Outcomes in the Utilization of Single Percutaneous Cholecystostomy in a Low-Income Population

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Data Source
2.2. Data Protection and Permission
2.3. Data Definition
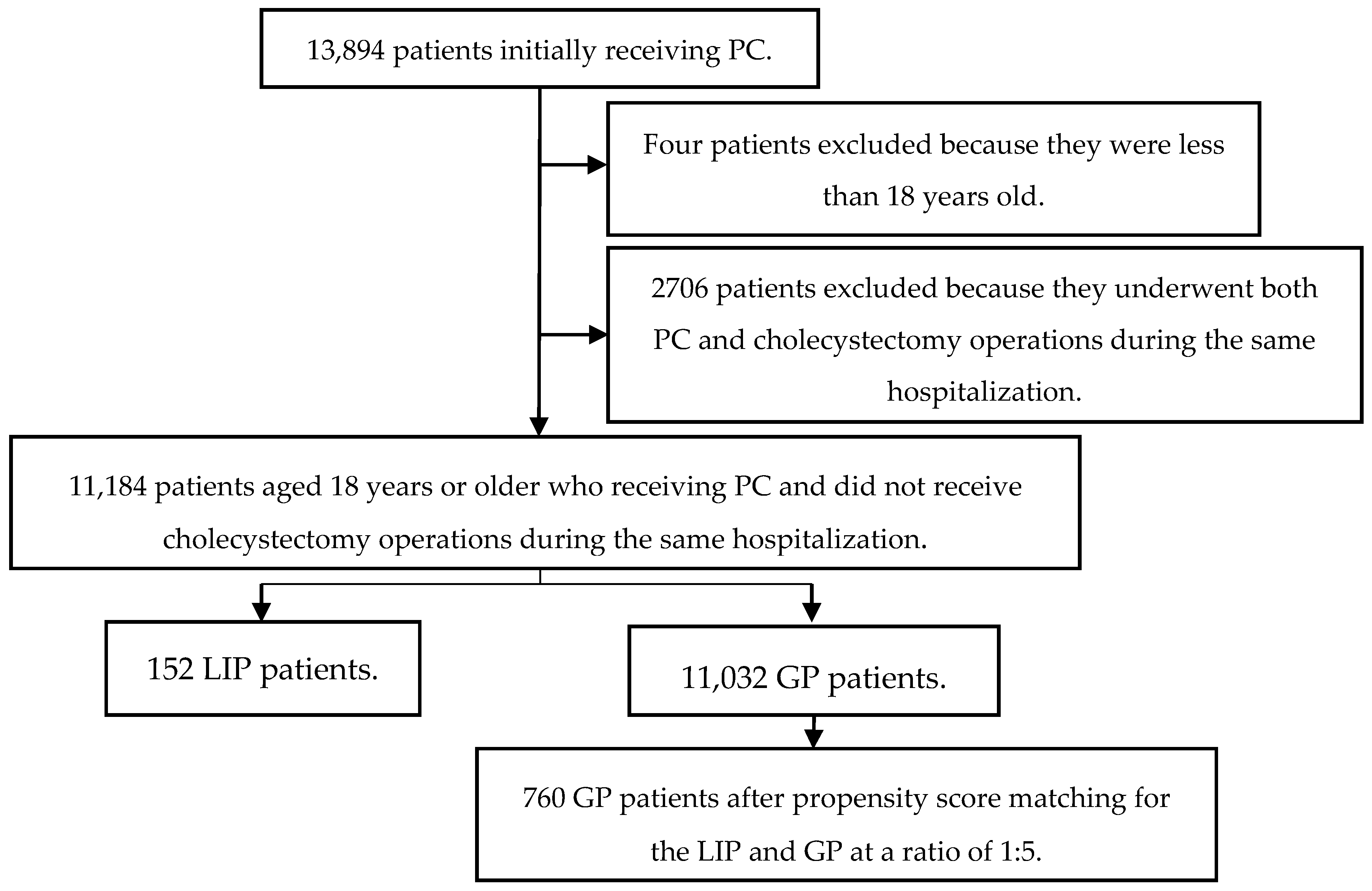
2.4. Patient Selection
2.5. Measurement Outcomes
2.5.1. Thirty-Day Mortality and In-Hospital Mortality
2.5.2. In-Hospital Complications
2.5.3. Routine Discharge
2.5.4. One-Year Recurrence
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Patterson, E.J.; Mcloughlin, R.F.; Mathieson, J.R.; Cooperberg, P.L.; Macfarlane, J.K. An alternative approach to acute cholecystitis. Percutaneous cholecystostomy and interval laparoscopic cholecystectomy. Surg. Endosc. 1996, 10, 1185–1188. [Google Scholar] [CrossRef] [PubMed]
- Abi-Haidar, Y.; Sanchez, V.; Williams, S.A.; Itani, K.M. Revisiting percutaneous cholecystostomy for acute cholecystitis based on a 10-year experience. Arch. Surg. 2012, 147, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Yoo, K.S. Efficacy of preoperative percutaneous cholecystostomy in the management of acute cholecystitis according to severity grades. Korean J. Intern. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Teoh, W.M.; Cade, R.J.; Banting, S.W.; Mackay, S.; Hassen, A.S. Percutaneous cholecystostomy in the management of acute cholecystitis. ANZ J. Surg. 2005, 75, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Mckay, A.; Abulfaraj, M.; Lipschitz, J. Short- and long-term outcomes following percutaneous cholecystostomy for acute cholecystitis in high-risk patients. Surg. Endosc. 2012, 26, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Aljundi, W.; Cannon, T.; Antakia, R.; Anoop, U.; Balamurugan, R.; Everitt, N.; Ravi, K. Percutaneous cholecystostomy as an alternative to cholecystectomy in high risk patients with biliary sepsis: A district general hospital experience. Ann. R. Coll Surg. Engl. 2012, 94, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.C.; Chang, C.W.; Chu, C.H. Percutaneous cholecystostomy for acute cholecystitis in high-risk elderly patients. Kaohsiung J. Med. Sci. 2016, 32, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Welschbilligmeunier, K.; Pessaux, P.; Lebigot, J.; Lermite, E.; Ch, A.; Brehant, O.; Hamy, A.; Arnaud, J.P. Percutaneous cholecystostomy for high-risk patients with acute cholecystitis. Surg. Endosc. Other Interv. Tech. 2005, 19, 1256–1259. