Identification of Genetic Interaction with Risk Factors Using a Time-To-Event Model


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Genotyping
2.2. Statistical Methods
2.3. Complementary Approaches to Validate the Results
2.4. Whole Blood Gene Expression
3. Results
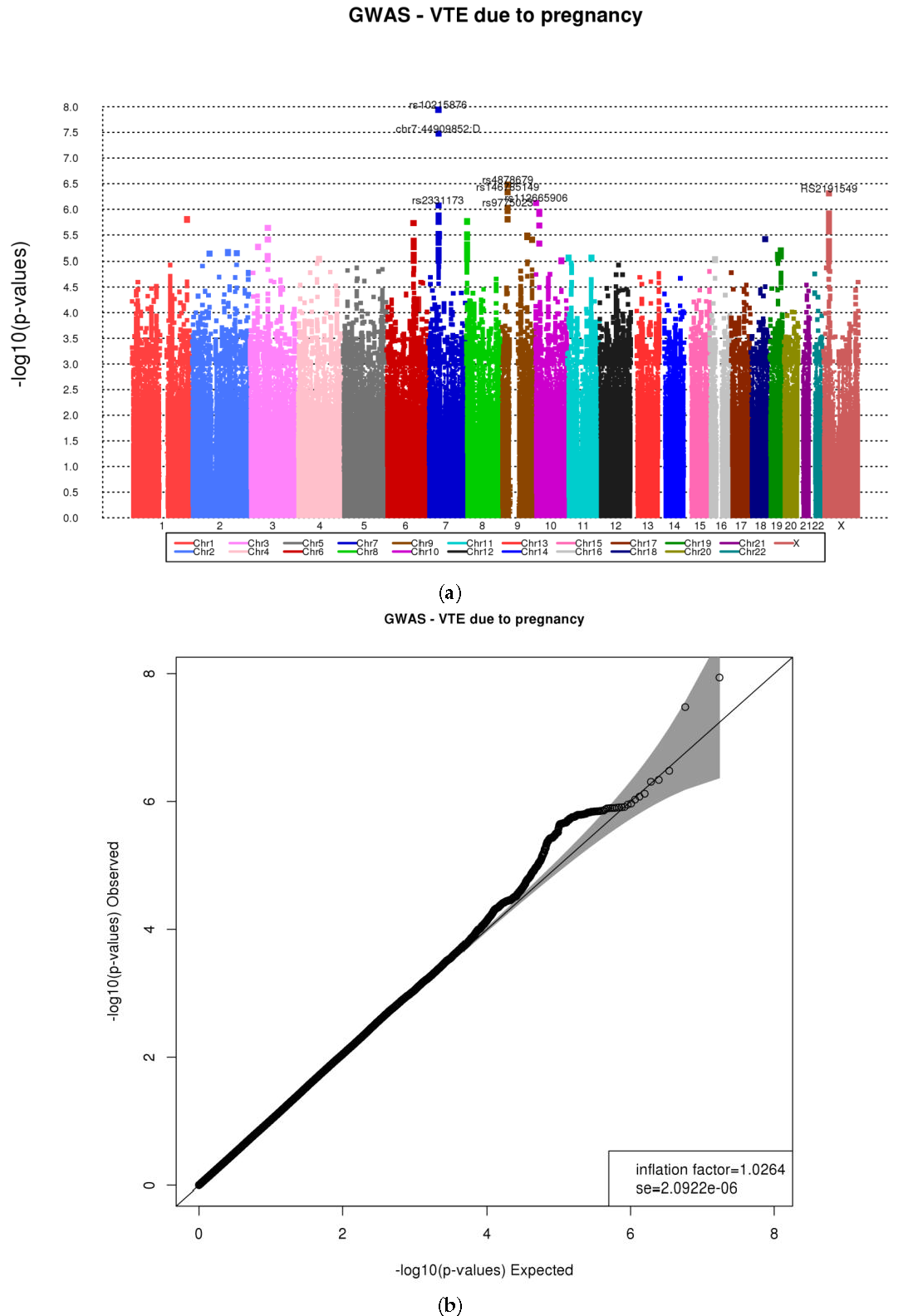
3.1. Genome-Wide Association Using CoxPH Model and 1000G Imputed Data
