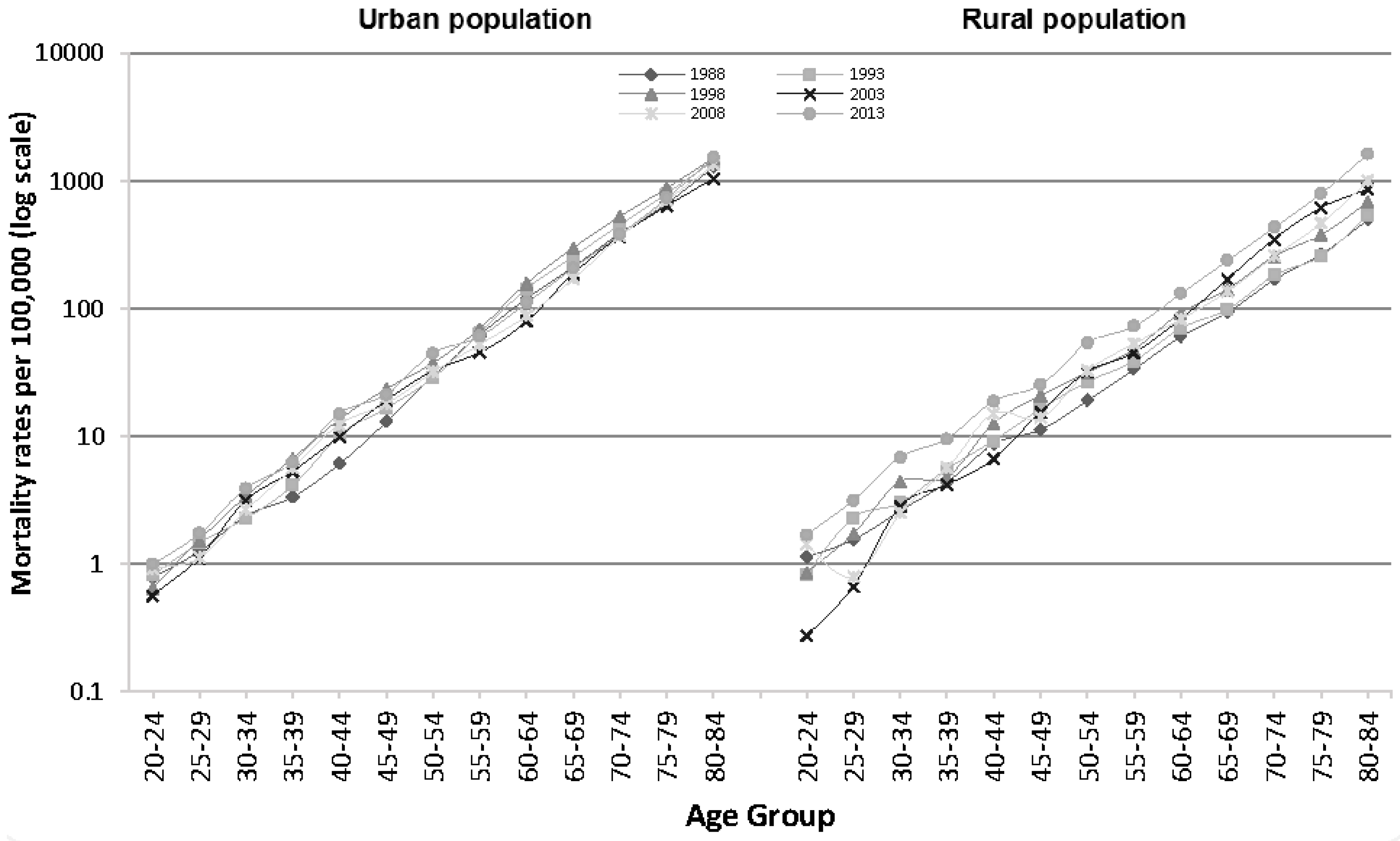
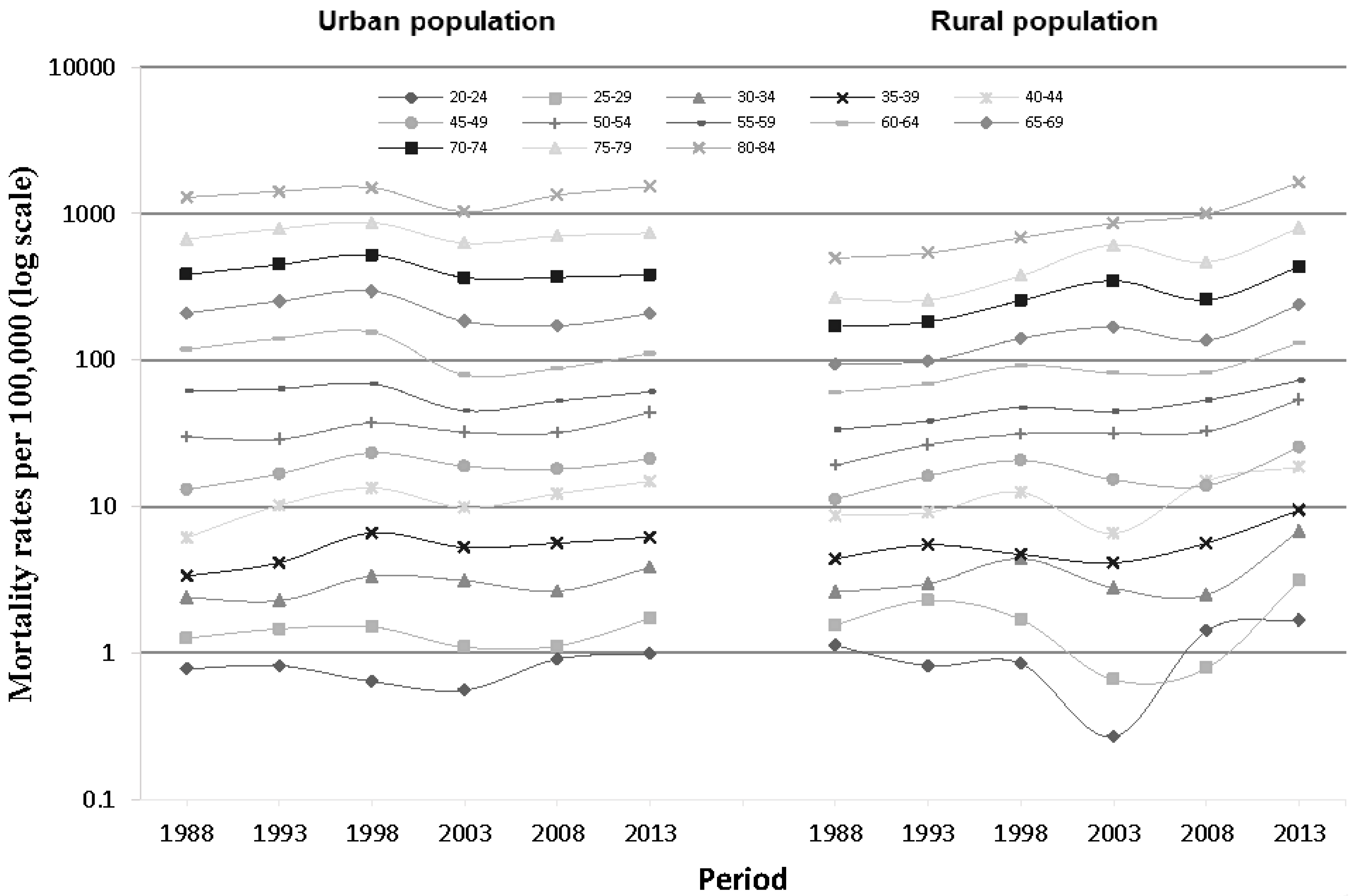
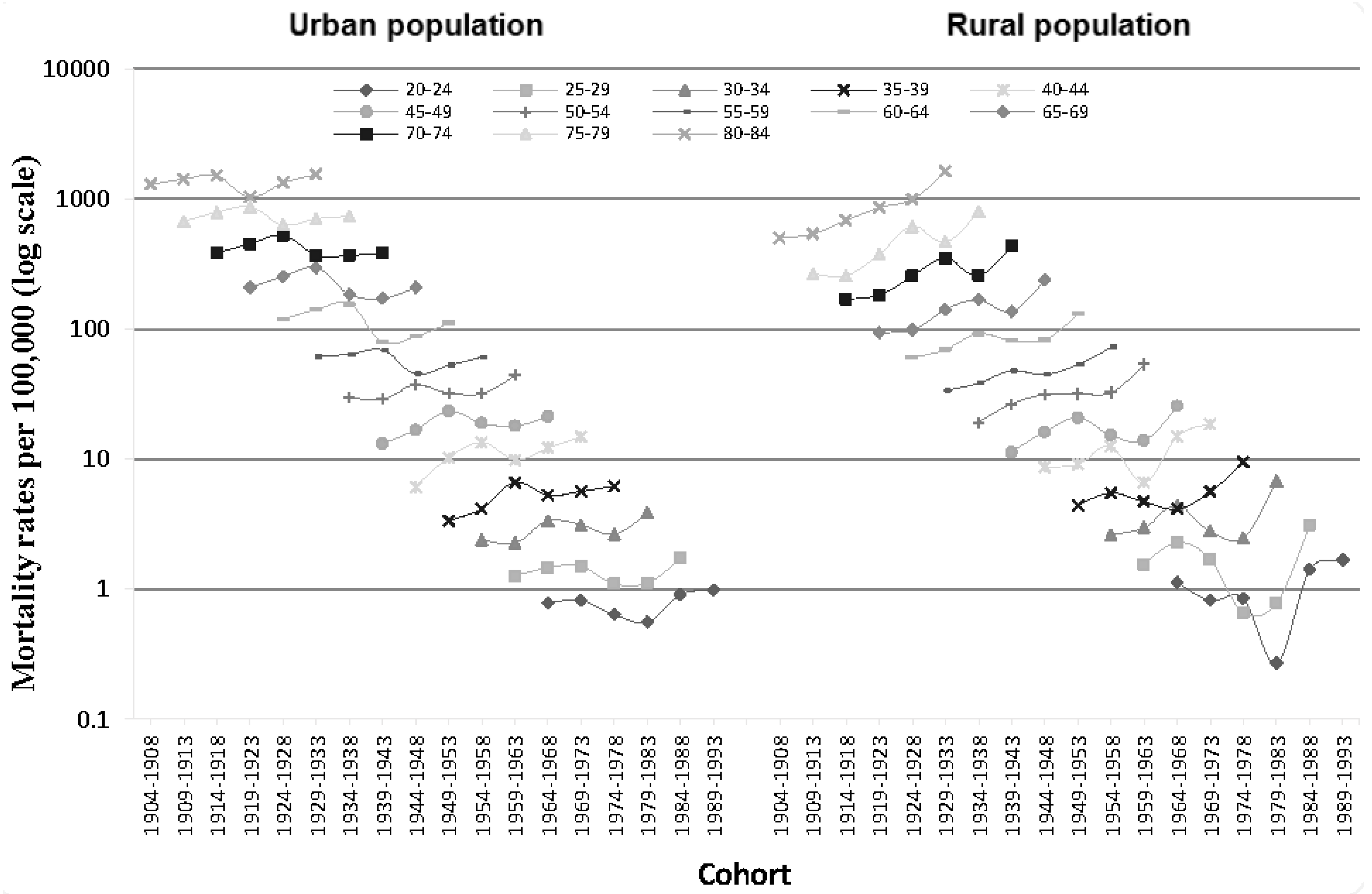
3.1. Descriptive Analysis
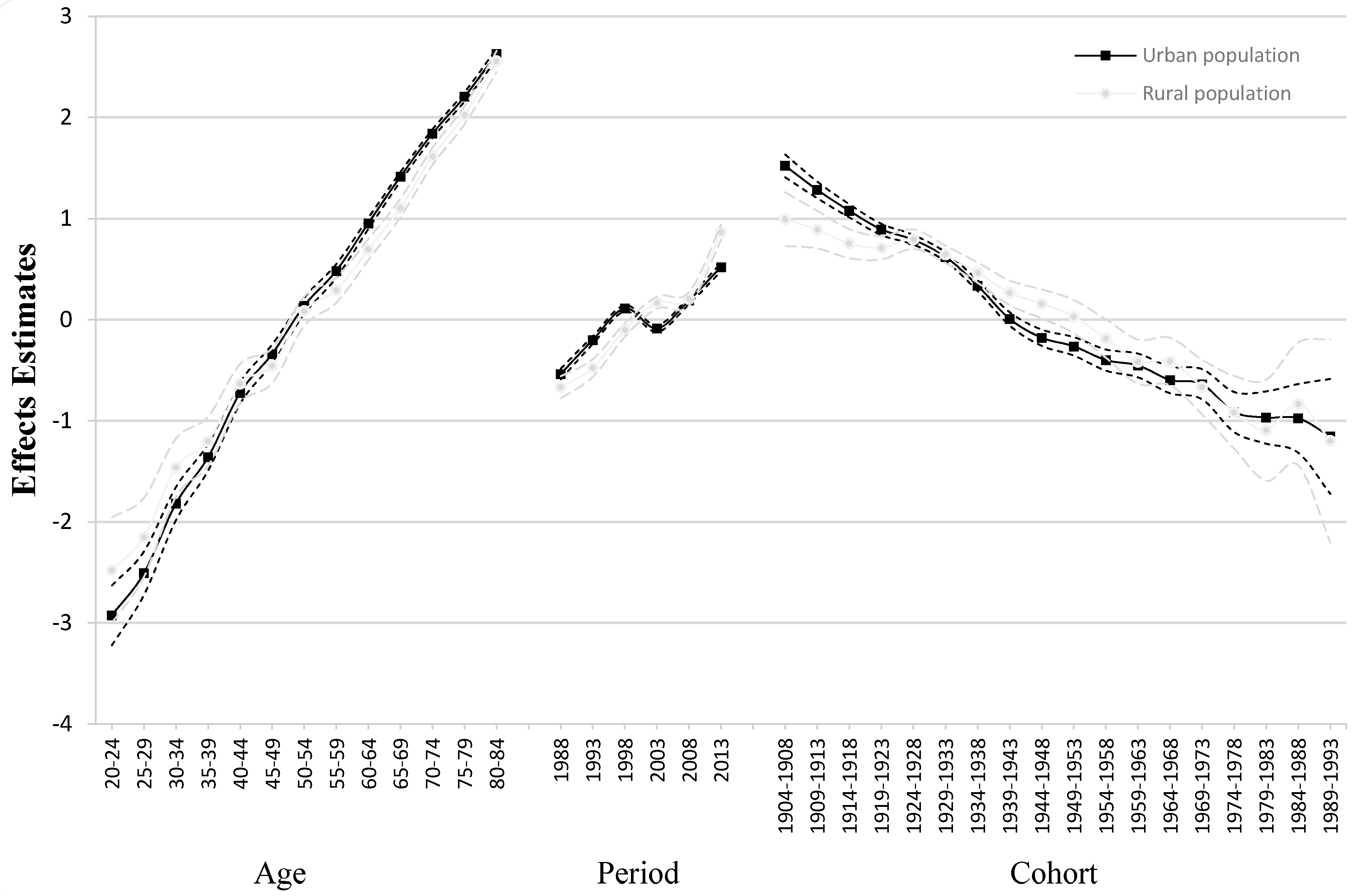
3.2. Statistical Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Moran, A.E.; Forouzanfar, M.H.; Roth, G.A.; Mensah, G.A.; Ezzati, M.; Flaxman, A.; Murray, C.J.; Naghavi, M. The global burden of ischemic heart disease in 1990 and 2010: The Global Burden of Disease 2010 study. Circulation 2014, 129, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.; VanderZanden, A.; Moran, A.; Naghavi, M.; Murray, C.; Roth, G. Ischemic Heart Disease Worldwide, 1990 to 2013: Estimates From the Global Burden of Disease Study 2013. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 455–456. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Moran, A.E.; Flaxman, A.D.; Roth, G.; Mensah, G.A.; Ezzati, M.; Naghavi, M.; Murray, C.J. Assessing the global burden of ischemic heart disease, part 2: Analytic methods and estimates of the global epidemiology of ischemic heart disease in 2010. Glob. Heart 2012, 7, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.E.; Oliver, J.T.; Mirzaie, M.; Forouzanfar, M.H.; Chilov, M.; Anderson, L.; Morrison, J.L.; Khan, A.; Zhang, N.; Haynes, N.; et al. Assessing the Global Burden of Ischemic Heart Disease: Part 1: Methods