The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Fukushima Health Management Survey
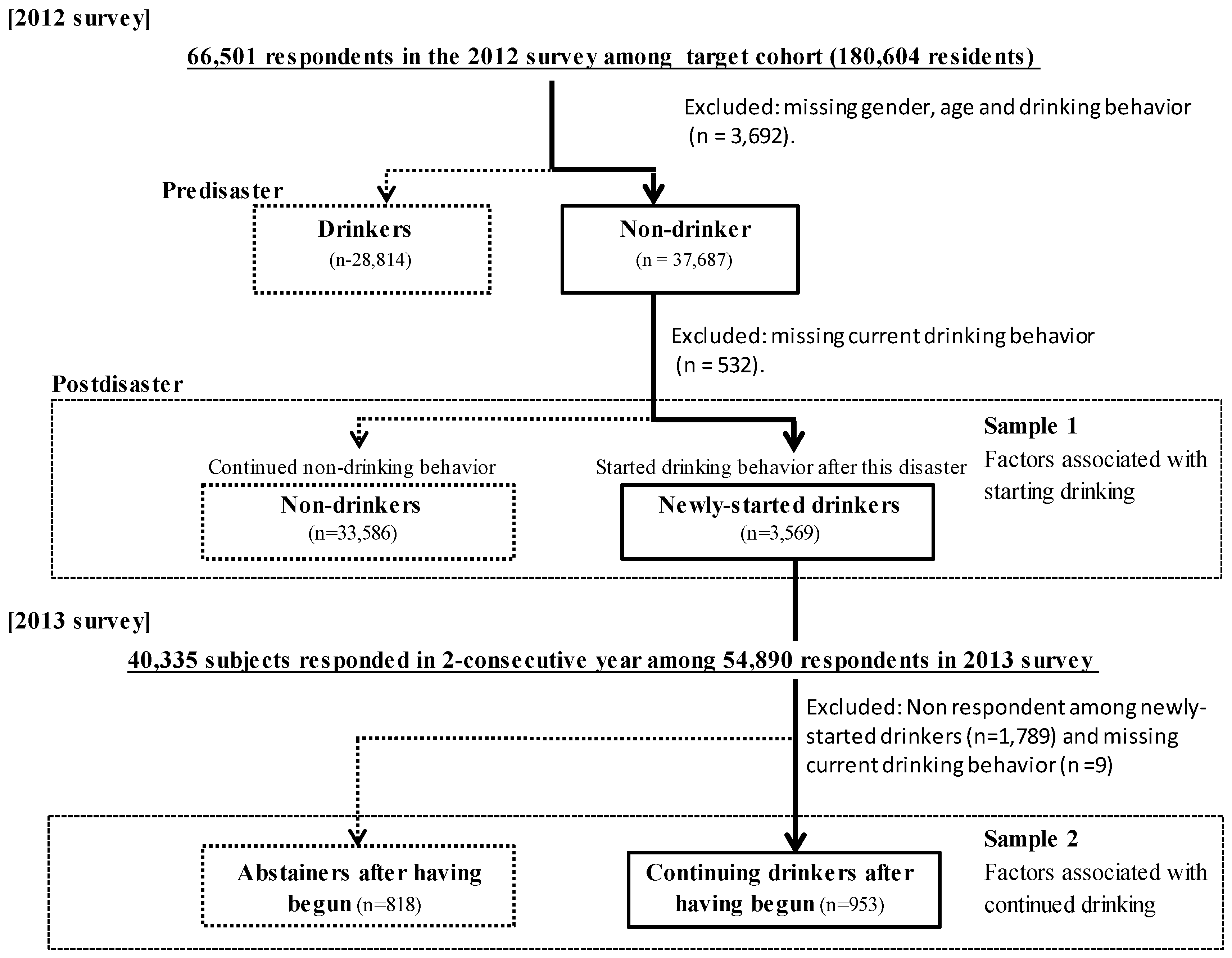
2.2. Participants
2.3. Classification of Drinking Behavioral Pattern
2.4. Measurements
2.4.1. Current Physical/Mental Health Status
2.4.2. Disaster-Related Experience
2.4.3. Effects of the Disaster on Socioeconomic Status
2.4.4. Perceived Risk of Radiation Exposure
2.5. Statistical Analysis
3. Results
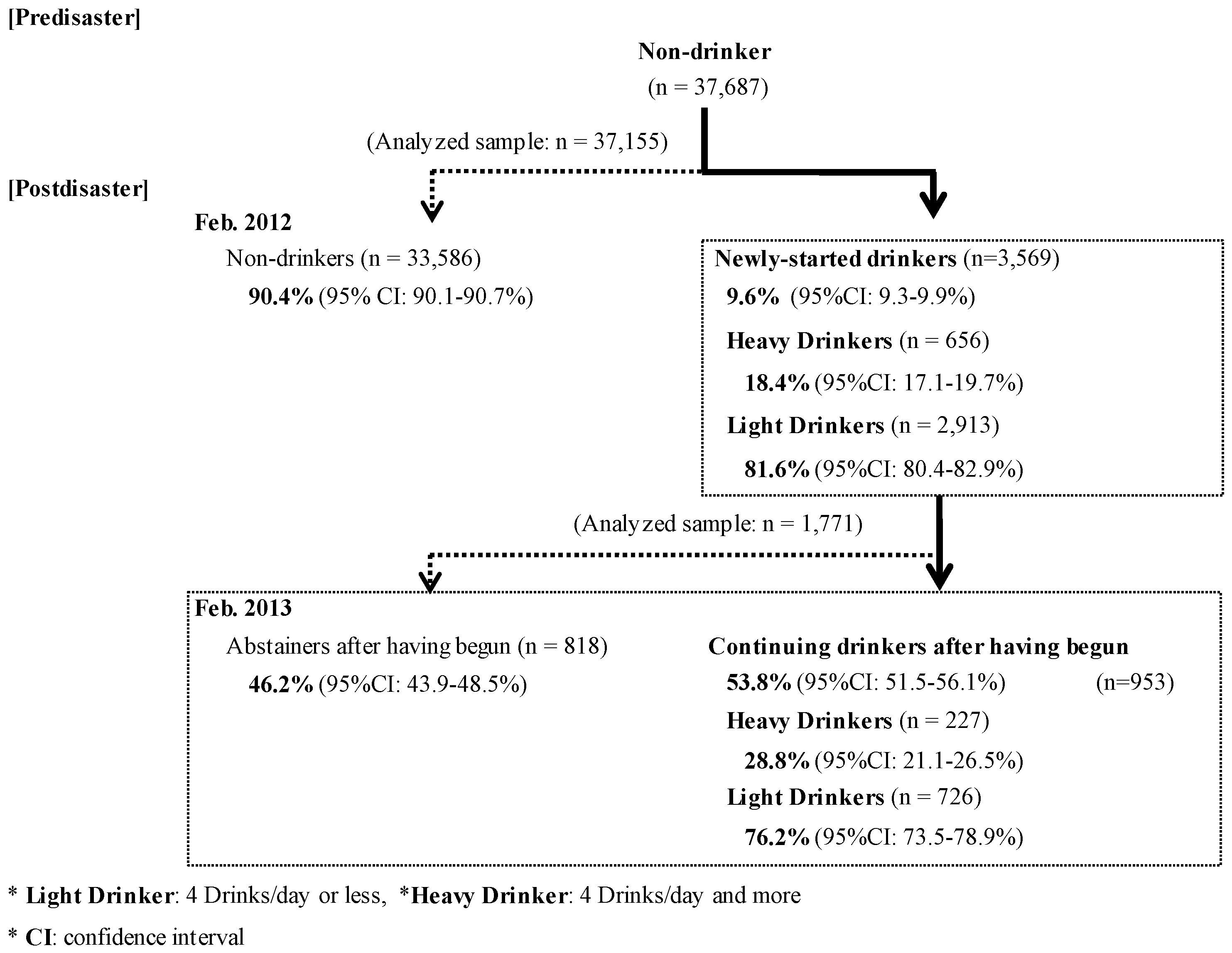
3.1. The Prevalence of Newly-Started Drinking Behavior and Continued Drinking after the Disaster
3.2. Factors Related to Newly-Started Drinking Behavior
3.3. Factors Related to Continued Drinking among Newly-Started Drinkers
4. Discussion
4.1. Factors Related to Newly-Started Drinking Behavior and Continued Drinking among Newly-Started Drinkers
4.2. Limitations and Strengths
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cabinet Office. White Paper on Disaster Management; Government of Japan: Tokyo, Japan, 2001.