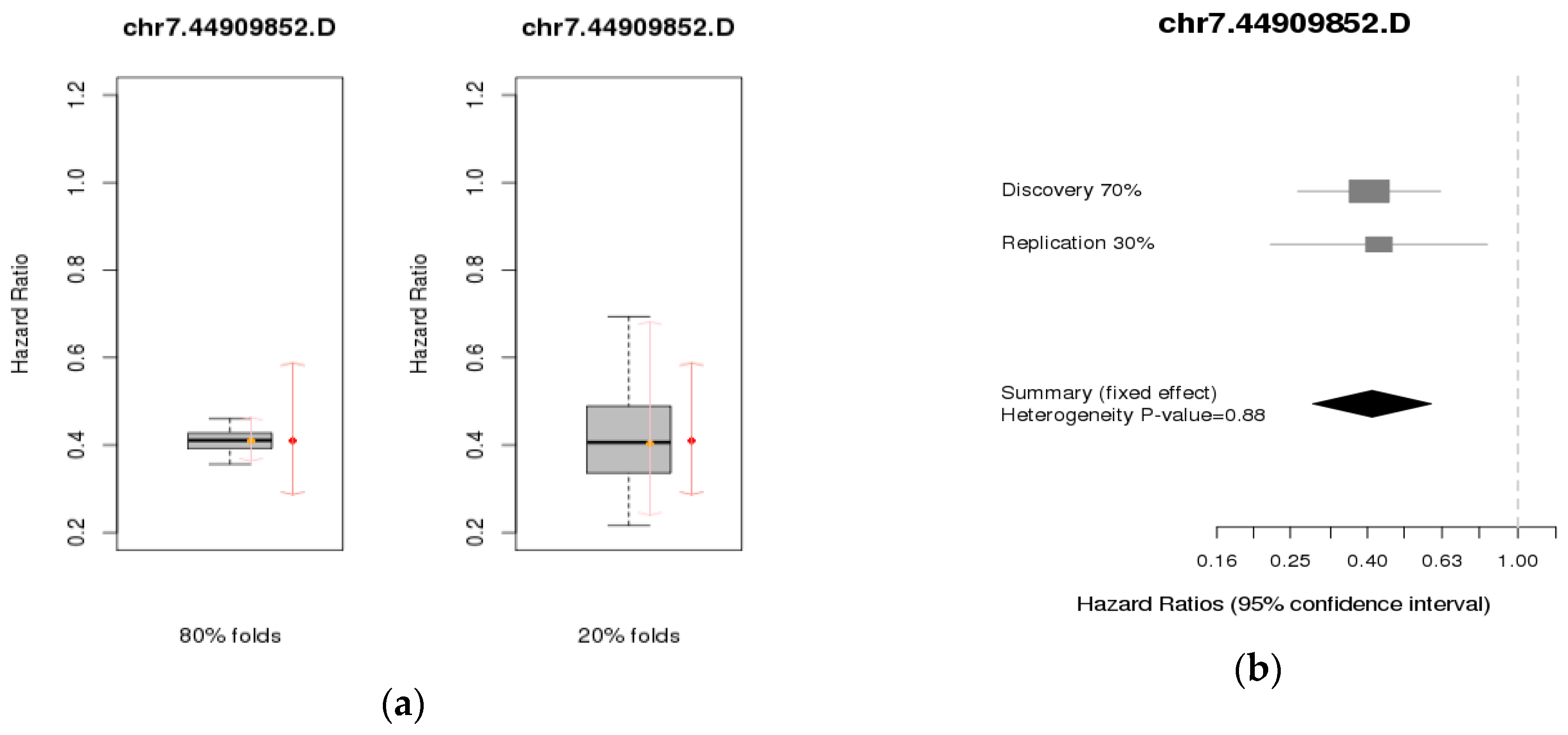
3.2. Validation Studies
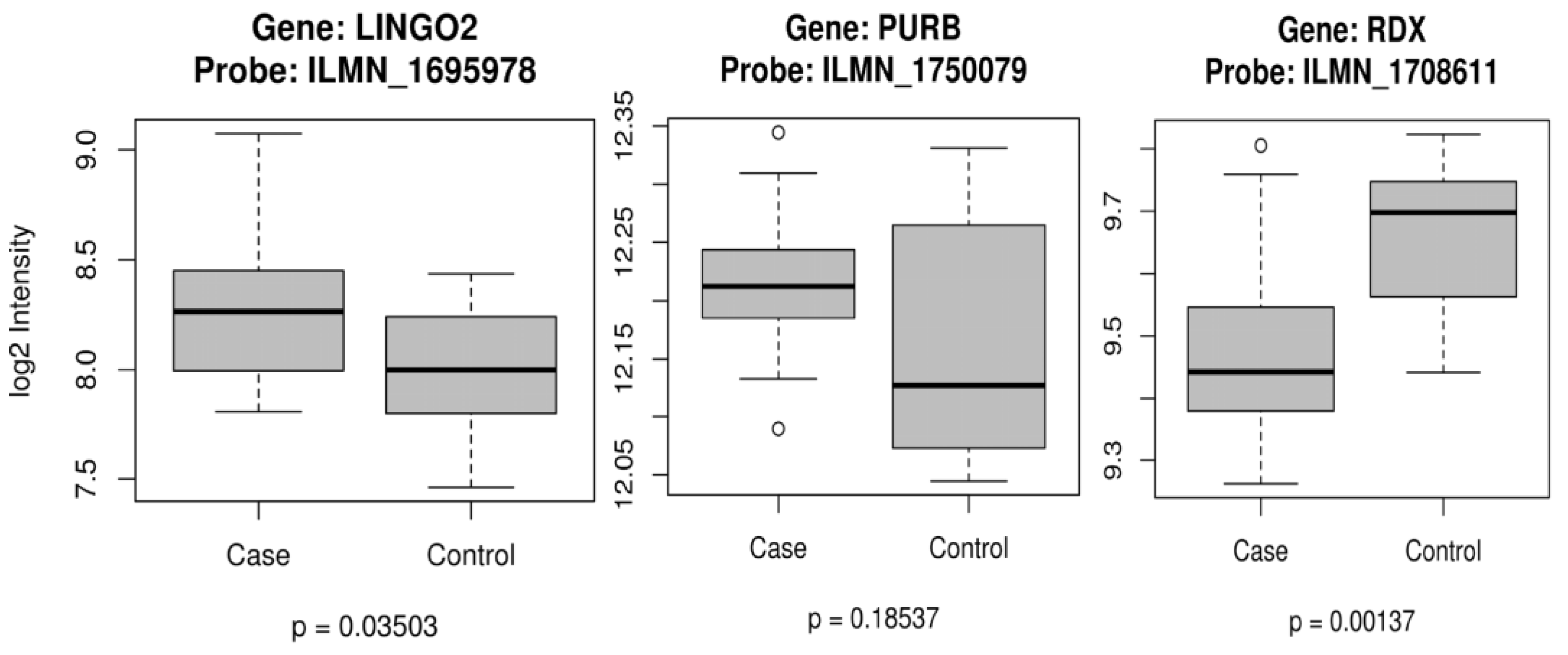
3.3. Gene Expression
3.5. Cox Proportional Hazards Model
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Heit, J.A. Epidemiology of venous thromboembolism. Nat. Rev. Cardiol. 2015, 12, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Snow, V.; Qaseem, A.; Barry, P.; Hornbake, E.R.; Rodnick, J.E.; Tobolic, T.; Ireland, B.; Segal, J.B.; Bass, E.B.; Weiss, K.B.; et al. Management of venous thromboembolism: A clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann. Intern. Med. 2007, 146, 204–210. [Google Scholar] [CrossRef] [PubMed]
- The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. Available online: https://www.ncbi.nlm.nih.gov/pubmed/20669525 (accessed on 11 October 2017).
