
Spatial Analysis of Ambient PM2.5 Exposure and Bladder Cancer Mortality in Taiwan

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
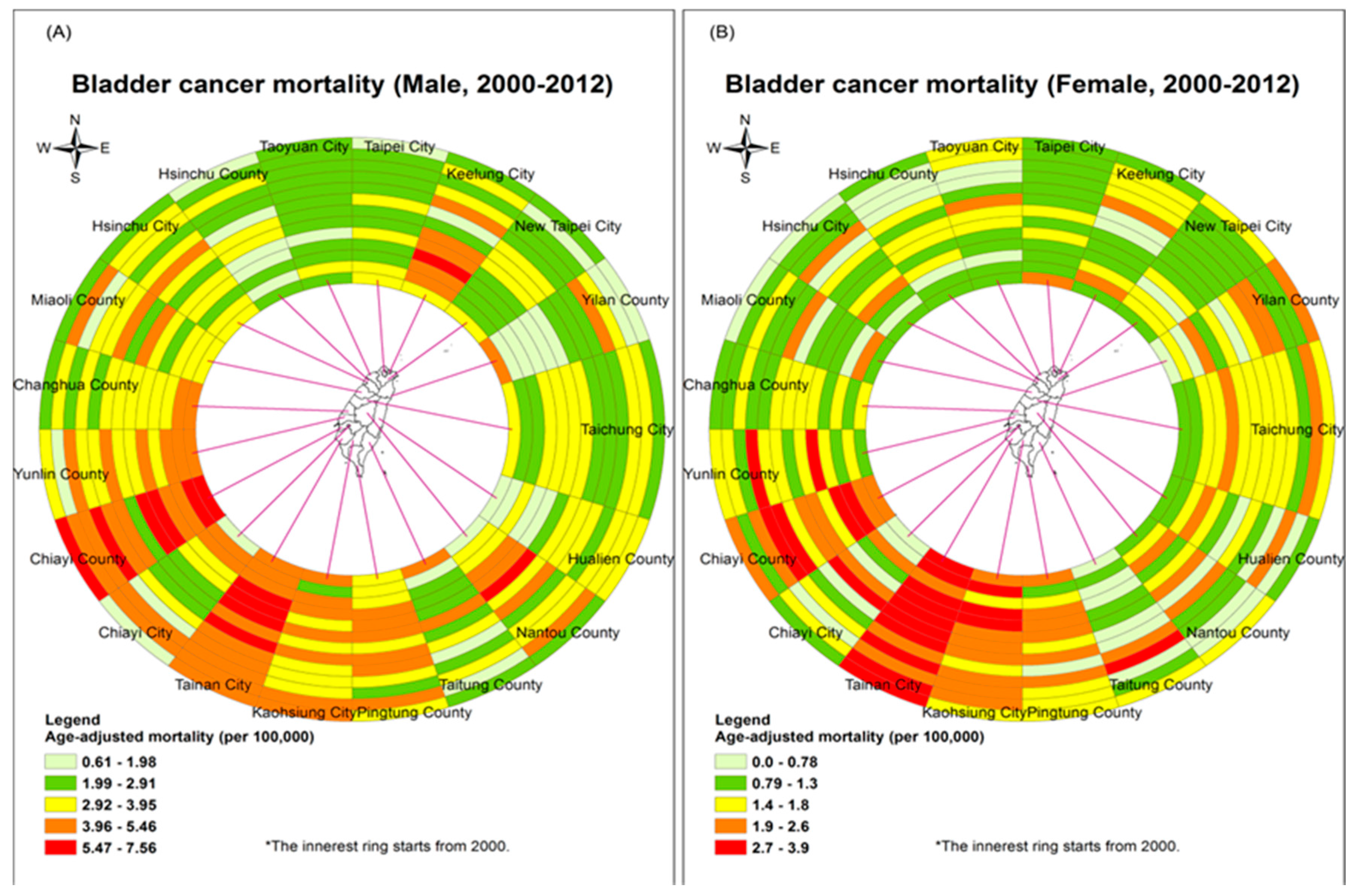
2.1. Age-Adjusted Mortality Rates
2.2. Smoking Rates
2.3. PM2.5 Concentration
2.4. Density of Health Care Facilities
2.5. Area Deprivation Index (ADI)
2.6. Percentage of Aboriginal and Elderly Population
2.7. Percentage of Workers in Textile Industry
2.8. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Coefficient | S.E. | p-Value | VIF |
|---|---|---|---|---|
| Male | ||||
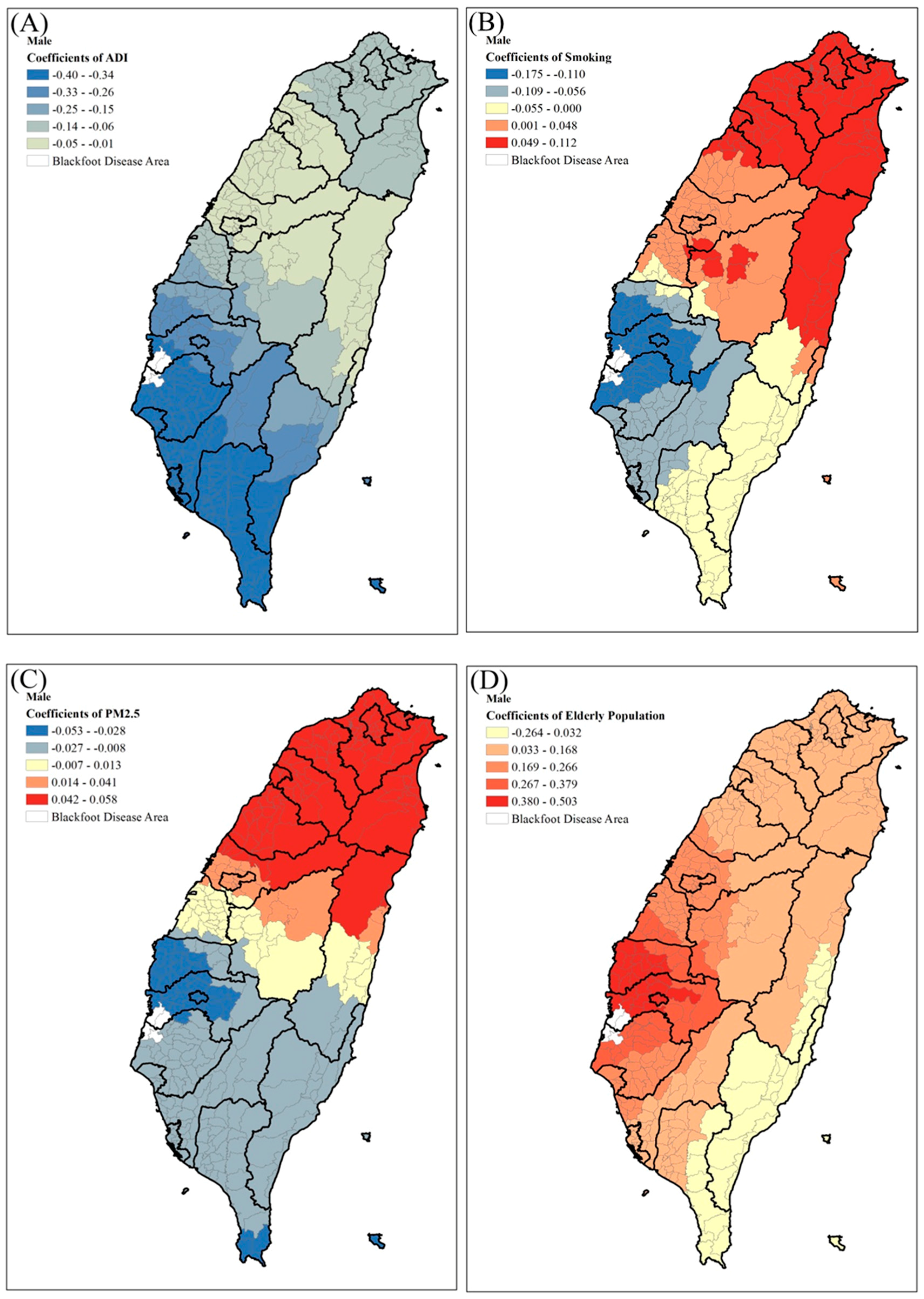
| Area deprivation index | −0.192 | 0.078 | 0.014 * | 1.267 |
| Lung cancer mortality | 0.042 | 0.012 | <0.001 * | 1.145 |
| PM2.5 concentration (μg/m3) | 0.048 | 0.012 | <0.001 * | 1.163 |