for a Systematic Review of the Global Epidemiology of Ischemic Heart Disease in 1990 and 2010. Glob. Heart 2012, 7, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Hartley, A.; Marshall, D.C.; Salciccioli, J.D.; Sikkel, M.B.; Maruthappu, M.; Shalhoub, J. Trends in Mortality From Ischemic Heart Disease and Cerebrovascular Disease in Europe: 1980 to 2009. Circulation 2016, 133, 1916–1926. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; McKee, M. Documenting the global burden of cardiovascular disease: A major achievement but still a work in progress. Circulation 2014, 129, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, T.A.; Bitton, A.; Anand, S.; Abrahams-Gessel, S.; Murphy, A. Growing epidemic of coronary heart disease in low- and middle-income countries. Curr. Probl. Cardiol. 2010, 35, 72–115. [Google Scholar] [CrossRef] [PubMed]
- Nowbar, A.N.; Howard, J.P.; Finegold, J.A.; Asaria, P.; Francis, D.P. 2014 global geographic analysis of mortality from ischaemic heart disease by country, age and income: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2014, 174, 293–298. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; World Heart Federation; World Stroke Organization. Global Atlas on Cardiovascular Disease Prevention and Control: Policies, Strategies and Interventions. 2011. Available online: http://www.who.int/cardiovascular_diseases/publications/atlas_cvd/en/ (accessed on 12 September 2016).