- Cushman, M.; Creager, M.A. Improving Awareness and Outcomes Related to Venous Thromboembolism. JAMA 2015, 314, 1913–1914. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Kobbervig, C.E.; James, A.H.; Petterson, T.M.; Bailey, K.R.; Melton, L.J., 3rd. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: A 30-year population-based study. Ann. Intern. Med. 2005, 143, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Phelps, M.A.; Ward, S.A.; Slusser, J.P.; Petterson, T.M.; De Andrade, M. Familial segregation of venous thromboembolism. J. Thromb. Haemost. 2004, 2, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Ariens, R.A.; de Lange, M.; Snieder, H.; Boothby, M.; Spector, T.D.; Grant, P.J. Activation markers of coagulation and fibrinolysis in twins: Heritability of the prethrombotic state. Lancet. 2002, 359, 667–671. [Google Scholar] [CrossRef]
- Zoller, B.; Ohlsson, H.; Sundquist, J.; Sundquist, K. Familial risk of venous thromboembolism in first-, second- and third-degree relatives: A nationwide family study in Sweden. Thromb. Haemost. 2013, 109, 458–463. [Google Scholar] [CrossRef] [PubMed]
- James, A.H.; Jamison, M.G.; Brancazio, L.R.; Myers, E.R. Venous thromboembolism during pregnancy and the postpartum period: Incidence, risk factors, and mortality. Am. J. Obstet. Gynecol. 2006, 194, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A. The epidemiology of venous thromboembolism in the community: Implications for prevention and management. J. Thromb. Thrombolysis. 2006, 21, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Zotz, R.B.; Gerhardt, A.; Scharf, R.E. Prediction, prevention, and treatment of venous thromboembolic disease in pregnancy. Semin. Thromb. Hemost. 2003, 29, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Sultan, A.A.; Tata, L.J.; West, J.; Fiaschi, L.; Fleming, K.M.; Nelson-Piercy, C.; Grainge, M.J. Risk factors for first venous thromboembolism around pregnancy: A population-based cohort study from the United Kingdom. Blood 2013, 121, 3953–3961. [Google Scholar] [CrossRef] [PubMed]
- Abdul Sultan, A.; Grainge, M.J.; West, J.; Fleming, K.M.; Nelson-Piercy, C.; Tata, L.J. Impact of risk factors on the timing of first postpartum venous thromboembolism: A population-based cohort study from England. Blood 2014, 124, 2827–2880. [Google Scholar] [CrossRef]
- Silverstein, M.D.; Heit, J.A.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J., 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: A 25-year population-based study. Arch. Intern. Med. 1998, 158, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Melton, L.J., 3rd.; Lohse, C.M.; Petterson, T.M.; Silverstein, M.D.; Mohr, D.N.; O’Fallon, W.M. Incidence of venous thromboembolism in hospitalized patients vs community residents. Mayo Clin. Proc. 2001, 76, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Rosendaal, F.R. Venous thrombosis: The role of genes, environment, and behavior. Hematology Am. Soc. Hematol. Educ. Program. 2005. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.F.; Austin, H.; Dilley, A.; Whitsett, C.; Evatt, B.L.; Hooper, W.C. The epidemiology of venous thromboembolism in Caucasians and African-Americans: The GATE Study1. J. Thromb. Haemost. 2003, 1, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Cunningham, J.M.; Petterson, T.M.; Armasu, S.M.; Rider, D.N.; DE Andrade, M. Genetic variation within the anticoagulant, procoagulant, fibrinolytic and innate immunity pathways as risk factors for venous thromboembolism. J. Thromb. Haemost. 2011, 9, 1133–1142. [Google Scholar] [CrossRef]
- Heit, J.A. The epidemiology of venous thromboembolism in the community. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Armasu, S.M.; Asmann, Y.W.; Cunningham, J.M.; Matsumoto, M.E.; Petterson, T.M.; De Andrade, M. A genome-wide association study of venous thromboembolism identifies risk variants in chromosomes 1q24.2 and 9q. J. Thromb. Haemost. 2012, 10, 1521–1531. [Google Scholar] [CrossRef]
- Howie, B.; Marchini, J.; Stephens, M. Genotype imputation with thousands of genomes. G3 (Bethesda) 2011, 1, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Delaneau, O.; Zagury, J.F.; Marchini, J. Improved whole-chromosome phasing for disease and population genetic studies. Nat. Methods. 2013, 10, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Electronic Medical Records and Genomics (eMERGE) Network. Available online: https://www.genome.gov/27540473/electronic-medical-records-and-genomics-emerge-network/ (accessed on 11 October 2017).