| Aborigines (%) | −0.008 | 0.004 | 0.043 * | 1.293 |
| Health care facilities (per km2) | 0.003 | 0.006 | 0.067 | 1.159 |
| Workers in textile industry (%) | −0.029 | 0.021 | 0.168 | 1.212 |
| Elderly population (%, age ≥ 65) | 0.185 | 0.065 | 0.004 * | 1.224 |
| Adjusted R-square | 11.7% | |||
| Female | ||||
| Area deprivation index | −0.049 | 0.049 | 0.314 | 1.442 |
| Lung cancer mortality | 0.058 | 0.013 | <0.001 * | 1.217 |
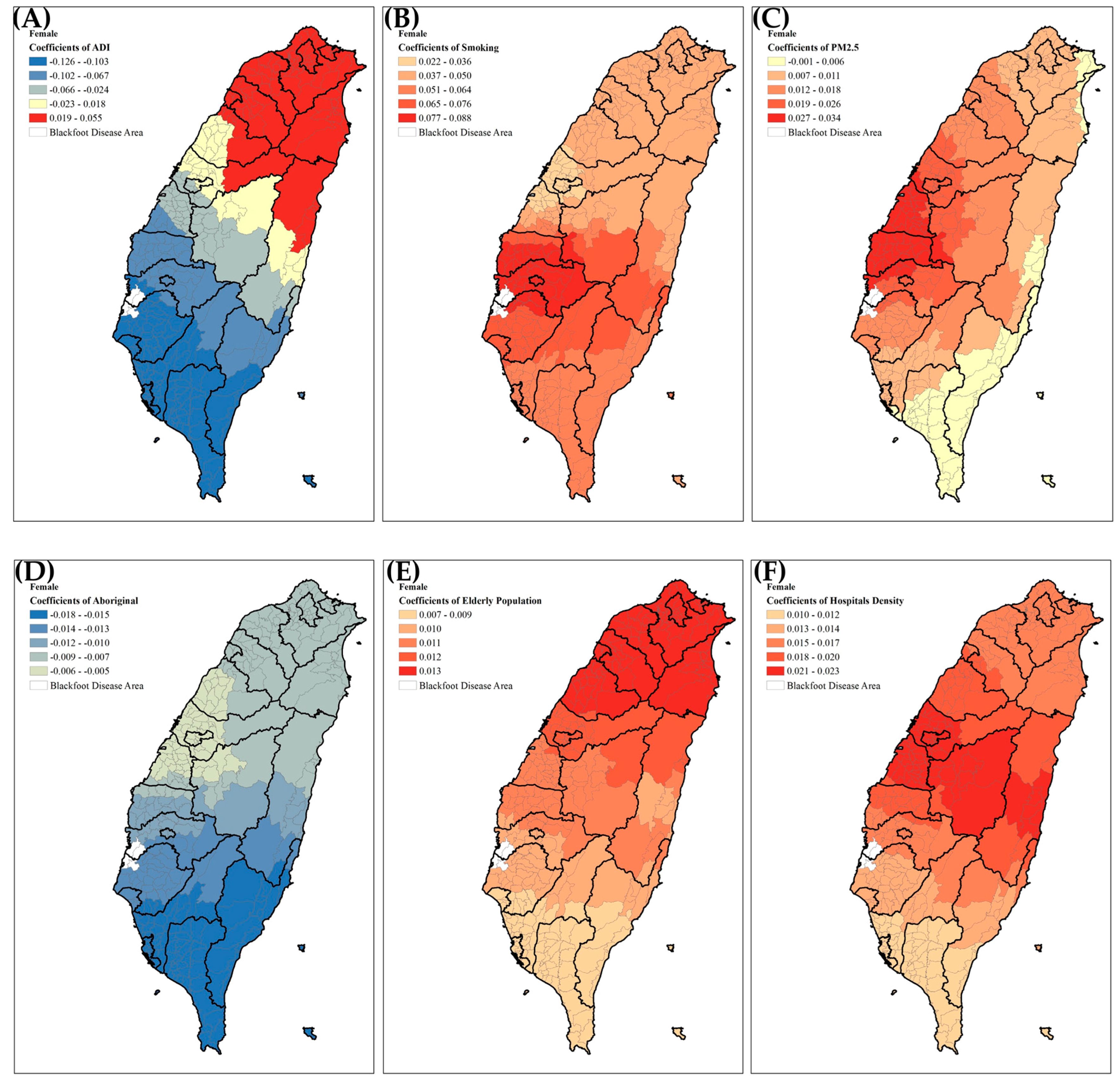
| PM2.5 concentration (μg/m3) | 0.026 | 0.008 | <0.001 * | 1.194 |
| Aborigines (%) | −0.015 | 0.003 | <0.001 * | 1.513 |
| Health care facilities (per km2) | 0.010 | 0.004 | 0.019 * | 1.135 |
| Workers in textiles industry (%) | 0.000 | 0.013 | 0.975 | 1.158 |
| Elderly population (%, age ≥ 65) | 0.016 | 0.027 | 0.567 | 1.446 |
