The Associations between Types of Ambient PM2.5 and Under-Five and Maternal Mortality in Africa



Abstract
:1. Introduction
2. Methods
2.1. The Spatial Domain
2.2. Variables
2.2.1. Under-Five and Maternal Mortality Data
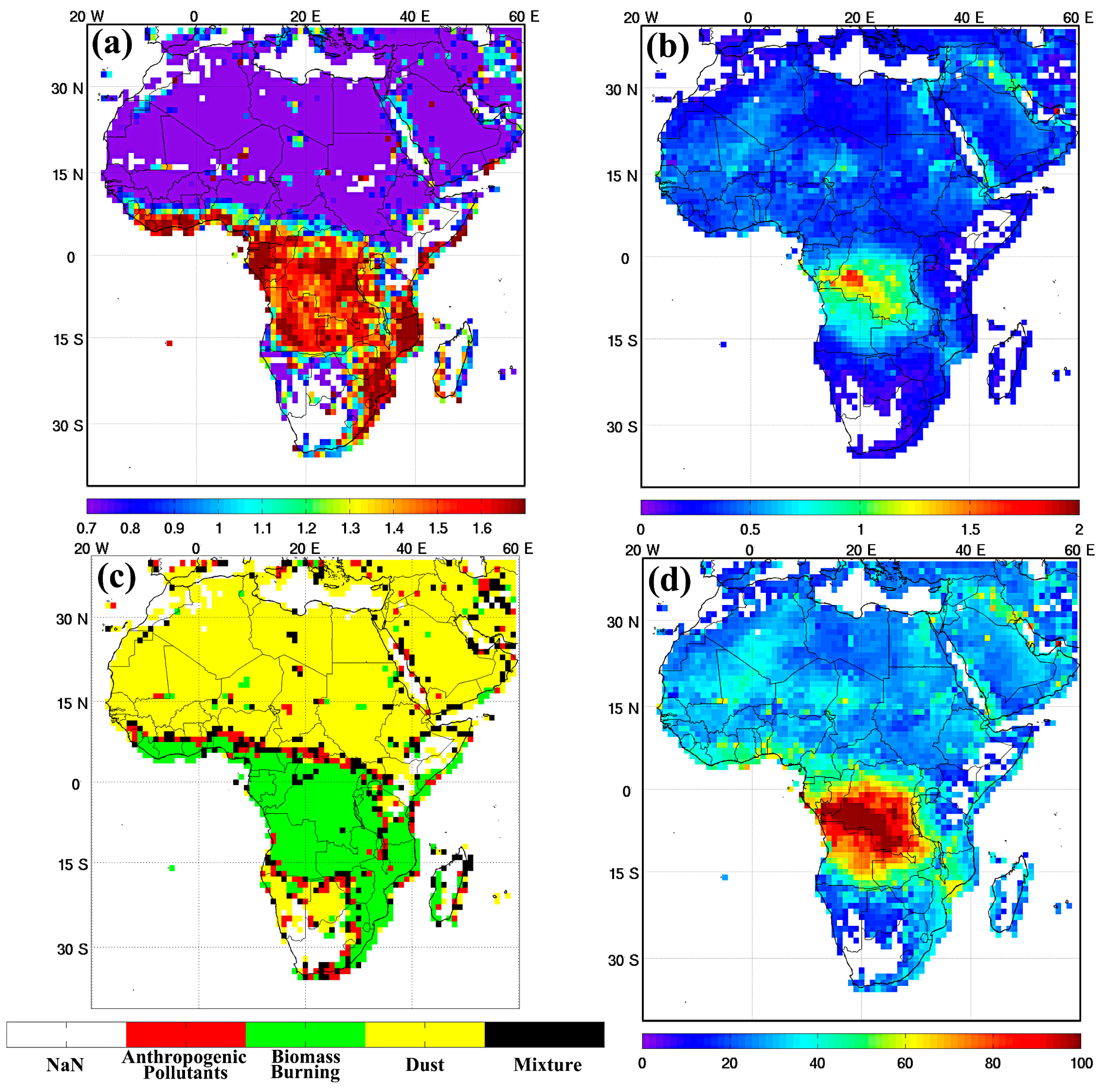
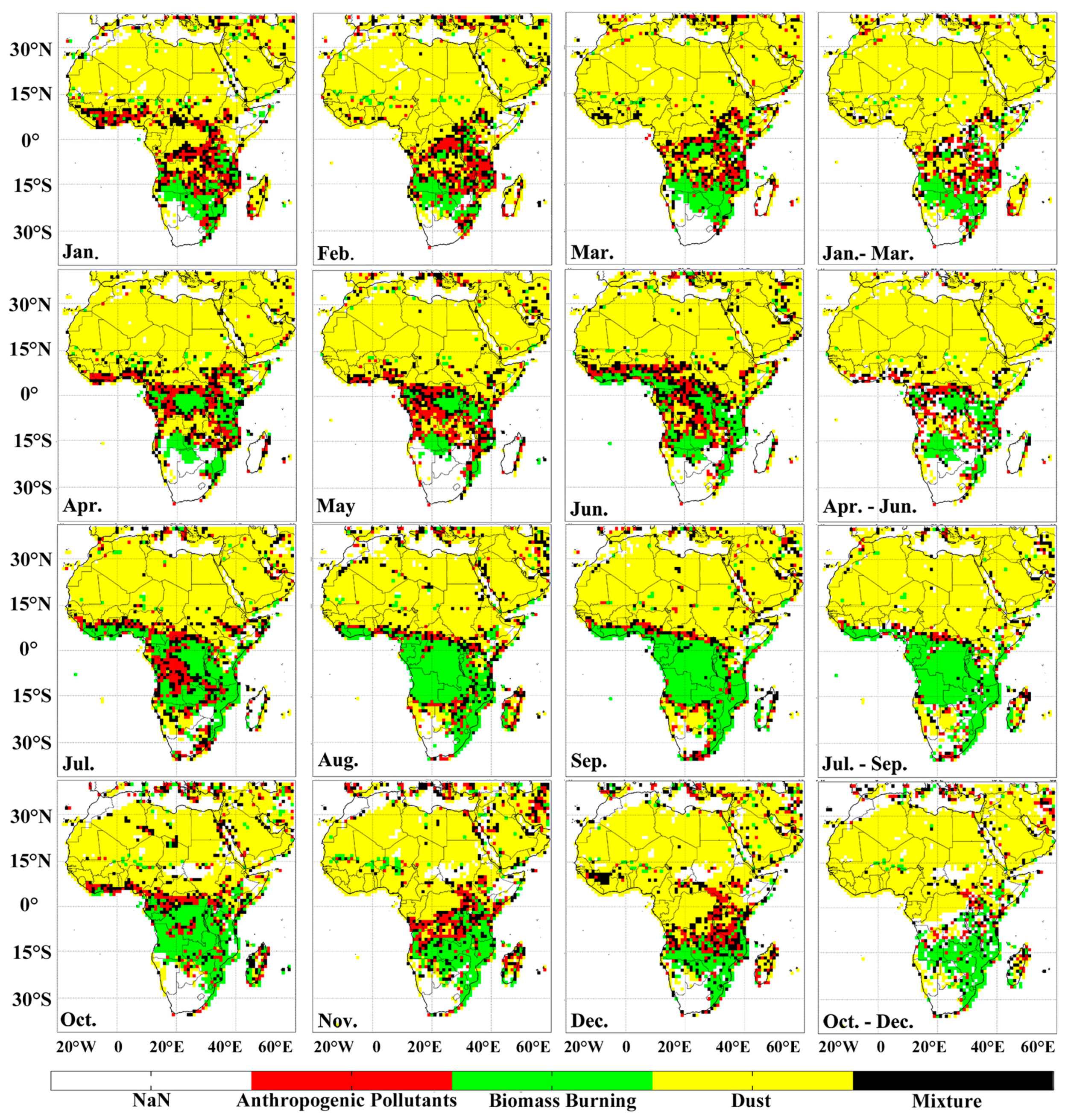
2.2.2. Types of Ambient PM2.5 Assessment
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A



References
- World Health Organization (WHO), Regional Office for Europe. Air Quality Guidelines Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; WHO Regional Office for Europe: Copenhagen, Denmark, 2006; p. 484. [Google Scholar]
- World Health Organization (WHO), Regional Office for Europe. Health Relevance of Particulate Matter from Various Sources; Report on a WHO Workshop; WHO Regional Office for Europe: Copenhagen, Denmark, 2007; p. 21. [Google Scholar]
- World Health Organization. World Health Organization Releases Country Estimates on Air Pollution Exposure and Health Impact. Available online: http://www.who.int/mediacentre/news/releases/2016/air-pollution-estimates/en/ (accessed on 22 December 2016).