- Dresang, L.T.; Fontaine, P.; Leeman, L.; King, V.J. Venous thromboembolism during pregnancy. Am. Fam. Physician. 2008, 77, 1709–1716. [Google Scholar] [PubMed]
- James, A.H. Venous thromboembolism in pregnancy. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Spinger-Verlag: New York, NY, USA, 2000. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference and Prediction; Spinger-Verlag: New York, NY, USA, 2009. [Google Scholar]
- Lumley, T. R Meta: Meta-Analysis, R Package Version 2.16, 2012. Available online: https://CRAN.R-project.org/package=rmeta (accessed on 9 October 2017).
- R: A Language and Environment for Statistical Computing; Version 2.15; R Foundation for Statistical Computing: Vienna, Austria, 2013.
- Lewis, D.A.; Suchindran, S.; Beckman, M.G.; Hooper, W.C.; Grant, A.M.; Heit, J.A.; Manco-Johnson, M.; Moll, S.; Philipp, C.S.; Kenney, K.; et al. Whole blood gene expression profiles distinguish clinical phenotypes of venous thromboembolism. Thromb. Res. 2015, 135, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Armasu, S.M.; McCauley, B.M.; Kullo, I.J.; Sicotte, H.; Pathak, J.; Chute, C.G.; Gottesman, O.; Bottinger, E.P.; Denny, J.C.; et al. Identification of unique venous thromboembolism-susceptibility variants in African-Americans. Thromb. Haemost. 2017, 117, 758–768. [Google Scholar] [CrossRef]
- Higashi, M.K.; Veenstra, D.L.; Kondo, L.M.; Wittkowsky, A.K.; Srinouanprachanh, S.L.; Farin, F.M.; Rettie, A.E. Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA 2002, 287, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Renoux, C.; Dell’Aniello, S.; Brenner, B.; Suissa, S. Bias from depletion of susceptibles: The example of hormone replacement therapy and the risk of venous thromboembolism. Pharmacoepidemiol. Drug Saf. 2017, 26, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, A.; Westhoff, C. Hormone replacement therapy and venous thromboembolism. J. Steroid Biochem. Mol. Biol. 2014, 142, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Vinogradova, Y.; Coupland, C.; Hippisley-Cox, J. Use of combined oral contraceptives and risk of venous thromboembolism: Nested case-control studies using the QResearch and CPRD databases. BMJ. 2015, 350. [Google Scholar] [CrossRef] [PubMed]
- dbSNP Short Genetic Variations. Available online: http://www.ncbi.nlm.nih.gov/projects/SNP/ (accessed on 9 October 2017).