- Barquera, S.; Pedroza-Tobías, A.; Medina, C.; Hernández-Barrera, L.; Bibbins-Domingo, K.; Lozano, R.; Moran, A.E. Global Overview of the Epidemiology of Atherosclerotic Cardiovascular Disease. Arch. Med. Res. 2015, 46, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Glenn, N.D. Age, Period, and Cohort Effects. In Encyclopedia of Social Measurement; Kempf-Leonard, K., Ed.; Elsevier: Amsterdam, The Netherlands, 2005; pp. 27–32. [Google Scholar]
- Yang, Y. Trends in U.S. adult chronic disease mortality, 1960–1999: Age, period, and cohort variations. Demography 2008, 45, 387–416. [Google Scholar] [CrossRef]
- Yu, I.T.; Li, W.; Wong, T.W. Effects of age, period and cohort on acute myocardial infarction mortality in Hong Kong. Int. J. Cardiol. 2004, 97, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Kong, L.; Zhao, W.; Wan, X.; Zhai, Y.; Chen, L.C.; Koplan, J.P. Emergence of chronic non-communicable diseases in China. Lancet 2008, 372, 1697–1705. [Google Scholar] [CrossRef]
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar]
- Ocaña-Riola, R.; Mayoral-Cortés, J.M.; Fernández-Ajuria, A.; Sánchez-Cantalejo, C.; Martín-Olmedo, P.; Blanco-Reina, E. Age, Period, and Cohort Effects on Mortality From Ischemic Heart Disease in Southern Spain. Rev. Esp. Cardiol. 