- World Health Organization Occupational and Environmental Health Team. Who Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005: Summary of Risk Assessment; World Health Organization: Geneva, Switzerland, 2006; p. 20. [Google Scholar]
- Kloog, I.; Ridgway, B.; Koutrakis, P.; Coull, B.A.; Schwartz, J.D. Long- and short-term exposure to PM2.5 and mortality: Using novel exposure models. Epidemiology 2013, 24, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Zanobetti, A.; Kloog, I.; Coull, B.A.; Koutrakis, P.; Melly, S.J.; Schwartz, J.D. Low-concentration PM2.5 and mortality: Estimating acute and chronic effects in a population-based study. Environ. Health Perspect. 2016, 124, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.R.; Stafoggia, M.; Faustini, A.; Berti, G.; Canova, C.; De Togni, A.; Di Biagio, K.; Gherardi, B.; Giannini, S.; Lauriola, P.; et al. Association between short-term exposure to PM2.5 and PM10 and mortality in susceptible subgroups: A multisite case-crossover analysis of individual effect modifiers. Am. J. Epidemiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Franklin, M.; Zeka, A.; Schwartz, J. Association between PM2.5 and all-cause and specific-cause mortality in 27 US communities. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Farhat, N.; Ramsay, T.; Jerrett, M.; Krewski, D. Short-term effects of ozone and PM2.5 on mortality in 12 Canadian cities. J. Environ. Prot. 2013, 4, 5. [Google Scholar] [CrossRef]
- Lepeule, J.; Laden, F.; Dockery, D.; Schwartz, J. Chronic exposure to fine particles and mortality: An extended follow-up of the Harvard Six Cities Study from 1974 to 2009. Environ. Health Perspect. 2012, 120, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.B.; Rifas-Shiman, S.L.; Litonjua, A.A.; Oken, E.; Gillman, M.W.; Kloog, I.; Luttmann-Gibson, H.; Zanobetti, A.; Coull, B.A.; Schwartz, J.; et al. Lifetime exposure to ambient pollution and lung function in children. Am. J. Respir. Crit. Care Med. 2016, 193, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Khamdan, S.A.; Al Madany, I.M.; Buhussain, E. Temporal and spatial variations of the quality of ambient air in the Kingdom of Bahrain during 2007. Environ. Monit. Assess. 2009, 154, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-H.; Liu, G.-R.; Liu, C.-Y. A novel index for atmospheric aerosol type categorization with spectral optical depths from satellite retrieval. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2016, XLI-B8, 277–279. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Suwa, T.; Hogg, J.C.; Quinlan, K.B.; Ohgami, A.; Vincent, R.; van Eeden, S.F. Particulate air pollution induces progression of atherosclerosis. J. Am. Coll. Cardiol. 2002, 39, 935–942. [Google Scholar] [CrossRef]
- Yue, W.; Schneider, A.; Stolzel, M.; Ruckerl, R.; Cyrys, J.; Pan, X.; Zareba, W.; Koenig, W.; Wichmann, H.E.; Peters, A. Ambient source-specific particles are associated with prolonged repolarization and increased levels of inflammation in male coronary artery disease patients. Mutat. Res. 2007, 621, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Urch, B.; Dvonch, J.T.; Bard, R.L.; Speck, M.; Keeler, G.; Morishita, M.; Marsik, F.J.; Kamal, A.S.; Kaciroti, N.; et al. Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 2009, 54, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulou, V.V.; Kalogeropoulos, A.P.; Psaty, B.M.; Rodondi, N.; Bauer, D.C.; Butler, A.B.; Koster, A.; Smith, A.L.; Harris, T.B.; Newman, A.B.; et al. Lung function and risk for heart failure among older adults: The health abc study. Am. J. Med. 2011, 124, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Sin, D.D.; Wu, L.; Man, S.F. The relationship between reduced lung function and cardiovascular mortality: A population-based study and a systematic review of the literature. Chest 2005, 127, 1952–1959. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.; Knuiman, M.W.; Divitini, M.L.; James, A.; Musk, A.W.; Bartholomew, H.C. Decline in lung function and mortality: The Busselton Health Study. J. Epidemiol. Community Health 1999, 53, 230–234. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health in 2015: From MDGS, Millennium Development Goals to SDGS, Sustainable Development Goals; World Health Organizationa: Geneva, Switzerland, 2015; p. 204. [Google Scholar]
- World Bank. World Development Indicators. Available online: http://databank.worldbank.org/data/home.aspx (accessed on 17 October 2016).
- Levy, R.; Hsu, C. MODIS Atmosphere l2 Aerosol Product; NASA MODIS Adaptive Processing System; Goddard Space Flight Center: Washington, DC, USA, 2015. [Google Scholar]
- Sano, I.; Mukai, M.; Iguchi, N.; Mukai, S. Suspended particulate matter sampling at an urban AERONET site in Japan, Part 2: Relationship between column aerosol optical thickness and PM2.5 concentration. APPRES 2010, 4, 43504. [Google Scholar]
- Hodnebrog, Ø.; Myhre, G.; Forster, P.M.; Sillmann, J.; Samset, B.H. Local biomass burning is a dominant cause of the observed precipitation reduction in Southern Africa. Nat. Commun. 2016, 7, 11236. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M.; Schafer, J.L.; Kam, C.M. A comparison of inclusive and restrictive strategies in modern missing data procedures. Psychol. Methods 2001, 6, 330–351. [Google Scholar] [CrossRef] [PubMed]
- Bolker, B.M.; Brooks, M.E.; Clark, C.J.; Geange, S.W.; Poulsen, J.R.; Stevens, M.H.; White, J.S. Generalized linear mixed models: A practical guide for ecology and evolution. Trends Ecol. Evol. 2009, 24, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Zhang, D. Inference in generalized additive mixed modelsby using smoothing splines. J. R. Stat. Soc. Ser. B Stat. Methodol. 1999, 61, 381–400. [Google Scholar] [CrossRef]
- Nakagawa, S.; Schielzeth, H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Meth. Ecol. Evol. 2013, 4, 133–142. [Google Scholar] [CrossRef]
- World Health Organization Media Centre. Ambient (Outdoor) Air Quality and Health. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/ (accessed on 23 December 2016).