- Kraft, P.; Yen, Y.C.; Stram, D.O.; Morrison, J.; Gauderman, W.J. Exploiting gene-environment interaction to detect genetic associations. Hum. Hered. 2007, 63, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Armasu, S.M.; Matsumoto, M.E.; Petterson, T.M.; Rider, D.N.; Cunningham, J.M.; Asmann, Y.W.; de Andrade, M. Association of Gene-Environment Interactions with Venous Thromboembolism (VTE): A Merged/Imputed Genome-Wide Scan/Candidate-Gene Case-Control Study. Blood 2011, 118, 2295. [Google Scholar]
- De Vivo, I.; Prescott, J.; Setiawan, V.W.; Olson, S.H.; Wentzensen, N.; Attia, J.; Black, A.; Brinton, L.; Chen, C.; Cook, L.S. Genome-Wide association study of endometrial cancer in E2C2. Human Genet. 2014, 133, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.P.; Grondin, C.J.; Johnson, R.J.; Sciaky, D.; King, B.L.; McMorran, R.; Wiegers, J.; Wiegers, T.C.; Mattingly, C.J. The Comparative Toxicogenomics Database: Update 2017. Nucleic Acids Res. 2017, 45, D972–D978. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| (a) | |||
| Risk Factors | N = 633 | HR * (95% CI) | p-Value |
| Pregnancy | |||
| Median (Q1, Q3) | 0 (0, 2) | 3.30 (2.24, 4.88) | 1.85 × 10−9 |
| Oral Contraceptive § | |||
| Yes ( N, %) | 103, 16.3% | 9.68 (7.48, 12.52) | <2 × 10−16 |
| No ( N, %) | 530, 83.7% | REF | |
| Hormone Replacement Therapy § | |||
| Yes | 14, 2.12% | 3.17 (1.84, 5.46) | 3.38 × 10−5 |
| No | 619, 97.8% | REF | |
| Family History of VTE | |||
| Yes | 216, 33.5% | (0.78, 1.29) | 0.983 |
| No | 373, 58.9% | REF | |
| Missing | 44, 6.95% | ||
| (b) | |||
| Variables | VTE during Pregnancy (N = 30) | VTE not during Pregnancy (N = 75) | VTE and Never Pregnant (N = 172) |
| Age at enrollment, years (SD) | 40.80 (16.24) | 40.32 (9.90) | 36.25 (11.46) |
| Age at VTE, years (SD) | 27.67 (6.20) | 34.91 (6.70) | 30.77 (9.01) |
| Stroke/MI, N (%) | 2 (6.67) | 5 (6.67) | 19 (11.05) |
| Minnesota resident, N (%) | 14 (46.67) | 30 (40.00) | 70 (40.70) |
| Non-Minnesota resident, N (%) | 16 (53.33) | 45 (60.00) | 102 (59.30) |
| Variables | VTE during Pregnancy 1 (N = 18) | VTE during Pregnancy 2 (N = 7) | VTE during Pregnancy 3+ (N = 5) | VTE not during Pregnancy (N = 75) | VTE and Never Pregnant (N = 172) |
|---|---|---|---|---|---|
| Age at enrollment, years (SD) | 39.11 (16.89) | 44.00 (18.82) | 42.40 (11.55) | 40.32 (9.90) | 36.25 (11.46) |
| Age at VTE, years (SD) | 25.08 (5.23) | 29.08 (4.71) | 35.02 (5.30) | 34.91 (6.70) | 30.77 (9.01 |
| Stroke/MI, N (%) | 1 (5.56) | 1 (14.29) | 0 (0.00) | 5 (6.67) | 19 (11.05) |
| Minnesota resident, N (%) | 8 (44.44) | 3 (42.86) | 3 (60.00) | 30 (40.00) | 70 (40.70) |
| Non-Minnesota resident, N (%) | 10 (55.56) | 4 (57.14) | 2 (40.00) | 45 (60.00) | 102 (59.30) |
| Caption | Characteristic | Hazard Ratio (95% Confidence Interval) | Standard Error | p-Value |
|---|---|---|---|---|