2015, 68, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Iso, H.; Takahashi, H.; Yamagishi, K.; Tanigawa, T. Age-Period-Cohort analysis of mortality due to ischemic heart disease in Japan, 1955 to 2000. Circ. J. 2008, 72, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Gero, K.; Eshak, E.S.; Ma, E.; Takahashi, H.; Noda, H.; Iso, H. Health Disparities in Ischaemic Heart Disease Mortality in Hungary From 1970 to 2010: An Age-Period-Cohort Analysis. J. Epidemiol. 2015, 25, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, M.; Asplund, K. Age-period-cohort effects on ischaemic heart disease mortality in Sweden from 1969 to 1993, and forecasts up to 2003. Eur. Heart J. 1997, 18, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.Y.; Schooling, C.M.; Cowling, B.J.; Leung, G.M. How does socioeconomic development affect risk of mortality? An age-period-cohort analysis from a recently transitioned population in China. Am. J. Epidemiol. 2010, 171, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.A.; Park, H. Trends in ischemic heart disease mortality in Korea, 1985–2009: An age-period-cohort analysis. J. Prev. Med. Public Health 2012, 45, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Zhao, D.; Gu, D.; Coxson, P.; Chen, C.-S.; Cheng, J.; Liu, J.; He, J.; Goldman, L. The future impact of population growth and aging on coronary heart disease in China: Projections from the Coronary Heart Disease Policy Model-China. BMC Public Health 2008, 8, 394. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Gu, D.; Zhao, D.; Coxson, P.; Wang, Y.C.; Chen, C.-S.; Liu, J.; Cheng, J.; Bibbins-Domingo, K.; Shen, Y.M. Future cardiovascular disease in China: Markov model and risk factor scenario projections from the coronary heart disease policy model-China. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Critchley, J.; Liu, J.; Zhao, D.; Wei, W.; Capewell, S. Explaining the increase in coronary heart disease mortality in Beijing between 1984 and 1999. Circulation 2004, 110, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.O.; Mason, W.M.; Winsborough, H.H.; Poole, W.K. Some Methodological Issues in Cohort Analysis of Archival Data. Am. Sociol. Rev. 1973, 38, 242–258. [Google Scholar] [CrossRef]
- Smith, H.L. Advances in Age-Period-Cohort Analysis. Sociol. Method Res. 2008, 36, 287–296. [Google Scholar] [CrossRef]
- Yang, Y.; Schulhofer-Wohl, S.; Fu, W.J.; Land, K.C. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar] [CrossRef]
