Prospective Analysis of the Influence of Sport and Educational Factors on the Prevalence and Initiation of Smoking in Older Adolescents from Croatia

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
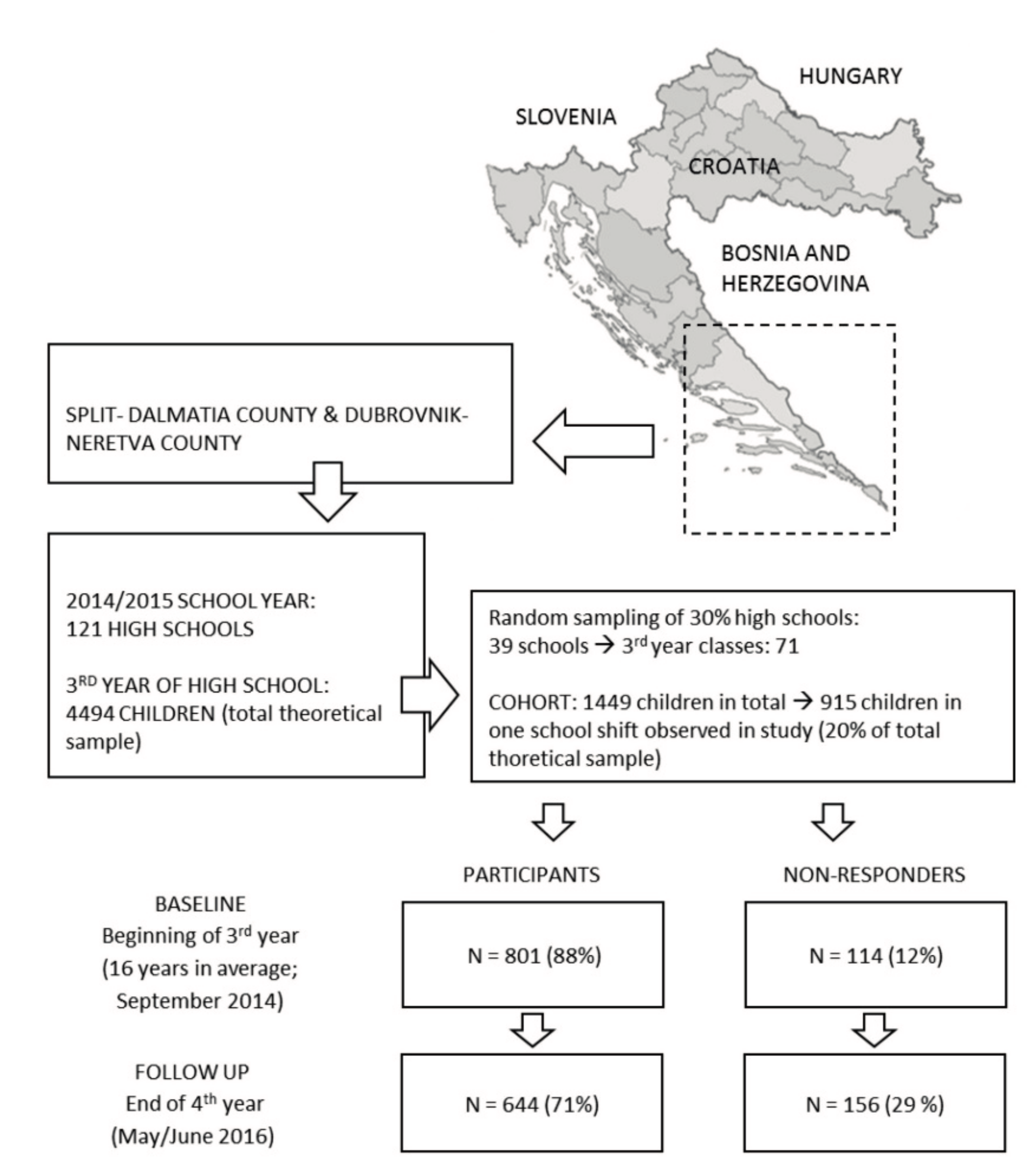
2.1. Participants
2.2. Variables
2.3. Statistics
3. Results
4. Discussion
4.1. Educational Factors and Smoking
4.2. Sport Factors and Smoking
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European School Survey Project on Alcohol and Other Drugs (ESPAD) Report 2015. Available online: http://www.Espad.Org/sites/espad.Org/files/td0116475enn.Pdf (accessed on 19 February 2017).