- Fukushima Prefectural Govt., Japan. Fukushima Revitalization Station. Available online: http://www.pref.fukushima.lg.jp/site/portal-english/ (accessed on 6 October 2017).
- Wu, H.C.; Chou, F.H.; Su, C.Y.; Tsai, K.Y.; Ou-Yang, W.C.; Su, T.T. Survey of quality of life and related risk factors for a Taiwanese village population 3 years post-earthquake. Aust. N. Z. J. Psychiatry 2006, 40, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Tsutsumi, A.; Fukasawa, M.; Honma, H.; Someya, T.; Kim, Y. Prevalence of Mental Disorders and Suicidal Thoughts among Community-Dwelling Elderly Adults 3 Years after the Niigata-Chuetsu Earthquake. J. Epidemiol. 2011, 21, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. Great East Japan earthquake and early mental-health-care response. Psychiatry Clin. Neurosci. 2011, 65, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M. Mental health care and East Japan Great Earthquake. Psychiatry Clin. Neurosci. 2011, 65, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.E.; Boscarino, J.A.; Galea, S. Alcohol use, mental health status and psychological well-being 2 years after the World Trade Center attacks in New York City. Am. J. Drug Alcohol Abuse 2006, 32, 203–224. [Google Scholar] [CrossRef] [PubMed]
- Nordløkken, A.; Pape, H.; Wentzel-Larsen, T.; Heir, T. Changes in alcohol consumption after a natural disaster: A study of Norwegian survivors after the 2004 Southeast Asia tsunami. BMC Public Health 2013, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Hatzenbuehler, M.L.; Hasin, D.S. Stressful life experiences, alcohol consumption, and alcohol use disorders: The epidemiologic evidence for four main types of stressors. Psychopharmacology 2011, 218, 1–17. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C. Epidemiological evidence about the relationship between PTSD and alcohol abuse: The nature of the association. Addict. Behav. 1998, 23, 813–825. [Google Scholar] [CrossRef]
- Lowe, S.R.; Sampson, L.; Young, M.N.; Galea, S. Alcohol and Nonmedical Prescription Drug Use to Cope With Posttraumatic Stress Disorder Symptoms: An Analysis of Hurricane Sandy Survivors. Subst. Use Misuse 2017, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Brower, K.J.; Aldrich, M.S.; Robinson, E.A.; Zucker, R.A.; Greden, J.F. Insomnia, self-medication, and relapse to alcoholism. Am. J. Psychiatry 2001, 158, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Bolton, J.M.; Robinson, J.; Sareen, J. Self-medication of mood disorders with alcohol and drugs in the National Epidemiologic Survey on Alcohol and Related Conditions. J. Affect. Disord. 2009, 115, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Kaneita, Y.; Uchiyama, M.; Takemura, S.; Yokoyama, E.; Miyake, T.; Harano, S. Use of alcohol and hypnotic medication as aids to sleep among the Japanese general population. Sleep Med. 2007, 8, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Sandlund, C.; Westman, J.; Hetta, J. Factors associated with self-reported need for treatment of sleeping difficulties: A survey of the general Swedish population. Sleep Med. 2016, 22, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Yabe, H.; Maeda, M.; Ohira, T.; Fujii, S.; Niwa, S. Drinking Behavior and Mental Illness among Evacuees in Fukushima Following the Great East Japan Earthquake: The Fukushima HealthManagement Survey. Alcohol. Clin. Exp. Res. 2016, 40, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; Ritson, E.B.; Hodgson, R.J. Alcohol-related problems in the primary health care setting: A review of early intervention strategies. Br. J. Addict. 1986, 81, 23–46. [Google Scholar] [CrossRef] [PubMed]