| Adjusted R-square | 17% | |||
| Variables | N | 1st Quartile | Median | 3rd Quartile | R. STD. |
|---|---|---|---|---|---|
| Male | |||||
| Area deprivation index | 348 | −0.330 | −0.135 | −0.058 | 0.201 |
| Lung cancer mortality | 348 | 0.017 | 0.045 | 0.069 | 0.039 |
| PM2.5 concentration (μg/m3) | 348 | −0.016 | 0.003 | 0.061 | 0.057 |
| Aborigines (%) | 348 | −0.015 | −0.012 | −0.010 | 0.004 |
| Health care facilities (per km2) | 348 | −0.006 | −0.001 | 0.016 | 0.016 |
| Workers in textiles industry (%) | 348 | −0.038 | −0.021 | 0.046 | 0.062 |
| Elderly population (%, age ≥ 65) | 348 | −0.141 | 0.091 | 0.213 | 0.262 |
| Adjusted R-square | 21.5% | ||||
| Female | |||||
| Area deprivation index | 348 | −0.088 | −0.044 | 0.023 | 0.083 |
| Lung cancer mortality | 348 | 0.049 | 0.050 | 0.054 | 0.003 |
| PM2.5 concentration (μg/m3) | 348 | 0.002 | 0.008 | 0.016 | 0.010 |
| Aborigines (%) | 348 | −0.018 | −0.012 | −0.011 | 0.005 |
| Health care facilities (per km2) | 348 | 0.013 | 0.015 | 0.018 | 0.004 |
| Workers in textile industry (%) | 348 | −0.002 | −0.001 | 0.003 | 0.004 |
| Elderly population (%, age ≥ 65) | 348 | 0.009 | 0.010 | 0.010 | 0.001 |
| Adjusted R-square | 22.5% | ||||
References
- Brown, J.S.; Gordon, T.; Price, O.; Asgharian, B. Thoracic and respirable particle definitions for human health risk assessment. Part. Fibre Toxicol. 2013, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Particulate Matter: Basic Information. U.S. Environmental Protection Agency. Available online: https://www.epa.gov/pm-pollution (accessed on 26 March 2017).