- European School Survey Project on Alcohol and Other Drugs (ESPAD) Report 2011. Available online: http://www.Espad.Org/sites/espad.Org/files/full-report-supplement-to-the-2011-espad-report-web.Pdf (accessed on 20 February 2017).
- Tahiraj, E.; Cubela, M.; Ostojic, L.; Rodek, J.; Zenic, N.; Sekulic, D.; Lesnik, B. Prevalence and factors associated with substance use and misuse among kosovar adolescents; cross sectional study of scholastic, familial- and sports-related factors of influence. Int. J. Environ. Res. Public Health 2016, 13, 502. [Google Scholar] [CrossRef] [PubMed]
- Idrizovic, K.; Zenic, N.; Tahirajl, E.; Rausavljevic, N.; Sekulic, D. Cigarette smoking among 17–18 years old adolescents—Prevalence and association with sociodemographic, familial, sport and scholastic factors. Med. Pr. 2015, 66, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, D.; Idrizovic, K.; Popovic, S.; Sisic, N.; Sekulic, D.; Ostojic, L.; Spasic, M.; Zenic, N. An examination of the ethnicity-specific prevalence of and factors associated with substance use and misuse: Cross-sectional analysis of Croatian and Bosniak adolescents in Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2016, 13, 968. [Google Scholar] [CrossRef] [PubMed]
- Loubeau, P.R. Selected aspects of tobacco control in Croatia. Central Eur. J. Public Health 2009, 17, 47–52. [Google Scholar]
- Lee, K.J. Current smoking and secondhand smoke exposure and depression among Korean adolescents: Analysis of a national cross-sectional survey. BMJ Open 2014, 4, e003734. [Google Scholar] [CrossRef] [PubMed]
- Gendall, P.; Hoek, J.; Marsh, L.; Edwards, R.; Healey, B. Youth tobacco access: Trends and policy implications. BMJ Open 2014, 4, e004631. [Google Scholar] [CrossRef] [PubMed]
- Mayer, D.; Simetin, I.P.; Rodin, U.; Benjak, T.; Puntaric, E.; Puntaric, I. The impacts of media messaging and age and sex variance on adolescent smoking habits in Croatia. J. Addict. Med. 2015, 9, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, V.; Diamond, P.M.; Spitz, M.R.; Wilkinson, A.V. Smoking initiation among Mexican heritage youth and the roles of family cohesion and conflict. J. Adolesc. Health 2015, 57, 24–30. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, K.; Attonito, J.; Madhivanan, P.; Yi, Q.; Mzayek, F.; Maziak, W. Determinants of cigarette smoking initiation in Jordanian schoolchildren: Longitudinal analysis. Nicotine Tob. Res. 2015, 17, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Kaleta, D.; Makowiec-Dabrowska, T.; Dziankowska-Zaborszczyk, E.; Fronczak, A. Predictors of smoking initiation—Results from the global adult tobacco survey (GATS) in Poland 2009–2010. Ann. Agric. Environ. Med. 2013, 20, 756–766. [Google Scholar] [PubMed]
- Parrinello, C.M.; Isasi, C.R.; Xue, X.N.; Bandiera, F.C.; Cai, J.W.; Lee, D.J.; Navas-Nacher, E.L.; Perreira, K.M.; Salgado, H.; Kaplan, R.C. Risk of cigarette smoking initiation during adolescence among US-born and non-US-born hispanics/latinos: The hispanic community health study/study of latinos. Am. J. Public Health 2015, 105, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Fakhfakh, R.; Jaidane, I.; Hsairi, M.; Ben Hamida, A.M. Cigarette smoking initiation among Tunisian adolescents: Risk and protective factors. Rev. Epidemiol. Sante 2015, 63, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Morin, A.J.; Rodriguez, D.; Fallu, J.S.; Maiano, C.; Janosz, M. Academic achievement and smoking initiation in adolescence: A general growth mixture analysis. Addiction 2012, 107, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Terzic, A.; Rodek, J.; Spasic, M.; Sekulic, D. Gender-specific analyses of the prevalence and factors associated with substance use and misuse among Bosniak adolescents. Int. J. Environ. Res. Public Health 2015, 12, 6626–6640. [Google Scholar] [CrossRef] [PubMed]