- Moyer, A.; Finney, J.W.; Swearingen, C.E.; Vergun, P. Brief interventions for alcohol problems: A meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction 2002, 97, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; McRee, B.G.; Kassebaum, P.A.; Grimaldi, P.L.; Ahmed, K.; Bray, J. Screening, Brief Intervention, and Referral to Treatment (SBIRT): Toward a public health approach to the management of substance abuse. Subst. Abuse 2007, 28, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Shinfuku, N. Disaster mental health: Lessons learned from the Hanshin Awaji earthquake. World Psychiatry 2002, 1, 158–159. [Google Scholar] [PubMed]
- Orui, M.; Harada, S.; Hayashi, M. A practical report on long-term disaster mental health services following the Great East Japan Earthquake: The psychological and social background of evacuees in Sendai City in the mid- to long-term post-disaster period. Disaster Med. Public Health Prep. 2017, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M. Study Protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatry Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tanno, K. Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS ONE 2014, 9, e102497. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Yabe, H.; Horikoshi, N.; Yasumura, S.; Kawakami, N.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Mental Health Group of the Fukushima Health Management Survey. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia Pac. Psychiatry 2016, 9. [Google Scholar] [CrossRef]
- North, C.S.; Ringwalt, C.L.; Downs, D. Postdisaster course of alcohol use disorders in systematically studied survivors of 10 disasters. Arch. Gen. Psychiatry 2011, 68, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Gallo, W.T.; Bradley, E.H.; Siegel, M.; Kasl, S.V. The impact of involuntary job loss on subsequent alcohol consumption by older workers: Findings from the health and retirement survey. J. Gerontol. 2001, 56, S3–S9. [Google Scholar] [CrossRef]
- Crowe, L.; Butterworth, P. The role of financial hardship, mastery and social support in the association between employment status and depression: Results from an Australian longitudinal cohort study. BMJ Open 2016, 6, e009834. [Google Scholar] [CrossRef] [PubMed]
- TEPCO: About Compensation for Nuclear Damages. Available online: http://www.tepco.co.jp/en/comp/index-e.html (accessed on 6 October 2017).
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.; Ohtsuru, A. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull. World Health Organ. 2015, 93, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Kaerlev, L.; Kolstad, H.A.; Hansen, A.M.; Thomsen, J.F.; Kærgaard, A.; Rugulies, R.; Mikkelsen, S.; Andersen, J.H.; Mors, O.; Grynderup, M.B.; et al. Are risk estimates biased in follow-up studies of psychosocial factors with low base-line participation? BMC Public Health 2011, 11, 539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercambre, M.N.; Gilbert, F. Respondents in an epidemiologic survey had fewer psychotropic prescriptions than nonrespondents: An insight into health-related selection bias using routine health insurance data. J. Clin. Epidemiol. 2012, 65, 1181–1189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pre-Disaster | p Value (χ2) | ||||
