
A Pilot Study to Examine Exposure to Residential Radon in Under-Sampled Census Tracts of DeKalb County, Georgia, in 2015

 ,
, 
Abstract
:1. Introduction
1.1. Background
1.2. Study Objective
- To describe a pilot study of randomly selected households for recruitment for in-home radon measurements in 14 census tracts in DeKalb County, GA, USA
- To analyze tract-level socio-economic and demographic characteristics to understand differences between the pilot study tracts and the remaining tracts in the county
- To analyze radon levels in homes and identify housing characteristics associated with radon in homes.
2. Materials and Methods
2.1. Training and Institutional Review Board (IRB) Approval
2.2. Study Recruitment Procedures
2.3. Data Collection
2.4. Data Analysis
2.5. American Community Survey Data
3. Results
3.1. Descriptive Statistics Regarding Census Tracts
3.2. Household Recruitment
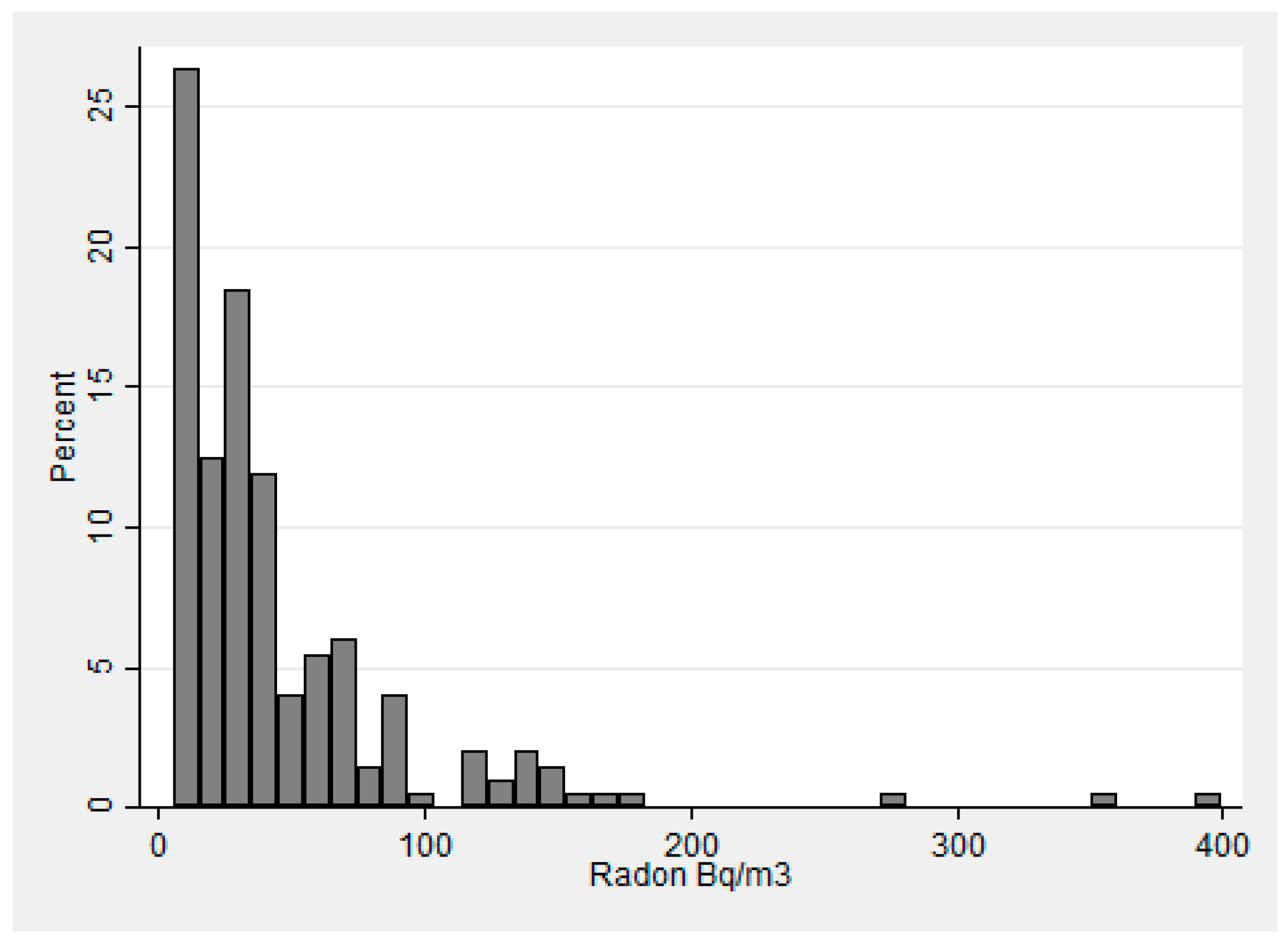