- Modric, T.; Zenic, N.; Sekulic, D. Substance use and misuse among 17- to 18-year-old Croatian adolescents: Correlation with scholastic variables and sport factors. Subst. Use Misuse 2011, 46, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Sisic, N.; Terzic, A.; Jasarevic, I.; Ostojic, L.; Pojskic, H.; Zenic, N. Sport and scholastic factors in relation to smoking and smoking initiation in older adolescents: A prospective cohort study in Bosnia and Herzegovina. BMJ Open 2017, 7, e014066. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, J.M.; Lindfors, P.; Rimpela, A.; Salmela-Aro, K.; Rathmann, K.; Perelman, J.; Federico, B.; Richter, M.; Kunst, A.E.; Lorant, V. Academic well-being and smoking among 14- to 17-year-old schoolchildren in six European cities. J. Adolesc. 2016, 50, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Mazur, J.; Tabak, I.; Dzielska, A.; Waz, K.; Oblacinska, A. The relationship between multiple substance use, perceived academic achievements, and selected socio-demographic factors in a Polish adolescent sample. Int. J. Environ. Res. Public Health 2016, 13, 1264. [Google Scholar] [CrossRef] [PubMed]
- Starr, J.M.; Deary, I.J.; Fox, H.C.; Whalley, L.J. Smoking and cognitive change from age 11 to 66 years: A confirmatory investigation. Addict. Behav. 2007, 32, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Whalley, L.J.; Fox, H.C.; Deary, I.J.; Starr, J.M. Childhood IQ, smoking, and cognitive change from age 11 to 64 years. Addict. Behav. 2005, 30, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Anstey, K.J.; von Sanden, C.; Salim, A.; O’Kearney, R. Smoking as a risk factor for dementia and cognitive decline: A meta-analysis of prospective studies. Am. J. Epidemiol. 2007, 166, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Bachman, J.G.; O’Malley, P.M.; Schulenberg, J.E.; Johnston, L.D.; Freedman-Doan, P.; Messersmith, E.E. The Education-Drug Use Connection: How Successes and Failures in School Relate to Adolescent Smoking, Drinking, Drug Use, and Delinquency; Taylor & Francis: Abingdon-on-Thames, UK, 2012. [Google Scholar]
- Zenic, N.; Ostojic, L.; Sisic, N.; Pojskic, H.; Peric, M.; Uljevic, O.; Sekulic, D. Examination of the community-specific prevalence of and factors associated with substance use and misuse among rural and urban adolescents: A cross-sectional analysis in Bosnia and Herzegovina. BMJ Open 2015, 5, e009446. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Ostojic, M.; Ostojic, Z.; Hajdarevic, B.; Ostojic, L. Substance abuse prevalence and its relation to scholastic achievement and sport factors: An analysis among adolescents of the Herzegovina-Neretva canton in Bosnia and Herzegovina. BMC Public Health 2012, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Guo, G. Peer influence on aggressive behavior, smoking, and sexual behavior: A study of randomly-assigned college roommates. J. Health Soc. Behav. 2016, 57, 297–318. [Google Scholar] [CrossRef] [PubMed]