| Multivariable model (null) | Pregnancy | 3.19 (2.16, 4.71) | 0.20 | 3.56 × 10−7 |
| Stroke/MI | 0.49 (0.33, 0.74) | 0.21 | 1.65 × 10−4 | |
| Minnesota resident | 0.84 (0.66, 1.07) | 0.12 | 0.162096 | |
| Multivariable model Chr7:rs10215876 | Pregnancy | 3.21 (2.17, 4.74) | 0.20 | 3.16 × 10−7 |
| Stroke/MI | 0.47 (0.32, 0.71) | 0.21 | 6.41 × 10−5 | |
| Minnesota resident | 0.83 (0.65, 1.06) | 0.12 | 0.130 | |
| Chr7: rs10215876 | 0.40 (0.28, 0.58) | 0.18 | 1.15 × 10−8 | |
| Multivariable model Chr7:44909852.D | Pregnancy | 3.23 (2.18, 4.77) | 0.20 | 2.78 × 10−7 |
| Stroke/MI | 0.47 (0.32, 0.71) | 0.21 | 6.45 × 10−5 | |
| Minnesota resident | 0.83 (0.66, 1.06) | 0.12 | 0.134 | |
| Chr7.44909852.D | 0.41 (0.29, 0.58) | 0.18 | 3.34 × 10−8 | |
| Multivariable model Chr9:rs4878679 | Pregnancy | 3.11 (2.10, 4.59) | 0.20 | 5.85 × 10−7 |
| Stroke/MI | 0.48 (0.32, 0.72) | 0.21 | 8.19 × 10−5 | |
| Minnesota resident | 0.80 (0.63, 1.02) | 0.12 | 0.0709 | |
| Chr9:rs4878679 | 0.63 (0.52, 0.75) | 0.09 | 3.31 × 10−7 | |
| Multivariable model ChrX:rs2191549 | Pregnancy | 3.26 (2.21, 4.82) | 0.20 | 2.24 × 10−7 |
| Stroke/MI | 0.49 (0.33,0.74) | 0.21 | 1.81 × 10−4 | |
| Minnesota resident | 0.83 (0.65,1.05) | 0.12 | 0.150 | |
| ChrX: rs2191549 | 0.52 (0.40, 0.69) | 0.14 | 4.92 × 10−7 |
| SNP | CHR | HR | 95% CI | Heter_Pvalue | Meta_Pvalue |
|---|---|---|---|---|---|
| rs10215876 | 7 | 0.410 | (0.288, 0.584) | 0.615 | 7.49 × 10−7 |
| chr7.44909852.D | 7 | 0.412 | (0.287, 0.590) | 0.883 | 1.41 × 10−6 |
| rs4878679 | 9 | 0.628 | (0.522, 0.754) | 0.587 | 6.49 × 10−7 |
| rs2191549 | 23 | 0.516 | (0.392, 0.679) | 0.983 | 2.29 × 10−6 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Andrade, M.; Armasu, S.M.; McCauley, B.M.; Petterson, T.M.; Heit, J.A. Identification of Genetic Interaction with Risk Factors Using a Time-To-Event Model. Int. J. Environ. Res. Public Health 2017, 14, 1228. https://doi.org/10.3390/ijerph14101228
De Andrade M, Armasu SM, McCauley BM, Petterson TM, Heit JA. Identification of Genetic Interaction with Risk Factors Using a Time-To-Event Model. International Journal of Environmental Research and Public Health. 2017; 14(10):1228. https://doi.org/10.3390/ijerph14101228
Chicago/Turabian StyleDe Andrade, Mariza, Sebastian M. Armasu, Bryan M. McCauley, Tanya M. Petterson, and John A. Heit. 2017. "Identification of Genetic Interaction with Risk Factors Using a Time-To-Event Model" International Journal of Environmental Research and Public Health 14, no. 10: 1228. https://doi.org/10.3390/ijerph14101228
APA StyleDe Andrade, M., Armasu, S. M., McCauley, B. M., Petterson, T. M., & Heit, J. A. (2017). Identification of Genetic Interaction with Risk Factors Using a Time-To-Event Model. International Journal of Environmental Research and Public Health, 14(10), 1228. https://doi.org/10.3390/ijerph14101228