|---|---|---|---|---|---|
| Drinkers | Non-Drinkers | ||||
| (n = 28,814) | (n = 37,687) | ||||
| n | (%) | n | (%) | ||
| Gender | |||||
| Male | 19,063 | (66.2) | 10,567 | (28.0) | <0.01 (χ2 = 9605.3) |
| Female | 9751 | (33.8) | 27,120 | (72.0) | |
| Age (as of 11 March 2011) | |||||
| 20–39 years | 6755 | (23.5) | 7766 | (20.8) | |
| 40–64 years | 14,342 | (49.9) | 14,642 | (39.2) | <0.01 (χ2 = 1329.9) |
| 65 years and older | 7628 | (26.6) | 14,907 | (39.9) | |
| Education | |||||
| Junior/Senior high school | 20,098 | (71.9) | 27,645 | (76.7) | <0.01 (χ2 = 190.6) |
| Vocational college, University, Graduated school | 7865 | (28.1) | 8415 | (23.3) | |
| Total | p Value (χ2) | Newly-Started Drinkers | p Value (χ2) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newly-Started Drinkers | Continuing Non-Drinkers | Heavy Drinkers | Light Drinkers | ||||||||
| (n = 3569) | (n = 33,593) | (n = 656) | (n = 2913) | ||||||||
| n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Gender | |||||||||||
| Male | 1506 | (42.2) | 8978 | (26.7) | <0.01 (χ2 = 381.0) | 375 | (57.2) | 1131 | (38.8) | <0.01 (χ2 = 73.8) | |
| Female | 2063 | (57.8) | 24,608 | (73.3) | 281 | (42.8) | 1782 | (61.2) | |||
| Age (as of 11 March 2011) | |||||||||||
| 20–39 years old | 1092 | (31.7) | 6667 | (20.0) | 304 | (27.8) | 788 | (27.9) | |||
| 40–64 years old | 1397 | (40.5) | 13,116 | (39.3) | <0.01 (χ2 = 332.7) | 251 | (23.0) | 1146 | (40.6) | <0.01 (χ2 = 145.4) | |
| 65 years old and older | 960 | (27.8) | 13,553 | (40.7) | 70 | (6.4) | 890 | (31.5) | |||
| Education | |||||||||||
| Junior/Senior high school | 2433 | (70.5) | 24,819 | (77.2) | <0.01 (χ2 = 78.3) | 410 | (64.5) | 2023 | (71.8) | <0.01 (χ2 = 13.5) | |
| Vocational college, University, Graduated school | 1020 | (29.5) | 7339 | (22.8) | 226 | (35.5) | 794 | (28.2) | |||
| General subjective health status | |||||||||||
| Poor | 691 | (19.8) | 7138 | (21.8) | 0.01 (χ2 = 7.42) | 450 | (78.5) | 1650 | (71.2) | <0.01 (χ2 = 12.4) | |
| Good/Unremarkable | 2803 | (80.2) | 25,650 | (78.2) | 123 | (21.5) | 667 | (28.8) | |||
| Sleep disturbance | |||||||||||
| Unsatisfied with sleep condition | Yes | 2100 | (72.7) | 17,965 | (66.5) | <0.01 (χ2 = 45.0) | 450 | (78.5) | 1650 | (71.2) | <0.01 (χ2 = 12.4) |
| No | 790 | (27.3) | 9051 | (33.5) | 123 | (21.5) | 667 | (28.8) | |||
| Psychological distress | |||||||||||
| K6 (13 points and more) | 13≤ | 670 | (20.3) | 4942 | (15.8) | <0.01 (χ2 = 43.4) | 178 | (28.2) | 492 | (18.4) | <0.01 (χ2 = 30.1) |
| ≤12 | 2634 | (79.7) | 26,273 | (84.2) | 454 | (71.8) | 2180 | (81.6) | |||
| Disaster-related experience | |||||||||||
| Experience of tsunami | Yes | 771 | (21.6) | 6179 | (18.4) | <0.01 (χ2 = 21.8) | 149 | (22.7) | 622 | (21.4) | 0.44 (χ2 = 0.59) |
| No | 2798 | (78.4) | 27,407 | (81.6) | 507 | (77.3) | 2291 | (78.6) | |||
| Experience of nuclear power plant accident | Yes | 1969 | (55.2) | 17,267 | (51.4) | <0.01 (χ2 = 18.3) | 394 | (60.1) | 1575 | (54.1) | 0.01 (χ2 = 7.78) |