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, R.L.; Ryan, C.M.; Lee, M.J.; Mueller, P.R.; Tompkins, R.G. Percutaneous cholecystostomy in the critically ill burn patient. J. Trauma 1995, 38, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Hermiz, S.J.; Diegidio, P.; Garimella, R.; Ortiz-Pujols, S.; Yu, H.; Isaacson, A.; Mauro, M.A.; Cairns, B.A.; Hultman, C.S. Acalculous Cholecystitis in Burn Patients: Is There a Role for Percutaneous Cholecystostomy? Clin. Plast. Surg. 2017, 44, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Moonka, R.; Stelzner, M. Percutaneous cholecystostomy for acute cholecystitis in veteran patients. Am. J. Surg. 2000, 180, 198–202. [Google Scholar] [CrossRef]
- Caliskan, K. The use of percutaneous cholecystostomy in the treatment of acute cholecystitis during pregnancy. Clin. Exp. Obstet. Gynecol. 2017, 44, 11–13. [Google Scholar]
- Allmendinger, N.; Hallisey, M.J.; Ohki, S.K.; Straub, J.J. Percutaneous cholecystostomy treatment of acute cholecystitis in pregnancy. Obstet. Gynecol. 1995, 86, 653–654. [Google Scholar] [CrossRef]
- Bonito, A.J.; Bann, C.; Eicheldinger, C.; Carpenter, L. Creation of New Race-Ethnicity Codes and Socioeconomic Status (SES) Indicators for Medicare Beneficiaries; RTI International, Agency for Healthcare Research and Quality: Chapel Hill, NC, USA, 2008.
- Bennett, K.M.; Scarborough, J.E.; Pappas, T.N.; Kepler, T.B. Patient socioeconomic status is an independent predictor of operative mortality. Ann. Surg. 2010, 252, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, N.J.; Gu, N.; Baser, O.; Morris, A.M.; Birkmeyer, J.D. Socioeconomic status and surgical mortality in the elderly. Med. Care 2008, 46, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.K.; Rosenthal, M.; Hazuda, H.P.; Comeaux, P.J.; Stern, M.P. Socioeconomic status and the prevalence of clinical gallbladder disease. J. Chronic Dis. 1985, 38, 1019–1026. [Google Scholar] [CrossRef]
- Ambur, V.; Taghavi, S.; Kadakia, S.; Jayarajan, S.; Gaughan, J.; Sjoholm, L.O.; Pathak, A.; Santora, T.; Rappold, J.; Goldberg, A.J. Does socioeconomic status predict outcomes after cholecystectomy? Am. J. Surg. 2016, 221, S68. [Google Scholar] [CrossRef]
- Department of Statistics (DOS). Ministry of the Interior, Survey of Living Conditions of Low-Income Households in Taiwan-Fuchien Area. 2008. Available online: http://www.mohw.gov.tw/cht/DOS/Statistic.aspx?f_list_no=312&fod_list_no=4699 (accessed on 5 February 2015).