- Rhind, S.M. Anthropogenic pollutants: A threat to ecosystem sustainability? Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2009, 364, 3391–3401. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease. Available online: http://apps.who.int/iris/bitstream/10665/250141/1/9789241511353-eng.pdf (accessed on 13 March 2017).
- Esposito, S.; Tagliabue, C.; Bosis, S. Tuberculosis in children. Mediterr. J. Hematol. Infect. Dis. 2013, 5, e2013064. [Google Scholar] [CrossRef] [PubMed]
- Brochu, P.J.; Yanosky, J.D.; Paciorek, C.J.; Schwartz, J.; Chen, J.T.; Herrick, R.F.; Suh, H.H. Particulate air pollution and socioeconomic position in rural and urban areas of the northeastern united states. Am. J. Public Health 2011, 101 (Suppl. 1), S224–S230. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Northern Africa | Southern Africa | Eastern Africa | Western Africa | Central Africa | p-Value a |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||
| Under-5 deaths | 24,064.0 (23,525.1) | 51,981.9 (53,012.2) | 63,287.3 (76,937.6) | 98,918.9 (203,881) | 63,762.6 (98,947.8) | <0.001 |
| Maternal deaths | 672.4 (511.8) | 2309.6 (2334.5) | 4289.9 (5251.0) | 6116.3 (13,813.6) | 4253.8 (6476.2) | <0.001 |
| Biomass | ||||||
| AOD, τ | 0.34 (0.14) | 0.16 (0.07) | 0.31 (0.14) | 0.36 (0.15) | 0.42 (0.15) | <0.001 |
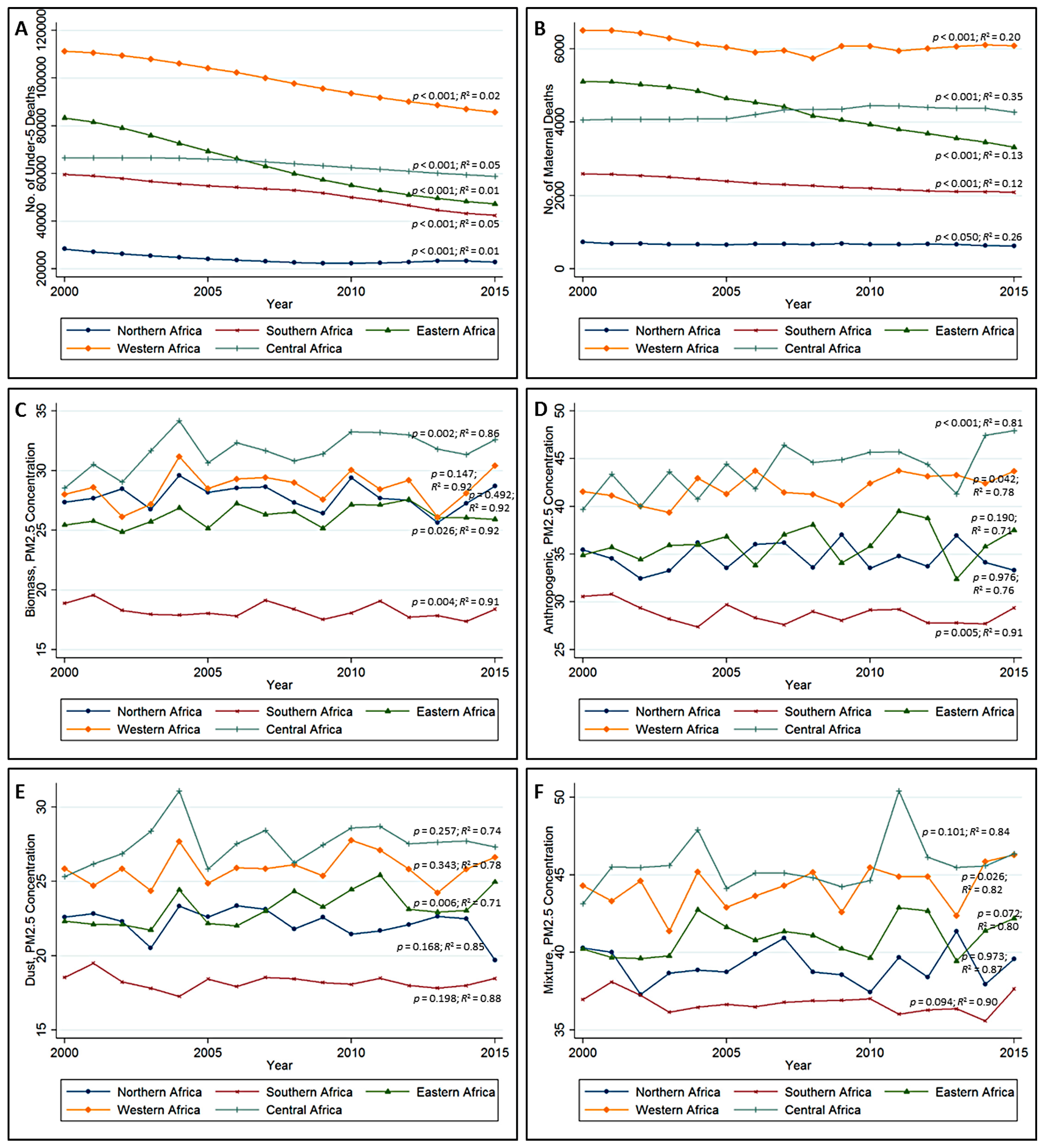
| Jan.–Mar. PM2.5, μg/m3 | 28.57 (10.42) | 19.09 (4.39) | 26.64 (9.60) | 30.72 (10.98) | 34.15 (10.51) | <0.001 |
| Jan.–Jun. PM2.5, μg/m3 | 29.83 (9.02) | 18.33 (4.55) | 27.80 (8.40) | 30.62 (9.42) | 33.63 (8.54) | <0.001 |
| Jan.–Sep. PM2.5, μg/m3 | 29.63 (8.61) | 18.29 (3.79) | 27.29 (7.95) | 29.74 (8.34) | 32.72 (8.27) | <0.001 |
| Jan.–Dec. PM2.5, μg/m3 | 27.82 (7.60) | 18.24 (3.43) | 26.19 (7.60) | 28.58 (8.08) | 31.63 (7.99) | <0.001 |
| Anthropogenic | ||||||
| AOD, τ | 0.20 (0.08) | 0.14 (0.06) | 0.21 (0.10) | 0.27 (0.13) | 0.29 (0.12) | <0.001 |