| No | 1600 | (44.8) | 16,319 | (48.6) | 262 | (39.9) | 1338 | (45.9) | |||
| Disaster effects on economic status | |||||||||||
| Loss of employment due to disaster | Yes | 823 | (23.1) | 6420 | (19.1) | <0.01 (χ2 = 32.0) | 158 | (24.1) | 665 | (22.8) | 0.49 (χ2 = 0.48) |
| No | 2746 | (76.9) | 27,166 | (80.9) | 498 | (75.9) | 2248 | (77.2) | |||
| No | 11,018 | (91.6) | 1012 | (8.4) | 833 | (82.3) | 179 | (17.7) | |||
| Perception of radiation risks | |||||||||||
| Delayed effects | Low | 2781 | (82.6) | 26,498 | (85.1) | 512 | (80.1) | 2269 | (83.2) | ||
| High | 1811 | (53.7) | 14,925 | (47.8) | <0.01 (χ2 = 43.5) | 376 | (58.7) | 1435 | (52.6) | 0.01 (χ2 = 6.53) | |
| Model 1 | Model 2 | Model 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Newly-Started Drinkers vs. Continued Non-Drinking in 2012 Survey | Newly-Started Drinkers | |||||||||
| Adjusted by Current Physical/Mental Health Status | Adjusted by Disaster-Related Experience, Disaster Effects on Economic Status and Perception of Radiation Risk | Heavy vs. Light Drinkers | ||||||||
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |||||
| Gender | ||||||||||
| Male | 1.99 | (1.83–2.17) | <0.01 | 1.95 | (1.78–2.13) | <0.01 | 2.56 | (2.07–3.16) | <0.01 | |
| Female (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Age (as of 11 March 2011) | ||||||||||
| 20–39 years | 2.26 | (2.01–2.55) | <0.01 | 2.30 | (2.03–2.60) | <0.01 | 5.24 | (3.62–7.59) | <0.01 | |
| 40–64 years | 1.46 | (1.33–1.61) | <0.01 | 1.46 | (1.32–1.61) | <0.01 | 1.72 | (1.38–2.15) | <0.01 | |
| 65 years and older (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Education | ||||||||||
| Junior/Senior high school | 0.96 | (0.94–0.98) | <0.01 | 0.96 | (0.94–0.99) | <0.01 | 0.97 | (0.92–1.03) | 0.35 | |
| Vocational college, University, Graduated school (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| General subjective health status | ||||||||||
| Poor | 0.96 | (0.93–0.98) | 0.01 | 0.96 | (0.93–0.98) | <0.01 | 1.02 | (0.95–1.10) | 0.51 | |
| Good/Unremarkable (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Sleep disturbance | ||||||||||
| Dissatisfied with sleep condition | Yes | 1.08 | (1.05–1.11) | <0.01 | 1.07 | (1.05–1.10) | <0.01 | 1.07 | (1.00–1.15) | 0.04 |
| No | 1.00 | 1.00 | 1.00 | |||||||
| Psychological distress | ||||||||||
| K6 (13 points and more) | 13≤ | 1.12 | (1.09–1.15) | <0.01 | 1.11 | (1.08–1.14) | <0.01 | 1.14 | (1.07–1.22) | <0.01 |
| ≤12 | 1.00 | 1.00 | 1.00 | |||||||
| Disaster–related experience | ||||||||||
| Experience of tsunami | Yes | – | – | – | 1.04 | (1.01–1.07) | 0.01 | 1.00 | (0.94–1.07) | 0.99 |
| No | – | 1.00 | 1.00 | |||||||
| Experience of nuclear power plant accident | Yes | – | – | – | 1.03 | (1.00–1.05) | 0.03 | 1.07 | (1.02–1.13) | 0.01 |
| No | – | 1.00 | 1.00 | |||||||
| Disaster effects on economic status | ||||||||||
| Loss of employment due to disaster | Yes | – | – | – | 1.02 | (0.99–1.05) | 0.12 | 0.97 | (0.91–1.03) | 0.27 |
| No | – | 1.00 | 1.00 | |||||||
| Perception of radiation risks | ||||||||||
| Delayed effects | High | 1.04 | (1.02–1.06) | <0.01 | 1.00 | (0.95–1.05) | 0.97 | |||
| Low | 1.00 | 1.00 | ||||||||