- Yang, H.H.; Lee, S.A.; Hsieh, D.P.; Chao, M.R.; Tunq, C.Y. PM2.5 and associated polycyclic aromatic hydrocarbon and mutagenicity emissions from motorcycles. Bull Environ. Contam. Toxicol. 2008, 81, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.Y.; Ding, H.; Jiang, L.N.; Chen, S.W.; Zheng, J.P.; Qiu, M.; Zhou, Y.X.; Chen, Q.; Guan, W.J. Association between air pollutants and asthma emergency room visits and hospital admissions in time series studies: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.K.; Chen, C.F.; Yeh, H.C.; Wang, Y.C. Emergency room visits associated with particulate concentration and Asian dust storms in metropolitan Taipei. J. Expo. Sci. Environ. Epidemiol. 2015, 26, 189–196. [Google Scholar] [CrossRef] [PubMed]
- DeFranco, E.; Hall, E.; Hossain, M.; Chen, A.; Haynes, E.N.; Jones, D.; Ren, S.; Lu, L.; Muglia, L. Air pollution and stillbirth risk: Exposure to airborne particulate matter during pregnancy is associated with fetal death. PLoS ONE 2015, 10, e0120594. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Kashima, S.; Doi, H. Associations of acute exposure to fine and coarse particulate matter and mortality among older people in Tokyo, Japan. Sci. Total Environ. 2016, 542, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Thurston, G.D.; Ahn, J.; Cromar, K.R.; Shao, Y.; Reynolds, H.R.; Jerrett, M.; Lim, C.C.; Shanley, R.; Park, Y.; Hayes, R.B. Ambient particulate matter air pollution exposure and mortality in the NIH-AARP diet and health cohort. Environ. Health Perspect. 2015, 124, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Adar, S.D.; Filigrana, P.A.; Clements, N.; Peel, J.L. Ambient coarse particulate matter and human health: A systematic review and meta-analysis. Curr. Environ. Health Rep. 2014, 1, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Castano-Vinyals, G.; Cantor, K.P.; Malats, N.; Tardon, A.; Garcia-Closas, R.; Serra, C.; Carrato, A.; Rothman, N.; Vermeulen, R.; Silverman, D.; et al. Air pollution and risk of urinary bladder cancer in a case-control study in Spain. Occup. Environ. Med. 2008, 65, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Tsai, S.S.; Chiu, H.F.; Wu, T.N.; Chen, C.C.; Yang, C.Y. Ambient exposure to criteria air pollutants and risk of death from bladder cancer in Taiwan. Inhal. Toxicol. 2009, 21, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, Y.; Assuncao, J.V.; Barrozo, L.V. The Impact of atmospheric particulate matter on cancer incidence and mortality in the city of Sao Paulo, Brazil. Cad. Saude Publica 2012, 28, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.D.; Prasad, S.M.; Patel, A.R.; Weiner, A.B.; Pariser, J.J.; Razmaria, A.; Maene, C.; Schuble, T.; Pierce, B.; Steinberg, G.D. Bladder cancer mortality in the United States: A geographic and temporal analysis of socioeconomic and environmental factors. J. Urol. 2015, 195, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Zeegers, M.P.A.; Swaen, G.M.H.; Kant, I.; Goldbohm, R.A.; van den Brandt, P.A. Occupational risk factors for male bladder cancer: Results from a population based case cohort study in The Netherlands. Occup. Environ. Med. 2001, 58, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Burstyn, I.; Kromhout, H.; Johansen, C.; Langard, S.; Kauppinen, T.; Shaham, J.; Ferro, G.; Boffetta, P. Bladder cancer incidence and exposure to polycyclic aromatic hydrocarbons among asphalt pavers. Occup. Environ. Med. 2007, 64, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, G.; Fedeli, U.; Fadda, E.; Milan, G.; Lange, J.H. Epidemiologic evidence of cancer risk in textile industry workers: A review and update. Toxicol. Ind. Health 2002, 18, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Malats, N.; Real, F.X. Epidemiology of bladder cancer. Hematol. Oncol. Clin. N. Am. 2015, 29, 177–189. [Google Scholar]
- Administration of Health Promotion, Ministry of Health and Welfare, ROC (Taiwan). Cancer Registration: Online Interactive Query System. Available online: http://cris.hpa.gov.tw (accessed on 10 August 2015).