- Phillips, J.A. A changing epidemiology of suicide? The influence of birth cohorts on suicide rates in the United States. Soc. Sci. Med. 2014, 114, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lin, F.; Stanton, B.; Zhang, X. APC modeling of smoking prevalence among US adolescents and young adults. Am. J. Health Behav. 2011, 35, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, P.; Czarnecka, D.; Wolfshaut-Wolak, R.; Łysek, R.; Łukaszewska, A.; Surowiec, S.; Loster, M.; Bogacki, P.; Bryniarska-Mirek, E.; Grodecki, J.; et al. Age, sex, and secondary prevention of ischaemic heart disease in everyday practice. Kardiol. Pol. 2013, 71, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Population Census Office under the State Council (PCO). Tabulation on the 2000 Population Census of the People’s Republic of China; China Statistics Press: Beijing, China, 2002. [Google Scholar]
- Population Census Office under the State Council (PCO). Tabulation on the 2010 Population Census of the People’s Republic of China; China Statistics Press: Beijing, China, 2012. [Google Scholar]
- Cheng, J.; Zhao, D.; Zeng, Z.; Critchley, J.A.; Liu, J.; Wang, W.; Sun, J.; Capewell, S. The impact of demographic and risk factor changes on coronary heart disease deaths in Beijing, 1999–2010. BMC Public Health 2009, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- WHO. Database: Outdoor Air Pollution in Cities. Available online: http://www.who.int/phe/health_topics/outdoorair/databases/cities-2011/en/ (accessed on 6 December 2016).