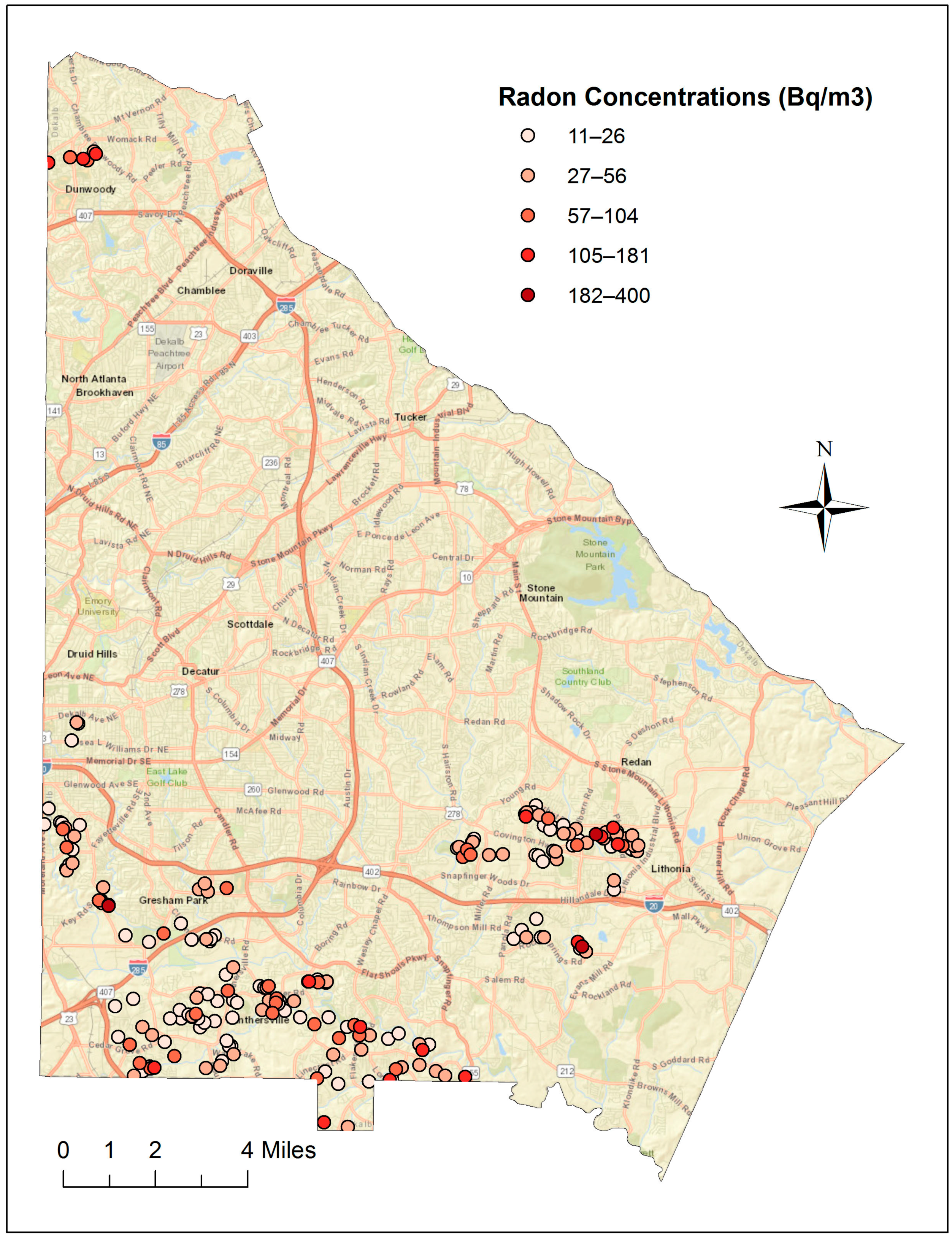
Radon Results
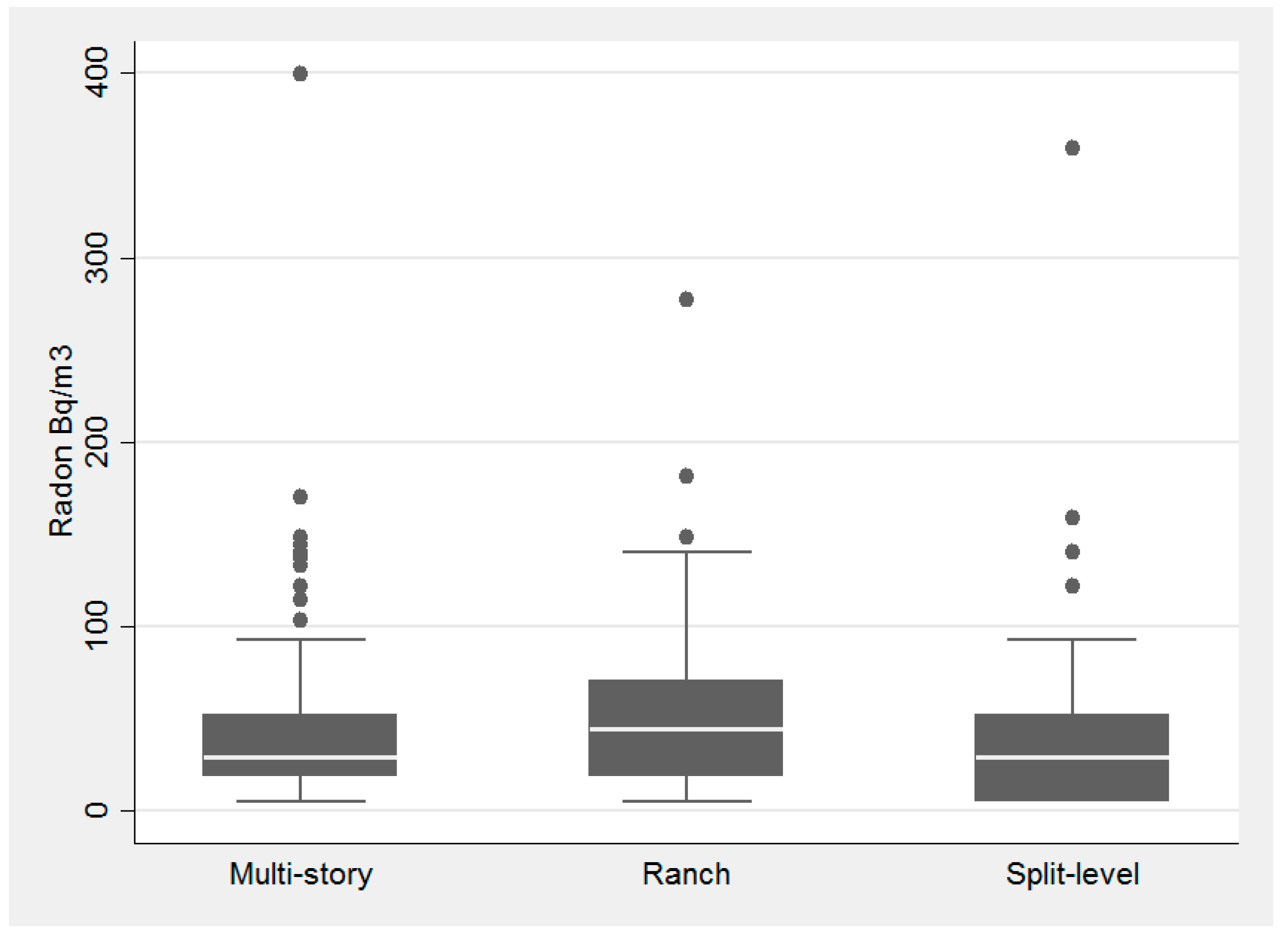
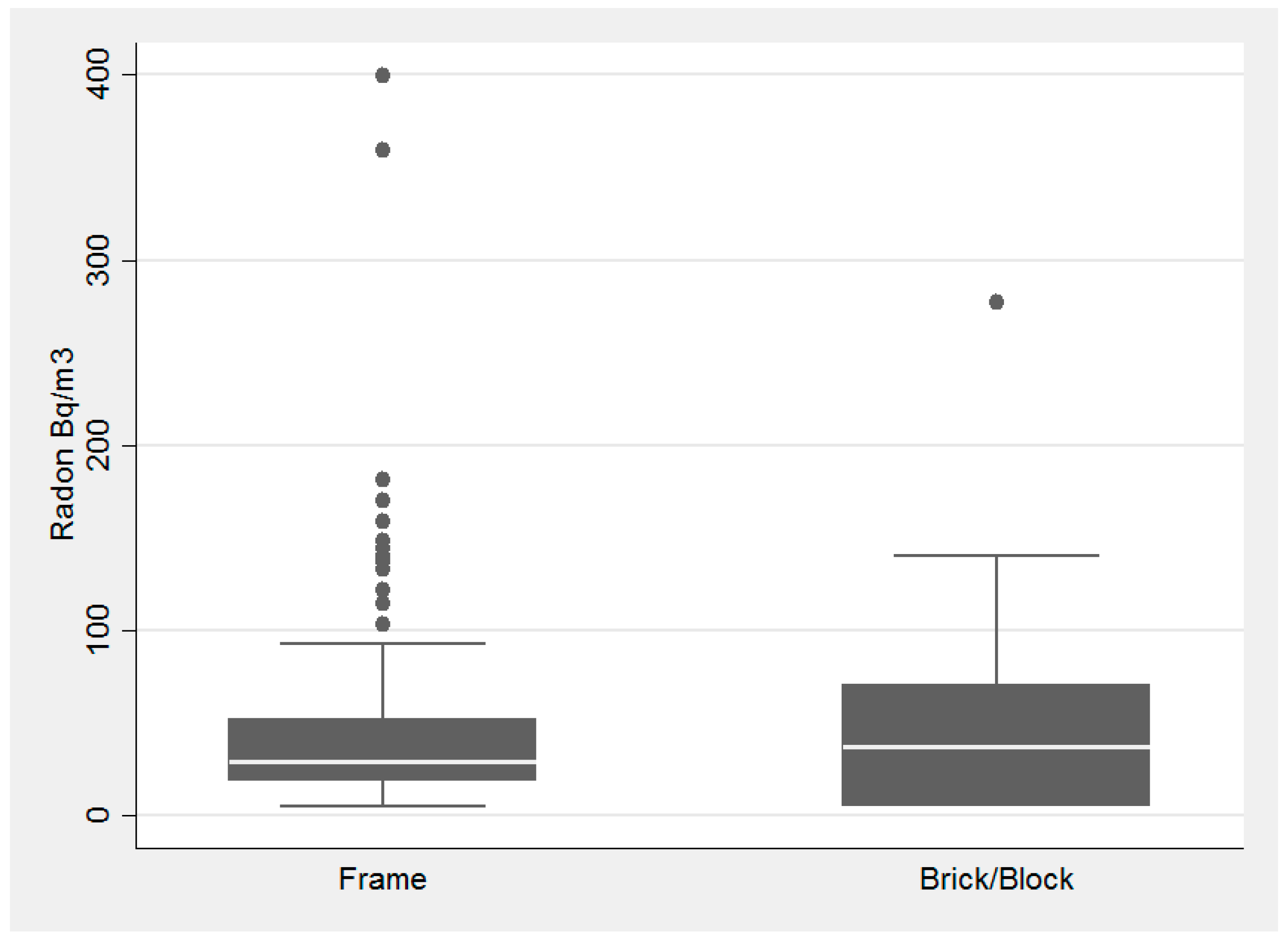
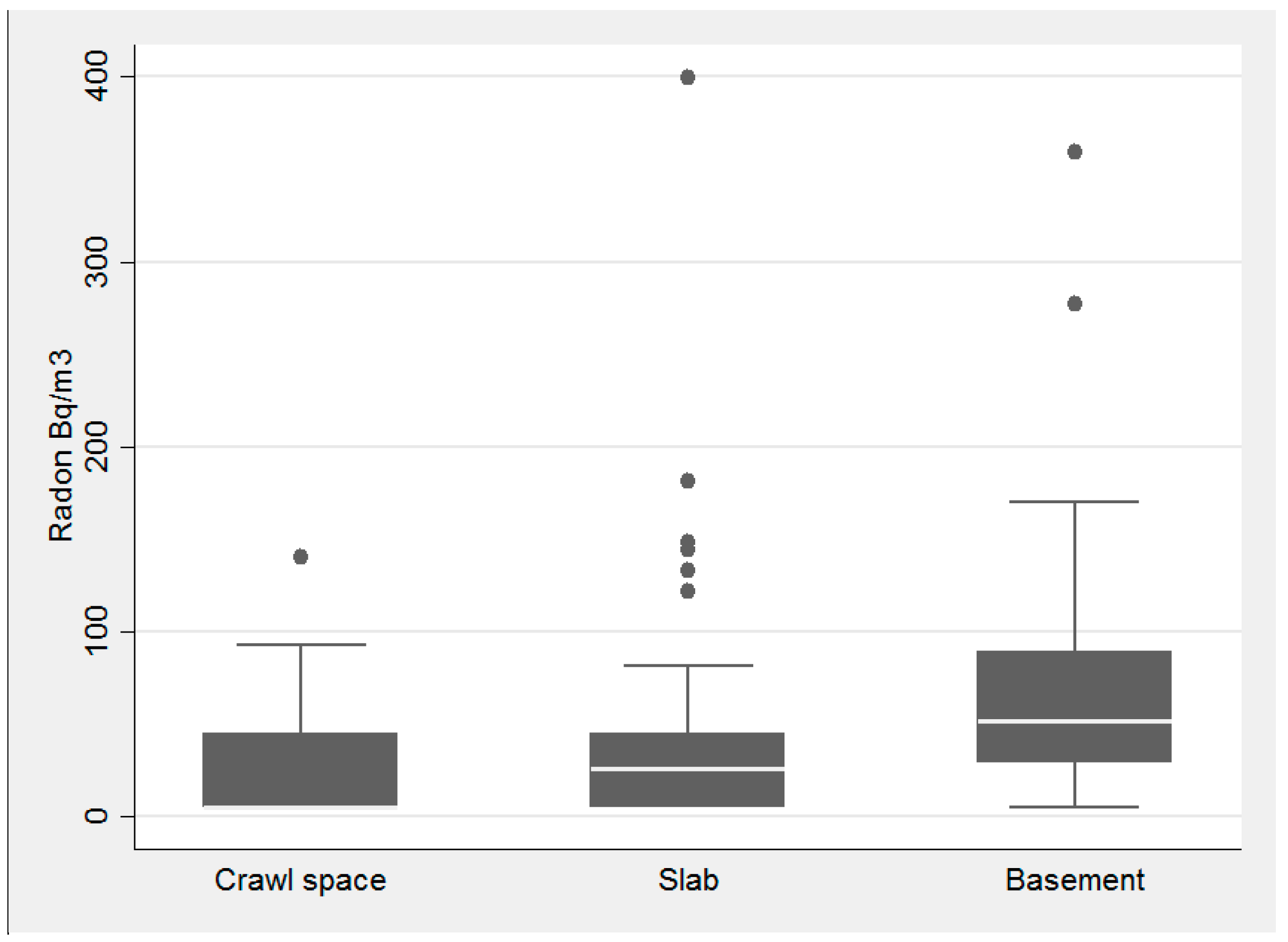
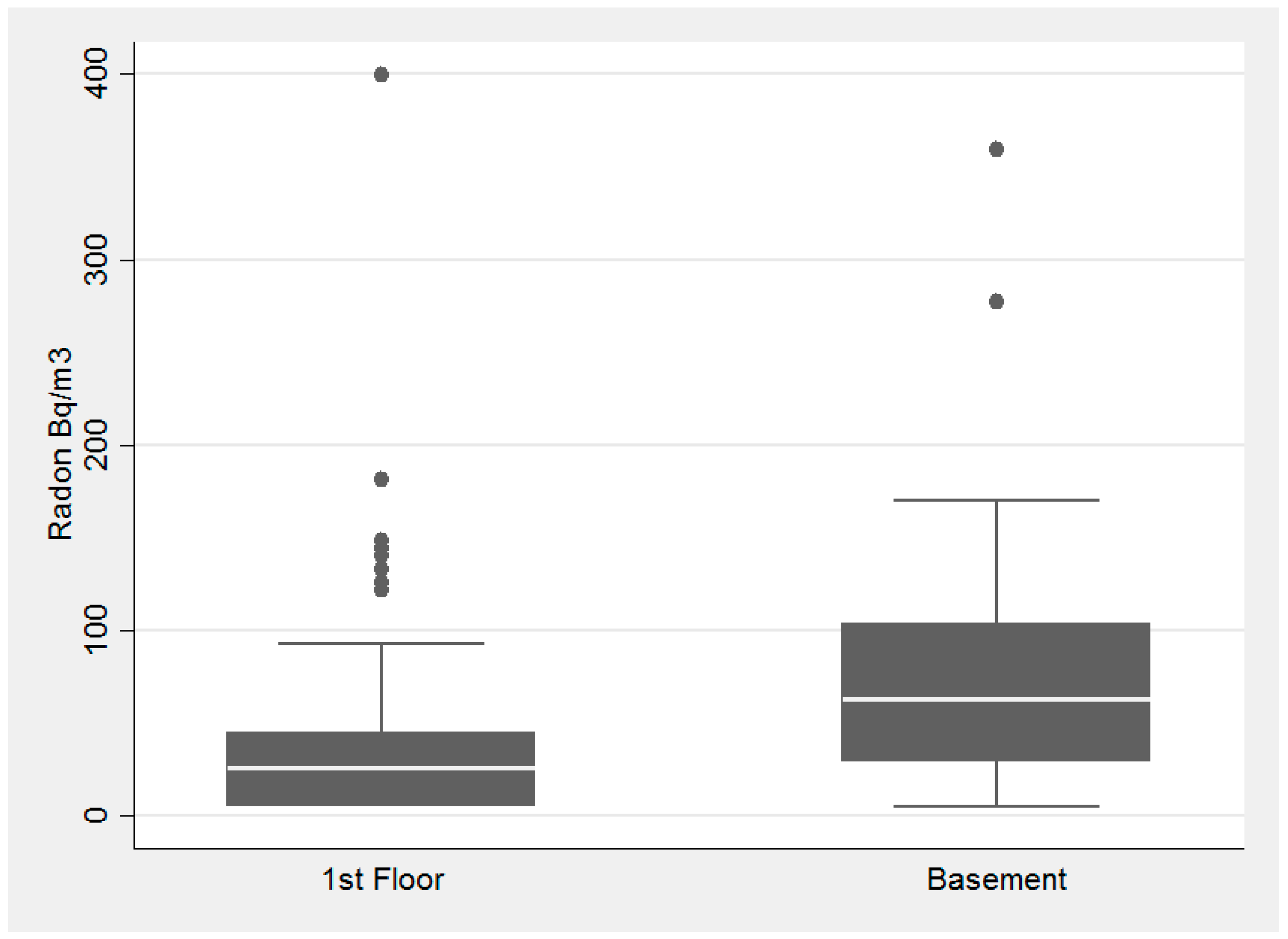
3.3. Examination of Radon and Housing Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- National Cancer Institute. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/radon/radon-fact-sheet (accessed on 13 February 2016).