| Jan.–Mar. PM2.5, μg/m3 | 35.66 (8.94) | 27.11 (5.85) | 35.26 (10.90) | 42.03 (13.81) | 43.95 (14.45) | <0.001 |
| Jan.–Jun. PM2.5, μg/m3 | 37.07 (8.65) | 25.83 (5.06) | 37.67 (11.59) | 43.92 (16.45) | 47.46 (15.78) | <0.001 |
| Jan.–Sep. PM2.5, μg/m3 | 36.02 (7.83) | 28.70 (6.90) | 37.87 (10.18) | 43.54 (13.60) | 45.60 (13.26) | <0.001 |
| Jan.–Dec. PM2.5, μg/m3 | 34.66 (7.59) | 28.74 (6.13) | 36.04 (9.62) | 41.99 (12.87) | 43.89 (12.25) | <0.001 |
| Dust | ||||||
| AOD, τ | 0.24 (0.11) | 0.16 (0.06) | 0.26 (0.12) | 0.31 (0.14) | 0.34 (0.12) | <0.001 |
| Jan.–Mar. PM2.5, μg/m3 | 22.76 (6.43) | 17.93 (2.62) | 22.87 (6.43) | 26.59 (8.66) | 28.40 (6.66) | <0.001 |
| Jan.–Jun. PM2.5, μg/m3 | 23.38 (5.89) | 17.37 (3.02) | 24.19 (6.73) | 27.08 (8.48) | 29.67 (6.85) | <0.001 |
| Jan.–Sep. PM2.5, μg/m3 | 23.02 (5.69) | 18.32 (3.34) | 23.99 (6.73) | 26.61 (7.56) | 28.70 (6.48) | <0.001 |
| Jan.–Dec. PM2.5, μg/m3 | 22.19 (5.69) | 18.23 (2.99) | 23.22 (6.58) | 25.88 (7.27) | 27.55 (6.26) | <0.001 |
| Mixture | ||||||
| AOD, τ | 0.25 (0.11) | 0.17 (0.06) | 0.26 (0.10) | 0.32 (0.14) | 0.35 (0.12) | <0.001 |
| Jan.–Mar. PM2.5, μg/m3 | 39.22 (8.45) | 35.53 (4.29) | 40.13 (7.84) | 44.58 (10.94) | 45.88 (8.28) | <0.001 |
| Jan.–Jun. PM2.5, μg/m3 | 40.39 (8.52) | 34.80 (4.18) | 42.22 (8.63) | 45.53 (10.17) | 47.59 (8.40) | <0.001 |
| Jan.–Sep. PM2.5, μg/m3 | 40.14 (8.56) | 36.63 (5.19) | 42.19 (8.29) | 45.65 (9.42) | 47.10 (8.65) | <0.001 |
| Jan.–Dec. PM2.5, μg/m3 | 39.15 (8.57) | 36.73 (4.78) | 40.96 (8.28) | 44.20 (8.78) | 45.60 (8.47) | <0.001 |
| Total population, million | 31.1 (25.4) | 14.1 (13.6) | 18.8 (21.5) | 18.8 (34.4) | 12.5 (17.8) | <0.001 |
| Urban population, million | 16.4 (10.8) | 5.9 (8.1) | 4.5 (4.4) | 7.4 (14.6) | 4.8 (7.2) | <0.001 |
| Female population, % | 49.73 (0.76) | 50.71 (0.51) | 50.17 (0.60) | 50.19 (0.63) | 50.08 (0.56) | 0.045 |