- Chan, T.C.; Wang, C.M.; Lee, Y.M. Looking at Temporal Changes-Use This Python Tool for Creating Ring Maps; ArcUser: Redlands, CA, USA, 2013; pp. 42–44. [Google Scholar]
- Administration of Health Promotion, Ministry of Health and Welfare, ROC (Taiwan). Adult Smoking Behavior Surveillance System. Available online: http://www.mohw.gov.tw/CHT/DOS/DisplayStatisticFile.aspx?d=12043&s=1 (accessed on 10 August 2015).
- Chan, T.C.; Chiang, P.H.; Su, M.D.; Wang, H.W.; Liu, M.S. Geographic Disparity in Chronic Obstructive Pulmonary Disease (COPD) mortality rates among the Taiwan population. PLoS ONE 2014, 9, e0098170. [Google Scholar] [CrossRef] [PubMed]
- Pilz, J.; Spock, G. Why do we need and how should we implement Bayesian kriging methods. Stoch. Environ. Res. Risk Assess. 2008, 22, 621–632. [Google Scholar] [CrossRef]
- Lee, Y.C.; Huang, Y.T.; Tsai, Y.W.; Huang, S.M.; Kuo, K.N.; Mckee, M.; Nolte, E. The impact of universal national health insurance on population health: The experience of Taiwan. BMC Health Serv. Res. 2010, 10, 225. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.C.; Lin, H.C.; Chiang, T.L. Area deprivation, socioeconomic status, and smoking behavior among male adults in Taiwan. Taiwan J. Public Health 2003, 22, 10–16. [Google Scholar]
- Directorate General of Budget, Accounting and Statistics, Executive Yuan, ROC (Taiwan). The Industry, Commerce and Service Census. Available online: http://www.dgbas.gov.tw/ct_view.asp?xItem=37563&ctNode=3267 (accessed on 10 August 2015).
- Ministry of the Interior, ROC (Taiwan). The Social-Economic Database System. Available online: http://210.65.89.57/STAT/Web/Portal/STAT_PortalHome.aspx (accessed on 10 August 2015).
- Dijkstra, A.; Janssen, F.; De Bakker, M.; Bos, J.; Lub, R.; Van Wissen, L.J.; Hak, E. Using spatial analysis to predict health care use at the local level: A case study of type 2 diabetes medication use and its association with demographic change and socioeconomic status. PLoS ONE 2013, 8, e0072730. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, A.S.; Brunsdon, C. Local forms of spatial analysis. Geogr. Anal. 1999, 31, 340–358. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M. Geographically weighted regression: A method for exploring spatial nonstationarity. Geogr. Anal. 1996, 28, 281–289. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Nakaya, T.; Fotheringham, A.S.; Charlton, M.; Brunsdon, C. Semiparametric Geographically Weighted Generalised Linear Modelling in GWR 4.0. Available online: http://eprints.maynoothuniversity.ie/4846/1/MC_Semiparametric.pdf (accessed on 2 August 2015).
- Nakaya, T.; Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically weighted poisson regression for disease association mapping. Stat. Med. 2005, 24, 2695–2717. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Bladder Cancer. Available online: http://www.cancer.org/acs/groups/cid/documents/webcontent/003085-pdf.pdf (accessed on 1 August 2016).