- Filippidis, F.T.; Agaku, I.T.; Vardavas, C.I. The association between peer, parental influence and tobacco product features and earlier age of onset of regular smoking among adults in 27 European countries. Eur. J. Public Health 2015, 25, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Poortinga, W. Associations of physical activity with smoking and alcohol consumption: A sport or occupation effect? Prev. Med. 2007, 45, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Verkooijen, K.T.; Nielsen, G.A.; Kremers, S.P. The association between leisure time physical activity and smoking in adolescence: An examination of potential mediating and moderating factors. Int. J. Behav. Med. 2008, 15, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Werch, C.E. Sport and physical activity participation and substance use among adolescents. J. Adolesc. Health 2005, 36, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Guagliardo, V.; Verger, P.; Pruvost, J.; Mignon, P.; Obadia, Y. Sporting activity and drug use: Alcohol, cigarette and cannabis use among elite student athletes. Addiction 2003, 98, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Bedendo, A.; Noto, A.R. Sports practices related to alcohol and tobacco use among high school students. Rev. Bras. Psiquiatr. 2015, 37, 2. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, D.; Audrain-McGovern, J. Team sport participation and smoking: Analysis with general growth mixture modeling. J. Pediatr. Psychol. 2004, 29, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.M.; Rooney, B.L.; Hannan, P.J.; Peterson, A.V.; Ary, D.V.; Biglan, A.; Botvin, G.J.; Evans, R.I.; Flay, B.R.; Futterman, R.; et al. Intraclass correlation among common measures of adolescent smoking: Estimates, correlates, and applications in smoking prevention studies. Am. J. Epidemiol. 1994, 140, 1038–1050. [Google Scholar] [CrossRef] [PubMed]
- Killip, S.; Mahfoud, Z.; Pearce, K. What is an intracluster correlation coefficient? Crucial concepts for primary care researchers. Ann. Fam. Med. 2004, 2, 204–208. [Google Scholar] [CrossRef]
- Wi, C.I.; Gauger, J.; Bachman, M.; Rand-Weaver, J.; Krusemark, E.; Ryu, E.; King, K.S.; Katusic, S.K.; Juhn, Y.J. Role of individual-housing-based socioeconomic status measure in relation to smoking status among late adolescents with asthma. Ann. Epidemiol. 2016, 26, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.B.; Sun, P.; Johnson, C.A. Socioeconomic correlates of smoking among an ethnically diverse sample of 8th grade adolescents in Southern California. Prev. Med. 2007, 44, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Andreeva, V.A.; Unger, J.B.; Conti, D.V.; Chou, C.P.; Palmer, P.H.; Sun, P.; Johnson, C.A. Age-related smoking progression among adolescents in China. J. Adolesc. Health 2006, 39, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Ostojic, M.; Vasilj, M.; Coric, S.; Zenic, N. Gender-specific predictors of cigarette smoking in adolescents: An analysis of sport participation, parental factors and religiosity as protective/risk factors. J. Subst. Use 2014, 19, 89–94. [Google Scholar] [CrossRef]
- Jessor, R.; Donovan, J.E.; Costa, F.M. Beyond Adolescence: Problem Behaviour and Young Adult Development; Cambridge University Press: Cambridge, UK, 1994. [Google Scholar]
- Goic-Barisic, I.; Bradaric, A.; Erceg, M.; Barisic, I.; Foretic, N.; Pavlov, N.; Tocilj, J. Influence of passive smoking on basic anthropometric characteristics and respiratory function in young athletes. Coll. Antropol. 2006, 30, 615–619. [Google Scholar] [PubMed]


{kind=link}
| Baseline (Model 3) | Follow-Up (Model 3) | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Grade Point Average (cont) | 2.01 * | 1.61–2.55 | 1.59 * | 1.31–1.94 |
| School absence (cont) | 1.40 * | 1.19–1.69 | 1.30 * | 1.08–1.58 |
| Behavioral grade (cont) | 1.80 * | 1.10–2.89 | 1.57 * | 1.03–2.41 |
| Participation in sport | ||||
| Currently involved | Ref | Ref | ||
| Quit | 2.07 * | 1.31–3.32 | 1.66 * | 1.09–2.56 |
| No, never | 0.98 | 0.61–1.59 | 0.87 | 0.56–1.39 |
| Recreation (physical exercising other than sport) | ||||
| Regularly | Ref | Ref | ||
| From time to time | 1.30 | 0.89–2.00 | 1.29 | 0.86–1.92 |