| Employed population, % | 42.23 (4.87) | 59.53 (13.04) | 62.72 (16.47) | 65.37 (7.74) | 66.33 (9.35) | <0.001 |
| AIDS death, thousand | 65.5 (128.5) | 56.4 (76.8) | 64.4 (105.8) | 19.7 (42.2) | 14.2 (15.2) | <0.001 |
| Tuberculosis death rate, per 100,000 | 6.64 (5.28) | 48.09 (23.12) | 35.00 (28.17) | 37.93 (24.46) | 46.72 (34.16) | <0.001 |
| Undernourished population, million | 0.74 (1.0) | 2.7 (2.7) | 4.8 (8.7) | 2.0 (2.3) | 1.2 (1.6) | 0.129 |
| Anemia in pregnancy, % | 32.76 (3.14) | 38.70 (7.93) | 40.18 (7.73) | 57.28 (6.54) | 53.15 (6.18) | <0.001 |
| Annual mean temperature, °C | 22.20 (2.08) | 21.16 (2.82) | 25.27 (2.32) | 27.04 (1.50) | 24.94 (1.53) | <0.001 |
| Variable | Under-5 Deaths, Unadjusted | Maternal Deaths, Unadjusted |
|---|---|---|
| GLMM, IRR (95% CI) b | GLMM, IRR (95% CI) b | |
| Type of PM2.5 a | ||
| Biomass | 1.02 (1.01, 1.03) **** | 1.07 (1.03, 1.10) **** |
| Anthropogenic | 0.99 (0.99, 1.01) | 1.03 (1.01, 1.04) **** |
| Dust | 1.03 (1.01, 1.06) ** | 0.91 (0.90, 0.92) **** |
| Mixture | 1.01 (1.01, 1.02) **** | 1.07 (1.06, 1.09) **** |
| Sub-regions (ref: North) | ||
| South | 1.74 (0.26, 11.53) | 3.33 (0.42, 26.67) |
| East | 1.39 (0.23, 8.35) | 3.56 (0.49, 25.40) |
| West | 2.48 (0.42, 14.76) | 5.82 (0.82, 41.48) |
| Central | 1.25 (0.18, 8.64) | 3.11 (0.37, 25.95) |
| Year | 0.66 (0.64, 0.68) **** | 0.81 (0.79, 0.82) **** |
| Total population | 0.83 (0.81, 0.85) **** | 1.02 (0.97, 1.05) |
| Urban population | 1.02 (1.00, 1.03) * | 0.99 (0.95, 1.03) |
| Female population | 0.97 (0.92, 1.04) | 1.10 (0.98, 1.24) |
| Employed population | 1.10 (1.06, 1.12) **** | 1.36 (1.33, 1.37) **** |
| AIDS death | 1.02 (0.99, 1.04) | 0.84 (0.78, 0.90) **** |
| Tuberculosis death | 1.11 (1.06, 1.15) **** | 1.37 (1.25, 1.49) **** |
| Undernourished population | 0.91 (0.90, 0.92) **** | 0.78 (0.75, 0.81) **** |
| Anemia in pregnancy | 1.01 (1.00, 1.03) * | 1.03 (0.95, 1.12) |
| Annual mean temperature | 0.98 (0.97, 1.01) | 1.05 (0.96, 1.14) |