| 2013 Drinking Status among Newly-Started Drinkers | p Value (χ2) | Continued Drinking | p Value (χ2) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Continued Drinking | Discontinued Drinking | Heavy Drinkers | Light Drinkers | ||||||||
| (n = 953) | (n = 818) | (n = 227) | (n = 726) | ||||||||
| n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Gender | |||||||||||
| Male | 398 | (41.8) | 286 | (35.0) | <0.01 (χ2 = 8.56) | 124 | (54.6) | 274 | (37.7) | <0.01 (χ2 = 20.3) | |
| Female | 555 | (58.2) | 532 | (65.0) | 103 | (45.4) | 452 | (62.3) | |||
| Age (as of 11 March 2011) | |||||||||||
| 20-39 years | 267 | (28.6) | 229 | (28.5) | 83 | (37.9) | 184 | (25.8) | |||
| 40-64 years | 434 | (46.5) | 313 | (39.0) | <0.01 (χ2 = 14.6) | 103 | (47.0) | 331 | (46.4) | <0.01 (χ2 = 19.7) | |
| 65 years and older | 232 | (24.9) | 261 | (32.5) | 33 | (15.1) | 199 | (27.9) | |||
| Education | |||||||||||
| Junior/Senior high school | 610 | (66.6) | 548 | (69.9) | 0.15 (χ2 = 2.12) | 129 | (60.3) | 481 | (68.5) | 0.03 (χ2 = 5.00) | |
| Vocational college, University, Graduated school | 306 | (33.4) | 236 | (30.1) | 85 | (39.7) | 221 | (31.5) | |||
| General subjective health status | |||||||||||
| Poor | 175 | (19.1) | 155 | (19.5) | 0.82 (χ2 = 0.05) | 53 | (23.9) | 122 | (17.5) | 0.04 (χ2 = 4.39) | |
| Good/ Unremarkable | 743 | (80.9) | 640 | (80.5) | 169 | (76.1) | 574 | (82.5) | |||
| Sleep disturbance | |||||||||||
| Dissatisfied with sleep condition | Yes | 644 | (69.3) | 525 | (66.5) | 0.22 (χ2 = 1.52) | 168 | (75.7) | 476 | (67.3) | 0.02 (χ2 = 5.54) |
| No | 285 | (30.7) | 264 | (33.5) | 54 | (24.3) | 231 | (32.7) | |||
| Psychological distress | |||||||||||
| K6 (13 points and more) | 13≤ | 141 | (15.6) | 90 | (11.7) | 0.02 (χ2 = 5.35) | 43 | (19.6) | 98 | (14.3) | 0.06 (χ2 = 3.64) |
| ≤12 | 765 | (84.4) | 682 | (88.3) | 176 | (80.4) | 589 | (85.7) | |||
| Disaster-related experience | |||||||||||
| Experience of tsunami | Yes | 205 | (21.5) | 166 | (20.3) | 0.53 (χ2 = 0.39) | 58 | (25.6) | 147 | (20.2) | 0.09 (χ2 = 2.88) |
| No | 748 | (78.5) | 652 | (79.7) | 169 | (74.4) | 579 | (79.8) | |||
| Experience of nuclear power plant accident | Yes | 863 | (90.6) | 725 | (88.6) | 0.18 (χ2 = 1.76) | 210 | (92.5) | 653 | (89.9) | 0.25 (χ2 = 1.33) |
| No | 90 | (9.4) | 93 | (11.4) | 17 | (7.5) | 73 | (10.1) | |||
| Effect of disaster on economic status | |||||||||||
| Loss of employment due to disaster | Yes | 241 | (25.3) | 216 | (26.4) | 0.59 (χ2 = 0.29) | 64 | (28.2) | 177 | (24.4) | 0.25 (χ2 = 1.33) |
| No | 712 | (74.7) | 602 | (73.6) | 163 | (71.8) | 549 | (75.6) | |||
| Perception of radiation risks | |||||||||||
| Delayed effects | Low | 486 | (54.3) | 451 | (58.4) | 0.09 (χ2 = 2.86) | 107 | (48.9) | 379 | (56.1) | 0.06 (χ2 = 3.46) |
| Low | 416 | (46.7) | 362 | (47.2) | 90 | (41.1) | 326 | (148.9) | |||
| Drinking behavior in 2012 | |||||||||||
| Heavy drinkers (4 drinks/day and more) | 216 | (22.7) | 90 | (11.0) | <0.01 (χ2 = 41.9) | 125 | (55.1) | 91 | (12.5) | <0.01 (χ2 = 178.5) | |
| Light drinkers (less than 4 drinks/day) | 737 | (77.3) | 728 | (89.0) | 102 | (44.9) | 635 | (87.5) | |||
| Model 1 | Model 2 | Model 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Continued vs. Discontinued Drinking | Continued Drinking | |||||||||
| Adjusted by Current Physical/Mental Health Status | Adjusted by Disaster–Related Experience, Disaster Effects on Economic Status, Perception of Radiation Risk and Heavy Drinking | Heavy vs. Light Drinkers | ||||||||