| Not involved | 1.40 | 0.90–2.03 | 1.48 | 0.93–2.35 |
| Experience in sport | ||||
| Never involved | Ref | Ref | ||
| Less than a year | 0.52 * | 0.29–0.89 | 1.04 | 0.52–2.09 |
| 2–5 years | 1.31 | 0.73–2.37 | 1.83 * | 1.09–3.08 |
| More than 5 years | 1.33 | 0.92–1.92 | 1.32 | 0.79–2.20 |
| Achieved result in sport | ||||
| Never involved/Never competed | Ref | Ref | ||
| Regional level | 1.23 | 0.86–1.79 | 1.05 | 0.74–1.51 |
| National/international level ¥ | 1.53 | 0.50–4.68 | 0.22 | 0.05–1.02 |
| Crude | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Grade Point Average (cont) | 0.87 | 0.62–1.22 | 1.03 | 0.72–1.48 | 1.03 | 0.72–1.48 | 1.00 | 0.69–1.45 |
| School absence (cont) | 1.22 | 0.91–1.66 | 1.21 | 0.89–1.65 | 1.21 | 0.89–1.65 | 1.19 | 0.87–1.63 |
| Behavioral grade (cont) | 0.57 | 0.21–1.55 | 0.95 | 0.34–2.69 | 0.95 | 0.34–2.69 | 0.85 | 0.29–2.45 |
| Participation in sport | ||||||||
| Currently involved | Ref | Ref | Ref | Ref | ||||
| Quit | 1.05 | 0.53–2.10 | 0.79 | 0.38–1.63 | 0.79 | 0.38–1.63 | 0.76 | 0.37–1.59 |
| No, never | 0.95 | 0.48–1.89 | 0.70 | 0.34–1.44 | 0.70 | 0.34–1.44 | 0.69 | 0.34–1.44 |
| Recreation (physical exercising other than sport) | ||||||||
| Regularly | Ref | Ref | Ref | Ref | ||||
| From time to time | 2.41 * | 1.15–5.07 | 1.91 | 0.89–4.12 | 1.94 | 0.89–4.19 | 1.92 | 0.89–4.15 |
| Not involved | 2.10 | 0.92–4.80 | 1.57 | 0.67–3.67 | 1.58 | 0.67–3.69 | 1.58 | 0.67–3.71 |
| Experience in sport | ||||||||
| Never involved | Ref | Ref | Ref | Ref | ||||
| Less than a year | 0.26 | 0.05–1.25 | 0.25 | 0.05–1.19 | 0.25 | 0.05–1.19 | 0.22 | 0.05–1.09 |
| 2–5 years | 1.23 | 0.59–2.57 | 1.30 | 0.61–2.78 | 1.31 | 0.61–2.81 | 1.27 | 0.59–2.72 |
| More than 5 years | 0.71 | 0.34–1.45 | 0.88 | 0.42–1.87 | 0.89 | 0.42–1.88 | 0.89 | 0.42–1.89 |
| Achieved result in sport | ||||||||
| Never involved/Never competed | Ref | Ref | Ref | Ref | ||||
| Regional level | 0.62 | 0.35–1.08 | 0.63 | 0.35–1.12 | 0.63 | 0.35–1.12 | 0.64 | 0.36–1.16 |
| National/international level ¥ | 0.42 * | 0.18–0.91 | 0.45 * | 0.21–0.90 | 0.45 * | 0.21–0.90 | 0.45 * | 0.21–0.91 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zenic, N.; Ban, D.; Jurisic, S.; Cubela, M.; Rodek, J.; Ostojic, L.; Jelicic, M.; Bianco, A.; Sekulic, D. Prospective Analysis of the Influence of Sport and Educational Factors on the Prevalence and Initiation of Smoking in Older Adolescents from Croatia. Int. J. Environ. Res. Public Health 2017, 14, 446. https://doi.org/10.3390/ijerph14040446
Zenic N, Ban D, Jurisic S, Cubela M, Rodek J, Ostojic L, Jelicic M, Bianco A, Sekulic D. Prospective Analysis of the Influence of Sport and Educational Factors on the Prevalence and Initiation of Smoking in Older Adolescents from Croatia. International Journal of Environmental Research and Public Health. 2017; 14(4):446. https://doi.org/10.3390/ijerph14040446
Chicago/Turabian StyleZenic, Natasa, Djivo Ban, Sanja Jurisic, Mladen Cubela, Jelena Rodek, Ljerka Ostojic, Mario Jelicic, Antonino Bianco, and Damir Sekulic. 2017. "Prospective Analysis of the Influence of Sport and Educational Factors on the Prevalence and Initiation of Smoking in Older Adolescents from Croatia" International Journal of Environmental Research and Public Health 14, no. 4: 446. https://doi.org/10.3390/ijerph14040446
APA StyleZenic, N., Ban, D., Jurisic, S., Cubela, M., Rodek, J., Ostojic, L., Jelicic, M., Bianco, A., & Sekulic, D. (2017). Prospective Analysis of the Influence of Sport and Educational Factors on the Prevalence and Initiation of Smoking in Older Adolescents from Croatia. International Journal of Environmental Research and Public Health, 14(4), 446. https://doi.org/10.3390/ijerph14040446