| Annual Mean PM2.5 a | Under-5 Deaths, Adjusted Model | Maternal Deaths, Adjusted Model | ||
|---|---|---|---|---|
| GLMM IRR (95% CI) b,c | GAMM Coef. (Se) b | GLMM IRR (95% CI) b,c | GAMM Coef. (Se) b | |
| Overall | ||||
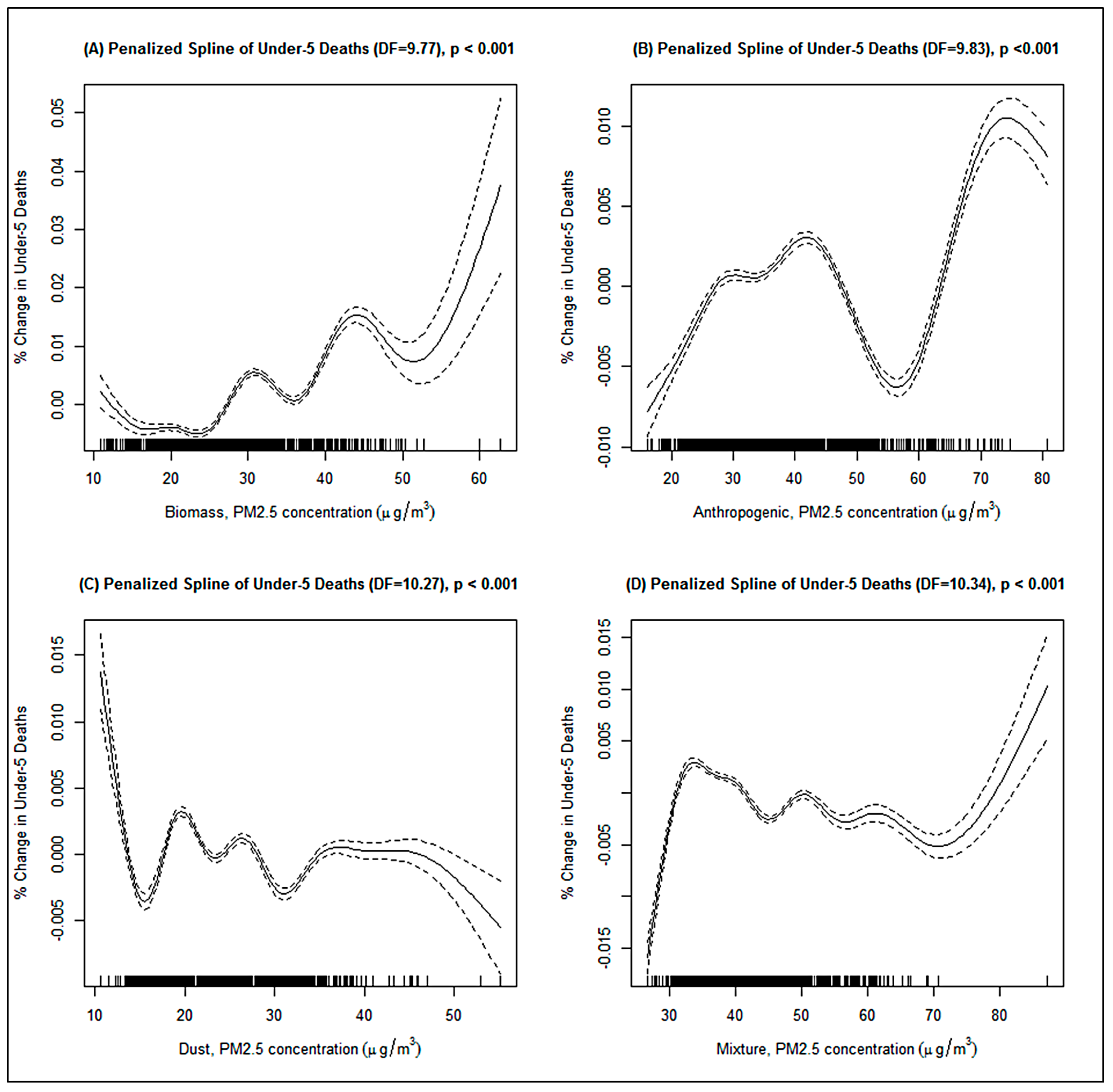
| Biomass | 0.99 (0.98, 1.02) | 0.02 (0.003) **** | 0.94 (0.88, 0.99) * | 0.06 (0.008) **** |
| Anthropogenic | 1.01 (1.01, 1.02) **** | 0.003 (0.0003) **** | 1.03 (1.01, 1.05) ** | 0.04 (0.002) **** |
| Dust | 0.98 (0.97, 0.98) **** | −0.003 (0.0005) **** | 0.93 (0.91, 0.95) **** | −0.08 (0.002) **** |
| Mixture | 0.94 (0.94, 0.94) **** | −0.01 (0.004) **** | 0.95 (0.92, 0.98) *** | 0.004 (0.006) |
| Sub-regions | ||||
| Northern Africa | ||||
| Biomass | 0.90 (0.86, 0.94) **** | −0.05 (0.006) **** | 1.02 (0.72, 1.42) | −0.03 (0.07) |
| Anthropogenic | 1.05 (1.02, 1.08) *** | 0.04 (0.002) **** | 1.10 (1.00, 1.20) * | 0.07 (0.03) ** |
| Dust | 1.03 (1.01, 1.06) ** | 0.03 (0.006) **** | 1.07 (0.96, 1.19) | 0.07 (0.04) |
| Mixture | 0.99 (0.96, 1.02) | 0.01 (0.004) *** | 1.01 (0.90, 1.12) | 0.02 (0.01) |
| Southern Africa | ||||
| Biomass | 1.03 (0.99, 1.05) | 0.03 (0.003) *** | 1.01 (0.93, 1.08) | 0.03 (0.02) |
| Anthropogenic | 0.99 (0.97, 1.01) | −0.03 (0.002) *** | 1.04 (0.94, 1.06) | 0.01 (0.02) |
| Dust | 1.01 (0.99, 1.02) | 0.006 (0.002) ** | 0.98 (0.93, 1.03) | −0.01 (0.02) |
| Mixture | 0.99 (0.95, 0.99) ** | 0.002 (0.003) | 0.96 (0.90, 1.03) | −0.01 (0.02) |
| Eastern Africa | ||||
| Biomass | 0.98 (0.97, 0.99) **** | −0.02 (0.003) **** | 0.95 (0.89, 1.01) | −0.08 (0.01) **** |
| Anthropogenic | 0.99 (0.99, 1.01) | −0.01 (0.001) * | 1.04 (1.02, 1.05) **** | 0.02 (0.006) ** |
| Dust | 1.01 (0.99, 1.04) | −0.01 (0.001) **** | 0.95 (0.93, 0.96) **** | −0.06 (0.01) **** |
| Mixture | 1.00 (0.99, 1.05) | 0.001 (0.001) | 1.06 (1.02, 1.09) *** | 0.04 (0.01) *** |
| Western Africa | ||||