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |||||
| Gender | ||||||||||
| Male | 1.38 | (1.12–1.71) | <0.01 | 1.22 | (0.97–1.53) | 0.08 | 1.84 | (1.25–2.72) | <0.01 | |
| Female (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Age (as of 11 March 2011) | ||||||||||
| 20–39 years | 1.20 | (0.90–1.61) | 0.22 | 1.01 | (0.74–1.37) | 0.97 | 1.74 | (0.96–3.15) | 0.07 | |
| 40–64 years | 0.78 | (0.61–0.99) | 0.05 | 0.69 | (0.53–0.89) | 0.01 | 1.18 | (0.76–1.81) | 0.46 | |
| 65 years and older (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Education | ||||||||||
| Junior/Senior high school | 0.97 | (0.92–1.03) | 0.29 | 0.96 | (0.91–1.02) | 0.20 | 0.93 | (0.84–1.03) | 0.15 | |
| Vocational college, University, Graduated school (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| General subjective health status | ||||||||||
| Poor | 0.96 | (0.90–1.04) | 0.31 | 0.96 | (0.89–1.04) | 0.31 | 1.04 | (0.91–1.19) | 0.54 | |
| Good/Unremarkable (Ref.) | 1.00 | 1.00 | 1.00 | |||||||
| Sleep disturbance | ||||||||||
| Dissatisfied with sleep condition | Yes | 1.02 | (0.96–1.08) | 0.57 | 1.00 | (0.95–1.07) | 0.92 | 1.02 | (0.92–1.14) | 0.69 |
| No | 1.00 | 1.00 | 1.00 | |||||||
| Psychological distress | ||||||||||
| K6 (13 points and more) | 13≤ | 1.09 | (1.00–1.19) | 0.04 | 1.10 | (1.00–1.20) | 0.04 | 1.06 | (0.92–1.22) | 0.39 |
| ≤12 | 1.00 | 1.00 | 1.00 | |||||||
| Disaster–related experience | ||||||||||
| Experience of tsunami | Yes | – | – | – | 1.02 | (0.95–1.09) | 0.56 | 1.10 | (0.98–1.23) | 0.10 |
| No | – | 1.00 | 1.00 | |||||||
| Experience of nuclear power plant accident | Yes | – | – | – | 1.06 | (0.97–1.16) | 0.22 | 1.00 | (0.83–1.20) | 0.97 |
| No | – | 1.00 | 1.00 | |||||||
| Effect of disaster on economic status | ||||||||||
| Loss of employment due to disaster | Yes | – | – | – | 0.95 | (0.89–1.01) | 0.07 | 1.07 | (0.96–1.19) | 0.23 |
| No | – | 1.00 | 1.00 | |||||||
| Perception of radiation risks | ||||||||||
| Delayed effects | High | – | – | – | 1.03 | (0.97–1.09) | 0.34 | 1.07 | (0.97–1.18) | 0.19 |
| Low | – | 1.00 | 1.00 | |||||||
| Drinking behavior in 2012 | ||||||||||
| Heavy drinkers (4 drinks/day and more) | – | – | – | 1.21 | (1.12–1.30) | <0.01 | 1.64 | (1.48–1.81) | <0.01 | |
| Light drinkers (less than 4 drinks/day) | – | 1.00 | 1.00 | |||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orui, M.; Ueda, Y.; Suzuki, Y.; Maeda, M.; Ohira, T.; Yabe, H.; Yasumura, S. The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2017, 14, 1281. https://doi.org/10.3390/ijerph14101281
Orui M, Ueda Y, Suzuki Y, Maeda M, Ohira T, Yabe H, Yasumura S. The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2017; 14(10):1281. https://doi.org/10.3390/ijerph14101281
Chicago/Turabian StyleOrui, Masatsugu, Yuka Ueda, Yuriko Suzuki, Masaharu Maeda, Tetsuya Ohira, Hirooki Yabe, and Seiji Yasumura. 2017. "The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 14, no. 10: 1281. https://doi.org/10.3390/ijerph14101281
APA StyleOrui, M., Ueda, Y., Suzuki, Y., Maeda, M., Ohira, T., Yabe, H., & Yasumura, S. (2017). The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health, 14(10), 1281. https://doi.org/10.3390/ijerph14101281