- Van Osch, F.H.; Jochems, S.H.; van Schooten, F.J.; Bryan, R.T.; Zeegers, M.P. Significant role for lifetime cigarette smoking in worsening bladder cancer and upper tract urothelial carcinoma prognosis: A meta-analysis. J. Urol. 2015, 195, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Colli, J.; Lee, B.R.; Thomas, R. Population densities in relation to bladder cancer mortality rates in America from 1950 to 1994. Int. Urol. Nephrol. 2012, 44, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Li, H.C.; Hsiao, Y.L.; Tang, C.H.; Jian, W.S.; Miao, N.F. Doctor shopping behavior among cancer patients: A nationwide population-based study in Taiwan. J. Exp. Clin. Med. 2013, 5, 172–176. [Google Scholar] [CrossRef]
- Li, T.; Cao, S.; Fan, D.; Zhang, Y.; Wang, B.; Zhao, X.; Duan, X. Household concentrations and personal exposure of PM2.5 among urban residents using different cooking fuels. Sci. Total Environ. 2016, 548, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Chiang, P.H.; Chen, C.W.; Hsieh, D.P.; Chan, T.C.; Chiang, H.C.; Wen, C.P. Lung cancer risk in females due to exposures to PM2.5 in Taiwan. Open Epidemiol. J. 2014, 7, 6–16. [Google Scholar] [CrossRef]
- Janssen, N.A.; Lanki, T.; Hoek, G.; Vallius, M.; de Hartog, J.J.; Van Grieken, R.; Pekkanen, J.; Brunekreef, B. Associations between ambient, personal, and indoor exposure to fine particulate matter constituents in Dutch and Finnish panels of cardiovascular patients. Occup. Environ. Med. 2005, 62, 868–877. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.N.; Wang, S.M.; Chen, P.C.; Chen, Y.Y.; Wang, J.D. Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010, 102, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Dickman, K.G.; Moriya, M.; Zavadil, J.; Sidorenko, V.S.; Edwards, K.L.; Pu, Y.S. Aristolochic acid-associated urothelial cancer in Taiwan. Proc. Natl. Acad. Sci. USA 2012, 109, 8241–8246. [Google Scholar] [CrossRef] [PubMed]
- Tuccori, M.; Filion, K.B.; Yin, H.; Oriana, H.Y.; Platt, R.W.; Azoulay, L. Pioglitazone use and risk of bladder cancer: Population based cohort study. BMJ 2016, 352, i1541. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, P.; Heintjes, E.M.; Williams, R.; Hoti, F.; Christopher, S.; Majak, M.; Bahmanyar, S. Pioglitazone use and risk of bladder cancer in patients with type 2 diabetes: Retrospective cohort study using datasets from four European countries. BMJ 2016, 354, i3903. [Google Scholar] [CrossRef] [PubMed]
- Al-Zalabani, A.H.; Stewart, K.F.; Wesselius, A.; Schols, A.M.; Zeegers, M.P. Modifiable risk factors for the prevention of bladder cancer: A systematic review of meta-analyses. Eur. J. Epidemiol. 2016, 31, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Washio, M.; Mori, M.; Mikami, K.; Miki, T.; Watanabe, Y.; Nakao, M.; Tamakoshi, A. Risk factors for upper and lower urinary tract cancer death in a Japanese population: Findings from the Japan collaborative cohort study for evaluation of cancer risk. Asian Pac. J. Cancer Prev. APJCP 2016, 17, 3545. [Google Scholar] [PubMed]
- Sun, J.W.; Zhao, L.G.; Yang, Y.; Ma, X.; Wang, Y.Y.; Xiang, Y.B. Obesity and risk of bladder cancer: A dose-response meta-analysis of 15 cohort studies. PLoS ONE 2015, 10, e0119313. [Google Scholar] [CrossRef] [PubMed]






| Variables | Coefficient | S.E. | p-Value | VIF |
|---|---|---|---|---|
| Male | ||||