| Biomass | 1.02 (1.01, 1.04) ** | −0.001 (0.003) * | 0.97 (0.91, 1.03) | 0.01 (0.01) |
| Anthropogenic | 1.01 (0.99, 1.02) | 0.002 (0.0004) **** | 1.02 (0.98, 1.06) | 0.03 (0.003) **** |
| Dust | 1.01 (1.01, 1.01) ** | −0.003 (0.0003) **** | 0.94 (0.92, 0.97) **** | −0.05 (0.003) **** |
| Mixture | 1.01 (1.00, 1.02) * | −0.005 (0.0003) **** | 0.93 (0.90, 0.96) **** | −0.04 (0.002) **** |
| Central Africa | ||||
| Biomass | 1.02 (1.02, 1.03) ** | 0.01 (0.002) **** | 1.19 (1.15, 1.23) **** | 0.04 (0.01) **** |
| Anthropogenic | 0.95 (0.99, 0.99) ** | −0.004 (0.01) | 1.00 (0.99, 1.00) | −0.01 (0.01) |
| Dust | 1.10 (1.09, 1.10) **** | −0.002 (0.0005) **** | 0.96 (0.93, 0.99) ** | −0.02 (0.01) ** |
| Mixture | 0.99 (0.99, 0.99) ** | −0.001 (0.001) | 1.00 (0.99, 1.01) | −0.01 (0.01) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owili, P.O.; Lien, W.-H.; Muga, M.A.; Lin, T.-H. The Associations between Types of Ambient PM2.5 and Under-Five and Maternal Mortality in Africa. Int. J. Environ. Res. Public Health 2017, 14, 359. https://doi.org/10.3390/ijerph14040359
Owili PO, Lien W-H, Muga MA, Lin T-H. The Associations between Types of Ambient PM2.5 and Under-Five and Maternal Mortality in Africa. International Journal of Environmental Research and Public Health. 2017; 14(4):359. https://doi.org/10.3390/ijerph14040359
Chicago/Turabian StyleOwili, Patrick Opiyo, Wei-Hung Lien, Miriam Adoyo Muga, and Tang-Huang Lin. 2017. "The Associations between Types of Ambient PM2.5 and Under-Five and Maternal Mortality in Africa" International Journal of Environmental Research and Public Health 14, no. 4: 359. https://doi.org/10.3390/ijerph14040359
APA StyleOwili, P. O., Lien, W.-H., Muga, M. A., & Lin, T.-H. (2017). The Associations between Types of Ambient PM2.5 and Under-Five and Maternal Mortality in Africa. International Journal of Environmental Research and Public Health, 14(4), 359. https://doi.org/10.3390/ijerph14040359