- Darby, S.; Hill, D.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M.; et al. Radon in homes and risk of lung cancer: Collaborative analysis of individual data from 13 European case-control studies. BMJ 2005, 330. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D.; Lubin, J.H.; Zielinkski, J.M.; Alavanja, M.; Catalan, V.S.; Field, R.W.; Klotz, J.B.; Létourneau, E.G.; Lynch, C.F.; Lyon, J.I.; et al. Residential radon and risk of lung cancer: A combined analysis of 7 North American case-control studies. Epidemiology 2005, 16, 137–145. [Google Scholar] [CrossRef] [PubMed]
- George, A.C. The history, development and the present status of the radon measurement programme in the United States of America. Radiat. Prot. Dosim. 2015, 167, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Environmental Protect Agency. Available online: https://www.epa.gov/radon/health-risk-radon (accessed on 10 April 2016).
- DeKalb County Board of Health. Available online: https://dekalbhealth.net/envhealth/radon/ (accessed on 21 December 2016).
- Duckworth, L.T.; Frank-Stromberg, M.; Oleckno, W.A.; Duffy, P.; Burns, K. Relationship of Perception of Radon as a Health Risk and Willingness to Engage in Radon Testing and Mitigation. Oncol. Nurs. Forum. 2002, 29, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- DeKalb County Radon Information. Available online: http://county-radon.info/GA/DeKalb.html (accessed on 20 March 2017).
- Neal, F. Geographic Variation of Radon Gas Concentrations in Relationship to Housing Characteristics in Dekalb County, Georgia. Master’s Thesis, Georgia State University, Atlanta, GA, USA, 2016. [Google Scholar]
- Wittle, K.; Berkowitz, J.M.; Lillie, J.M.; Cameron, K.A.; Kiu, W.Y. Radon awareness and reduction campaigns for African Americans: A theoretically based evaluation. Health Educ. Behav. 1998, 25, 284–303. [Google Scholar] [CrossRef] [PubMed]
- Berens, A. The Use of In Situ Gamma Radiation Measurements as a Method of Determining Radon Potential in Urban Environments. Master’s Thesis, Georgia State University, Atlanta, GA, USA, 2016. [Google Scholar]
- Halpern, M.T.; Warner, K.E. Radon risk perception and testing: Sociodemographic correlates. J. Environ. Health 1994, 56, 31–35. [Google Scholar]
- Georgia Department of Public Health. Available online: https://dph.georgia.gov/sites/dph.georgia.gov/files/2015%20Georgia%20Tobacco%20Use%20Surveillance%20Report.pdf (accessed on 29 December 2016).