- Fang, D.; Wang, Q.; Li, H.; Yu, Y.; Lu, Y.; Qian, X. Mortality effects assessment of ambient PM2.5 pollution in the 74 leading cities of China. Sci. Total Environ. 2016, 569–570, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Bao, J.; Yu, C.; Wang, J.; Li, C. Secular Trends of Breast Cancer in China, South Korea, Japan and the United States: Application of the Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2015, 12, 15409–15418. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yu, C.; Wang, J.; Bao, J.; Gao, X.; Xiang, H. Age-period-cohort analysis of suicide mortality by gender among white and black Americans, 1983–2012. Int. J. Equity Health 2016, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Chinese Center of Disease Control and Prevention. Global Adults Tobacco Survey (GATS) China 2010 Country Report. 2011. Available online: http://www.who.int/tobacco/surveillance/survey/gats/en_gats_china_report.pdf?ua=1 (accessed on 14 September 2016).
- Yang, G.; Wang, Y.; Wu, Y.; Yang, J.; Wan, X. The road to effective tobacco control in China. Lancet 2015, 385, 1019–1028. [Google Scholar] [CrossRef]
- Wang, J.; Bai, Z.; Wang, Z.; Yu, C. Comparison of Secular Trends in Cervical Cancer Mortality in China and the United States: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2016, 13, 1148. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.T.; Pope, C.A., 3rd; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the Global Burden of Disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ambient (Outdoor) Air Quality and Health. Fact Sheet No. 313. 2014. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/ (accessed on 15 September 2016).
- Evans, J.; van Donkelaar, A.; Martin, R.V.; Burnett, R.; Rainham, D.G.; Birkett, N.J.; Krewski, D. Estimates of global mortality attributable to particulate air pollution using satellite imagery. Environ. Res. 2013, 120, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Li, G.; Zhao, D.; Xie, X.; Wei, Z.; Wang, W.; Wang, M.; Li, G.; Liu, W.; Sun, J.; et al. Relationship between fine particulate air pollution and is chaemic heart disease morbidity and mortality. Heart 2015, 101, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Guo, Y.; Zhang, Y.; Westerdahl, D.; Mo, Y.; Liang, F.; Pan, X. Spatiotemporal analysis of particulate air pollution and ischemic heart disease mortality in Beijing, China. Environ. Health 2014, 13, 109. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zeng, Q.; Pan, X. Disease burden of ischaemic heart disease from short-term outdoor air pollution exposure in Tianjin, 2002–2006. Eur. J. Prev. Cardiol. 2016, 23, 1774–1782. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Period | Cohort | Age-Period | Age-Cohort | Period-Cohort | Age-Period-Cohort | |
|---|---|---|---|---|---|---|---|
| Urban population | |||||||
| Deviance | 19,896.83 | 2,899,129.19 | 648,370.43 | 7322.31 | 14,118.80 | 3152.12 | 1653.67 |
| AIC | 265.72 | 37,178.78 | 9349.67 | 104.64 | 192.08 | 51.30 | 32.37 |
| BIC | 19,613.65 | 2,898,816 | 648,109 | 7060.91 | 13,909.68 | 2912.50 | 1461.98 |
| DOF | 65 | 72 | 60 | 60 | 48 | 55 | 44 |
| Rural population | |||||||