- Chou, Y.; Lin, S. Report of the Survey of the Basic Needs for Low-Income Families in Taoyuan County, Taiwan; Hsuan Chuang University: Hsinchu City, Taiwan, 2007. [Google Scholar]
- Department of Statistics Mohaw. Report on the Low-Income and Middle-Income Family Living Condition Survey 2013; Department of Health and Welfare of the Executive Yuan: Taipei City, Taiwan, 2014.
- Anderson, J.E.; Chang, D.C.; Talamini, M.A. A nationwide examination of outcomes of percutaneous cholecystostomy compared with cholecystectomy for acute cholecystitis, 1998–2010. Surg. Endosc. 2013, 27, 3406–3411. [Google Scholar] [CrossRef] [PubMed]
- Public Assistance Act. Available online: http://law.moj.gov.tw/LawClass/LawAll.aspx?PCode=D0050078 (accessed on 5 September 2017).
- Taiwan NHI Information for the Public: Essential Data of Ensured Affair. Available online: http://www.nhi.gov.tw/webdata/webdata.aspx?menu=17&menu_id=661&WD_ID=689&webdata_id=805 (accessed on 7 December 2013).
- Caliendo, M.; Kopeinig, S. Some Practical Guidance for the Implementation of Propensity Score Matching. J. Econ. Surv. 2008, 22, 31–72. [Google Scholar] [CrossRef]
- Joinpoint Regression Program; version 4.3.1.0; Statistical Methodology and Applications Branch, Surveillance Research Program; National Cancer Institute: Bethesda, MD, USA, April 2016.
- National Cancer Institute; version 4.3.1.0; Surveillance Research Program, Statistical Methodology and Applications Branch, Joinpoint Regression Program Online Help System; National Cancer Institute: Bethesda, MD, USA, April 2016.
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-T. Poverty in Taiwan: A review of related studies. NTU Soc. Work Rev. J. 2005, 10, 1–54. [Google Scholar]
- Chang, Y.R.; Ahn, Y.J.; Jang, J.Y.; Kang, M.J.; Kwon, W.; Jung, W.H.; Kim, S.W. Percutaneous cholecystostomy for acute cholecystitis in patients with high comorbidity and re-evaluation of treatment efficacy. Surgery 2014, 155, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Duszak, R.; Behrman, S.W. National trends in percutaneous cholecystostomy between 1994 and 2009: Perspectives from Medicare provider claims. J. Am. Coll. Radiol. 2012, 9, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Manske, J.G.; Mathiason, M.A.; Kallies, K.J.; Kothari, S.N. Changing trends and outcomes in the use of percutaneous cholecystostomy tubes for acute cholecystitis. Ann. Surg. 2013, 257, 1112–1115. [Google Scholar] [CrossRef] [PubMed]
- Cherng, N.; Witkowski, E.T.; Sneider, E.B.; Wiseman, J.T.; Lewis, J.; Litwin, D.E.M.; Santry, H.P.; Cahan, M.; Shah, S.A. Use of cholecystostomy tubes in the management of patients with primary diagnosis of acute cholecystitis. J. Am. Coll. Surg. 2012, 214, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Takada, T.; Kawarada, Y.; Nimura, Y.; Miura, F.; Yoshida, M.; Mayumi, T.; Strasberg, S.; Pitt, H.A.; Gadacz, T.R.; et al. Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, Y.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Buchler, M.W.; Gomi, H.; Dervenis, C.; Windsor, J.A.; et al. TG13 surgical management of acute cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Li, J.C.; Lee, D.W.; Lai, C.W.; Li, A.C.; Chu, D.W.; Chan, A.C. Percutaneous cholecystostomy for the treatment of acute cholecystitis in the critically ill and elderly. Hong Kong Med. J. 2004, 10, 389–393. [Google Scholar] [PubMed]