| Area deprivation index | −0.181 | 0.079 | 0.022 * | 1.267 |
| Smoking rates (%) | 0.050 | 0.034 | 0.146 | 1.551 |
| PM2.5 concentration (μg/m3) | 0.045 | 0.012 | <0.001 * | 1.155 |
| Aborigines (%) | −0.010 | 0.004 | 0.020 * | 1.307 |
| Health care facilities (per km2) | 0.003 | 0.007 | 0.708 | 1.227 |
| Workers in textile industry (%) | 0.006 | 0.022 | 0.805 | 1.364 |
| Elderly population (%, age ≥ 65) | 0.172 | 0.067 | 0.011 * | 1.289 |
| Adjusted R-square | 9.2% | |||
| Female | ||||
| Area deprivation index | −0.062 | 0.050 | 0.216 | 1.451 |
| Smoking rates (%) | 0.064 | 0.039 | 0.100 | 2.294 |
| PM2.5 concentration (μg/m3) | 0.036 | 0.010 | 0.001 * | 2.042 |
| Aborigines (%) | −0.011 | 0.003 | <0.001 * | 1.332 |
| Health care facilities (per km2) | 0.010 | 0.004 | 0.021 * | 1.144 |
| Workers in textiles industry (%) | 0.008 | 0.013 | 0.566 | 1.234 |
| Elderly population (%, age ≥ 65) | 0.025 | 0.028 | 0.381 | 1.480 |
| Adjusted R-square | 13.2% | |||
| Variables | N | 1st Quartile | Median | 3rd Quartile | R. STD. |
|---|---|---|---|---|---|
| Male | |||||
| Area deprivation index | 348 | −0.363 | −0.114 | −0.068 | 0.219 |
| Smoking rates (%) | 348 | −0.070 | 0.022 | 0.061 | 0.097 |
| PM2.5 concentration (μg/m3) | 348 | −0.020 | −0.002 | 0.056 | 0.056 |
| Aborigines (%) | 348 | −0.017 | −0.016 | −0.013 | 0.003 |
| Health care facilities (per km2) | 348 | −0.005 | 0.007 | 0.013 | 0.013 |
| Workers in textiles industry (%) | 348 | −0.024 | −0.014 | 0.011 | 0.026 |
| Elderly population (%, age ≥ 65) | 348 | 0.121 | 0.143 | 0.230 | 0.081 |
| Adjusted R-square | 16.2% | ||||
| Female | |||||
| Area deprivation index | 348 | −0.113 | −0.060 | 0.028 | 0.105 |
| Smoking rates (%) | 348 | 0.042 | 0.052 | 0.065 | 0.017 |
| PM2.5 concentration (μg/m3) | 348 | 0.007 | 0.012 | 0.022 | 0.011 |
| Aborigines (%) | 348 | −0.015 | −0.009 | −0.008 | 0.005 |
| Health care facilities (per km2) | 348 | 0.013 | 0.015 | 0.018 | 0.004 |
| Workers in textile industry (%) | 348 | 0.005 | 0.008 | 0.016 | 0.008 |
| Elderly population (%, age ≥ 65) | 348 | 0.009 | 0.011 | 0.012 | 0.003 |
| Adjusted R-square | 20% | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, H.-L.; Hsu, S.-W.; Chang, Y.-C.; Chan, T.-C.; Tsou, H.-C.; Chang, Y.-C.; Chiang, P.-H. Spatial Analysis of Ambient PM2.5 Exposure and Bladder Cancer Mortality in Taiwan. Int. J. Environ. Res. Public Health 2017, 14, 508. https://doi.org/10.3390/ijerph14050508
Yeh H-L, Hsu S-W, Chang Y-C, Chan T-C, Tsou H-C, Chang Y-C, Chiang P-H. Spatial Analysis of Ambient PM2.5 Exposure and Bladder Cancer Mortality in Taiwan. International Journal of Environmental Research and Public Health. 2017; 14(5):508. https://doi.org/10.3390/ijerph14050508
Chicago/Turabian StyleYeh, Hsin-Ling, Shang-Wei Hsu, Yu-Chia Chang, Ta-Chien Chan, Hui-Chen Tsou, Yen-Chen Chang, and Po-Huang Chiang. 2017. "Spatial Analysis of Ambient PM2.5 Exposure and Bladder Cancer Mortality in Taiwan" International Journal of Environmental Research and Public Health 14, no. 5: 508. https://doi.org/10.3390/ijerph14050508
APA StyleYeh, H.-L., Hsu, S.-W., Chang, Y.-C., Chan, T.-C., Tsou, H.-C., Chang, Y.-C., & Chiang, P.-H. (2017). Spatial Analysis of Ambient PM2.5 Exposure and Bladder Cancer Mortality in Taiwan. International Journal of Environmental Research and Public Health, 14(5), 508. https://doi.org/10.3390/ijerph14050508