| Deviance | 230,787.78 | 5,216,118.22 | 2,004,389.54 | 28,468.26 | 47,406.37 | 23,521.58 | 14,191.24 |
| AIC | 2970.23 | 66,884.54 | 25,708.84 | 376.51 | 619.62 | 313.22 | 193.88 |
| BIC | 230,504.60 | 5,215,805 | 2,004,128 | 28,206.85 | 47,197.24 | 23,281.96 | 13,999.55 |
| DOF | 65 | 72 | 60 | 60 | 48 | 55 | 44 |
| Urban Population | Rural Population | |||
|---|---|---|---|---|
| Coeff. | S.E. | Coeff. | S.E. | |
| Intercept | −7.97 * | 0.02 | −8.19 * | 0.04 |
| Age (Year) | ||||
| 20–24 | −2.92 * | 0.15 | −2.48 * | 0.27 |
| 25–29 | −2.51 * | 0.11 | −2.15 * | 0.20 |
| 30–34 | −1.82 * | 0.08 | −1.46 * | 0.15 |
| 35–39 | −1.36 * | 0.07 | −1.20 * | 0.12 |
| 40–44 | −0.72 * | 0.05 | −0.63 * | 0.10 |
| 45–49 | −0.34 * | 0.05 | −0.45 | 0.09 |
| 50–54 | 0.14 * | 0.04 | 0.08 * | 0.07 |
| 55–59 | 0.48 * | 0.03 | 0.29 * | 0.06 |
| 60–64 | 0.95 * | 0.03 | 0.70 * | 0.05 |
| 65–69 | 1.42 * | 0.02 | 1.11 * | 0.05 |
| 70–74 | 1.84 * | 0.02 | 1.62 * | 0.04 |
| 75–79 | 2.21 * | 0.02 | 2.02 * | 0.05 |
| 80–84 | 2.63 * | 0.03 | 2.56 * | 0.05 |
| Period (Year) | ||||
| 1988 | −0.54 * | 0.03 | −0.67 * | 0.06 |
| 1993 | −0.20 * | 0.02 | −0.48 * | 0.04 |
| 1998 | 0.11 * | 0.02 | −0.10 * | 0.03 |
| 2003 | −0.09 * | 0.02 | 0.17 * | 0.03 |
| 2008 | 0.19 * | 0.02 | 0.21 * | 0.03 |
| 2013 | 0.52 * | 0.02 | 0.87 * | 0.04 |
| Cohort (Year) | ||||
| 1904–1908 | 1.52 * | 0.06 | 0.99 * | 0.14 |
| 1909–1913 | 1.28 * | 0.04 | 0.89 * | 0.09 |
| 1914–1918 | 1.08 * | 0.03 | 0.75 * | 0.07 |
| 1919–1923 | 0.89 * | 0.03 | 0.71 * | 0.06 |
| 1924–1928 | 0.79 | 0.02 | 0.80 * | 0.05 |
| 1929–1933 | 0.62 * | 0.02 | 0.65 * | 0.04 |
| 1934–1938 | 0.34 * | 0.03 | 0.47 | 0.05 |
| 1939–1943 | 0.01 * | 0.03 | 0.27 | 0.06 |
| 1944–1948 | −0.18 * | 0.04 | 0.16 * | 0.07 |
| 1949–1953 | −0.26 * | 0.05 | 0.03 * | 0.08 |
| 1954–1958 | −0.40 * | 0.05 | −0.19 * | 0.10 |
| 1959–1963 | −0.45 * | 0.06 | −0.41 * | 0.11 |
| 1964–1968 | −0.60 * | 0.07 | −0.41 * | 0.12 |
| 1969–1973 | −0.64 * | 0.08 | −0.67 * | 0.14 |
| 1974–1978 | −0.91 * | 0.10 | −0.92 * | 0.18 |
| 1979–1983 | −0.97 * | 0.13 | −1.09 * | 0.26 |
| 1984–1988 | −0.98 * | 0.17 | −0.83 * | 0.31 |
| 1989–1993 | −1.15 * | 0.29 | −1.20 * | 0.51 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.; Li, B.; Li, J.; Sun, Y. The Effects of Age, Period, and Cohort on Mortality from Ischemic Heart Disease in China. Int. J. Environ. Res. Public Health 2017, 14, 50. https://doi.org/10.3390/ijerph14010050
Chang J, Li B, Li J, Sun Y. The Effects of Age, Period, and Cohort on Mortality from Ischemic Heart Disease in China. International Journal of Environmental Research and Public Health. 2017; 14(1):50. https://doi.org/10.3390/ijerph14010050
Chicago/Turabian StyleChang, Jie, Boyang Li, Jingjing Li, and Yang Sun. 2017. "The Effects of Age, Period, and Cohort on Mortality from Ischemic Heart Disease in China" International Journal of Environmental Research and Public Health 14, no. 1: 50. https://doi.org/10.3390/ijerph14010050
APA StyleChang, J., Li, B., Li, J., & Sun, Y. (2017). The Effects of Age, Period, and Cohort on Mortality from Ischemic Heart Disease in China. International Journal of Environmental Research and Public Health, 14(1), 50. https://doi.org/10.3390/ijerph14010050