- Horn, T.; Christensen, S.D.; Kirkegård, J.; Larsen, L.P.; Knudsen, A.R.; Mortensen, F.V. Percutaneous cholecystostomy is an effective treatment option for acute calculous cholecystitis: A 10-year experience. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2015, 17, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Sanjay, P.; Mittapalli, D.; Marioud, A.; White, R.D.; Ram, R.; Alijani, A. Clinical outcomes of a percutaneous cholecystostomy for acute cholecystitis: A multicentre analysis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2013, 15, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Nasim, S.; Khan, S.; Alvi, R.; Chaudhary, M. Emerging indications for percutaneous cholecystostomy for the management of acute cholecystitis—A retrospective review. Int. J. Surg. 2011, 9, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Winbladh, A.; Gullstrand, P.; Svanvik, J.; Sandström, P. Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2009, 11, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Hadashalpern, I.; Patlas, M.; Knizhnik, M.; Zaghal, I.; Fisher, D. Percutaneous cholecystostomy in the management of acute cholecystitis. IMAJ 2003, 5, 170–171. [Google Scholar]
- Li, M.; Li, N.; Ji, W.; Quan, Z.; Wan, X.; Wu, X.; Li, J. Percutaneous cholecystostomy is a definitive treatment for acute cholecystitis in elderly high-risk patients. Am. Surg. 2013, 79, 524–527. [Google Scholar] [PubMed]
- Mcgillicuddy, E.A.; Schuster, K.M.; Barre, K.; Suarez, L.; Hall, M.R.; Kaml, G.J.; Davis, K.A.; Longo, W.E. Non-operative management of acute cholecystitis in the elderly. Br. J. Surg. 2012, 99, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.H.; Wu, C.Y.; Yang, J.C.; Lien, W.C.; Wang, H.P.; Liu, K.L.; Wu, Y.M.; Chen, S.C. Long-Term Outcomes of Patients with Acute Cholecystitis after Successful Percutaneous Cholecystostomy Treatment and the Risk Factors for Recurrence: A Decade Experience at a Single Center. PLoS ONE 2016, 11, e0148017. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Low-Income Population (N = 152) | General Population (N = 11,032) | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | 0.005 | ||||
| Female | 45 | 29.61% | 4525 | 41.02% | |
| Male | 107 | 70.39% | 6507 | 58.98% | |
| Age Stratum | <0.001 | ||||
| 18–29 y/o | 0 | 0.00% | 111 | 1.01% | |
| 30–39 y/o | 8 | 5.26% | 302 | 2.74% | |
| 40–49 y/o | 27 | 17.76% | 614 | 5.57% | |
| 50–59 y/o | 31 | 20.39% | 1336 | 12.11% | |
| 60–69 y/o | 19 | 12.50% | 1856 | 16.82% | |
| 70 y/o or more | 67 | 44.08% | 6813 | 61.76% | |
| CCI Score | 0.445 | ||||
| 0 | 72 | 47.37% | 5422 | 49.15% | |
| 1 | 46 | 30.26% | 2782 | 25.22% | |
| 2 | 19 | 12.50% | 1407 | 12.75% | |
| ≥3 | 15 | 9.87% | 1421 | 12.88% | |
| Cause of Procedure | 0.386 | ||||
| AC with a C/S | 53 | 34.87% | 4063 | 36.83% | |
| AC without a C/S | 55 | 36.18% | 3369 | 30.54% | |
| Calculus without AC | 16 | 10.53% | 1228 | 11.13% | |
| ODGBT | 12 | 7.89% | 1369 | 12.41% | |
| MNDOP | 7 | 4.61% | 347 | 3.15% | |
| Other | 9 | 5.92% | 656 | 5.95% | |
| Hospital Level | <0.001 | ||||
| Medical Center | 60 | 39.47% | 6205 | 56.25% | |
| Regional Hospital | 76 | 50.00% | 4551 | 41.25% | |
| District Hospital | 16 | 10.53% | 276 | 2.50% | |
| Variables | Low-Income Population (N = 152) | Control Group (N = 760) | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | 1.00 | ||||
| Female | 45 | 29.61% | 225 | 29.61% | |
| Male | 107 | 70.39% | 535 | 70.39% | |
| Age Stratum | 0.927 | ||||
| 18–29 y/o | 0 | 0.00% | 4 | 0.53% | |
| 30–39 y/o | 8 | 5.26% | 32 | 4.21% | |
| 40–49 y/o | 27 | 17.76% | 126 | 16.58% | |