- Kitto, M.E. Assessing radon concentrations in areas with few measurements. Environ. Monit. Assess. 2003, 83, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Price, P.N.; Nero, A.V.; Gelman, A. Bayesian predictions of mean indoor radon concentrations for Minnesota counties. Health Phys. Soc. 1996, 71, 922–936. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Characteristics | 14 Sampled Tracts | Remaining 130 Census Tracts | |
|---|---|---|---|
| Population | |||
| Race | White * | 12.0% | 41.6% |
| Black/African American * | 81.7% | 46.5% | |
| American Indian/Alaska Native | 0.2% | 0.5% | |
| Asian * | 3.6% | 6.0% | |
| Native Hawaiian & Other Pacific Islander | <0.1% | <0.1% | |
| Other * | 0.7% | 3.1% | |
| Education (≥25 years) | Less than Highschool (HS) | 10.2% | 12.7% |
| HS Graduate (includes equivalency) * | 27.4% | 20.2% | |
| Some college * | 31.7% | 24.5% | |
| Bachelor’s degree or higher ** | 30.7% | 42.5% | |
| Poverty Status | Mean income at household level | $60,789 | $77,244 |
| Median income at household level | $49,387 | $58,481 | |
| Below poverty level | 18% | 15.3% | |
| Household Characteristics | All n (%) | Valid Radon Test n (%) | |
|---|---|---|---|
| Total households | 217 | 201 | |
| Smoking in home | Yes | 49 (22.6) | 49 (24.3) |
| Children in home | Yes | 109 (50.2) | 100 (49.8) |
| Heard of radon | No | 115 (53.0) | 106 (52.7) |
| Floor tested | First | 171 (78.8) | 156 (77.6) |
| Basement | 45 (20.7) | 45 (22.4) | |
| Missing | 1 (0.5) | ||
| Housing type | Split-level | 61 (28.1) | 56 (27.8) |
| Ranch | 45 (20.7) | 41 (20.4) | |
| Multi-story | 113 (52.1) | 103 (51.7) | |
| Building type | Block/Brick | 44 (20.3) | 43 (21.4) |
| Frame | 140 (64.5) | 127 (63.2) | |
| Combination | 32 (14.8) | 30 (14.9) | |
| Missing | 1 (0.5) | 1 (0.5) | |
| Foundation type | Basement | 59 (27.2) | 57 (28.4) |
| Crawl Space | 25 (11.5) | 23 (11.4) | |
| Slab | 133 (61.3) | 121 (60.2) | |
| Housing Characteristic Variable | Bivariate Logistic Model (Outcome Radon above ≥11.1) OR (95% CI) | Multivariate Model (Outcome Radon above ≥11.1) OR (95% CI) | Bivariate Logistic Model (Outcome Radon above ≥148) OR (95% CI) | Multivariate Model (Outcome Radon above ≥148) OR (95% CI) |
|---|---|---|---|---|
| Building type (dichotomous) | 0.76 (0.36, 1.61) | 0.56 (0.24, 1.32) | 0.51 (0.06, 4.26) | 0.27 (0.03, 2.44) |
| Foundation type (three-level ordinal) | 3.65 (1.99, 6.67) | 3.97 (1.96, 8.02) | 4.25 (1.07, 16.80) | 2.19 (0.31, 15.54) |
| Floor of sample (dichotomous) | 2.27 (0.94, 5.45) | 0.80 (0.26, 2.42) | 6.38 (1.46, 27.81) | 4.08 (0.47, 35.16) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stauber, C.E.; Dai, D.; Chan, S.R.; Diem, J.E.; Weaver, S.R.; Rothenberg, R. A Pilot Study to Examine Exposure to Residential Radon in Under-Sampled Census Tracts of DeKalb County, Georgia, in 2015. Int. J. Environ. Res. Public Health 2017, 14, 332. https://doi.org/10.3390/ijerph14030332
Stauber CE, Dai D, Chan SR, Diem JE, Weaver SR, Rothenberg R. A Pilot Study to Examine Exposure to Residential Radon in Under-Sampled Census Tracts of DeKalb County, Georgia, in 2015. International Journal of Environmental Research and Public Health. 2017; 14(3):332. https://doi.org/10.3390/ijerph14030332
Chicago/Turabian StyleStauber, Christine E., Dajun Dai, Sydney R. Chan, Jeremy E. Diem, Scott R. Weaver, and Richard Rothenberg. 2017. "A Pilot Study to Examine Exposure to Residential Radon in Under-Sampled Census Tracts of DeKalb County, Georgia, in 2015" International Journal of Environmental Research and Public Health 14, no. 3: 332. https://doi.org/10.3390/ijerph14030332
APA StyleStauber, C. E., Dai, D., Chan, S. R., Diem, J. E., Weaver, S. R., & Rothenberg, R. (2017). A Pilot Study to Examine Exposure to Residential Radon in Under-Sampled Census Tracts of DeKalb County, Georgia, in 2015. International Journal of Environmental Research and Public Health, 14(3), 332. https://doi.org/10.3390/ijerph14030332