| 50–59 y/o | 31 | 20.39% | 166 | 21.84% | |
| 60–69 y/o | 19 | 12.50% | 99 | 13.03% | |
| 70 y/o or more | 67 | 44.08% | 333 | 43.82% | |
| CCI Score | 0.95 | ||||
| 0 | 72 | 47.37% | 377 | 49.61% | |
| 1 | 46 | 30.26% | 214 | 28.16% | |
| 2 | 19 | 12.50% | 97 | 12.76% | |
| ≥3 | 15 | 9.87% | 72 | 9.47% | |
| Cause of Procedure | 1.00 | ||||
| AC with a C/S | 53 | 34.87% | 265 | 34.87% | |
| AC without a C/S | 55 | 36.18% | 278 | 36.58% | |
| Calculus without AC | 16 | 10.53% | 84 | 11.05% | |
| ODGBT | 12 | 7.89% | 56 | 7.37% | |
| MNDOP | 7 | 4.61% | 36 | 4.74% | |
| Other | 9 | 5.92% | 41 | 5.39% | |
| Hospital Level | 0.865 | ||||
| Medical Center | 60 | 39.47% | 290 | 38.16% | |
| Regional Hospital | 76 | 50.00% | 397 | 52.24% | |
| District Hospital | 16 | 10.53% | 73 | 9.61% | |
| Outcome Variable | Total (N = 912) | Low-Income Population (N = 152) | Control (N = 760) | p Value a | |||
|---|---|---|---|---|---|---|---|
| n | Percent (%) | n | Percent (%) | n | Percent (%) | ||
| In-Hospital Mortality | 92 | 10.09% | 23 | 15.13% | 69 | 9.08% | 0.024 |
| Crude OR (95% CI) | -- | 1.786 (1.074, 2.967) | 1.0 | 0.025 | |||
| Adjusted OR (95% CI) | -- | 1.816 (1.079, 3.056) | 1.0 | 0.025 | |||
| 30-Day Mortality | 41 | 4.50% | 9 | 5.92% | 32 | 4.21% | 0.353 |
| Crude OR (95% CI) | -- | 1.432 (0.669, 3.064) | 1.0 | 0.355 | |||
| Adjusted OR (95% CI) | -- | 1.431 (0.651, 3.146) | 1.0 | 0.373 | |||
| In-Hospital Complications | 18 | 1.97% | 4 | 2.63% | 14 | 1.84% | 0.523 |
| Crude OR (95% CI) | -- | 1.440 (0.468, 4.436) | 1.0 | 0.525 | |||
| Adjusted OR (95% CI) | -- | 1.446 (0.464, 4.501) | 1.0 | 0.525 | |||
| Rate of Routine Discharge | 766 | 83.99% | 121 | 79.61% | 645 | 84.87% | 0.106 |
| Crude OR (95% CI) | -- | 0.696 (0.447, 1.082) | 1.0 | 0.108 | |||
| Adjusted OR (95% CI) | -- | 0.682 (0.430, 1.083) | 1.0 | 0.104 | |||
| One-Year Recurrence | 199 | 21.82% | 23 | 15.13% | 176 | 23.16% | 0.029 |
| Crude OR (95% CI) | -- | 0.592 (0.368, 0.951) | 1.0 | 0.030 | |||
| Adjusted OR (95% CI) | -- | 0.583 (0.360, 0.945) | 1.0 | 0.029 | |||
| Length of Hospital Stay (Mean ± SE) | -- | 18.26 ± 1.16 | 17.18 ± 0.15 | 0.894 | |||
| Hospital Costs (Mean ± SE) b | -- | 3914.52 ± 329.89 | 4109.36 ± 53.06 | 0.048 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, P.; Yang, N.-P.; Chang, N.-T.; Lai, K.R.; Lin, K.-B.; Chan, C.-L. Outcomes in the Utilization of Single Percutaneous Cholecystostomy in a Low-Income Population. Int. J. Environ. Res. Public Health 2017, 14, 1601. https://doi.org/10.3390/ijerph14121601
Lu P, Yang N-P, Chang N-T, Lai KR, Lin K-B, Chan C-L. Outcomes in the Utilization of Single Percutaneous Cholecystostomy in a Low-Income Population. International Journal of Environmental Research and Public Health. 2017; 14(12):1601. https://doi.org/10.3390/ijerph14121601
Chicago/Turabian StyleLu, Ping, Nan-Ping Yang, Nien-Tzu Chang, K. Robert Lai, Kai-Biao Lin, and Chien-Lung Chan. 2017. "Outcomes in the Utilization of Single Percutaneous Cholecystostomy in a Low-Income Population" International Journal of Environmental Research and Public Health 14, no. 12: 1601. https://doi.org/10.3390/ijerph14121601
APA StyleLu, P., Yang, N.-P., Chang, N.-T., Lai, K. R., Lin, K.-B., & Chan, C.-L. (2017). Outcomes in the Utilization of Single Percutaneous Cholecystostomy in a Low-Income Population. International Journal of Environmental Research and Public Health, 14(12), 1601. https://doi.org/10.3390/ijerph14121601